Phys · respiratory
Respiratory Failure and Non-Invasive Ventilation
Also known as respiratory failure · type 1 respiratory failure · type 2 respiratory failure · NIV · BiPAP · CPAP · HFNO · controlled oxygen therapy · hypercapnic respiratory failure · acute hypercapnic respiratory failure · AHRF
Consultant-physician-depth guide to acute respiratory failure — type 1 versus type 2 physiology, systematic ABG interpretation, controlled oxygen therapy, NIV in acidotic COPD exacerbation, CPAP in cardiogenic pulmonary oedema, HFNO, intubation triggers, domiciliary NIV and ceilings of care — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Respiratory Failure and Non-Invasive Ventilation
The answer first
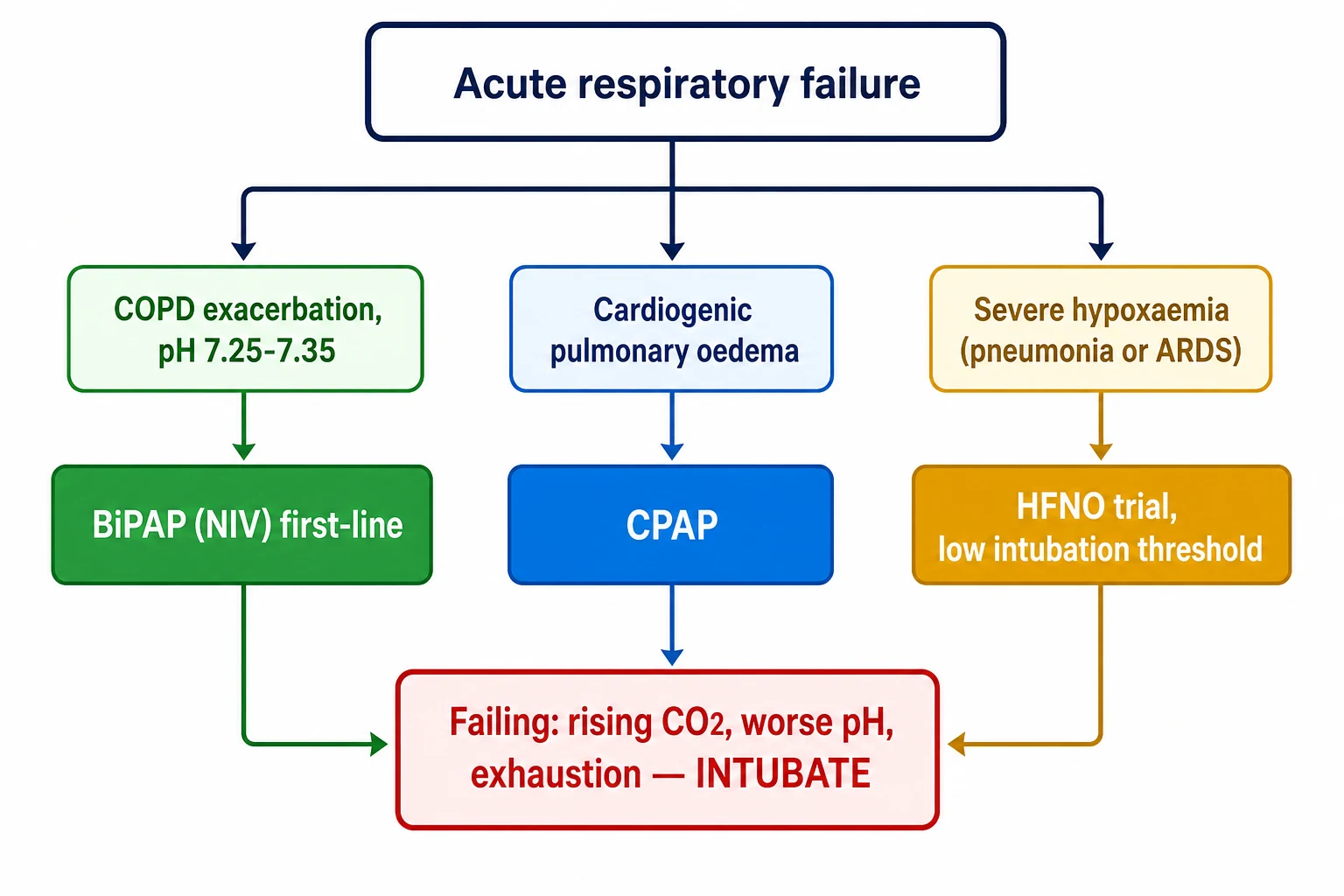
Acute respiratory failure is a failure of gas exchange, defined on arterial blood gas — and the entire clinical game is matching the type of failure to the right respiratory support, early. Four rules carry you through almost every DWE question and every after-hours ward call [1] [2]:
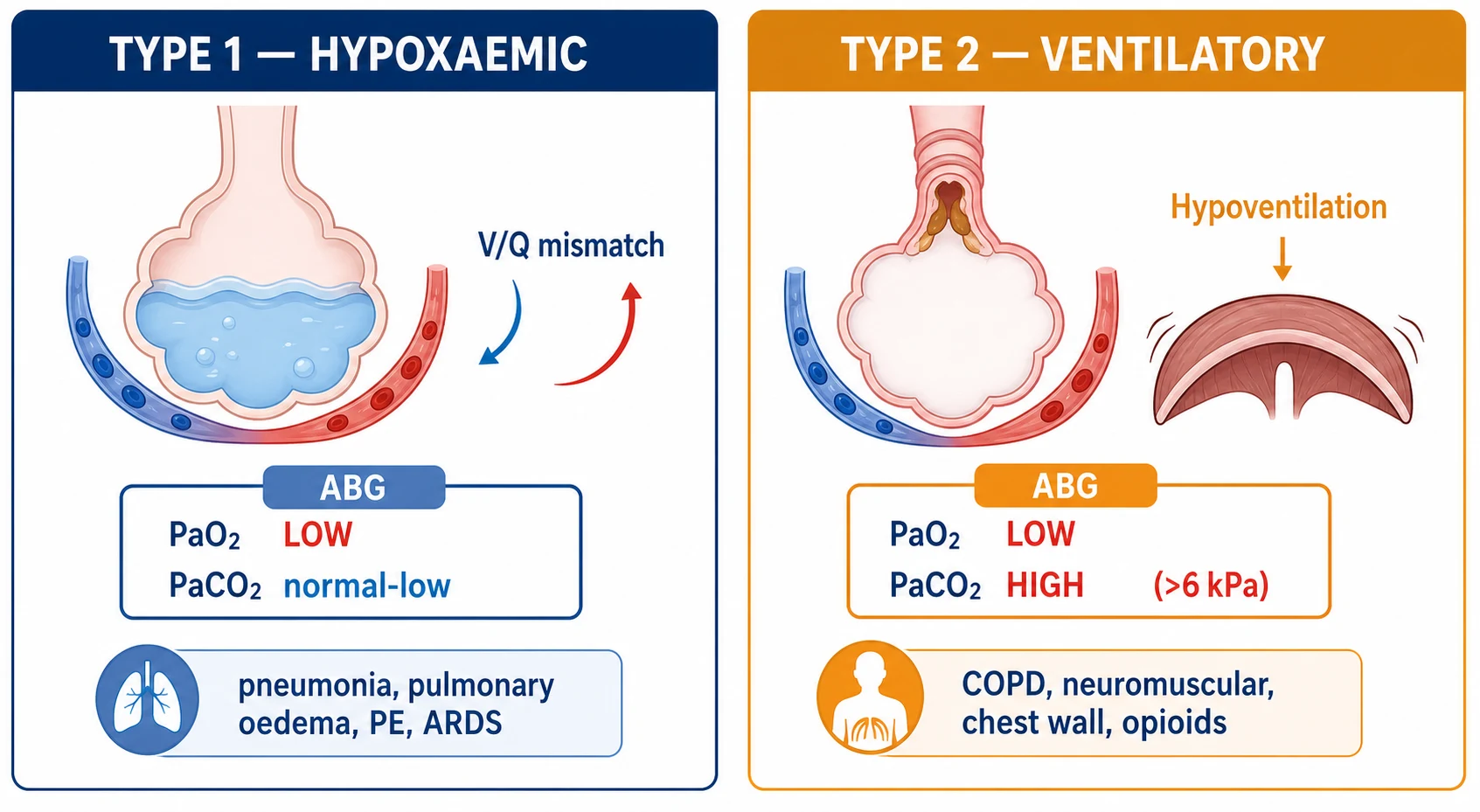
- Type 1 is oxygenation failure; type 2 is ventilation failure. Type 1 is a PaO₂ below 8 kPa with a normal or low PaCO₂ — the problem is the lung (V/Q mismatch, shunt). Type 2 adds a PaCO₂ above 6 kPa — the problem is the pump (reduced ventilatory drive, muscle weakness, or a load the muscles cannot meet) [2] [20].
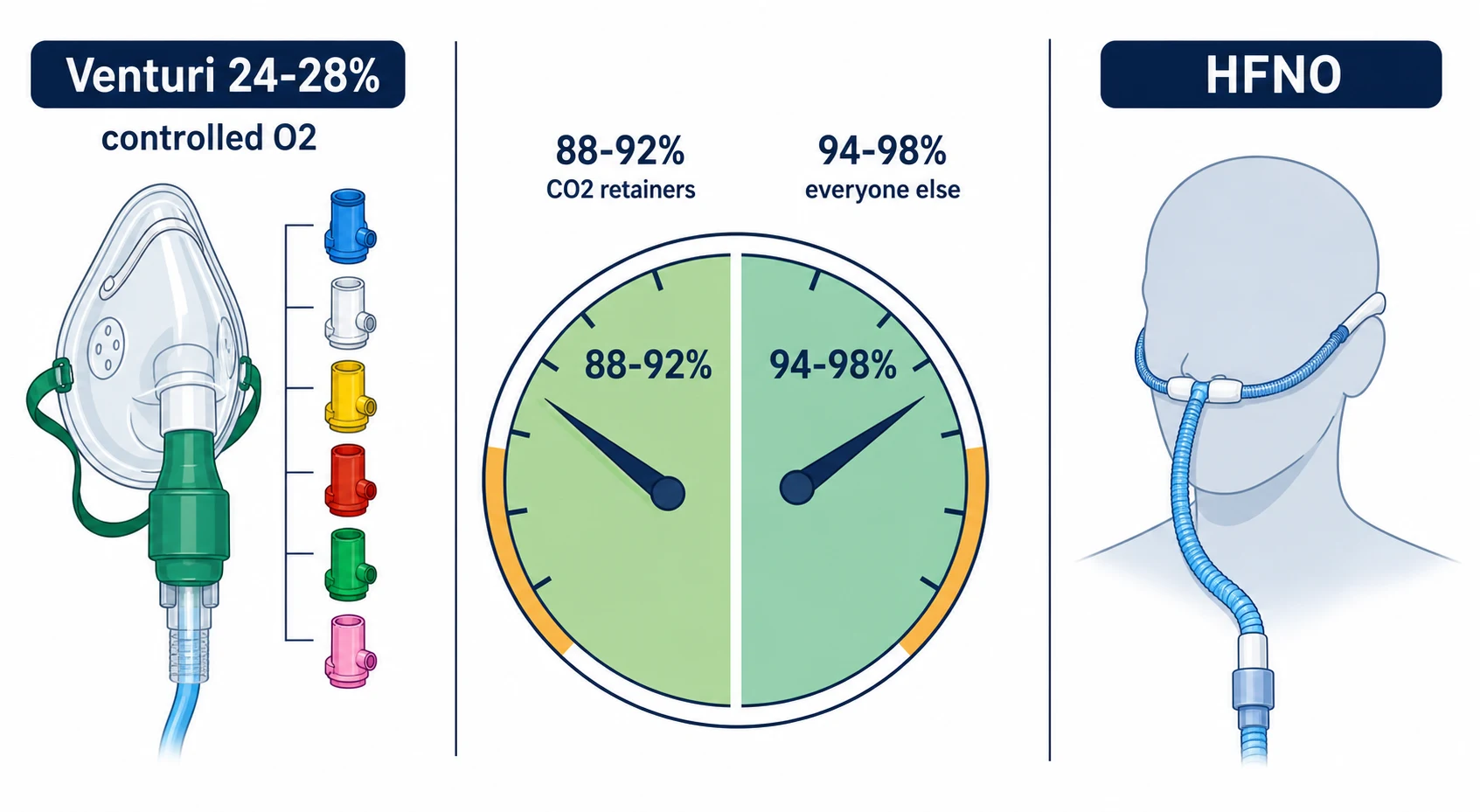
- Oxygen is a drug with a target, not a reflex. Most acutely ill adults are targeted to 94–98%, but anyone at risk of CO₂ retention — COPD above all — gets controlled oxygen (24–28% Venturi) aiming for 88–92%, with a blood gas checked after any change [3] [4].
- An acidotic COPD exacerbation is an NIV emergency. pH below 7.35 with hypercapnia despite maximal medical therapy means BiPAP now — it reduces intubation and death, and the evidence is among the strongest in acute medicine. Cardiogenic pulmonary oedema, by contrast, gets CPAP [2] [7] [9].
- NIV is a trial with an exit, not a destination. Repeat the blood gas at 1–2 hours. Improving pH and PaCO₂ means continue; worsening acidosis, exhaustion, secretions or agitation means stop escalating and intubate — delayed intubation is the classic fatal error [2] [19].
Two failures, one physiology
The two types of respiratory failure are not arbitrary ABG labels — they are two different physiological catastrophes, and the therapy that fixes one can be irrelevant to the other [20].
Type 1 — hypoxaemic failure. Oxygen fails to cross from alveolus to blood. The dominant mechanism is ventilation–perfusion mismatch: alveoli that are perfused but poorly ventilated (pneumonia consolidation, pulmonary oedema, atelectasis) let blood pass without picking up oxygen; at the extreme this is true shunt. Diffusion limitation and low inspired oxygen (altitude) contribute in narrower settings. Crucially, CO₂ clearance is preserved — CO₂ is about twenty times more diffusible than oxygen and the surviving ventilated lung increases its minute ventilation, so the PaCO₂ is normal or low. The clinical signature is breathlessness, tachypnoea, and hypoxaemia that may partly correct with oxygen [20] [21].
Type 2 — ventilatory failure. The pump fails and alveolar ventilation falls; PaCO₂ rises in direct proportion to the fall in ventilation, and PaO₂ falls with it. The causes sort into three bins: central drive (opioids, sedatives, brainstem lesions), neuromuscular and chest wall (motor neurone disease, Guillain–Barré, myasthenia, kyphoscoliosis, obesity hypoventilation), and increased load with fatiguing muscles — above all COPD, where airways obstruction, hyperinflation and flattened diaphragms mean the muscles cannot sustain the work [2] [21].
| Feature | Type 1 (hypoxaemic) | Type 2 (hypercapnic / ventilatory) |
|---|---|---|
| PaO₂ | Below 8 kPa (60 mmHg) | Below 8 kPa (often, not always) |
| PaCO₂ | Normal or low | Above 6 kPa (45 mmHg) |
| Core mechanism | V/Q mismatch, shunt, diffusion limitation | Alveolar hypoventilation [20] |
| Classic causes | Pneumonia, pulmonary oedema, PE, ARDS, fibrosis | COPD, neuromuscular disease, chest wall, opioids, obesity hypoventilation |
| First-line support | Oxygen to target; HFNO if escalating; treat the cause | Treat the cause; NIV if acidotic; controlled oxygen if a retainer [1] [2] |
Reading the ABG properly — oxygenation, acid–base, compensation
Examiners can tell within ten seconds whether you read a gas systematically or scan it for the number you fear. The method below is fast, defensible, and works for every gas you will ever be shown [21].
The four-step gas read
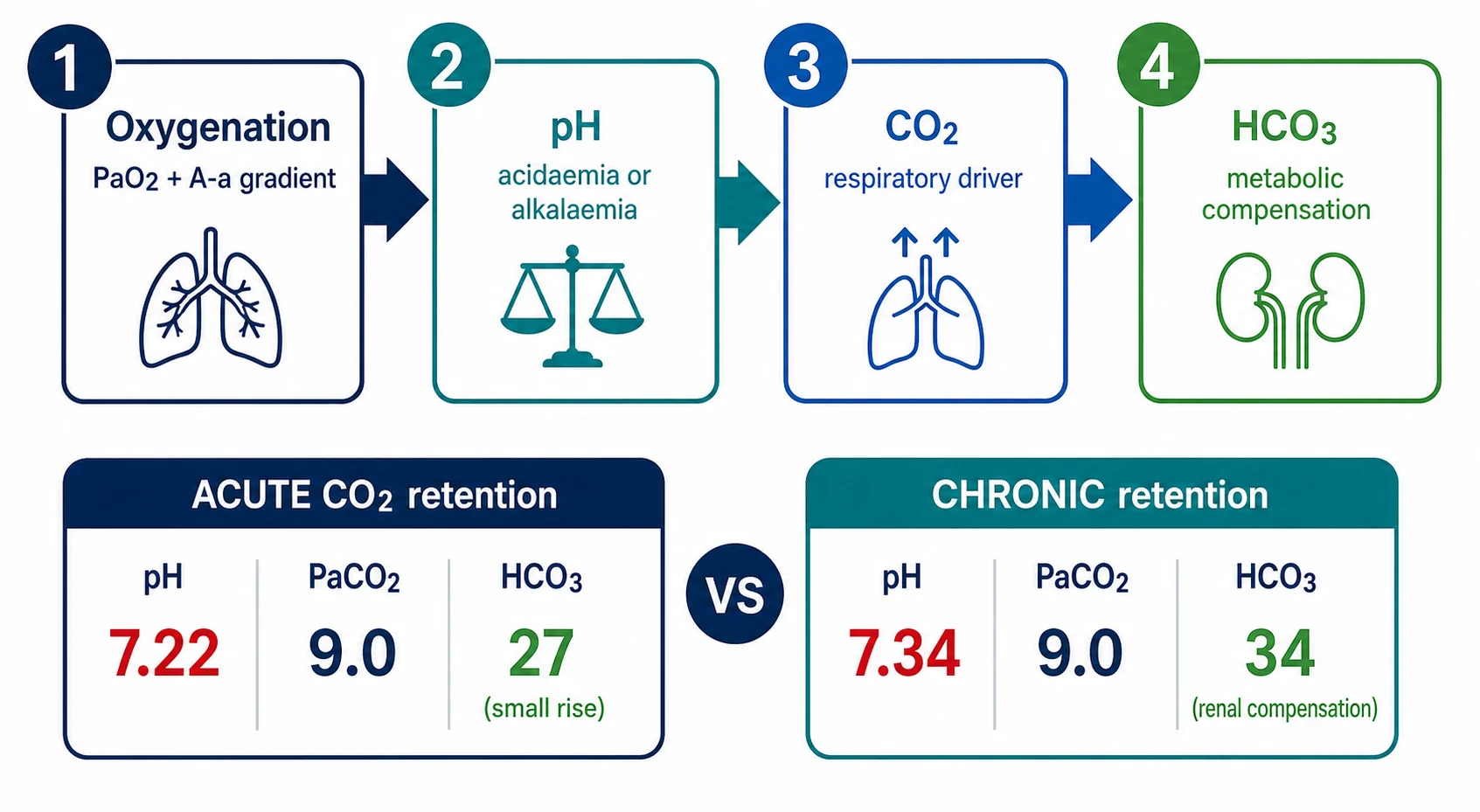
Oxygenation
PaO2 against the FiO2 the patient was on when sampled (never quote a gas without its oxygen context); compute the A-a gradient if the picture is mixed
pH
Acidaemia (below 7.35) or alkalaemia (above 7.45) — this defines the primary direction of the disturbance and its physiological threat
PaCO2
Is the CO2 moving with the pH (respiratory driver: high CO2 with low pH) or against it (metabolic driver with respiratory compensation)?
HCO3 and compensation
Is the bicarbonate appropriate? A high HCO3 out of proportion to an acute CO2 rise signals chronic retention with renal compensation — the gas of stable severe COPD
Acute versus chronic retention is read from the pH–HCO₃ pair. In acute CO₂ retention, the kidneys have had no time to compensate: bicarbonate is near normal (rises only about 1 mmol/L per 1.3 kPa rise in PaCO₂ from tissue buffering), so the pH falls sharply — pH 7.22 with PaCO₂ 9 kPa and HCO₃ 27. In chronic retention, renal bicarbonate retention (over 3–5 days) drags the pH back toward normal: pH 7.34 with the same PaCO₂ 9 kPa but HCO₃ 34. The acute-on-chronic gas — the decompensated COPD exacerbation — shows a high HCO₃ with a pH that has nonetheless fallen: the compensation was there, and the new insult has overwhelmed it [21] [2].
| Gas pattern | pH | PaCO₂ | HCO₃ | Interpretation |
|---|---|---|---|---|
| Acute ventilatory failure | 7.22 | 9.0 kPa | 27 | Acute CO₂ retention — no renal compensation yet [21] |
| Chronic compensated | 7.36 | 8.5 kPa | 36 | Stable severe COPD at baseline — do not treat the number |
| Acute-on-chronic | 7.26 | 10.5 kPa | 34 | Decompensation on a compensated baseline — the classic NIV gas [2] |
| Type 1 failure | 7.46 | 4.2 kPa | 23 | Hypoxaemia-driven hyperventilation — look for pneumonia, PE, oedema [20] |
Oxygen therapy — a drug with a prescription
Oxygen is the most commonly prescribed drug in acute medicine and the least commonly prescribed properly. The modern framing — written into both the BTS guideline and the Thoracic Society of Australia and New Zealand guideline — is that oxygen is prescribed to a target saturation range, with the device and flow chosen to hit that range, and the response checked [3] [4].
Oxygen targets by context — BTS and TSANZ consensus
Why controlled oxygen matters in the retainer — and why the old story is wrong. The teaching you inherited is that COPD patients "breathe off their hypoxic drive" and that oxygen switches off ventilation. That is a myth, and it is dangerous in both directions — it makes juniors terrified of oxygen in the hypoxaemic, and it makes them casual about it in the retainer. The measured mechanisms of oxygen-induced hypercapnia are, in order of importance: reversal of hypoxic pulmonary vasoconstriction (oxygen re-opens vessels in poorly ventilated lung, worsening V/Q mismatch and dead space), the Haldane effect (oxygenated haemoglobin carries less CO₂, raising PaCO₂ at a fixed ventilation), and only a small true fall in minute ventilation. The practical point stands despite the mechanism being mislabelled: uncontrolled oxygen in a susceptible retainer produces real, sometimes fatal, rises in PaCO₂ [16].
The evidence for controlled oxygen is not theoretical. In a randomised trial of prehospital care for suspected COPD exacerbations, titrated oxygen delivered by nasal cannulae to an SpO₂ of 88–92% reduced mortality by more than half compared with high-flow oxygen — with less acidosis and less hypercapnia on arrival [14]. And the IOTA meta-analysis of acutely ill adults found that liberal oxygen strategies increased mortality in a dose-dependent way compared with conservative targets — hyperoxia is a treatment exposure with a harm profile, not a safety blanket [15].
The acidotic COPD exacerbation — NIV is the treatment
This is the single highest-yield indication in the whole topic, and one of the strongest evidence bases in acute medicine. A COPD exacerbation that has progressed to respiratory acidosis — pH below 7.35 with a raised PaCO₂ — despite maximal medical therapy (controlled oxygen, nebulised bronchodilators, steroids, antibiotics where indicated) is an indication for NIV, and every hour of delay costs benefit [2] [7].
The trial sequence examiners expect, in order [5]:
| Trial | Setting | Population | What it showed | What it changed |
|---|---|---|---|---|
| Brochard (1995) | ICU | COPD exacerbation, acute respiratory failure | NIV vs standard therapy: lower intubation rate, shorter stay, lower mortality | Established NIV as more than a bridge to intubation [5] |
| Plant (2000) | General respiratory wards | Mild–moderate acidosis (mean pH about 7.34) | Ward-based NIV halved the need for intubation and reduced in-hospital mortality | Moved NIV out of the ICU and onto the ward [6] |
| Cochrane (Osadnik 2017) | Meta-analysis | Acute hypercapnic failure due to COPD exacerbation | NIV reduced mortality (NNT roughly a dozen), reduced intubation, shortened stay | Cemented NIV as standard of care; effect strongest once pH is below 7.35 [7] |
NIV in the acidotic COPD exacerbation — the working numbers
What BiPAP actually does. The two pressures do two different jobs, and viva candidates who can say this cleanly stand out. IPAP (inspiratory positive airway pressure) is the ventilatory pressure — it augments tidal volume, rests fatigued inspiratory muscles, and clears CO₂; titrating IPAP up is how you treat the acidosis. EPAP (expiratory positive airway pressure) splints the airway against dynamic collapse and offsets intrinsic PEEP (auto-PEEP) so the patient does not have to overcome trapped-gas pressure before each breath can begin; it also recruits alveoli and helps oxygenation. The gradient between IPAP and EPAP is the pressure support — that is what does the ventilating [2] [1].
Starting NIV on the ward — the first hour
Confirm the indication
ABG: pH below 7.35, PaCO2 raised, on controlled oxygen with medical therapy running; check contraindications (vomiting, reduced GCS, shock, facial trauma, untreated pneumothorax, copious secretions)
Set the ceiling and the plan
Is this patient for intubation if NIV fails? Document the escalation plan and ceiling of care BEFORE starting
Explain and fit
Show the mask, explain it will feel like strong wind, start with the mask held (not strapped) so the patient keeps control — tolerance is the first battle
Settings
IPAP 10 rising toward 20-30 cmH2O as tolerated over the first hour, EPAP 4-5 cmH2O; controlled oxygen entrained to keep SpO2 88-92%
Monitor
Continuous oximetry, respiratory rate, synchrony with the machine, mask leak; repeat ABG at 1-2 hours — pH and PaCO2 trajectory is the verdict
Respond to the gas
Improving pH: continue, wean over 24-48 h as acidosis resolves. Worse or static with exhaustion: this is NIV failure — intubate if for escalation
Cardiogenic pulmonary oedema — CPAP, and an honest evidence story
Acute cardiogenic pulmonary oedema is type 1 failure driven by flooded alveoli — but the positive-pressure story here is CPAP, not BiPAP, and the evidence needs stating precisely because the trials say slightly different things [8] [9].
A single continuous pressure recruits fluid-filled alveoli, improves compliance and oxygenation, and — by raising intrathoracic pressure — reduces venous return and left ventricular afterload, offloading the failing heart in both directions. The Cochrane synthesis of non-invasive positive pressure in cardiogenic pulmonary oedema found CPAP (and bilevel) reduced mortality and intubation compared with standard oxygen therapy [9]. The large pragmatic 3CPO trial then compared CPAP and bilevel NIV against standard oxygen in over a thousand emergency patients: neither modality improved mortality, but both produced faster relief of breathlessness, acidosis and hypercapnia — and there was no excess of myocardial infarction with bilevel, burying an old safety fear [8].
The honest summary for an examiner: CPAP is first-line respiratory support for cardiogenic pulmonary oedema with persisting hypoxaemia or distress despite oxygen and medical therapy; expect rapid symptomatic benefit, claim mortality benefit cautiously (meta-analyses yes, the largest single trial no), and prefer CPAP over bilevel unless there is concurrent hypercapnia with acidosis. And it is an adjunct — the definitive treatment is vasodilators (glyceryl trinitrate), diuretics where volume-overloaded, and treatment of the trigger [8] [9] [1].
Monitoring NIV — and recognising failure early
NIV is prescribed like a drug with a therapeutic window, and the repeat blood gas is the serum level. The BTS/ICS guideline is explicit: reassess clinically and repeat the ABG at 1–2 hours after starting, and after any change in settings or FiO₂ [2].
Success looks like: a rising pH (even a small rise matters), a falling PaCO₂, falling respiratory rate, improving synchrony and comfort, and a patient who can talk and eventually doze. Failure looks like: a pH that is static or falling at 1–2 hours, rising PaCO₂, persisting tachypnoea and exhaustion, copious secretions the patient cannot clear, agitation or deteriorating conscious level, haemodynamic instability, or a mask the patient simply cannot tolerate despite adjustment [2] [19].
For hypoxaemic indications the same discipline applies with harder stakes. In a multicentre study of NIV in acute hypoxaemic respiratory failure, NIV failure — and subsequent intubation — was common and was predicted by older age, higher severity scores, ARDS or pneumonia as the cause, and failure to improve oxygenation early; intubation after failed NIV carried high mortality, which is why the threshold to stop must be low and predefined [19].
Absolute and near-absolute contraindications — the list that wins or loses DWE marks [2]:
- Immediately life-threatening failure needing emergent intubation (respiratory arrest, peri-arrest, severe refractory hypoxaemia).
- Inability to protect the airway: vomiting or high aspiration risk, reduced conscious level (unless rapidly reversible, e.g., hypercapnic narcosis that wakes on NIV — a nuance examiners enjoy), uncontrolled upper GI bleeding, facial trauma or recent upper airway surgery.
- Haemodynamic instability or serious arrhythmia.
- Copious secretions the patient cannot clear.
- Untreated pneumothorax.
- Undrained facial burns / inability to fit a mask, and patient refusal [2].
Where NIV needs caution — pneumonia and the immunosuppressed
The NIV evidence base was built on COPD and cardiogenic pulmonary oedema. Extrapolating it to de novo hypoxaemic failure — pneumonia and ARDS — is where candidates get burned [1] [23].
The one RCT examiners cite is Confalonieri: in severe community-acquired pneumonia with acute respiratory failure, NIV reduced intubation and ICU mortality only in the subgroup with underlying COPD — patients without COPD derived no clear benefit. Read it as a COPD study wearing pneumonia clothes, not as a mandate to ventilate pneumonias non-invasively [23]. The ERS/ATS guideline, weighing this and the failure data, suggests NIV in de novo hypoxaemic failure only cautiously and selectively — with experienced teams, close monitoring, and a low, predefined intubation threshold — because failed NIV followed by late intubation is associated with harm [1] [19].
The immunosuppressed patient deserves its own line because the trial story flipped. Older teaching favoured early NIV in immunocompromised patients to avoid intubation-related infection; the Lemiale JAMA trial (2015) randomised immunocompromised patients with acute hypoxaemic respiratory failure to NIV versus standard oxygen and found no difference in mortality or intubation — stripping NIV of any special advantage in this group. Modern practice: HFNO is often chosen for comfort and oxygenation, but the survival lever is the underlying diagnosis and early intubation when indicated, not the interface [11] [22].
High-flow nasal oxygen — where it fits
HFNO delivers heated, humidified oxygen at up to 60 L/min through wide-bore nasal prongs, washing out nasopharyngeal dead space, providing a small flow-dependent positive pressure, and — because the FiO₂ is set rather than entrained — delivering a reliable inspired fraction with far better comfort than a mask [22].
The landmark trial is FLORALI: in patients with acute hypoxaemic (non-hypercapnic) respiratory failure, mostly pneumonia, HFNO was compared with standard oxygen and with NIV. The primary intubation endpoint did not differ overall, but in the more hypoxaemic stratum intubation was reduced, and 90-day mortality was lower with HFNO — plausibly because NIV delivered high tidal volumes that aggravated lung injury. FLORALI repositioned HFNO as the default high-end oxygen device in hypoxaemic failure [10]. The ERS HFNO guideline gives HFNO a conditional recommendation over conventional oxygen in hypoxaemic respiratory failure, and a conditional recommendation over NIV in that setting — while emphasising that HFNO must not delay intubation when it is failing (watch the ROX pattern: saturations, FiO₂ requirement, and respiratory rate trajectory) [22].
When to intubate — the triggers
Intubation is the answer when the disease is winning faster than the non-invasive strategy. The triggers below are deliberately written as bedside observations, not numbers alone, because that is how the decision is actually made [2] [19]:
- Failed NIV trial: pH or PaCO₂ worsening at 1–2 hours, or any persisting severe acidosis with exhaustion.
- Refractory hypoxaemia: oxygenation deteriorating despite HFNO or NIV — particularly with rising work of breathing.
- Exhaustion and deteriorating conscious level — including CO₂ narcosis that is not lifting on NIV.
- Airway threat: vomiting, aspiration, secretions the patient cannot clear.
- Haemodynamic collapse or malignant arrhythmia.
- Multi-organ failure where respiratory failure is one failing organ among several [19].
The corollary: intubation must also be the answer you are allowed to give. A patient with a documented decision against ICU admission is not "failed NIV" — they are a patient at their ceiling, and the job changes to symptom control [2].
Domiciliary NIV — who actually benefits at home
Long-term home NIV is not "acute NIV that never stopped" — it is a selected, titrated therapy for chronic ventilatory failure, and the evidence is diagnosis-specific [12] [13].
| Population | Evidence | Practical selection |
|---|---|---|
| COPD with persistent hypercapnia 2–4 weeks after an acidotic exacerbation | HOT-HMV: home NIV plus oxygen versus oxygen alone extended the time to readmission or death (median about 4.3 vs 1.4 months) | Recheck gases 2–4 weeks post-discharge; offer home NIV if PaCO₂ remains above 7 kPa — NOT to everyone with COPD [12] |
| Stable severe COPD with chronic hypercapnia | Köhnlein RCT: home NIV targeting a marked PaCO₂ reduction improved one-year survival in stable hypercapnic COPD | The signal is for high-intensity NIV titrated to normalise CO₂, in genuinely hypercapnic patients [13] |
| Obesity hypoventilation syndrome | Masa (2019): in severe OHS with coexisting severe OSA, NIV and CPAP produced similar long-term improvements — choose by phenotype | Severe OSA-dominant disease: CPAP; hypoventilation-dominant or CPAP failure: NIV. Weight loss and diuretics for cor pulmonale underpin both [17] |
| Neuromuscular disease (MND/ALS and others) | Bourke RCT: NIV improved survival and quality of life in ALS with respiratory impairment, benefit strongest without severe bulbar dysfunction | Start at symptoms or early ventilatory decline — not at crisis; bulbar failure limits benefit [18] |
Weaning NIV and ceilings of care
Weaning is symptom- and gas-led, not clock-led. As the exacerbation resolves, move from near-continuous NIV to sessions (off for meals and nebulisers), then to nights only, then off — typically over 48–72 hours. The failure mode to name in the exam is the abrupt stop on day one because the first gas looked better, followed by relapse overnight; the acidosis took days to develop and the muscles have not recovered in an afternoon [2].
Ceilings of care are decided before the machine is switched on, not during failure. Every NIV order should carry two explicit, documented answers: is this patient for intubation and ICU if NIV fails?, and what was discussed with the patient and family? The BTS/ICS guideline treats NIV-as-ceiling as a legitimate, common plan in advanced COPD — NIV relieves dyspnoea and can return a drowsy hypercapnic patient to lucidity for a proper goals-of-care conversation — but it insists the status is recorded so the 3 a.m. team is not improvising someone's last hours [2].
The DCE angles
Long case — severe COPD with recurrent acidotic exacerbations. The examiner's interest moves quickly from the acute gas to the program. Your framework [2] [12]:
- The exacerbation that brought them in: severity, pH, NIV course, ICU exposure, and what this second admission says about trajectory.
- Optimising the disease: inhaler technique and escalation, pulmonary rehabilitation after every hospitalised exacerbation, vaccination, smoking cessation support, treatment of comorbid heart failure and OSA overlap.
- The domiciliary decisions: a 2–4 week post-discharge gas to find persistent hypercapnia (HOT-HMV selection for home NIV); long-term oxygen assessment if persistently hypoxaemic on air — remembering LTOT and home NIV answer different problems [12].
- Ceilings and advance care planning: prognosis stated honestly, NIV/intubation ceilings documented, an advance care plan made while well.
- The social frame: function, carer strain, anxiety around breathlessness, and palliative symptom strategies for refractory dyspnoea.
Short case — the breathless patient. Work from the end of the bed: respiratory rate and pattern, accessory muscle use and tracheal tug, pursed-lip breathing, thoracoabdominal paradox (fatigue and impending arrest), ability to speak in sentences. Then the CO₂-retention cluster — coarse flap (asterixis), bounding pulse, warm peripheries, drowsiness — distinguished from the fine tremor of salbutamol, and central cyanosis at the tongue. Then the chest: hyperinflation, breath sounds, added sounds, and the cor pulmonale triad of raised JVP, loud P₂, parasternal heave and peripheral oedema. Close by saying what you would do next: sit them up, controlled oxygen, and a blood gas [2] [16].
Exam traps, collected
References
- [1]Rochwerg B, Brochard L, Elliott MW, et al. Official ERS/ATS clinical practice guidelines: noninvasive ventilation for acute respiratory failure Eur Respir J, 2017.PMID 28860265
- [2]Davidson AC, Banham S, Elliott M, et al. BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults Thorax, 2016.PMID 26976648
- [3]O'Driscoll BR, Howard LS, Earis J, et al. BTS guideline for oxygen use in adults in healthcare and emergency settings Thorax, 2017.PMID 28507176
- [4]Beasley R, Chien J, Douglas J, et al. Thoracic Society of Australia and New Zealand oxygen guidelines for acute oxygen use in adults: 'Swimming between the flags' Respirology, 2015.PMID 26486092
- [5]Brochard L, Mancebo J, Wysocki M, et al. Noninvasive ventilation for acute exacerbations of chronic obstructive pulmonary disease N Engl J Med, 1995.PMID 7651472
- [6]Plant PK, Owen JL, Elliott MW Early use of non-invasive ventilation for acute exacerbations of chronic obstructive pulmonary disease on general respiratory wards: a multicentre randomised controlled trial Lancet, 2000.PMID 10859037
- [7]Osadnik CR, Tee VS, Carson-Chahhoud KV, et al. Non-invasive ventilation for the management of acute hypercapnic respiratory failure due to exacerbation of chronic obstructive pulmonary disease Cochrane Database Syst Rev, 2017.PMID 28702957
- [8]Gray A, Goodacre S, Newby DE, et al. Noninvasive ventilation in acute cardiogenic pulmonary edema N Engl J Med, 2008.PMID 18614781
- [9]Vital FM, Ladeira MT, Atallah AN Non-invasive positive pressure ventilation (CPAP or bilevel NPPV) for cardiogenic pulmonary oedema Cochrane Database Syst Rev, 2013.PMID 23728654
- [10]Frat JP, Thille AW, Mercat A, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure N Engl J Med, 2015.PMID 25981908
- [11]Lemiale V, Mokart D, Resche-Rigon M, et al. Effect of Noninvasive Ventilation vs Oxygen Therapy on Mortality Among Immunocompromised Patients With Acute Respiratory Failure: A Randomized Clinical Trial JAMA, 2015.PMID 26444879
- [12]Murphy PB, Rehal S, Arbane G, et al. Effect of Home Noninvasive Ventilation With Oxygen Therapy vs Oxygen Therapy Alone on Hospital Readmission or Death After an Acute COPD Exacerbation: A Randomized Clinical Trial JAMA, 2017.PMID 28528348
- [13]Köhnlein T, Windisch W, Köhler D, et al. Non-invasive positive pressure ventilation for the treatment of severe stable chronic obstructive pulmonary disease: a prospective, multicentre, randomised, controlled clinical trial Lancet Respir Med, 2014.PMID 25066329
- [14]Austin MA, Wills KE, Blizzard L, et al. Effect of high flow oxygen on mortality in chronic obstructive pulmonary disease patients in prehospital setting: randomised controlled trial BMJ, 2010.PMID 20959284
- [15]Chu DK, Kim LH, Young PJ, et al. Mortality and morbidity in acutely ill adults treated with liberal versus conservative oxygen therapy (IOTA): a systematic review and meta-analysis Lancet, 2018.PMID 29726345
- [16]Abdo WF, Heunks LM Oxygen-induced hypercapnia in COPD: myths and facts Crit Care, 2012.PMID 23106947
- [17]Masa JF, Mokhlesi B, Benítez I, et al. Long-term clinical effectiveness of continuous positive airway pressure therapy versus non-invasive ventilation therapy in patients with obesity hypoventilation syndrome: a multicentre, open-label, randomised controlled trial Lancet, 2019.PMID 30935737
- [18]Bourke SC, Tomlinson M, Williams TL, et al. Effects of non-invasive ventilation on survival and quality of life in patients with amyotrophic lateral sclerosis: a randomised controlled trial Lancet Neurol, 2006.PMID 16426990
- [19]Antonelli M, Conti G, Moro ML, et al. Predictors of failure of noninvasive positive pressure ventilation in patients with acute hypoxemic respiratory failure: a multi-center study Intensive Care Med, 2001.PMID 11810114
- [20]Petersson J, Glenny RW Gas exchange and ventilation-perfusion relationships in the lung Eur Respir J, 2014.PMID 25063240
- [21]Williams AJ ABC of oxygen: assessing and interpreting arterial blood gases and acid-base balance BMJ, 1998.PMID 9794863
- [22]Oczkowski S, Ergan B, Bos L, et al. ERS clinical practice guidelines: high-flow nasal cannula in acute respiratory failure Eur Respir J, 2022.PMID 34649974
- [23]Confalonieri M, Potena A, Carbone G, et al. Acute respiratory failure in patients with severe community-acquired pneumonia. A prospective randomized evaluation of noninvasive ventilation Am J Respir Crit Care Med, 1999.PMID 10556125