Phys · respiratory
Respiratory Investigation: PFTs, Bronchoscopy and Thoracoscopy
Also known as pulmonary function tests · PFTs · spirometry · flow-volume loop · lung volumes · DLCO · transfer factor · TLCO · methacholine challenge · bronchoprovocation · flexible bronchoscopy · EBUS-TBNA · endobronchial ultrasound · medical thoracoscopy · pleuroscopy · pleural biopsy · thoracentesis · Light's criteria
Consultant-physician-depth guide to respiratory investigation — spirometry and flow-volume loops, lung volumes and DLCO, bronchoprovocation testing, flexible bronchoscopy and EBUS-TBNA, navigational bronchoscopy, thoracentesis with Light's criteria, pleural biopsy routes and medical thoracoscopy — built around the question-first framework for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Respiratory Investigation: PFTs, Bronchoscopy and Thoracoscopy
The answer first
Respiratory investigation is question-driven, not panel-driven. Every test in this topic answers one named question, and the consultant-level skill is stating the question before stating the test: Is this obstruction or restriction? (spirometry plus lung volumes). Is the gas-transfer membrane diseased? (DLCO). Is this asthma with normal spirometry today? (bronchoprovocation). What is this node, nodule or effusion made of? (bronchoscopy, EBUS or pleural biopsy). The examiner's favourite trap is the candidate who orders everything and interprets nothing [1].
Three rules carry you through most DWE questions and every data station [1]:
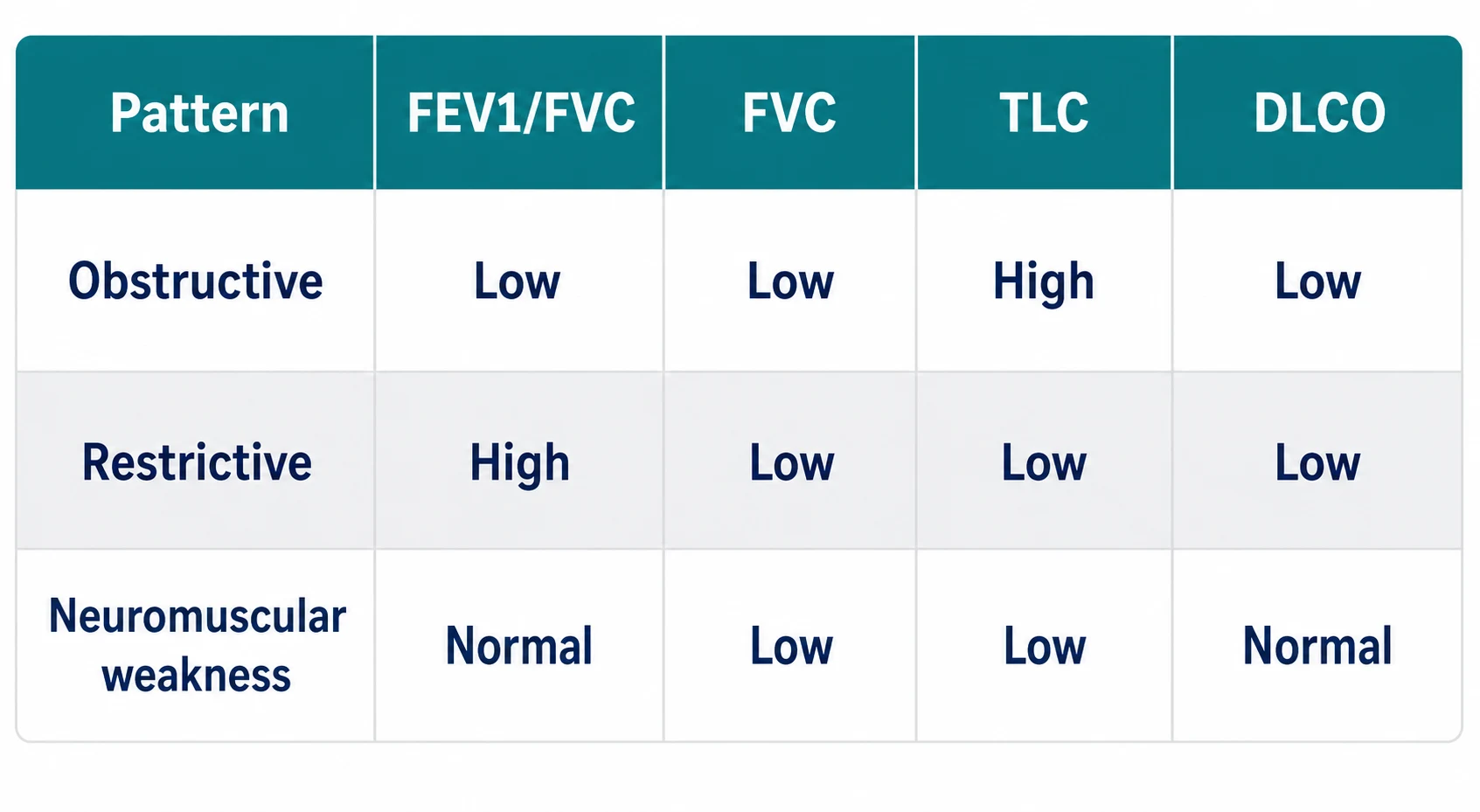
- Spirometry diagnoses obstruction; it can only suggest restriction. A low FEV1/FVC ratio (below the lower limit of normal) is obstruction. A low FVC with a preserved ratio is suspected restriction — but restriction is a diagnosis of lung volumes, confirmed only when the total lung capacity is low [1].
- DLCO is the membrane test — and it lies when haemoglobin is abnormal. Interstitial lung disease, emphysema and pulmonary vascular disease lower it; asthma, obesity and alveolar haemorrhage raise it; and anaemia lowers the measured value without any lung disease at all, which is why haemoglobin adjustment is built into the standard [4].
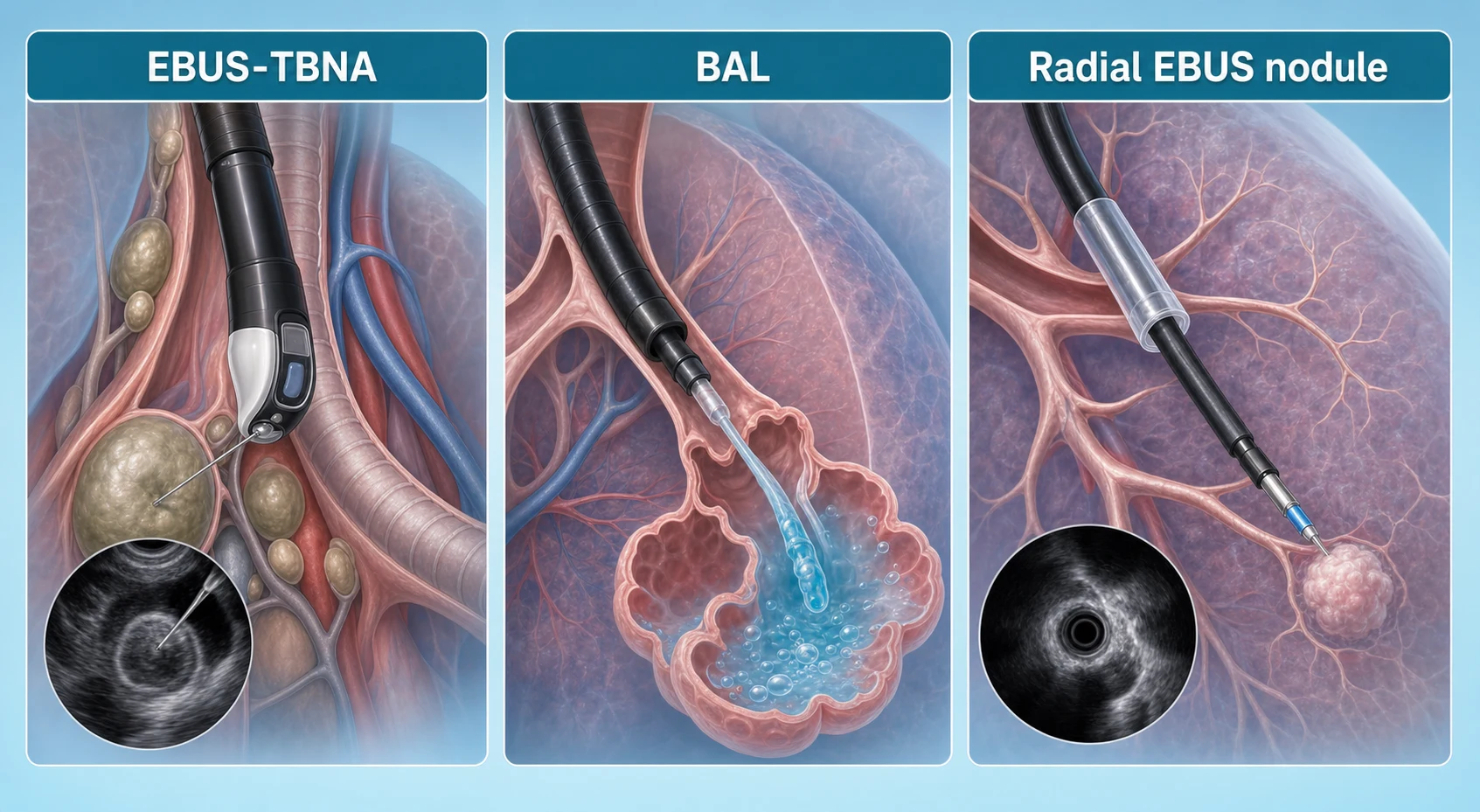
- Tissue questions are answered by the least invasive route that reaches the lesion. Mediastinal nodes go to EBUS-TBNA first (not mediastinoscopy), peripheral nodules to navigational or radial-EBUS bronchoscopy, and unexplained exudative pleura to image-guided biopsy or medical thoracoscopy [10] [17].
Spirometry — the gateway measurement
Spirometry measures forced expiratory volume in one second (FEV1) and forced vital capacity (FVC) during a maximal forced manoeuvre from full inflation. Before any number is interpreted, the manoeuvre must be acceptable and reproducible: a maximal blast without hesitation, no cough in the first second, complete expiration, and repeatability between the two best efforts within about 150 mL — numbers from a badly performed test are worse than no numbers [2].
Obstruction is a low FEV1/FVC ratio — below the lower limit of normal (LLN), conventionally the 5th percentile of the predicted reference distribution. The modern ERS/ATS position is LLN-based interpretation using validated reference equations (the Global Lung Function Initiative set), because a fixed ratio of 0.70 ignores the normal age-related fall in elastic recoil and over-diagnoses obstruction in older adults while under-diagnosing it in the young [1]. Severity is then graded by the FEV1 as a percentage of predicted [3].
| Severity band (classic ATS/ERS) | FEV1 (% predicted) | Working example |
|---|---|---|
| Mild | 70 or above | Often asymptomatic; found on screening spirometry [3] |
| Moderate | 60–69 | Exertional dyspnoea appears |
| Moderately severe | 50–59 | Limits ordinary activity |
| Severe | 35–49 | Dyspnoea on minimal exertion; exacerbations dominate |
| Very severe | Below 35 | Respiratory failure territory — correlate with gases and clinical state |
Reversibility testing asks whether obstruction improves after a bronchodilator — classically salbutamol 200–400 micrograms by spacer, repeating spirometry after 10–15 minutes. The classic positive response is an increase in FEV1 or FVC of at least 12% of baseline and 200 mL; the 2022 ERS/ATS technical standard expresses it as an increase exceeding 10% of the predicted value. Either way, the physiological claim is the same: a large, immediate improvement supports asthma over fixed airflow limitation — but a negative test does not exclude asthma, because airway calibre in asthma varies over time and with treatment [3] [1].
Spirometry in one row
Flow-volume loops — the shape is the diagnosis
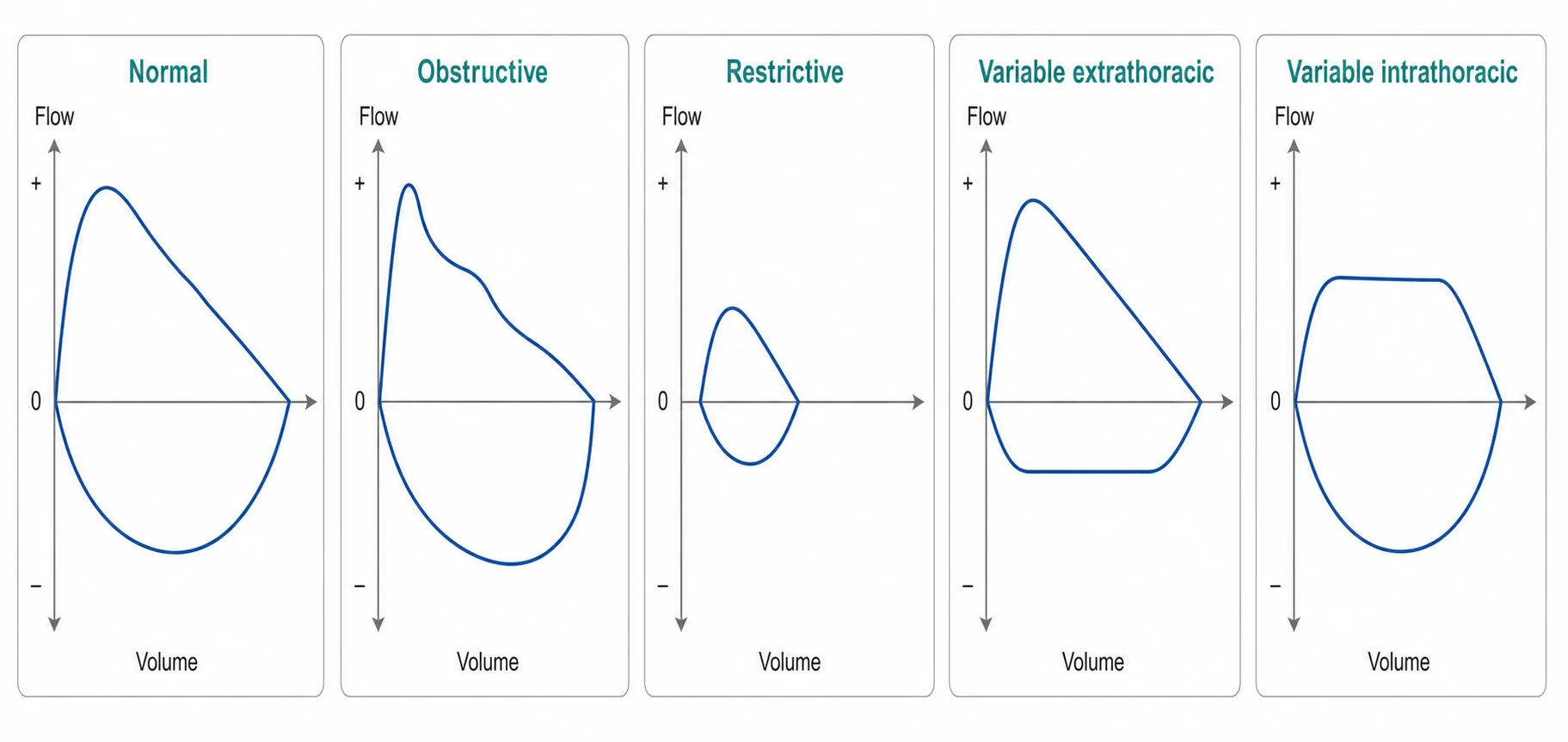
Plotting flow against volume through the whole forced manoeuvre turns one number into a picture. The classic patterns were defined by Miller and Hyatt for tracheal and laryngeal lesions, and they remain a favourite DCE data-station gift [8].
| Pattern | Loop appearance | Physiological meaning | Classic causes |
|---|---|---|---|
| Normal | Rapid peak, near-linear expiratory descent, smooth inspiratory curve | Unobstructed central and peripheral airways | — |
| Obstructive (intrapulmonary) | Scooped, concave expiratory limb with reduced flows at low lung volumes | Dynamic airway collapse from recoil loss or airway narrowing | COPD/emphysema, asthma [3] |
| Restrictive | Small, narrow loop — normal shape, reduced size, often a steep descent | Reduced lung volumes with preserved emptying rate | ILD, chest-wall disease [1] |
| Fixed upper-airway obstruction | Flattening of BOTH inspiratory and expiratory limbs (a "box" loop) | A rigid stenosis that cannot change calibre with pressure | Tracheal stenosis, large goitre, bilateral cord palsy [8] |
| Variable extrathoracic obstruction | Flattened INSPIRATORY limb; expiration near normal | The lesion sits outside the thorax — negative intraluminal inspiratory pressure sucks it closed | Vocal cord dysfunction, tracheomalacia above the sternum, laryngeal tumour [8] |
| Variable intrathoracic obstruction | Flattened EXPIRATORY limb; inspiration near normal | The lesion sits inside the thorax — positive pleural pressure in expiration compresses it | Tracheomalacia of the intrathoracic trachea, distal tracheal or main-bronchus tumours [8] |
The mnemonic that survives exams: the limb that flattens tells you where the pressure works against the airway. Inspiration draws extrathoracic lesions shut (inspiratory plateau); expiration compresses intrathoracic lesions (expiratory plateau); a lesion that cannot move at all flattens both [8].
Lung volumes — spirometry cannot diagnose restriction
This is the single most examined concept in the whole topic, so say it plainly: restriction is defined by a reduced total lung capacity (TLC), and spirometry does not measure TLC. A low FVC with a preserved or high FEV1/FVC ratio raises the possibility of restriction — the "spirometric restrictive pattern" — but small lungs from a submaximal effort, severe obesity, early neuromuscular disease or true parenchymal restriction can all produce it. Only a measured TLC below the LLN confirms the diagnosis [1] [5].
Lung volumes are measured by body plethysmography or gas-dilution techniques, and the numbers that matter are TLC, residual volume (RV) and the RV/TLC ratio [5]:
- TLC below LLN — true restriction. Now use DLCO to split parenchymal from extrapulmonary causes [1].
- TLC normal or high with a low FVC — not restriction; think obstruction with air trapping, poor effort, or a mixed picture.
- Raised RV and RV/TLC — air trapping; supports obstructive disease, especially emphysema.
- Discrepancy between plethysmographic and gas-dilution volumes — trapped, non-communicating gas (bullous emphysema) is seen by the box but missed by dilution [5].
The neuromuscular pattern deserves its own paragraph because it is a DWE staple: respiratory muscle weakness (motor neurone disease/ALS, myasthenia, myopathy, phrenic nerve palsy) gives a low FVC, a low TLC, a normal DLCO and a normal or raised KCO — the alveolar-capillary membrane is intact, and the ventilated units are simply underfilled. The supporting clues are orthopnoea (the diaphragm works hardest lying flat), a weak cough, and low maximal inspiratory and expiratory pressures (MIP, MEP) or a low sniff nasal inspiratory pressure; a meaningful drop in FVC from sitting to supine points specifically at the diaphragm [1].
DLCO and KCO — the gas-transfer test
DLCO (transfer factor for carbon monoxide) measures how much CO crosses from alveolus to capillary blood in a single breath-hold. It integrates membrane thickness, capillary blood volume, haemoglobin availability and the alveolar volume actually ventilated — which is why it must be read with the haemoglobin and with KCO, the transfer coefficient per unit alveolar volume [4].
| DLCO finding | Mechanism | Classic causes |
|---|---|---|
| Low DLCO, low KCO | Membrane thickened or capillary bed destroyed | ILD/pulmonary fibrosis, emphysema [4] |
| Low DLCO with normal spirometry | Early disease invisible to spirometry, or vascular | Early ILD, pulmonary hypertension, CTEPH, recent PE — also anaemia [3] |
| Low DLCO, high KCO | Reduced ventilated volume with an intact membrane | Extrapulmonary restriction: neuromuscular weakness, chest-wall disease, pneumonectomy [1] |
| High DLCO | More blood or more haemoglobin exposed to alveolar gas | Asthma (often high-normal or high), obesity, polycythaemia, left-to-right shunt, alveolar haemorrhage [3] |
The two exam-critical subtleties: first, anaemia lowers measured DLCO artefactually because CO uptake depends on haemoglobin binding, and polycythaemia raises it — the 2017 ERS/ATS standard includes haemoglobin-adjustment equations and expects them to be applied before interpretation [4]. Second, alveolar haemorrhage can raise DLCO dramatically because free haemoglobin within alveoli binds the test CO directly — a classic DWE discriminator in the dyspnoea-plus-falling-haemoglobin vignette, and the reason DLCO is sometimes used to track pulmonary capillaritis activity [3].
Bronchoprovocation — answering "is this asthma?" when spirometry is normal
Asthma is variable airflow obstruction, so a normal spirometry result on a single day proves nothing. Bronchial challenge testing provokes the airway with a controlled stimulus and measures the fall in FEV1: methacholine (a direct muscarinic agonist) and mannitol (an indirect osmotic stimulus that triggers mast-cell mediator release) are the two in routine use, with exercise and eucapnic voluntary hyperpnoea as the physiological alternatives [6] [7].
Practical rules the exam expects [6] [7]:
- A negative challenge has a high negative predictive value — it makes current, untreated asthma unlikely, which is the main clinical use of the test [6].
- A positive challenge does not diagnose asthma by itself — airway hyperresponsiveness occurs in rhinitis, post-viral states, COPD and cystic fibrosis; the result only counts when it fits the clinical picture [7].
- Preparation matters: withhold short-acting bronchodilators for at least 6–8 hours, long-acting agents and leukotriene antagonists for longer, avoid caffeine on the day, and do not test within weeks of a respiratory infection — all of these blunt or exaggerate the response [6].
- The endpoint is the provocative dose or concentration causing a 20% fall in FEV1 (PD20/PC20 for methacholine; PD15 for mannitol) — the lower the dose needed, the more hyperresponsive the airway [7].
Reading PFTs as one physiological statement
The DCE data station gives you all four datasets at once — spirometry, the loop, lung volumes and DLCO — and the pass-level answer is one integrated sentence per dataset, then a synthesis and the next test [1].
| Dataset | Pattern you are handed | Integrated reading | Next step |
|---|---|---|---|
| Spirometry | FEV1/FVC low, FEV1 45% predicted | Obstruction, severe by FEV1 | Reversibility; clinical split asthma vs COPD [3] |
| Loop | Flattened inspiratory limb | Variable extrathoracic upper-airway obstruction | Laryngoscopy — not asthma escalation [8] |
| Volumes | TLC low, DLCO low | Confirmed parenchymal restriction | HRCT for ILD pattern [1] |
| Volumes + DLCO | TLC low, DLCO normal, KCO high | Extrapulmonary restriction | MIP/MEP, sniff test, diaphragm ultrasound [4] |
| DLCO | DLCO low with normal spirometry and volumes | Isolated gas-transfer defect | Check haemoglobin; HRCT; echo for pulmonary hypertension; consider CTEPH [4] |
| Spirometry | Normal, strong clinical asthma story | Non-diagnostic — asthma not excluded | Bronchoprovocation challenge [6] |
The data-station sequence (say it aloud in this order)
Quality
Are the manoeuvres acceptable and reproducible — can these numbers be trusted at all?
Ratio
FEV1/FVC against LLN: obstruction present or absent?
Volumes
TLC: restriction confirmed, refuted, or not yet testable?
Gas transfer
DLCO and KCO, haemoglobin-adjusted: membrane disease, vascular disease, or intact membrane?
Synthesis
One sentence naming the physiological defect and its most likely cause
Next test
The single investigation that will now change management
Bronchoscopy — match the tool to the question
Flexible bronchoscopy is not one test but a delivery platform, and the yield depends entirely on matching the sampling tool to the question [9].
| Clinical question | Tool | What it samples | Practical note |
|---|---|---|---|
| Visible central lesion (haemoptysis, collapse, stridor) | Endobronchial biopsy, brushings, washings | Tumour, mucosal pathology | Biopsy forceps give the highest yield for visible lesions [9] |
| Infection or diffuse infiltrate | Bronchoalveolar lavage (BAL) | Microbiology, cytology, cell count | Wedge the scope in the abnormal segment; BAL is the workhorse for opportunistic infection in the immunosuppressed [9] |
| Mediastinal or hilar nodes — cancer staging, sarcoidosis | EBUS-TBNA | Node core under real-time ultrasound | First-line for accessible nodes; mediastinoscopy reserved for negative EBUS with persistent suspicion [10] |
| Peripheral pulmonary nodule | Radial EBUS with guide sheath, or electromagnetic navigation | Nodule brushings/biopsy/washings | Yield around 70% in prospective multicentre data, with low pneumothorax rates — far safer than percutaneous biopsy for many nodules [12] |
| Diffuse ILD needing tissue | Transbronchial forceps biopsy (limited), transbronchial cryobiopsy (selected centres) | Parenchyma | Surgical lung biopsy remains the reference when histology will change management [9] |
EBUS-TBNA changed mediastinal diagnosis. In a prospective controlled trial against mediastinoscopy for lung-cancer staging, EBUS-TBNA achieved equivalent sensitivity for nodal disease with a fraction of the invasiveness — which is why guidelines place endosonography first and keep mediastinoscopy for the EBUS-negative high-suspicion case [10]. For sarcoidosis, the GRANULOMA randomised trial showed endosonography roughly doubled the granuloma-detection yield of conventional bronchoscopic biopsy — making EBUS-TBNA the standard first tissue test for bilateral hilar lymphadenopathy [11].
Safety is part of the exam answer. Diagnostic bronchoscopy is usually done under topical lignocaine plus conscious sedation (midazolam, with or without an opioid), with continuous oximetry and supplemental oxygen. The BTS guideline's anticoagulation rules are a recurring DWE item [9]:
- Aspirin: continue, including for biopsy [9].
- Clopidogrel and other P2Y12 inhibitors: withhold (typically 5 days) before biopsy — simple inspection and BAL carry lower bleeding concern than forceps sampling [9].
- Warfarin: withhold and confirm a safe INR before biopsy; DOACs: omit doses around the procedure per renal function and bleeding risk [9].
- Transbronchial biopsy, not forceps biopsy of a visible lesion, is the manoeuvre that carries the pneumothorax risk — arrange imaging after transbronchial parenchymal sampling in symptomatic or higher-risk patients [9].
Thoracoscopy and the pleural space
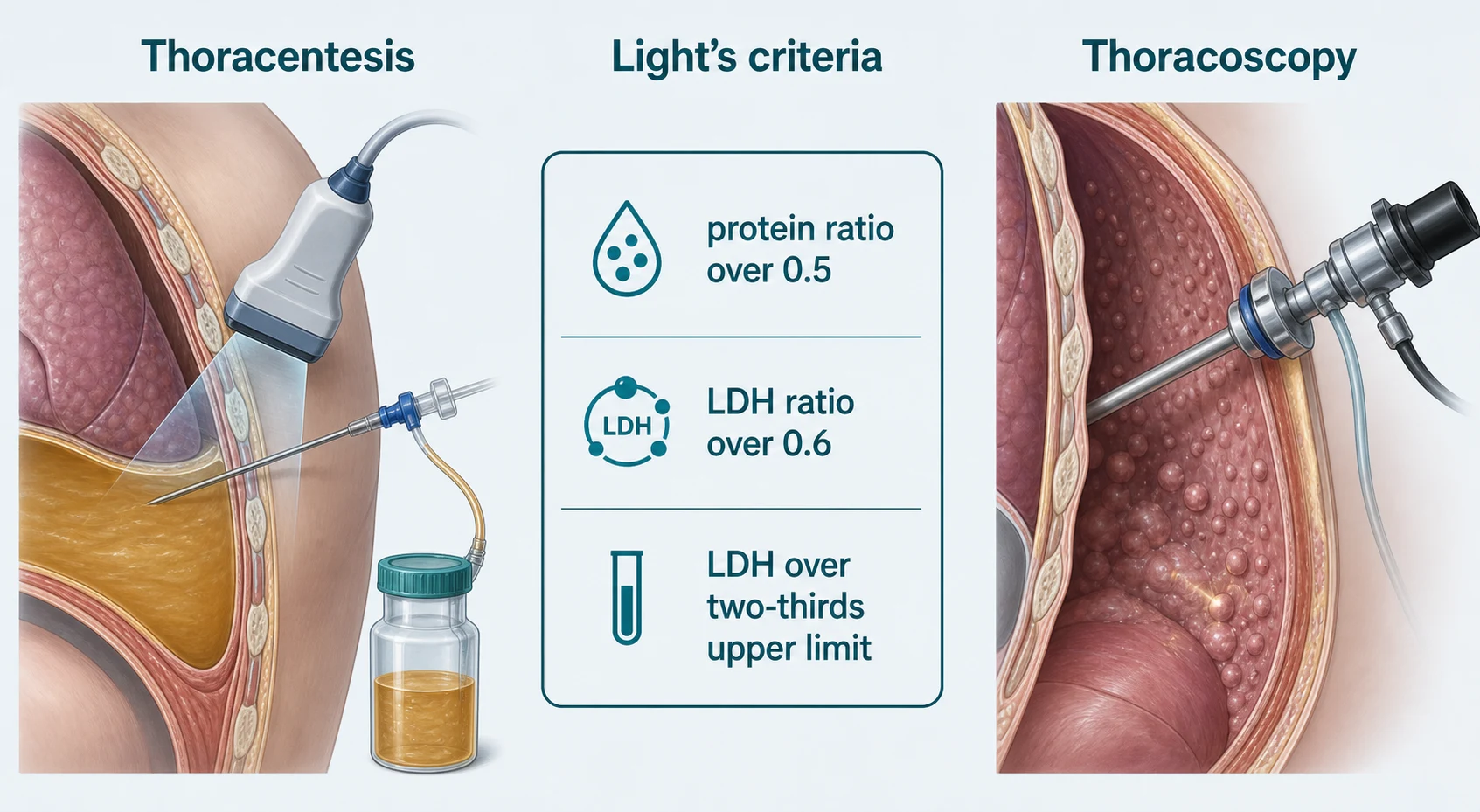
Every pleural effusion workup begins with the same two questions: is it an exudate, and does it need a drain? Both are answered by the fluid, not the scan — and the fluid should be obtained under ultrasound guidance, which BTS pleural guidance ties to fewer failed taps and fewer pneumothoraces [18].
The diuretic trap. Diuresis concentrates a heart-failure transudate: protein and LDH rise in the pleural space faster than in serum, and Light's criteria flip the fluid to "exudate" — the pseudoexudate. When the clinical picture says transudate but Light's criteria say exudate, the corrective move is a serum-to-pleural-fluid protein gradient above 3.1 g/dL (31 g/L) (or an albumin gradient above 1.2 g/dL), which pulls the fluid back to transudate [15] [14].
pH guides drainage in parapneumonic effusion. Meta-analysis of parapneumonic chemistry shows that a pleural pH at or below 7.2 (with low glucose and high LDH as concordant markers) identifies effusions that will not resolve with antibiotics alone — they need tube drainage. A pH above that threshold, with a non-purulent fluid and no organisms, supports antibiotics and observation [16].
| When the pleura itself must be sampled | Route | Strengths | Limits |
|---|---|---|---|
| No imaging target, cytology negative, thoracoscopy unavailable | Blind Abram's needle biopsy | Cheap, bedside | Lowest sensitivity; blind sampling of a patchy disease [17] |
| CT shows focal pleural thickening or nodules | Image-guided cutting-needle biopsy | High yield when a target exists; day-case | Misses patchy disease without a CT target [17] |
| Undiagnosed exudate after cytology; talc pleurodesis wanted at the same sitting | Medical thoracoscopy (pleuroscopy) | Direct vision, large targeted biopsies, drainage plus talc in one procedure | Needs a pleural space and physician pleuroscopy expertise [17] |
| Failed lung, complex septation, or surgical pathology likely | VATS | Full access, decortication possible | Anaesthesia and surgical cost; not a first diagnostic step [18] |
The randomised comparison by Metintas and colleagues found both CT-guided Abram's biopsy and medical thoracoscopy highly sensitive, with image-guided biopsy performing best where CT shows focal pleural disease and thoracoscopy adding value through vision, larger samples and same-session pleurodesis — so the modern answer is not "which is better" but "which suits this pleura and this question" [17].
Pneumothorax, briefly. The investigative overlap is small but examinable: recurrent spontaneous pneumothorax is the setting where VATS (surgical) rather than medical thoracoscopy is the intervention — for bullectomy and pleurodesis — while the physician's procedures (aspiration, intercostal drainage) remain ultrasound-and-safety governed by the same pleural guidance [18].
Choosing the test — the question-first framework
The whole topic compresses into one discipline: state the question, choose the least invasive test that answers it, and know in advance what each possible result will change [1].
The investigation-planning sequence
Name the question
Diagnosis, staging, severity, progression, or treatment response — a test without a question is noise
Pick the least invasive answerer
Physiology before imaging, imaging before needle, needle before scope, scope before surgery
Pre-decide the branches
Write down what you will do if the test is positive, negative and non-diagnostic
Check the patient can have it
Can they perform the test (spirometry), tolerate the sedation (bronchoscopy), or survive the complication (biopsy on anticoagulation)?
Sequence for information gain
Order tests so each result re-ranks the next step — EBUS before mediastinoscopy, cytology before biopsy, HRCT before lung biopsy decisions
The DCE angles
Short case — the PFT data station. This is the classic data-driven viva: you are handed spirometry, a loop, volumes and DLCO for a patient with dyspnoea, and examined on the read. The winning structure is the six-step sequence above — quality, ratio, volumes, gas transfer, synthesis, next test — delivered in about ninety seconds, ending with the single investigation that changes management. The three station archetypes to rehearse: ILD (restrictive with low DLCO → HRCT), obesity (low FVC, normal TLC, normal DLCO → no lung disease, deconditioning workup) and ALS/neuromuscular (low TLC, normal DLCO, high KCO → MIP/MEP and sniff pressures) [1] [4].
Long case — the ILD workup. Progressive dyspnoea with Velcro crackles integrates everything in this topic: HRCT pattern first (UIP versus non-UIP changes the whole pathway), PFTs to quantify the restrictive defect and the gas-transfer impairment (and to follow progression or treatment response), serology and exposure history to hunt a cause, and then the multidisciplinary question of whether tissue is needed at all — BAL cellularity in selected phenotypes, cryobiopsy or surgical biopsy only when the result would change treatment, weighed against procedural risk in a fibrotic lung [1] [9]. The examiner is listening for the discipline: the test is chosen because its answer changes management, and deferred when it does not.
Exam traps, collected
References
- [1]Stanojevic S, Kaminsky DA, Miller MR, et al. ERS/ATS technical standard on interpretive strategies for routine lung function tests Eur Respir J, 2022.PMID 34949706
- [2]Graham BL, Steenbruggen I, Miller MR, et al. Standardization of Spirometry 2019 Update. An Official American Thoracic Society and European Respiratory Society Technical Statement Am J Respir Crit Care Med, 2019.PMID 31613151
- [3]Pellegrino R, Viegi G, Brusasco V, et al. Interpretative strategies for lung function tests Eur Respir J, 2005.PMID 16264058
- [4]Graham BL, Brusasco V, Burgos F, et al. 2017 ERS/ATS standards for single-breath carbon monoxide uptake in the lung Eur Respir J, 2017.PMID 28049168
- [5]Wanger J, Clausen JL, Coates A, et al. Standardisation of the measurement of lung volumes Eur Respir J, 2005.PMID 16135736
- [6]Coates AL, Wanger J, Cockcroft DW, et al. ERS technical standard on bronchial challenge testing: general considerations and performance of methacholine challenge tests Eur Respir J, 2017.PMID 28461290
- [7]Crapo RO, Casaburi R, Coates AL, et al. Guidelines for methacholine and exercise challenge testing-1999. This official statement of the American Thoracic Society was adopted by the ATS Board of Directors, July 1999 Am J Respir Crit Care Med, 2000.PMID 10619836
- [8]Miller RD, Hyatt RE. Evaluation of obstructing lesions of the trachea and larynx by flow-volume loops Am Rev Respir Dis, 1973.PMID 4745245
- [9]Du Rand IA, Blaikley J, Booton R, et al. British Thoracic Society guideline for diagnostic flexible bronchoscopy in adults: accredited by NICE Thorax, 2013.PMID 23860341
- [10]Yasufuku K, Pierre A, Darling G, et al. A prospective controlled trial of endobronchial ultrasound-guided transbronchial needle aspiration compared with mediastinoscopy for mediastinal lymph node staging of lung cancer J Thorac Cardiovasc Surg, 2011.PMID 21963329
- [11]von Bartheld MB, Dekkers OM, Szlubowski A, et al. Endosonography vs conventional bronchoscopy for the diagnosis of sarcoidosis: the GRANULOMA randomized clinical trial JAMA, 2013.PMID 23780458
- [12]Folch EE, Pritchett MA, Nead MA, et al. Electromagnetic Navigation Bronchoscopy for Peripheral Pulmonary Lesions: One-Year Results of the Prospective, Multicenter NAVIGATE Study J Thorac Oncol, 2019.PMID 30476574
- [13]Light RW, Macgregor MI, Luchsinger PC, Ball WC Jr. Pleural effusions: the diagnostic separation of transudates and exudates Ann Intern Med, 1972.PMID 4642731
- [14]Heffner JE, Brown LK, Barbieri CA. Diagnostic value of tests that discriminate between exudative and transudative pleural effusions. Primary Study Investigators Chest, 1997.PMID 9106577
- [15]Romero-Candeira S, Hernandez L, Romero-Brufao S, et al. Influence of diuretics on the concentration of proteins and other components of pleural transudates in patients with heart failure Am J Med, 2001.PMID 11403751
- [16]Heffner JE, Brown LK, Barbieri C, DeLeo JM. Pleural fluid chemical analysis in parapneumonic effusions. A meta-analysis Am J Respir Crit Care Med, 1995.PMID 7767510
- [17]Metintas M, Ak G, Dundar E, et al. Medical thoracoscopy vs CT scan-guided Abrams pleural needle biopsy for diagnosis of patients with pleural effusions: a randomized, controlled trial Chest, 2010.PMID 20154079
- [18]Havelock T, Teoh R, Laws D, Gleeson F. Pleural procedures and thoracic ultrasound: British Thoracic Society Pleural Disease Guideline 2010 Thorax, 2010.PMID 20696688