Phys · respiratory
Solitary Pulmonary Nodule
Also known as SPN · pulmonary nodule · lung nodule · coin lesion · incidental pulmonary nodule · ground-glass nodule · GGN · subsolid nodule · part-solid nodule · Fleischner nodule
Consultant-physician-depth guide to the solitary pulmonary nodule — the old-imaging-first principle, CT features that shift malignancy probability, subsolid nodule rules, Fleischner 2017 surveillance tables, Brock and Mayo risk models, the real limits of PET-CT, biopsy route selection (bronchoscopic, CT-guided, surgical) and the surveillance-plan conversation — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Solitary Pulmonary Nodule

The answer first
A solitary pulmonary nodule is a probability problem wearing a radiology report, and the whole discipline of this topic is converting a circle on a CT into a defensible malignancy probability and then acting on that number [1] [3]. The examiners are not testing whether you can recite a table; they are testing whether you know which framework applies to this patient — because the single commonest error in the DWE is quoting the right guideline for the wrong person [1].
Three working rules carry almost every answer [1] [2]:
- Find the old imaging before you do anything else. A solid nodule unchanged for two years is effectively benign, and growth on serial imaging overrides every reassuring static feature — the cheapest, highest-yield step in the entire workup costs nothing [1].
- Stratify risk with a number, not a vibe. Patient factors (age, smoking, emphysema, family history) and nodule factors (size — the dominant variable, spiculation, upper-lobe location, part-solid morphology, growth) combine into a malignancy probability through the Brock or Mayo model, and the probability band chooses surveillance, PET or tissue [2] [3].
- Subsolid nodules run on a different clock. A persistent part-solid nodule is the highest-risk morphology, its solid component — not its overall diameter — drives management, and its surveillance tail is five years, not two [1] [11].
What a solitary pulmonary nodule actually is
The definition is examinable to the millimetre: a rounded opacity up to 30 mm in diameter, completely surrounded by aerated lung, without associated atelectasis, hilar enlargement or pleural effusion [1] [18]. Anything larger is by definition a pulmonary mass — and masses carry a malignancy probability so high that the surveillance framework no longer applies; they enter the lung-cancer pathway directly [18].
The first classification happens at the workstation, not the bedside, and it splits every nodule into one of three morphologies [1]:
- Solid — soft-tissue density that obscures the underlying lung architecture; the morphology every size-threshold table was built around [1].
- Pure ground-glass (nonsolid) — hazy increased density through which vessels and bronchi remain visible; the slow-moving adenocarcinoma-spectrum morphology [11] [19].
- Part-solid — ground-glass with a solid core; the highest-risk morphology per millimetre, managed by the size of its solid component [11].
The differential the examiner wants to hear spans both shelves of the benign–malignant divide [18]:
| Shelf | Causes | Signature clue |
|---|---|---|
| Benign | Granuloma (healed histoplasmosis, TB), hamartoma, intrapulmonary lymph node, arteriovenous malformation, rounded atelectasis, resolving infection or infarct | Benign calcification pattern, macroscopic fat, feeding and draining vessels, subpleural triangular shape, documented stability [18] |
| Malignant | Adenocarcinoma and its spectrum (atypical adenomatous hyperplasia, adenocarcinoma in situ, minimally invasive adenocarcinoma), squamous cell carcinoma, carcinoid, solitary metastasis, lymphoma | Spiculation, lobulation, growth, part-solid morphology, upper-lobe location in a smoker [2] [11] |
How likely is any given nodule to be cancer? In population and screening series the large majority of small incidentally detected nodules are benign — in the NELSON volumetry data, nodules below 100 cubic millimetres carried a lung-cancer probability under 1%, while probability climbed steeply with size and volume doubling time [14]. That asymmetry — most nodules are benign, but the malignant ones are curable exactly at this stage — is the entire economic and emotional logic of surveillance [1] [22].
The first move, always: find the old imaging
Before any risk model, any PET, any needle — compare with prior imaging [1]. This is the highest-yield zero-cost step in the whole topic, and skipping it is a recurring exam trap and real-world harm.
The reasoning is temporal, not morphological. Malignant nodules grow; benign scars do not. A solid nodule unchanged over two years has a malignancy probability low enough that Fleischner treats it as benign and discharges it [1]. The biology behind that threshold is volume doubling time: most malignant solid nodules double in roughly 20 to 400 days, so two clean years of stability sits far outside malignant behaviour — with the critical exception of the adenocarcinoma-spectrum subsolid lesions, which can double over years and are exactly the nodules the two-year rule was never designed for [12] [19].
The converse matters more: demonstrated growth overrides every reassuring static feature. A smoothly marginated 8 mm nodule that was 5 mm last year is more dangerous than a spiculated 8 mm nodule unchanged for a decade — growth is the loudest single signal a nodule can send, and it routes the patient out of surveillance into tissue [1] [14].
Practically, growth is judged more sensitively by volume than by diameter. A 25% volume increase corresponds to a barely perceptible diameter change, and volumetry-based protocols (NELSON, and the British Thoracic Society guideline) exploit exactly this: they define growth as a volume rise of about 25% or more and use volume doubling time bands to decide escalation [5] [14].
Reading the CT: features that shift probability
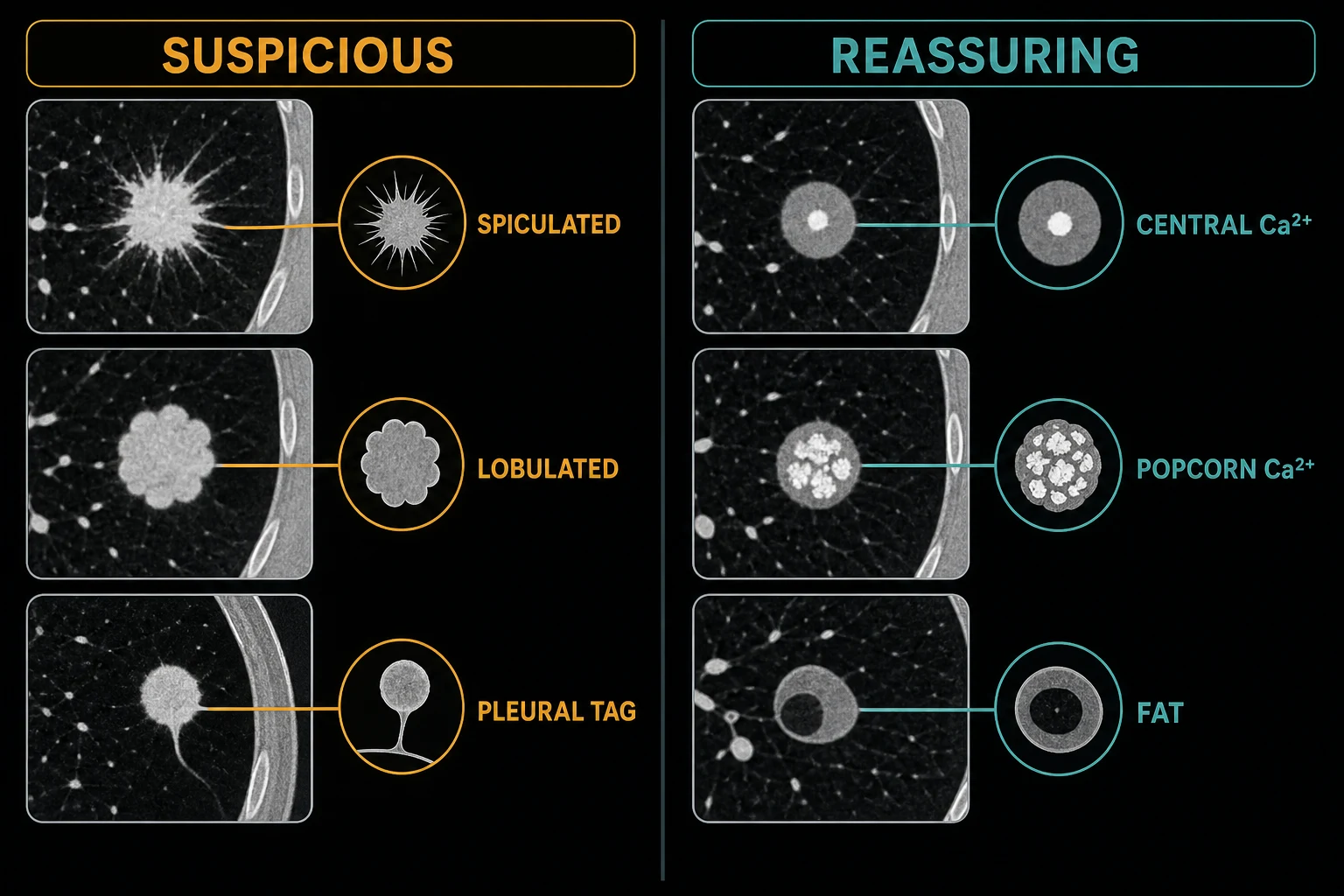
Once the temporal question is settled, morphology sets the prior. The features below are not decorative — several are actual variables in the validated risk models, and the examiner expects you to say which direction each pushes the probability [2] [3].
| Feature | Direction | Why |
|---|---|---|
| Size | Dominant malignant predictor — probability climbs steeply with every millimetre band | The single strongest variable in every model; a nodule above 8 mm is a different clinical object from one below 6 mm [1] [2] |
| Spiculation | Strongly malignant | Radial strands of tumour or desmoplasia into surrounding lung; the highest-odds morphological feature in the Mayo model [3] |
| Lobulation | Malignant-leaning | Differential growth rates across the nodule surface |
| Air bronchograms / bubble lucencies | Malignant-leaning (adenocarcinoma) | Tumour grows around, not through, airways — a classic lepidic signature [11] |
| Pleural tag / vessel convergence | Malignant-leaning | Desmoplastic tethering to pleura; vessels drawn into the lesion |
| Upper-lobe location | Malignant-leaning | A model variable in both Mayo and Brock — carcinogens deposit apically [2] [3] |
| Cavitation | Context-dependent | Thick, irregular, nodular walls favour malignancy; thin smooth walls favour benignity |
| Central, diffuse, laminated or popcorn calcification | Strongly benign | Healed granuloma (central/diffuse/laminated) or chondroid hamartoma (popcorn) — but eccentric or stippled calcification can occur inside cancers, so the pattern, not the presence, is what reassures [18] |
| Macroscopic fat | Diagnostic of hamartoma | Fat density inside the nodule on thin-section CT is effectively pathognomonic [18] |
| Feeding artery and draining vein | Diagnostic of AVM | Vascular malformation, not a nodule — embolisation territory, and a biopsy you must never do |
| Subpleural, triangular or oval, below a fissure | Benign-leaning | The morphology of an intrapulmonary lymph node [1] |
| Ground-glass or part-solid morphology | Adenocarcinoma spectrum | See the subsolid section — a different disease tempo entirely [11] |
Two honest caveats belong in the consultant answer. First, individual features shift probability; none, except fat, a benign calcification pattern and long-term stability, settles it alone — the models exist precisely because single signs mislead [2] [3]. Second, measurement technique is a feature in itself: small nodules should be measured on thin-section CT, and a part-solid nodule's solid component should be measured on the images where it is best defined — because the management of a part-solid nodule hangs on that single number [1].
Growth and volume doubling time: the tempo of the thing
Volume doubling time (VDT) is the quantitative spine of nodule follow-up, and its bands are worth memorising as behaviour, not just numbers [12] [14]:
- Doubling faster than about 20–30 days — too fast for carcinoma; think infection, inflammation or infarction.
- Doubling in roughly 20 to 400 days — the classic malignant window for solid nodules; Hasegawa's screening series measured the tempo of small screen-detected cancers and grounded this range [12].
- Doubling slower than about 400–600 days — the territory of indolent adenocarcinoma-spectrum lesions, especially ground-glass; NELSON treated a VDT beyond 600 days as reassuring, 400–600 as indeterminate, and faster as positive [14].
The histology maps to the tempo: squamous and small-cell cancers sit at the fast end, invasive adenocarcinoma in the middle, and lepidic-predominant or ground-glass adenocarcinomas at the very slow end — some pure ground-glass lesions take years to declare themselves, which is the biological reason subsolid surveillance runs for five years rather than two [12] [19].
Subsolid nodules: the different clock
Subsolid nodules are the examiner's favourite way to separate candidates who have read Fleischner from candidates who have memorised one table. The I-ELCAP analysis established the hierarchy that still frames everything: among screen-detected nodules, the frequency of malignancy was highest for part-solid lesions (63%), intermediate for pure nonsolid (18%) and lowest for solid (7%) — part-solid morphology is a risk factor in its own right, independent of size [11].
Pure ground-glass nodules are the adenocarcinoma spectrum's slow lane — atypical adenomatous hyperplasia and adenocarcinoma in situ at the indolent end, minimally invasive and lepidic-predominant adenocarcinoma as they enlarge [11]. Two management consequences follow. First, many are transient — inflammation and focal haemorrhage mimic ground-glass, so a short-interval CT (around 6–12 months for a persistent-looking lesion) exists largely to let transient opacities disappear [1]. Second, the ones that persist behave slowly: Kakinuma's long follow-up of pure ground-glass opacities showed that a substantial minority enlarge or develop a solid component only after years of apparent stability — the direct evidence behind the five-year surveillance tail [19].
Part-solid nodules are managed by the solid component, full stop. The overall diameter matters less than the invasive core: a 14 mm part-solid nodule with a 3 mm solid component is a surveillance problem, while a 12 mm nodule with a 7 mm solid component is a biopsy-and-resection problem [1] [11]. Fleischner operationalises this: a persistent part-solid nodule 6 mm or larger gets a short-interval CT at 3–6 months; if the solid component stays below 6 mm, annual CT for five years; a solid component of 6 mm or more flags the nodule as highly suspicious and routes it to PET, biopsy or resection [1].
Surveillance: the Fleischner 2017 tables
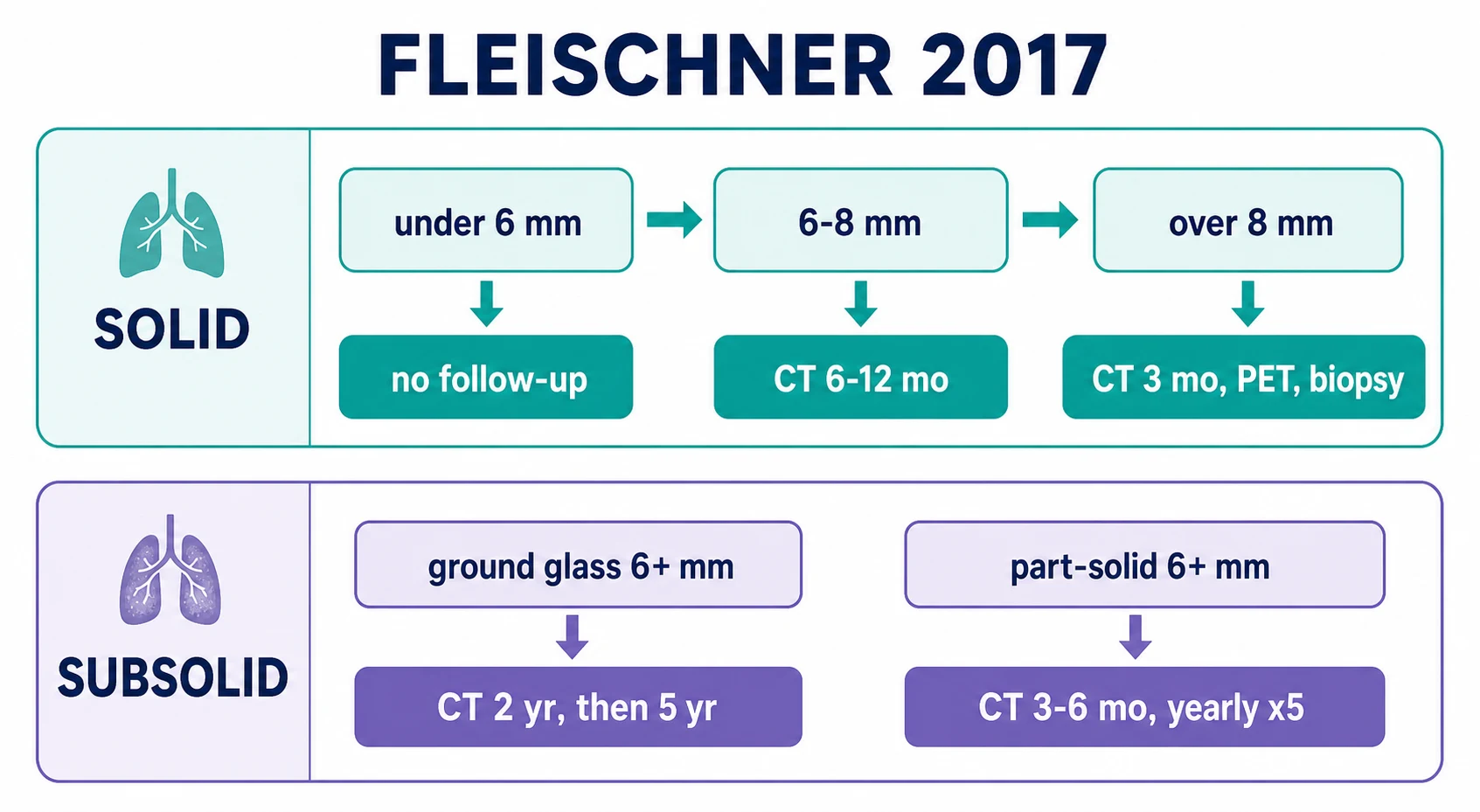
Fleischner 2017 is the incidental-nodule operating system, and the DWE expects the intervals cold — but only ever quoted together with who the tables are for: adults 35 or older, with nodules found incidentally, who are not known-cancer patients, not immunosuppressed, and not in a screening programme [1].
Single solid nodules — intervals by size band and risk category [1]:
| Size | Low-risk patient | High-risk patient |
|---|---|---|
| Under 6 mm (under 100 cubic mm) | No routine follow-up | Optional CT at 12 months [1] |
| 6–8 mm | CT at 6–12 months, then consider CT at 18–24 months | CT at 6–12 months, then CT at 18–24 months [1] |
| Above 8 mm | Consider CT at 3 months, PET/CT or tissue sampling — same options, chosen by risk | Same options, with a lower threshold for PET and tissue [1] |
Single subsolid nodules — the five-year tail is the point [1]:
| Morphology and size | Recommendation |
|---|---|
| Pure ground-glass under 6 mm | No routine follow-up (CT at 2 and 4 years only for suspicious morphology close to 6 mm) [1] |
| Pure ground-glass 6 mm or larger | CT at 6–12 months to confirm persistence, then CT every 2 years for 5 years [1] |
| Part-solid under 6 mm | No routine follow-up |
| Part-solid 6 mm or larger | CT at 3–6 months; if persistent with solid component under 6 mm, annual CT for 5 years; solid component 6 mm or more is highly suspicious — PET, biopsy or resection [1] |
The British Thoracic Society 2015 guideline is the alternative framework worth naming: it stratifies nodules 8 mm or larger with the Brock model, routes Brock probability of 10% or more toward PET-CT (with the Herder model layered on the PET result), prefers volumetry over diameter for follow-up, and discharges solid nodules after a year of volumetric stability — a meaningfully different grammar from Fleischner that examiners accept as equally correct [5].
And for completeness: Lung-RADS governs screening-detected nodules in the United States — validated retrospectively on NLST data, where applying it cut the false-positive rate substantially compared with the raw NLST positivity criteria, at the cost of a small sensitivity trade-off [10]. Mention it whenever the vignette says "screening CT", and never apply Fleischner there.
Risk models: putting a number on it
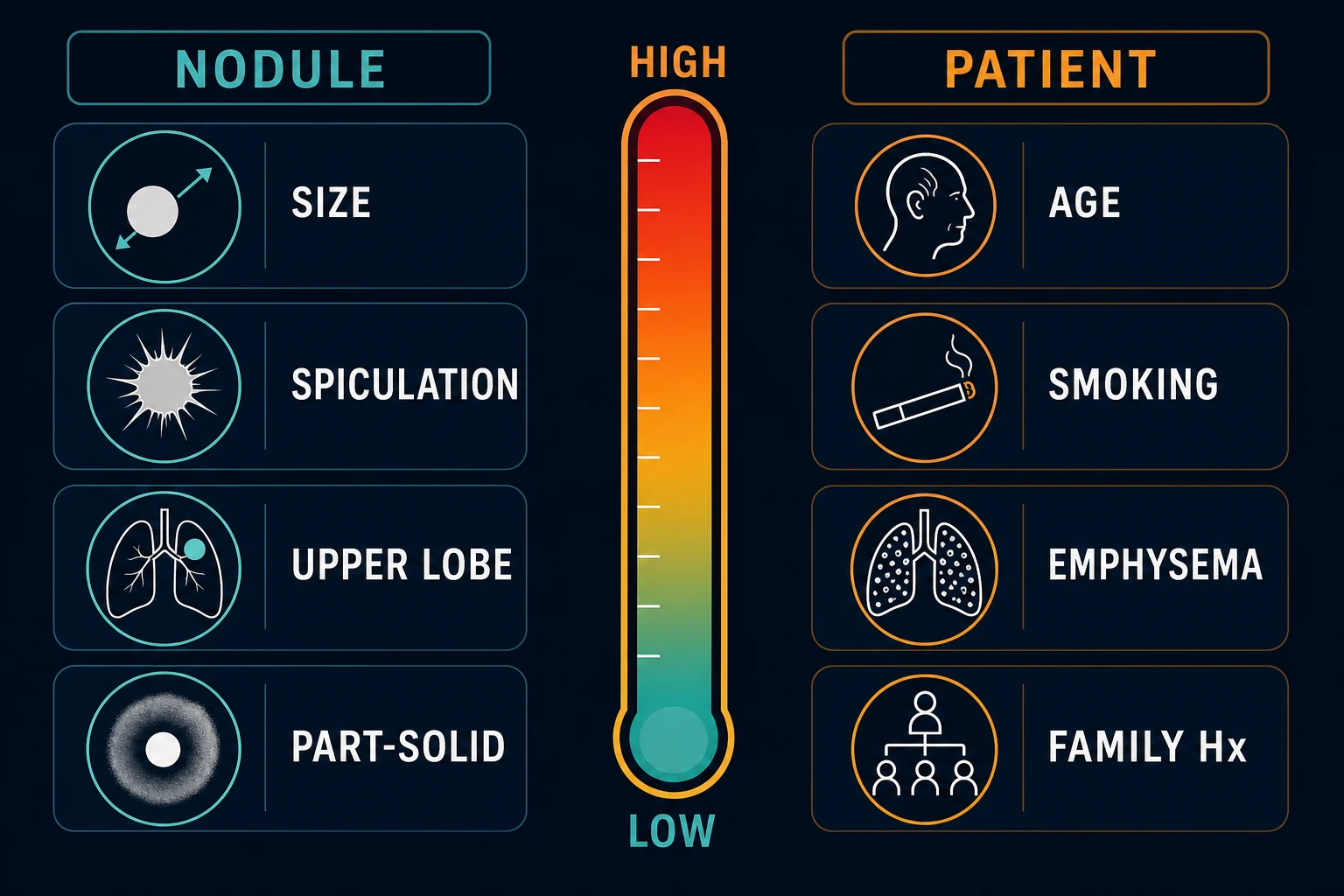
Gestalt underestimates and overestimates nodules with impressive consistency, which is why the validated models are examinable by name and by variable list [2] [3].
| Model | Origin | Variables | When it shines |
|---|---|---|---|
| Mayo (1997) | Retrospective cohort of resected nodules | Age, smoking (and years quit), prior extrathoracic cancer, size, upper-lobe location, spiculation [3] | The historical anchor; still quoted, and the substrate the Herder PET model builds on [15] |
| Brock / PanCan (2013) | Pan-Canadian screening cohorts, validated in British Columbia data | Age, sex, family history of lung cancer, emphysema, size, nodule type (solid, part-solid, nonsolid), upper lobe, spiculation, nodule count [2] | The current favourite — validated in screening and incidental cohorts, captures part-solid morphology and emphysema, and is the model BTS 2015 embeds in its pathway [2] [5] |
| Herder (2005) | Mayo model plus FDG-PET result | Mayo variables plus semiquantitative PET avidity [15] | After the PET, when a pre-test probability needs updating by the scan's metabolic answer |
The working bands a consultant carries: low probability (roughly under 5–10%) earns surveillance; intermediate (about 10–70%) is the PET-CT and biopsy band; high (above about 70%) heads for tissue or, in a fit patient with a typical lesion, straight to resection [5] [15]. The models do not replace judgement — they discipline it, and in the viva saying "I would calculate a Brock probability" is always a better answer than "it looks suspicious to me" [2].
Risk stratification in one row
PET-CT: powerful, with edges
FDG-PET is the intermediate band's referee, and its numbers are worth quoting with their limits attached. The Gould meta-analysis put sensitivity at about 97% and specificity at about 78% for characterising focal pulmonary lesions — excellent, and calibrated mostly on lesions at the larger end of the nodule range [4].
The limits are exactly where the DWE lives [4] [15]:
- Small nodules. Spatial resolution and partial-volume effects erode sensitivity below about 8–10 mm — a PET-negative 7 mm nodule is uninformative, not reassuring [4].
- Ground-glass and indolent adenocarcinoma. Low metabolic activity makes subsolid lesions and adenocarcinoma in situ routinely PET-cold; PET is close to useless for a pure ground-glass nodule [4] [11].
- Carcinoid and low-grade tumours. Classically under-avid.
- Granuloma-endemic regions. Histoplasmosis, tuberculosis and other inflammatory granulomas are PET-hot — specificity collapses where these are common, which is why a positive PET is a biopsy indication, not a cancer diagnosis [4].
The correct exam posture: PET revises probability, it does not replace it. The Herder model formalises this — Mayo pre-test probability plus the PET result yields a post-test probability that then chooses biopsy or surveillance — and a negative PET in a small or subsolid nodule never closes the case; surveillance continues on the nodule's own terms [15] [1].
Tissue: choosing the biopsy route
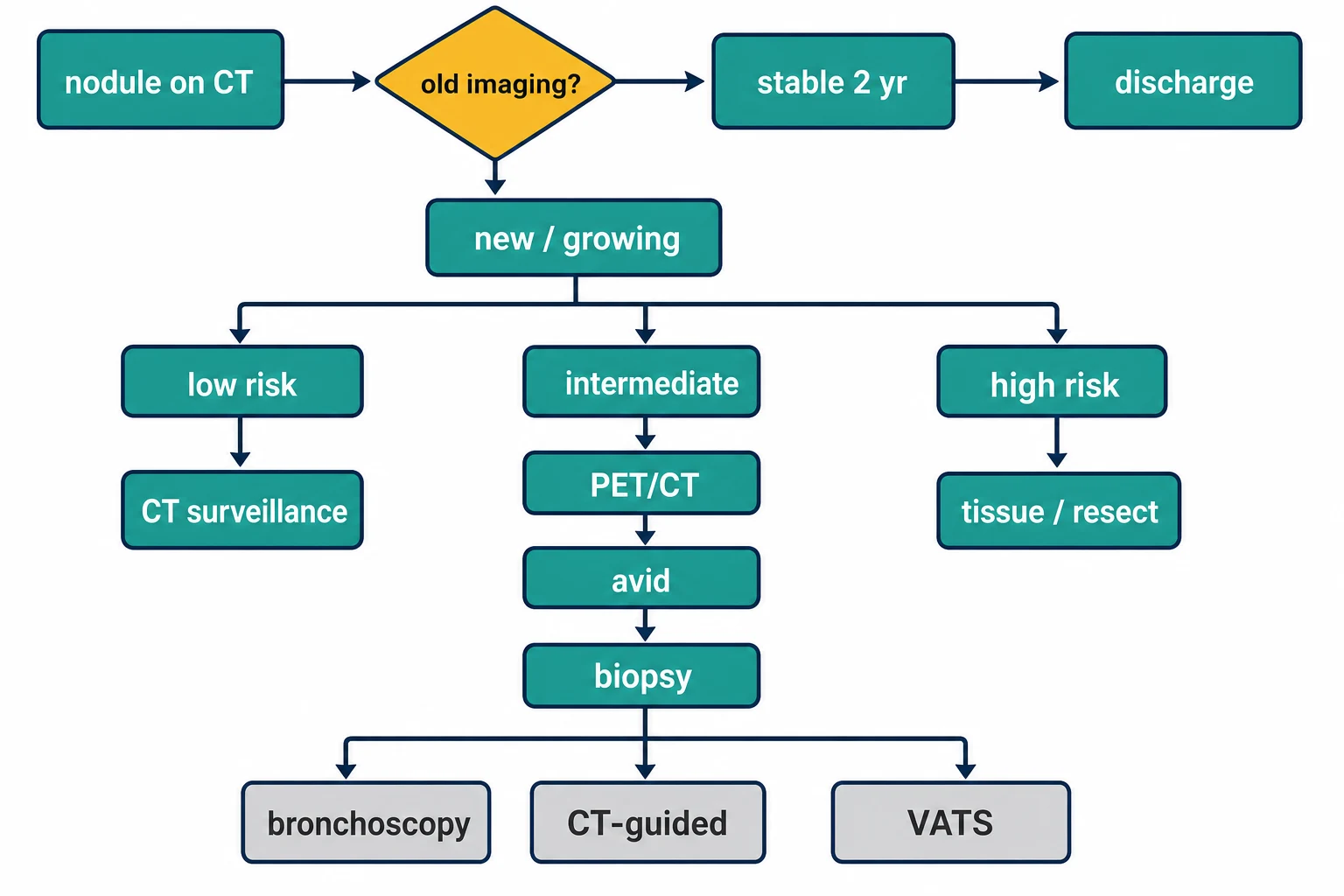
When probability says tissue, the route is chosen by location, risk, fitness and what else the procedure can stage — and each route has one number the examiner wants attached to it [5].
| Route | Best for | The number to quote |
|---|---|---|
| CT-guided transthoracic biopsy | Accessible peripheral and pleural-based nodules; patients who can cooperate with breath-holding | Diagnostic accuracy around 90%; pneumothorax in roughly one in five to one in four procedures, with a chest drain in about 5–7%; population data show older, emphysematous patients carry the higher complication burden [6] [7] |
| Navigational bronchoscopy (electromagnetic navigation) | Peripheral nodules with a bronchus sign; emphysema patients in whom a transthoracic needle is dangerous | NAVIGATE: diagnostic yield about 73% at 12 months with pneumothorax in only a few percent — the yield-for-safety trade that defines it [8] |
| Radial EBUS bronchoscopy | Peripheral lesions the bronchoscope can be steered into, confirmed by the ultrasound probe's concentric signal | Pooled sensitivity about 73% for peripheral lung cancer with a pneumothorax rate near 1% [9] |
| Surgical biopsy — VATS wedge with frozen section | High-probability nodules in fit patients, deeply seated lesions needles cannot safely reach, and nodules that have failed percutaneous and bronchoscopic attempts | Diagnosis and potential cure in one anaesthetic — the wedge confirms, and the resection follows in the same sitting if malignant |
| Resection as the first tissue | The classic high-probability, fit-patient, peripheral lesion | JCOG0802 supports segmentectomy as oncologically sound for small peripheral tumours up to 2 cm — the modern default when a diagnostic wedge becomes a curative operation [13] |
Two selection heuristics earn marks. Emphysema tilts toward the bronchoscope: CT-guided pneumothorax risk climbs with emphysema and smaller, deeper targets, so a severe-COPD patient with a bronchus-sign nodule is a navigational or radial-EBUS case [6] [8]. Probability tilts toward the knife: when the Brock estimate is high, the nodule is peripheral, and the patient is operable, sending them for a needle that will only confirm what everyone believes costs time and a pneumothorax — the MDT answer is often diagnostic-therapeutic VATS [5] [13].
And the safety line that must never blur: a vascular lesion is not biopsied. A nodule with a feeding artery and draining vein is an AVM; the biopsy of that lesion is a catastrophe, which is why contrast enhancement characteristics belong in the pre-biopsy checklist [18].
Who decides: the nodule MDT and when to refer
No nodule above 8 mm, no part-solid nodule with a growing or 6-mm-plus solid component, no discordant PET, and no biopsy decision should be a solo act — the lung nodule or lung cancer multidisciplinary meeting (respiratory physician, radiologist, thoracic surgeon, oncologist, pathologist, nurse coordinator) exists precisely because the surveillance–PET–needle–knife trade-offs are exactly the decisions committees make better than individuals [5].
Referral triggers worth listing in the exam: any solid nodule above 8 mm; any nodule with suspicious morphology at any size; any demonstrated growth; any part-solid nodule 6 mm or larger; any nodule in a patient with haemoptysis, weight loss or prior malignancy; and any surveillance nodule whose patient is too anxious to live with watchful waiting — distress is itself an indication to escalate the conversation, sometimes to a definitive procedure [1] [5].
The useful referral contains the things that change the decision: prior imaging or a statement that none exists, smoking and occupational history, cardiorespiratory fitness and comorbidity, anticoagulation and antiplatelet status (it shapes biopsy choice), and what the patient has been told and fears [5].
Emerging tools: biomarkers and AI — adjuncts, not verdicts
Two developments deserve a brief, guideline-anchored mention because examiners increasingly ask "what's new" [16] [17].
Blood biomarkers. The PANOPTIC trial tested a plasma proteomic classifier (two proteins integrated with clinical risk factors) on indeterminate nodules 8–30 mm with low-to-intermediate pre-test probability: the integrated classifier reached a negative predictive value of about 98% in the intended-use cohort — a genuine down-classification tool, though still an adjunct that must slot into, not bypass, the surveillance framework [16].
Artificial intelligence. Deep-learning models applied to low-dose CT have matched or exceeded radiologist performance for cancer detection in retrospective screening datasets — Ardila's three-dimensional system is the landmark proof of concept — and AI tools are beginning to standardise volumetry, flag growth and triage worklists [17]. The consultant framing: promising for consistency and workflow, validated retrospectively, and not yet a replacement for the guideline pathways that govern what actually happens to the patient [1] [17].
Screening context: where nodules come from
Most SPN conversations eventually touch screening, so the anchors belong in this topic even though screening is not surveillance [22] [21]. NLST showed a 20% relative reduction in lung-cancer mortality with annual low-dose CT versus chest X-ray in heavy smokers — and a very high nodule-detection rate whose false-positive tail is exactly what nodule-management protocols exist to tame [22]. NELSON confirmed the mortality benefit with volumetric management and demonstrated that volume-based protocols cut false positives dramatically [21] [14]. USPSTF 2021 recommends annual LDCT for adults 50–80 with at least a 20 pack-year history who smoke or quit within 15 years — and every screening answer ends with smoking cessation, the intervention that outperforms the scan [20].
The DCE angles
Long case — the nodule found while looking for something else. The classic DCE scenario is not a lung-cancer patient; it is a person whose abdominal CT, trauma scan or pre-operative work-up surfaced a nodule, sitting in clinic frightened. The marks live in the conversation: stating the probability plainly ("most small nodules are not cancer, and this is how we will be certain"), laying out the surveillance plan as a plan rather than a wait, naming the exit ramps (stability ends it; growth escalates it), and handling scanxiety — the dread that attaches to each follow-up scan — with scheduled reviews, clear contact routes and honest timelines [1]. Shared decision-making is the examinable skill: for a low-probability nodule, some patients choose a definitive procedure over years of surveillance, and some choose surveillance over a biopsy with a one-in-five pneumothorax risk — both are defensible when informed, and the examiner wants to hear you elicit the preference rather than impose the algorithm [5] [7]. Close with smoking cessation framed as the highest-yield intervention available, offered without judgement [20].
Short case — the data station. There is no examination short case for a 9 mm nodule; there is a data-interpretation station that hands you the CT report. The winning structure: read it aloud in categories (what, where, how big, what morphology, what comparison), state the single most important next step (find prior imaging), classify the nodule (solid versus subsolid, solid component if part-solid), name the applicable framework and whether this patient is eligible for it, give the Fleischner interval or the escalation, and finish with the MDT. Traps baked into the report: an age under 35, a line about known breast cancer, the words "part-solid, solid component 7 mm", or a comparison study the candidate fails to notice [1] [11].
Exam traps, collected
References
- [1]MacMahon H, Naidich DP, Goo JM, et al. Guidelines for Management of Incidental Pulmonary Nodules Detected on CT Images: From the Fleischner Society 2017 Radiology, 2017.PMID 28240562
- [2]McWilliams A, Tammemagi MC, Mayo JR, et al. Probability of cancer in pulmonary nodules detected on first screening CT N Engl J Med, 2013.PMID 24004118
- [3]Swensen SJ, Silverstein MD, Ilstrup DM, et al. The probability of malignancy in solitary pulmonary nodules. Application to small radiologically indeterminate nodules Arch Intern Med, 1997.PMID 9129544
- [4]Gould MK, Maclean CC, Kuschner WG, et al. Accuracy of positron emission tomography for diagnosis of pulmonary nodules and mass lesions: a meta-analysis JAMA, 2001.PMID 11180735
- [5]Callister ME, Baldwin DR, Akram AR, et al. British Thoracic Society guidelines for the investigation and management of pulmonary nodules Thorax, 2015.PMID 26082159
- [6]Wiener RS, Schwartz LM, Woloshin S, et al. Population-based risk for complications after transthoracic needle lung biopsy of a pulmonary nodule: an analysis of discharge records Ann Intern Med, 2011.PMID 21810706
- [7]Heerink WJ, de Bock GH, de Jonge GJ, et al. Complication rates of CT-guided transthoracic lung biopsy: meta-analysis Eur Radiol, 2017.PMID 27108299
- [8]Folch EE, Pritchett MA, Nead MA, et al. Electromagnetic Navigation Bronchoscopy for Peripheral Pulmonary Lesions: One-Year Results of the Prospective, Multicenter NAVIGATE Study J Thorac Oncol, 2019.PMID 30476574
- [9]Steinfort DP, Khor YH, Manser RL, et al. Radial probe endobronchial ultrasound for the diagnosis of peripheral lung cancer: systematic review and meta-analysis Eur Respir J, 2011.PMID 20693253
- [10]Pinsky PF, Gierada DS, Black W, et al. Performance of Lung-RADS in the National Lung Screening Trial: a retrospective assessment Ann Intern Med, 2015.PMID 25664444
- [11]Henschke CI, Yankelevitz DF, Mirtcheva R, et al. CT screening for lung cancer: frequency and significance of part-solid and nonsolid nodules AJR Am J Roentgenol, 2002.PMID 11959700
- [12]Hasegawa M, Sone S, Takashima S, et al. Growth rate of small lung cancers detected on mass CT screening Br J Radiol, 2000.PMID 11205667
- [13]Saji H, Okada M, Tsuboi M, et al. Segmentectomy versus lobectomy in small-sized peripheral non-small-cell lung cancer (JCOG0802/WJOG4607L): a multicentre, open-label, phase 3, randomised, controlled, non-inferiority trial Lancet, 2022.PMID 35461558
- [14]Horeweg N, van Rosmalen J, Heuvelmans MA, et al. Lung cancer probability in patients with CT-detected pulmonary nodules: a prespecified analysis of data from the NELSON trial of low-dose CT screening Lancet Oncol, 2014.PMID 25282285
- [15]Herder GJ, van Tinteren H, Golding RP, et al. Clinical prediction model to characterize pulmonary nodules: validation and added value of 18F-fluorodeoxyglucose positron emission tomography Chest, 2005.PMID 16236914
- [16]Silvestri GA, Tanner NT, Kearney P, et al. Assessment of Plasma Proteomics Biomarker's Ability to Distinguish Benign From Malignant Lung Nodules: Results of the PANOPTIC (Pulmonary Nodule Plasma Proteomic Classifier) Trial Chest, 2018.PMID 29496499
- [17]Ardila D, Kiraly AP, Bharadwaj S, et al. End-to-end lung cancer screening with three-dimensional deep learning on low-dose chest computed tomography Nat Med, 2019.PMID 31110349
- [18]Khouri NF, Meziane MA, Zerhouni EA, et al. The solitary pulmonary nodule. Assessment, diagnosis, and management Chest, 1987.PMID 3792065
- [19]Kakinuma R, Ohmatsu H, Kaneko M, et al. Progression of focal pure ground-glass opacity detected by low-dose helical computed tomography screening for lung cancer J Comput Assist Tomogr, 2004.PMID 14716227
- [20]US Preventive Services Task Force Screening for Lung Cancer: US Preventive Services Task Force Recommendation Statement JAMA, 2021.PMID 33687470
- [21]de Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial N Engl J Med, 2020.PMID 31995683
- [22]National Lung Screening Trial Research Team Reduced lung-cancer mortality with low-dose computed tomographic screening N Engl J Med, 2011.PMID 21714641