Phys · rheumatological
Fibromyalgia and Chronic Widespread Pain
Also known as fibromyalgia · fibromyalgia syndrome · chronic widespread pain · central sensitisation syndrome · central pain amplification · fibrositis (obsolete)
Consultant-physician-depth guide to fibromyalgia and chronic widespread pain — central sensitisation pathophysiology (amplified CNS pain processing, deficient descending inhibition, the neurotransmitter profile), chronic widespread musculoskeletal pain with fatigue, sleep disturbance and cognitive dysfunction, the cluster of central sensitivity syndromes, the 2016 ACR diagnostic criteria (WPI and SSS, abolition of tender points), the distinction from inflammatory and endocrine mimics, the non-pharmacological-first management (exercise, CBT, sleep hygiene, pacing) with symptom-targeted pharmacotherapy (amitriptyline, duloxetine, pregabalin), the explicit avoidance of opioids and glucocorticoids, and the multidisciplinary approach — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Fibromyalgia and Chronic Widespread Pain

The one-minute consultant answer
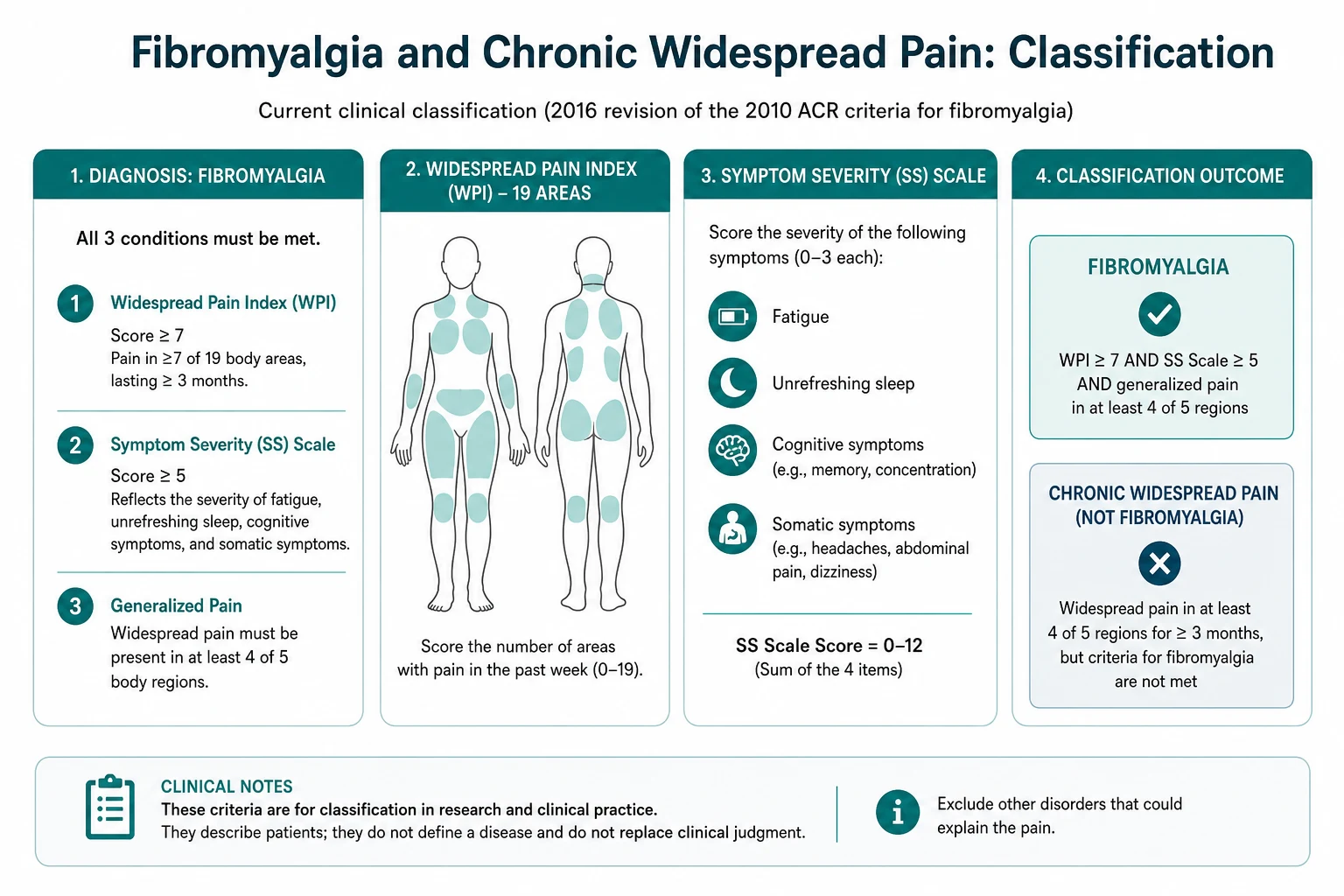
Fibromyalgia is a chronic central pain syndrome defined by widespread musculoskeletal pain lasting at least three months, accompanied by fatigue, non-restorative sleep disturbance, cognitive dysfunction (fibro fog) and somatic symptoms. The mechanism is central sensitisation — amplified processing of nociceptive input in the central nervous system, with deficient descending inhibition. It is NOT inflammatory, NOT autoimmune and NOT a disease of peripheral tissue damage [2]. The 2016 ACR revised criteria abolish the obsolete tender point examination and instead use the Widespread Pain Index (WPI) and the Symptom Severity Scale (SSS): WPI 7 or more with SSS 5 or more, OR WPI 4 to 6 with SSS 9 or more, with generalised pain (at least 4 of 5 body regions) for at least 3 months [1]. Normal inflammatory markers (CRP, ESR) with widespread pain is the single most important diagnostic clue. Management is non-pharmacological first — patient education and validation, graded aerobic exercise (the only EULAR strong-for recommendation), cognitive behavioural therapy, sleep hygiene and pacing [3][7] — with symptom-targeted pharmacotherapy (amitriptyline at night, duloxetine, pregabalin or gabapentin) as adjunct. Opioids, glucocorticoids and repeated invasive investigations are explicitly to be avoided.
Pathophysiology — why fibromyalgia does what it does
Understanding the neurobiology of central sensitisation is not optional. Every evidence-based treatment — exercise, CBT, tricyclics, SNRIs and gabapentinoids — targets a different limb of this mechanism. You cannot reason about the management, or about why the patient's inflammatory markers are normal, without it. [1]
Central sensitisation: the volume control is turned up
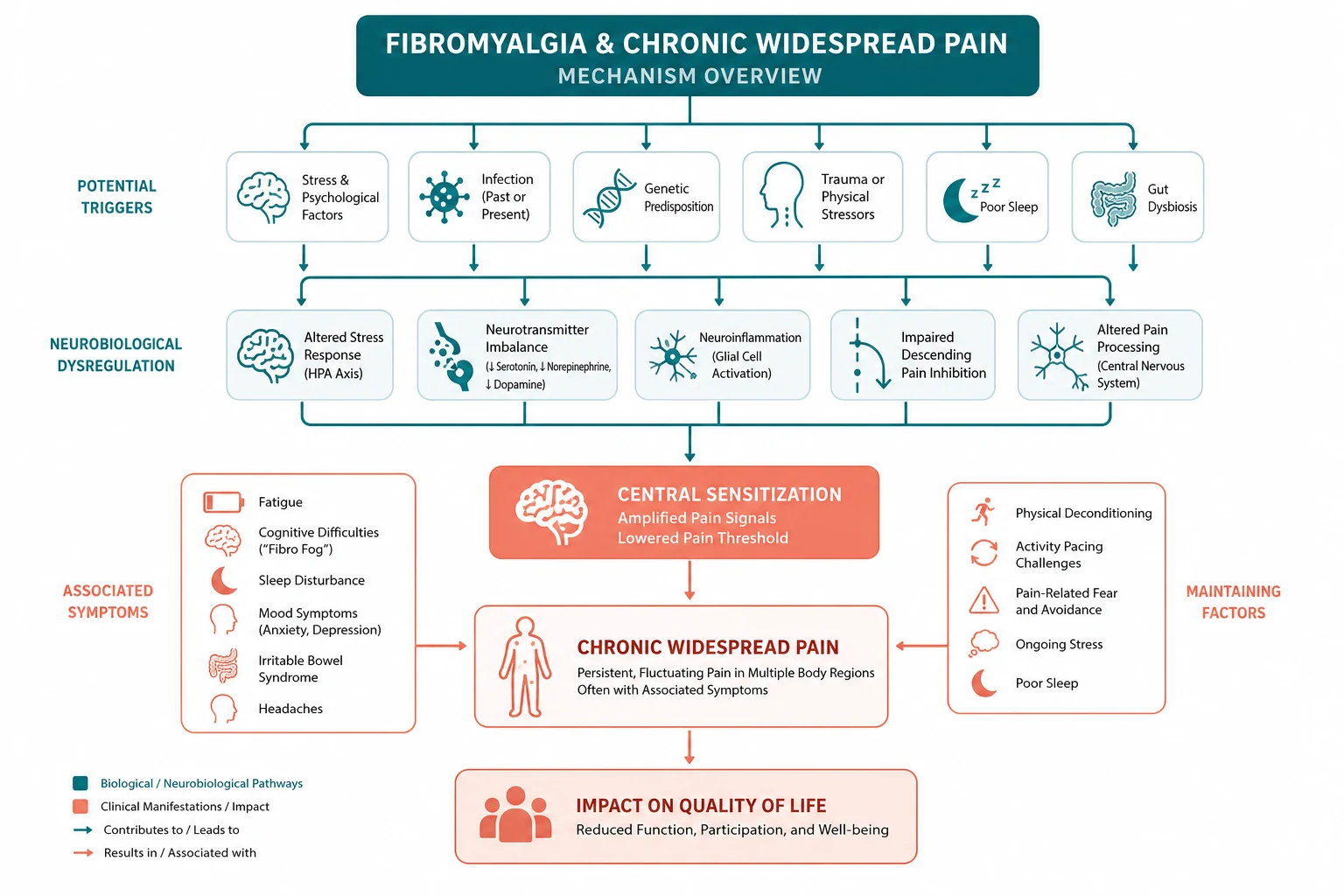
Fibromyalgia is a disorder of central pain processing. In health, a nociceptive stimulus of a given intensity produces a proportional pain experience. In fibromyalgia, the gain on the central pain system is amplified, so the same stimulus produces a disproportionately large pain experience — this is hyperalgesia. Furthermore, stimuli that are normally non-painful — light touch, a blood-pressure cuff, the pressure of clothing — are experienced as pain — this is allodynia [2].
Functional MRI studies provide objective evidence of this amplification: when fibromyalgia patients and healthy controls receive equal pressure stimuli to the thumbnail, the patients report more pain and show greater activation in the pain-processing regions of the brain (the insula, the secondary somatosensory cortex, the anterior cingulate). This is not imaginary. The brain is processing the signal differently. [1]
The clinical correlate is the quality of the pain. Patients describe widespread, deep, aching, migratory and fluctuating pain that worsens with stress, poor sleep and exertion. They often use bizarre descriptors — burning, stabbing, throbbing, electric — that should prompt the thought of central amplification rather than of a structural lesion. [1]
The failure of descending inhibition
The central nervous system does not merely receive nociceptive input passively. It has a descending inhibitory system — a network originating in the periaqueductal grey, relayed through the rostral ventromedial medulla and the dorsal horn, that uses serotonin and noradrenaline to suppress incoming nociceptive signals before they reach consciousness. This is the "diffuse noxious inhibitory control" or "conditioned pain modulation" system. [1]
In fibromyalgia, this descending inhibition is impaired. The experimental demonstration is the conditioned pain modulation test: a painful conditioning stimulus (immersion of the foot in cold water) normally suppresses the pain of a test stimulus elsewhere on the body, because the descending system is engaged. In fibromyalgia, this suppression is reduced or absent. The result is that nociceptive input that should be filtered out is instead amplified [2].
This is the mechanism that explains why tricyclic antidepressants (amitriptyline) and serotonin-noradrenaline reuptake inhibitors (duloxetine) work in fibromyalgia: they boost the deficient descending serotonergic and noradrenergic inhibition. It is not because the patient is depressed. The pain and the mood share a neurotransmitter substrate. [1]
The neurotransmitter profile
| Neurotransmitter | Level in fibromyalgia | Role | Targeted by |
|---|---|---|---|
| Serotonin | Reduced | Descending inhibition, mood, sleep | Amitriptyline, duloxetine |
| Noradrenaline | Reduced | Descending inhibition, arousal | Duloxetine, amitriptyline |
| Dopamine | Reduced | Reward processing, central pain modulation | (Indirectly, by exercise) |
| Substance P | Elevated (in CSF) | Excitatory neurotransmission, pain amplification | Pregabalin, gabapentin (reduce release) |
| Glutamate | Elevated (in insula on MR spectroscopy) | Excitatory neurotransmission | Pregabalin, gabapentin |
| Nerve growth factor | Elevated | Sensitisation of nociceptors | (Monoclonal antibodies under study) |
The treatment logic follows directly: the deficient inhibitory transmitters are boosted by tricyclics and SNRIs; the excess excitatory transmitters are dampened by gabapentinoids, which bind the alpha-2-delta subunit of the voltage-gated calcium channel and reduce the release of glutamate and substance P [5][6].
Why it is NOT inflammatory, NOT autoimmune, NOT tissue damage

This single fact drives the entire management logic: [1]
- Inflammatory markers are normal. CRP and ESR are within the reference range and remain so over months and years of symptoms. There is no acute-phase response.
- There is no synovitis. The joints are not swollen, warm or tender in an articular distribution. The tenderness is generalised and soft-tissue, not joint-line.
- Autoantibodies, when present, are incidental. ANA is positive in up to 15 per cent of the healthy population and does not diagnose SLE in a patient with fibromyalgia and no objective features of lupus. RF and anti-CCP are negative unless there is genuine comorbid rheumatoid arthritis.
- There is no muscle damage. CK is normal. Muscle biopsy, when performed historically, shows no myopathy.
- There is no structural lesion. Imaging of the painful regions is normal or shows incidental age-appropriate changes. [1]
The consequence: glucocorticoids have no role (the disease is not inflammatory), immunosuppression has no role (the disease is not autoimmune), and repeated investigations in search of a peripheral cause reinforce the illness belief without yielding a diagnosis. [1]
Epidemiology
Fibromyalgia has a prevalence of 2 to 8 per cent in the general population, depending on the criteria applied and the population surveyed — the 2016 criteria, which removed the tender point requirement, identify a broader population than the 1990 criteria [1].
| Feature | Detail |
|---|---|
| Prevalence | 2 to 8 per cent of the general population |
| Sex ratio | Female-predominant, approximately 7 to 9:1 in clinic populations, less skewed in community surveys |
| Peak age | 30 to 50 years at presentation, but the spectrum extends from adolescence to the elderly |
| Comorbid inflammatory disease | Rheumatoid arthritis 10 to 20 per cent; systemic lupus erythematosum; ankylosing spondylitis; Sjogren syndrome |
| Comorbid central sensitivity syndromes | Irritable bowel syndrome, chronic fatigue syndrome, tension-type headache, temporomandibular disorder, interstitial cystitis, multiple chemical sensitivity |
The female predominance is striking in tertiary care (where the most disabled patients are seen) but less marked in population-based studies, suggesting that ascertainment bias contributes — women are more likely to present, to be referred and to be labelled. Men with fibromyalgia are under-diagnosed. [1]
The comorbidity with inflammatory rheumatological disease is clinically critical. Secondary fibromyalgia — fibromyalgia occurring in a patient with established RA, SLE or ankylosing spondylitis — is the commonest cause of apparently refractory inflammatory disease. The fibromyalgia inflates the composite disease-activity scores (DAS28, SLEDAI, BASDAI) because these scores include a tender joint count and a patient global assessment, both of which are driven by the central sensitisation. The result is a patient whose inflammatory markers are quiet but whose disease-activity score is high — and the correct response is to recognise the fibromyalgia, not to escalate the immunosuppression. [1]
Clinical features — the full spectrum
The core symptom cluster
Fibromyalgia presents with a cluster of symptoms that, taken together, point to a central pain mechanism: [1]
- Chronic widespread pain — pain in the axial skeleton (neck, back, chest), above and below the waist, and on the left and right sides, for at least three months. The pain is deep, aching, migratory and fluctuating.
- Fatigue — profound, disproportionate to activity, and not relieved by rest.
- Sleep disturbance — non-restorative sleep is the hallmark. The patient sleeps but wakes unrefreshed. Polysomnography shows an alpha-delta sleep anomaly (alpha waves intruding into the slow-wave delta sleep), though this is not required for diagnosis.
- Cognitive dysfunction (fibro fog) — deficits in working memory, attention, verbal fluency and executive function. These are objectively demonstrable on neuropsychological testing and are a source of major distress and functional impairment.
- Somatic symptoms — headaches, irritable bowel symptoms (abdominal pain, bloating, altered bowel habit), bladder symptoms (frequency, urgency, pelvic pain), paresthaesias, dry eyes and dry mouth, and a heightened sensitivity to sensory stimuli (light, noise, smell). [1]
The central sensitivity syndromes
Fibromyalgia does not exist in isolation. It is the flagship of a cluster of central sensitivity syndromes — conditions that share the mechanism of central sensitisation and that co-occur far more often than chance: [1]
- Irritable bowel syndrome (IBS) — abdominal pain, bloating, altered bowel habit, no structural abnormality.
- Chronic fatigue syndrome (CFS / myalgic encephalomyelitis) — profound fatigue, post-exertional malaise, unrefreshing sleep, cognitive dysfunction.
- Tension-type headaches — bilateral, pressing, band-like, no migraine features.
- Temporomandibular disorder (TMD) — jaw pain, facial pain, limited mouth opening.
- Interstitial cystitis / painful bladder syndrome — bladder pain, urgency, frequency, sterile urine.
- Multiple chemical sensitivity — symptoms on exposure to low levels of environmental chemicals.
- Vulvodynia, endometriosis-associated pain, chronic pelvic pain — pelvic pain syndromes. [1]
The clinical point: a patient who presents with several of these has a central sensitisation syndrome, and the management principle is the same — validate the symptoms, address the central mechanism, avoid the pursuit of a peripheral lesion in each organ system. [1]
The atypical presentations
Older-onset fibromyalgia (onset above 60) is commonly confused with polymyalgia rheumatica. The discriminator is the inflammatory marker: PMR has a markedly raised ESR and CRP (typically above 40) and a dramatic rapid response to prednisolone 15 mg; fibromyalgia has normal markers and no response to prednisolone. [1]
Male fibromyalgia is under-diagnosed. Men present with less tender-point burden and are more likely to be labelled with "chronic pain syndrome" or to be investigated extensively for an occult malignancy before the central mechanism is recognised. [1]
Fibromyalgia with comorbid inflammatory disease (secondary fibromyalgia) presents as worsening pain and fatigue in a patient whose inflammatory disease has been well controlled. The inflammatory markers are normal, the synovitis is absent, and the composite activity score (DAS28, SLEDAI) is elevated by the tender joint count and the patient global. [1]
Diagnosis — the 2016 ACR revised criteria

The 2016 revision of the ACR criteria (Wolfe 2016) abolished the tender point examination and replaced it with two patient-reported scales [1]. The tender point count was not reproducible, required an examination that most non-rheumatologists did not perform reliably, and identified a narrower population than the condition actually affects.
The Widespread Pain Index (WPI)
The WPI counts the number of body areas in which the patient has felt pain in the past week, out of 19 predefined areas: [1]
- Left upper body (3): shoulder girdle, upper arm, lower arm
- Right upper body (3): shoulder girdle, upper arm, lower arm
- Left lower body (3): hip (buttock, trochanter), upper leg, lower leg
- Right lower body (3): hip (buttock, trochanter), upper leg, lower leg
- Axial skeleton (7): neck, upper back, lower back, chest, abdomen) [1]
Generalised pain is defined as pain in at least 4 of 5 body regions (the four limbs counted separately, plus the axial region). This requirement was added in 2016 to prevent the misclassification of regional pain syndromes (such as a frozen shoulder or a lumbar disc) as fibromyalgia. [1]
Maximum WPI score: 19. [1]
The Symptom Severity Scale (SSS)
The SSS scores the severity of three core symptoms (fatigue, waking unrefreshed, cognitive symptoms) on a 0 to 3 scale each (0 = none, 1 = mild, 2 = moderate, 3 = severe), plus the extent of somatic symptoms in general on a 0 to 3 scale. The maximum SSS score is 12. [1]
The diagnostic threshold
A diagnosis of fibromyalgia requires ALL of the following [1]:
-
Generalised pain — pain in at least 4 of 5 body regions.
-
Symptoms present at a similar level for at least 3 months.
-
Either:
- WPI 7 or more AND SSS 5 or more, OR
- WPI of 4 to 6 AND SSS 9 or more. [1]
-
The diagnosis is not excluded by the presence of another diagnosable illness. This was a key change: a patient with rheumatoid arthritis can also have fibromyalgia, and the diagnosis of one does not exclude the other. [1]
The diagnosis is clinical. It does not require any investigation to be positive — it requires the appropriate symptom pattern and the exclusion of mimics by the focused investigation screen. [1]
Why the tender point examination is obsolete
The 1990 ACR criteria required 11 of 18 tender points on digital palpation at a standardised pressure (approximately 4 kg per cm squared). These criteria are obsolete for three reasons: [1]
- The tender point count is not reproducible between examiners.
- The 18 points do not sample the body symmetrically or representatively.
- The criteria identified a narrower population than the condition actually affects — patients with fewer than 11 tender points but with the full symptom cluster were missed. [1]
Exam trap: A question stem that asks for "11 of 18 tender points" is using the 1990 criteria. The 2016 criteria use the WPI and the SSS. The correct answer is the 2016 criteria. [1]
The diagnosis of exclusion
Fibromyalgia is a diagnosis of exclusion in the sense that the focused investigation must exclude the mimics before the label is applied. The mimics to exclude: [1]
- Inflammatory arthritis (RA, spondyloarthritis, SLE) — synovitis, raised CRP or ESR, specific autoantibodies.
- Polymyalgia rheumatica — markedly raised ESR and CRP, shoulder and pelvic girdle stiffness, dramatic prednisolone response.
- Endocrine disease — hypothyroidism (check TSH and free T4), and less commonly hyperparathyroidism or Addison disease.
- Myopathy — polymyositis or dermatomyositis (proximal weakness, raised CK).
- Vitamin D deficiency and osteomalacia — diffuse bone and muscle pain, proximal weakness.
- Malignancy — weight loss, night sweats, a rising inflammatory marker, organ-specific symptoms.
- Drug-induced — statin-related myalgia (check CK), and opioid-induced hyperalgesia. [1]
Assessment
History
Take a structured history that maps to the symptom cluster and that screens for the mimics: [1]
- Pain distribution — ask the patient to shade a body diagram. The WPI is derived from this. Is the pain generalised (at least 4 of 5 regions)? Is it articular (joint-line) or non-articular (soft tissue)? Is it constant or fluctuating?
- Sleep quality — "Do you wake feeling refreshed?" Non-restorative sleep is the hallmark.
- Fatigue — "Is the fatigue worse than the pain?" In many patients it is the dominant symptom.
- Cognitive function — "Do you have trouble with memory, concentration or word-finding?" Fibro fog is a core symptom and a source of distress.
- Mood — screen for depression (PHQ-9) and anxiety (GAD-7). The comorbidity is high and bidirectional.
- Functional impact — "What can you not do now that you could do before?" Quantify the impact on work, family and self-care.
- Screening for central sensitivity syndromes — ask specifically about irritable bowel symptoms, headaches, jaw pain, bladder pain and chemical sensitivity.
- Screening for mimics — morning stiffness (inflammatory), weight loss or night sweats (malignancy), proximal weakness (myopathy), a single hot joint (sepsis). [1]
Examination
The examination in suspected fibromyalgia is performed to demonstrate generalised tenderness with no objective abnormality and to exclude the mimics. [1]
- Inspection — look for the absence of joint deformity, synovitis, effusion, muscle wasting or skin changes. The patient looks well, which is itself a discriminating feature from inflammatory disease.
- Palpation — palpate the joints for synovitis (bogginess, warmth, effusion) and find it absent. Palpate the soft tissues and find generalised tenderness — the patient hurts everywhere, which is the point. The tenderness is non-articular and reproducible across regions.
- Range of movement — active range of movement is preserved at all major joints, even though the patient reports pain. The discrepancy between full movement and reported pain is characteristic.
- Neurological examination — no focal deficit. The patient may report subjective numbness or weakness, but the examination is normal.
- Hypermobility screen — perform the Beighton score (fifth-finger dorsiflexion, thumb apposition, elbow and knee hyperextension, palms to the floor; maximum 9). Hypermobility is over-represented in fibromyalgia and contributes a biomechanical component to the pain.
- Screen for mimics — check for the synovitis of RA, the proximal weakness of myopathy, the temporal artery tenderness of giant cell arteritis (in the older patient), and any focal abnormality. [1]
The key examination finding: generalised soft-tissue tenderness with no objective joint, neurological or tissue abnormality. [1]
Investigations
The investigation is targeted to exclude the mimics. The goal is to do ENOUGH to exclude inflammatory, endocrine and malignant causes, and NOT to over-investigate. [1]
| Test | Purpose | Expected result in fibromyalgia |
|---|---|---|
| FBC | Exclude anaemia, malignancy, chronic disease | Normal |
| ESR and CRP | Exclude inflammation | Normal (the key clue) |
| TSH and free T4 | Exclude hypothyroidism | Normal |
| CK | Exclude myopathy, statin myalgia | Normal |
| Creatinine and electrolytes | Baseline, exclude metabolic cause | Normal |
| Vitamin D | Exclude osteomalacia | Normal or low (treat if low) |
| ANA | Only if clinical suggestion of SLE | Negative (or low-titre incidental) |
| RF and anti-CCP | Only if clinical suggestion of RA | Negative |
| HLA-B27 | Only if clinical suggestion of spondyloarthritis | Not routinely required |
The single most important diagnostic clue: persistent normality of CRP and ESR with widespread pain, over months of symptoms, in the absence of an alternative explanation. This pattern supports a central pain mechanism and argues against ongoing peripheral inflammation. [1]
Avoid over-investigation. Each normal result that is sought reinforces the patient's belief that there must be a hidden peripheral cause, and each repeated scan or biopsy that is normal delays the move to an evidence-based management plan. Make the diagnosis, explain it, and resist the pressure for further negative investigations. [1]
Assessment tools
The Fibromyalgia Impact Questionnaire Revised (FIQR) (Bennett 2009) is a 21-item patient-reported measure across three domains — function, overall impact and symptoms — each scored 0 to 10, with a maximum total of 100 [9]. It is used to baseline the disease impact at diagnosis and to track the response to management over time. It is not diagnostic in isolation.
The Polysymptomatic Distress Scale is the combined WPI and SSS, and it tracks the symptom burden over time. [1]
Management

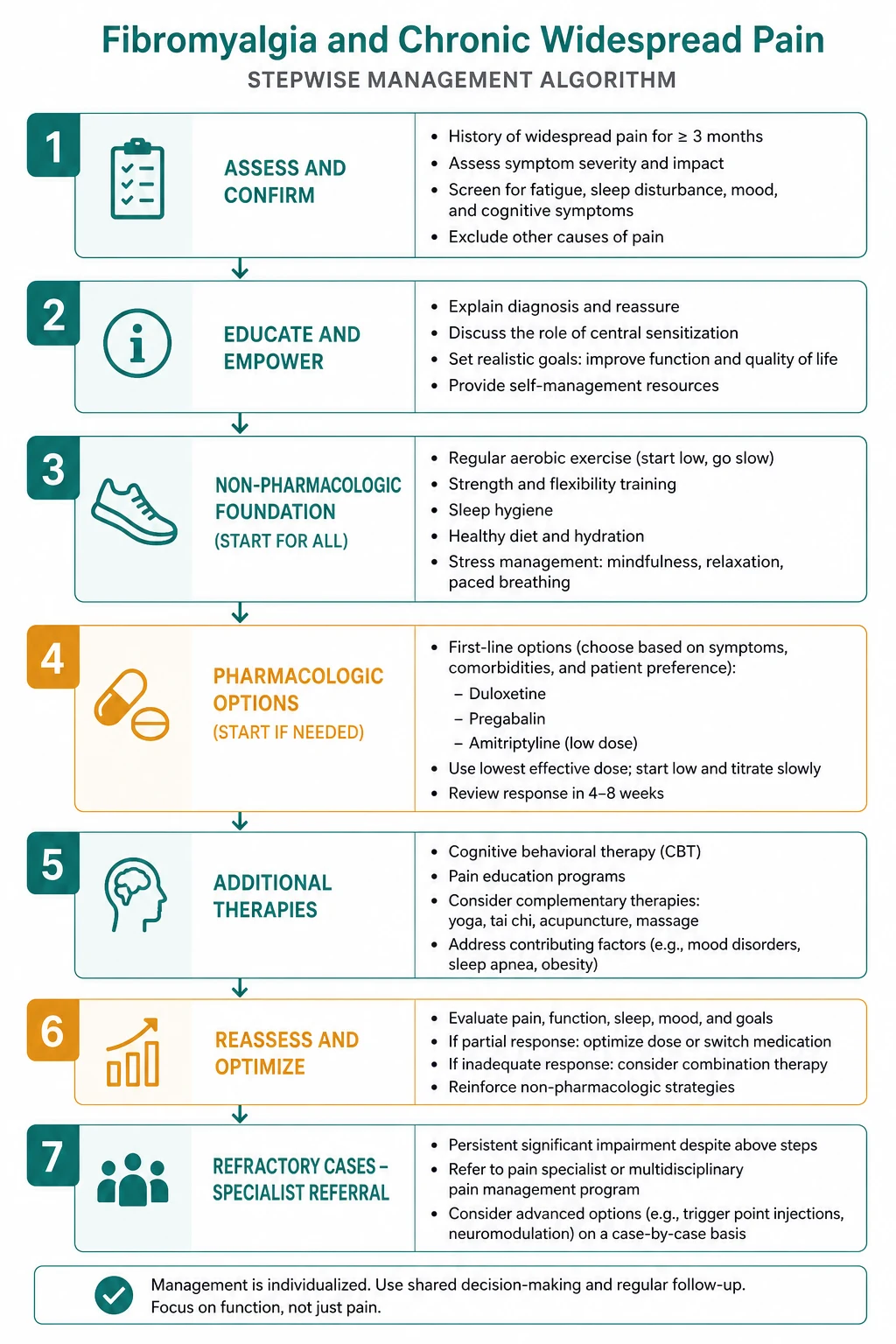
The management of fibromyalgia is non-pharmacological first, with symptom-targeted pharmacotherapy as adjunct, delivered within a multidisciplinary framework. The 2017 EULAR recommendations make exercise the only therapy-based strong-for recommendation [3]. Pharmacotherapy alone is insufficient.
The non-pharmacological foundation (first-line)
| Therapy | Evidence and detail |
|---|---|
| Patient education and validation | Acknowledge the pain as real, explain the central sensitisation mechanism in plain language ("the volume control on the pain system is turned up"), set the expectation of management rather than cure. |
| Graded aerobic exercise | The cornerstone. The Hauser meta-analysis (2010) of 28 RCTs showed aerobic exercise reduced pain, fatigue, depressed mood and improved quality of life and physical fitness [7]. The Cochrane review confirmed supervised aerobic training has beneficial effects on physical capacity and symptoms [8]. Start low (walking, swimming, cycling), progress slowly, aim for moderate intensity two to three times weekly. The key is grading — starting too hard flares the pain and reinforces avoidance. |
| Cognitive behavioural therapy (CBT) | Addresses unhelpful illness beliefs (catastrophising, fear-avoidance), teaches coping strategies, and improves function even when pain intensity is unchanged. EULAR recommends CBT for mood disorder or unhelpful coping. |
| Sleep hygiene | Fixed sleep and wake times, avoidance of caffeine and screens before bed, a cool dark bedroom, and a wind-down routine. The sleep is the foundation of the fatigue and the cognitive dysfunction. |
| Graded activity and pacing | The patient learns to balance activity and rest to avoid the boom-and-bust cycle (overdoing it on a good day, crashing for days after). Pacing is a skill taught by an occupational therapist or physiotherapist. |
| Mindfulness-based stress reduction (MBSR) | An 8-week programme of mindfulness meditation and yoga, with trial evidence of improved pain, function and coping. |
| Tai chi and yoga | Mind-body exercise with trial evidence of benefit, particularly for the pain and the sleep, and with high adherence compared with aerobic exercise. |
The pharmacological adjunct (symptom-targeted)
Pharmacotherapy is adjunct to the non-pharmacological foundation. It is chosen on the basis of the predominant symptom and titrated to response. [1]
| Drug | Dose and route | Mechanism | Indication | Key cautions |
|---|---|---|---|---|
| Amitriptyline | 10 to 25 mg orally at night (start at 10 mg, titrate slowly) | Tricyclic — inhibits reuptake of serotonin and noradrenaline; also improves sleep architecture | First-line, particularly when sleep disturbance is prominent | Anticholinergic effects (dry mouth, constipation, urinary retention), morning sedation, QT prolongation; avoid in glaucoma and prostatism |
| Duloxetine | 30 mg daily for one week, then 60 mg daily (maximum 120 mg daily) | SNRI — enhances descending serotonergic and noradrenergic inhibition; pain reduction independent of mood effect (Arnold 2005) [6] | Particularly when comorbid depression or when pain is the predominant symptom | Nausea, insomnia, sexual dysfunction, hyponatraemia (SIADH), blood pressure elevation; avoid in uncontrolled hypertension, hepatic impairment; do not combine with MAOIs |
| Pregabalin | 75 mg twice daily, titrate to 150 to 300 mg twice daily (maximum 600 mg daily) | Alpha-2-delta ligand — binds voltage-gated calcium channel, reduces excitatory neurotransmitter (glutamate, substance P) release; improved pain and sleep (Crofford 2005) [5] | Particularly when the neuropathic component or the sleep disturbance is prominent | Dizziness, somnolence, weight gain, peripheral oedema; reduce dose in renal impairment; misuse potential; taper on cessation |
| Gabapentin | 300 mg at night, titrate to 1200 to 2400 mg daily in divided doses | As pregabalin | Alternative to pregabalin, cheaper | As pregabalin; adjust for renal function |
| Cyclobenzaprine | 5 to 10 mg at night | Structurally related to tricyclics; muscle relaxant | Short-term adjunct for sleep and muscle pain | Sedation, anticholinergic effects |
Combination therapy: where monotherapy is insufficient, combine agents from different mechanistic classes — for example, amitriptyline at night for sleep with duloxetine in the morning for pain and mood, or pregabalin for the neuropathic component with an antidepressant for the central component. The combination must be rational (no two serotonergic agents at risk of serotonin syndrome) and titrated carefully. [1]
What to AVOID (the high-yield exam discriminator)
| Therapy | Why avoid |
|---|---|
| Opioids | No evidence of sustained benefit; worsen central sensitisation through opioid-induced hyperalgesia (a neuroplastic phenomenon of increased pain sensitivity); carry dependence, misuse and overdose risk; observational data show worse long-term outcomes in fibromyalgia patients prescribed opioids. This is the single most important prescribing decision in fibromyalgia. |
| Glucocorticoids | The disease is not inflammatory. There is no inflammatory marker, no synovitis, no autoantibody-driven process. Glucocorticoids cause harm (osteoporosis, diabetes, infection, adrenal suppression) with no mechanistic rationale. |
| NSAIDs as primary therapy | No central pain benefit. May help comorbid osteoarthritis or dysmenorrhoea, but do not address the fibromyalgia mechanism. Long-term NSAID use carries gastrointestinal, renal and cardiovascular harm. |
| Benzodiazepines | Sedating, dependence-forming, disrupt sleep architecture, and do not address the mechanism. |
| Repeated invasive investigations | Each normal result that is sought reinforces the illness belief and the search for a hidden peripheral cause. |
| Surgery for non-specific findings | No evidence of benefit; exposes to harm. |
The multidisciplinary approach
Fibromyalgia is best managed by a multidisciplinary team: [1]
- The rheumatologist or general physician makes the diagnosis, excludes the mimics, and provides the initial education.
- The GP provides longitudinal continuity, titrates the pharmacotherapy, and coordinates the team.
- The physiotherapist supervises the graded exercise programme and teaches pacing.
- The clinical psychologist delivers CBT and addresses the unhelpful illness beliefs, the catastrophising and the comorbid mood disorder.
- The pain specialist manages refractory cases and coordinates the opioid deprescribing where needed.
- The occupational therapist addresses the functional impact, the workplace accommodation and the graded return-to-work plan. [1]
Early multidisciplinary intervention improves long-term functional outcome. Late referral of a chronically disabled, opioid-exposed, investigation-saturated patient is much harder to turn around. [1]
Distinguishing fibromyalgia from inflammatory rheumatological disease
This is the single highest-yield clinical discrimination in the topic. The patient with widespread pain may have fibromyalgia, an inflammatory rheumatological disease, or both (secondary fibromyalgia). [1]
| Feature | Fibromyalgia | Inflammatory disease (RA, SLE, SpA) |
|---|---|---|
| Pain pattern | Widespread, non-articular, soft-tissue | Articular, symmetrical (RA), specific distribution |
| Morning stiffness | May be present but brief and non-specific | Prolonged (more than 1 hour), improves with activity |
| Synovitis | Absent | Present (bogginess, warmth, effusion) |
| CRP and ESR | Normal | Elevated (in active disease) |
| Autoantibodies | Negative (or incidental low-titre) | RF and anti-CCP (RA), ANA and anti-dsDNA (SLE), HLA-B27 (SpA) |
| Response to activity | Variable; overexertion flares the pain | Stiffness improves with activity (the gelling phenomenon) |
| Response to glucocorticoids | None | Dramatic (RA, PMR) |
| Imaging | Normal | Erosions (RA), sacroiliitis (SpA), effusions |
The discordant case — a patient with established inflammatory disease whose markers are quiet but whose activity score is high — is the classic scenario for secondary fibromyalgia. The correct response is to recognise the central sensitisation component, not to escalate the immunosuppression. [1]
Prognosis
Fibromyalgia is a chronic condition with a fluctuating course. The functional outcome is highly variable: [1]
- A subgroup of patients, with early diagnosis, multidisciplinary intervention and engagement with the non-pharmacological foundation, achieve meaningful functional improvement and return to work.
- A subgroup, particularly those with late diagnosis, opioid exposure, multiple comorbid central sensitivity syndromes and psychiatric comorbidity, remain chronically disabled.
- The pain intensity fluctuates with stress, sleep, mood and activity, and the patient can be taught to manage these triggers. [1]
The prognosis is not benign. Fibromyalgia is associated with reduced quality of life comparable to RA, increased healthcare utilisation, increased work disability, and an increased prevalence of depression and anxiety. The role of the physician is to shift the trajectory — by early diagnosis, by validation, by the non-pharmacological foundation, and by the avoidance of iatrogenic harm (opioids, over-investigation, invalidation). [1]
High-yield exam discriminators (the viva and MCQ traps)
- The criteria: 2016 ACR — WPI and SSS, NOT the 1990 tender points. The 11-of-18 tender point examination is obsolete.
- The markers: Normal CRP and ESR with widespread pain is the clue. A raised marker means a different diagnosis.
- The pharmacology: Amitriptyline, duloxetine, pregabalin — NOT opioids, NOT glucocorticoids.
- The mechanism: Central sensitisation — NOT inflammation, NOT autoimmunity, NOT tissue damage.
- The comorbidity: Secondary fibromyalgia inflates the DAS28 and the SLEDAI and drives inappropriate biologic escalation.
- The management: Exercise is the only EULAR strong-for recommendation. Non-pharmacological first.
- The communication: Validate the pain as real. Invalidation worsens outcomes.
- The mimics: PMR (raised ESR, dramatic steroid response), hypothyroidism (raised TSH), polymyositis (raised CK, proximal weakness). [1]
Summary for the viva
Fibromyalgia is a chronic central pain syndrome of amplified CNS pain processing (central sensitisation) with deficient descending inhibition, presenting as widespread musculoskeletal pain for at least three months with fatigue, non-restorative sleep, cognitive dysfunction and somatic symptoms. The 2016 ACR criteria (WPI 7 plus SSS 5, or WPI 4 to 6 plus SSS 9, with generalised pain and at least three months of symptoms) replace the obsolete tender point examination. Normal inflammatory markers with widespread pain is the key diagnostic clue. Management is non-pharmacological first — patient education and validation, graded aerobic exercise (the only EULAR strong-for recommendation), CBT, sleep hygiene and pacing — with symptom-targeted pharmacotherapy (amitriptyline 10 to 25 mg at night, duloxetine 30 to 60 mg, pregabalin or gabapentin) as adjunct. Opioids (worsen central sensitisation), glucocorticoids (not inflammatory) and repeated invasive investigations (reinforce illness belief) are explicitly avoided. The multidisciplinary team — physician, GP, physiotherapist, psychologist, pain specialist — delivers the integrated care, and early multidisciplinary intervention improves long-term functional outcome. The highest-yield clinical discrimination is fibromyalgia from inflammatory rheumatological disease (normal markers, no synovitis, no morning stiffness improvement, widespread non-articular pattern) and the recognition of secondary fibromyalgia inflating the composite disease-activity scores. [1]
References
- [1]Wolfe F, Clauw DJ, Fitzcharles MA, et al. 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria Semin Arthritis Rheum, 2016.PMID 27916278
- [2]Clauw DJ Fibromyalgia: a clinical review JAMA, 2014.PMID 24737367
- [3]Macfarlane GJ, Kronisch C, Atzeni F, et al. EULAR revised recommendations for the management of fibromyalgia Ann Rheum Dis, 2017.PMID 27377815
- [4]Fitzcharles MA, Ste-Marie PA, Pereira JX, et al. 2012 Canadian Guidelines for the diagnosis and management of fibromyalgia syndrome: executive summary Pain Res Manag, 2013.PMID 23748251
- [5]Crofford LJ, Rowbotham MC, Mease PJ, et al. Pregabalin for the treatment of fibromyalgia syndrome: results of a randomized, double-blind, placebo-controlled trial Arthritis Rheum, 2005.PMID 15818684
- [6]Arnold LM, Lu Y, Crofford LJ, et al. A randomized, double-blind, placebo-controlled trial of duloxetine in the treatment of women with fibromyalgia with or without major depressive disorder Pain, 2005.PMID 16298061
- [7]Hauser W, Klose-Becker A, Bartholomeuszik G, et al. Efficacy of different types of aerobic exercise in fibromyalgia syndrome: a systematic review and meta-analysis of randomised controlled trials Arthritis Res Ther, 2010.PMID 20459730
- [8]Busch AJ, Barber KAR, Overend TJ, Peloso PMJ, Schachter CL Exercise for treating fibromyalgia syndrome Cochrane Database Syst Rev, 2007.PMID 17943797
- [9]Bennett RM, Friend R, Jones KD, Ward R, Han BK, Ross RL The Revised Fibromyalgia Impact Questionnaire (FIQR): validation and psychometric properties Arthritis Res Ther, 2009.PMID 19664287