Phys · rheumatological
Rheumatoid Arthritis
Also known as rheumatoid arthritis · RA · seropositive polyarthritis · autoimmune synovitis · rheumatoid disease
Consultant-physician-depth guide to rheumatoid arthritis — autoimmune synovitis pathophysiology (T-cell driven, B-cell antibodies, cytokine cascades, pannus formation), symmetrical small-joint polyarthritis with extra-articular manifestations, ACR/EULAR 2010 classification, treat-to-target management with conventional synthetic, biologic and targeted synthetic DMARDs, pre-biologic screening, and comorbidity management — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Rheumatoid Arthritis

The one-minute consultant answer
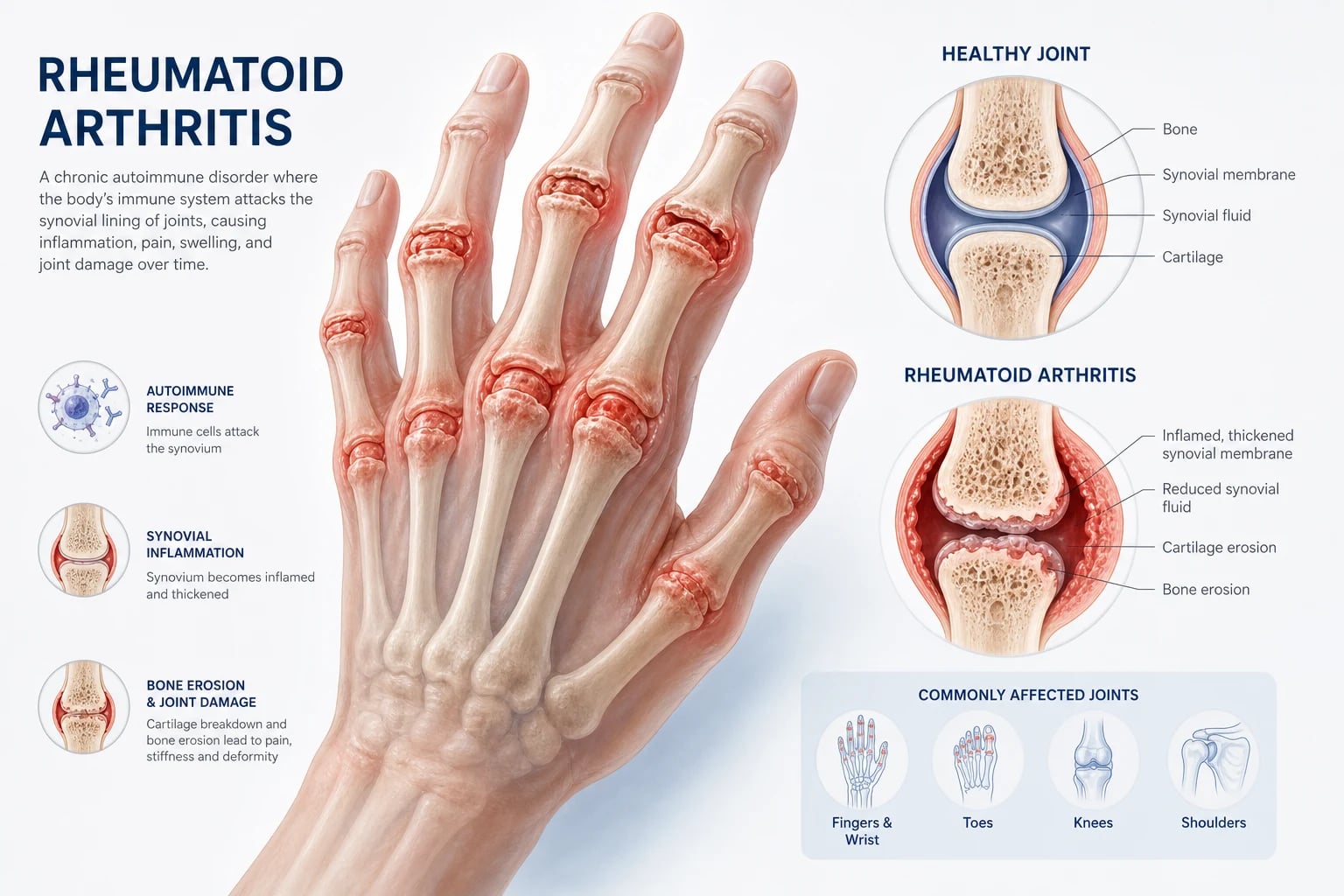
Rheumatoid arthritis (RA) is a chronic, symmetrical, inflammatory polyarthritis characterised by autoimmune-driven synovial proliferation that erodes cartilage and bone. The classical pattern targets the small joints of the hands and feet — metacarpophalangeal joints (MCPs), proximal interphalangeal joints (PIPs), wrists and metatarsophalangeal joints (MTPs) — with morning stiffness lasting more than one hour. The 2010 ACR/EULAR classification criteria combine joint involvement, serology (RF and anti-CCP), acute-phase reactants (CRP or ESR) and symptom duration to identify definite RA with a score of 6 or more out of 10 [1]. Management follows the treat-to-target paradigm: aim for remission or low disease activity, monitor every 1 to 3 months with a composite score (DAS28, CDAI or SDAI), and escalate if the target is not reached within 3 to 6 months [3][4]. Methotrexate is the anchor DMARD and first-line therapy; if the target is not met, add or switch to a biologic (anti-TNF, anti-IL-6 receptor, anti-CD20) or a JAK inhibitor. This is a systemic disease — extra-articular manifestations and comorbidities (cardiovascular disease, interstitial lung disease, osteoporosis, infection risk) determine mortality as much as joint damage does.
Pathophysiology — why RA does what it does

Understanding the immunopathogenesis is not optional for a physician trainee. Every modern treatment — from methotrexate through anti-TNF to JAK inhibitors — targets a specific step in this cascade. You cannot reason about escalation or adverse effects without knowing the mechanism. [1]
The two-hit model: genetics plus environment
RA is not a single disease but a syndrome with two immunologically distinct subsets: anti-CCP-positive (seropositive) RA and anti-CCP-negative (seronegative) RA. The seropositive subset accounts for approximately 70 per cent of cases and has a more aggressive, erosive course with a stronger genetic contribution. [1]
The dominant genetic association is the HLA-DRB1 shared epitope — a conserved amino acid sequence (QKRAA, QRRAA or RRRAA) in the beta-chain of HLA-DR that presents citrullinated peptides to CD4+ T cells. The shared epitope is necessary but not sufficient: the disease requires a second hit, and the best-established environmental trigger is cigarette smoking [11].
The Klareskog model describes the sequence: smoking induces oxidative stress and inflammation in the lungs, activating peptidylarginine deiminases (PAD enzymes) that convert arginine to citrulline in self-proteins. Citrullinated proteins become neoantigens. In individuals carrying the HLA-DRB1 shared epitope, these neoantigens are efficiently presented to the adaptive immune system, breaking tolerance. The result is production of anti-citrullinated protein antibodies (ACPAs) — the family that includes anti-CCP [11]. These autoantibodies can appear in serum 5 to 10 years before the onset of clinical arthritis, which is why anti-CCP is both a diagnostic and a prognostic marker.
The cellular orchestra: T cells, B cells and macrophages
Once tolerance is broken, the synovium transforms from a thin, quiescent membrane into a hypertrophic, invasive tissue. [1]
CD4+ T cells (Th1 and Th17 subsets) infiltrate the synovium and provide help to B cells. They also activate macrophages through cell contact and cytokines, sustaining the inflammatory loop. Th17 cells produce IL-17, which synergises with TNF and IL-1 to amplify inflammation and recruit neutrophils. [1]
B cells produce the autoantibodies (RF and anti-CCP), present antigen to T cells, and form ectopic lymphoid structures (germinal centre-like aggregates) within the synovium in severe disease. B-cell depletion with rituximab demonstrates that B cells are not merely passive antibody factories but active amplifiers of the immune response. [1]
Macrophages are the principal source of the destructive cytokines — TNF-alpha, IL-1 and IL-6 — that drive synovial inflammation, pannus formation and systemic features (fatigue, anaemia of chronic disease, acute-phase response). The macrophage-T cell cytokine loop is the pharmacological target of every biologic DMARD. [1]
The cytokine cascade and why it matters for treatment
Three cytokines dominate the RA inflammatory cascade: [1]
| Cytokine | Principal source | Key effects | Targeted by |
|---|---|---|---|
| TNF-alpha | Macrophages, mast cells | Amplify inflammation, activate endothelium, upregulate RANKL (osteoclast activation, erosions) | Infliximab, adalimumab, etanercept, certolizumab, golimumab |
| IL-6 | Macrophages, synovial fibroblasts | Acute-phase response (CRP), B-cell differentiation, hepcidin upregulation (anaemia of chronic disease) | Tocilizumab, sarilumab |
| IL-1 | Macrophages | Less dominant in RA than in autoinflammatory disease; synergises with TNF | Anakinra (rarely used in RA) |
The cascade feeds into the JAK-STAT intracellular signalling pathway — the target of the oral JAK inhibitors (tofacitinib, baricitinib, upadacitinib). Multiple cytokine receptors signal through JAK, so inhibiting JAK blocks several inflammatory pathways simultaneously. [1]
Pannus formation and joint destruction
The proliferating synovium invades cartilage and bone as a pannus — a tumour-like mass of activated synovial fibroblasts, macrophages, osteoclasts and lymphocytes. Pannus destroys joints through three mechanisms: [1]
- Cartilage degradation — synovial fibroblasts and macrophages secrete matrix metalloproteinases (MMPs) that digest cartilage collagen and proteoglycans.
- Marginal erosions — osteoclasts, activated by RANKL (expressed by activated T cells and synovial fibroblasts), erode bone at the joint margin where bare bone is exposed. This is the earliest radiographic sign (visible earlier on MRI or ultrasound than on plain X-ray).
- Joint space narrowing — cartilage loss produces concentric joint space narrowing, distinct from the asymmetric narrowing of osteoarthritis. [1]
The rate of radiographic progression is highest in the first 1 to 2 years of disease, which is why early, aggressive treatment is essential. The treat-to-target window is real — erosions that form are irreversible. [1]
Clinical features — the full spectrum
Articular manifestations
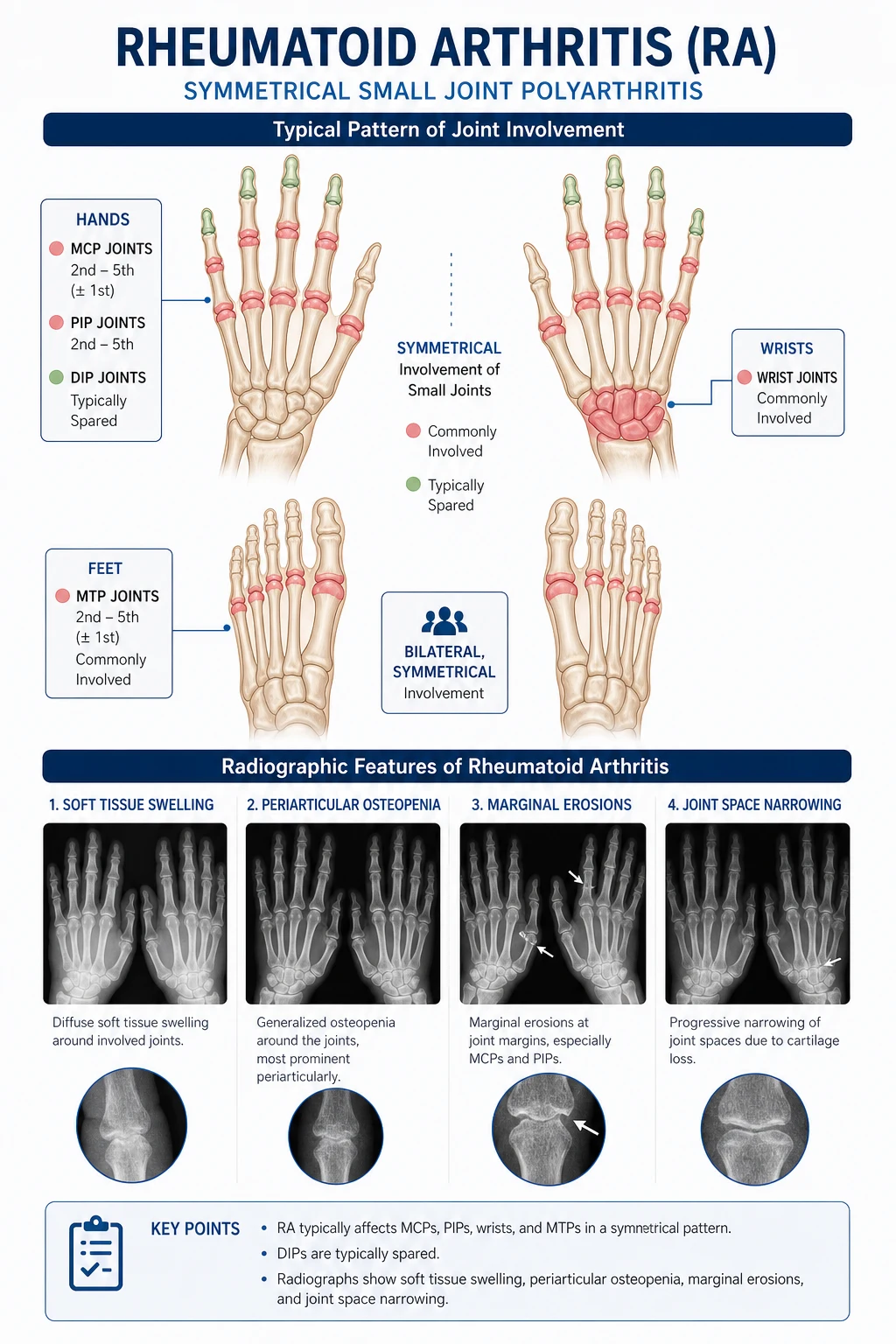
The classical articular presentation is symmetrical polyarthritis of the small joints: [1]
| Site | Pattern | Key features |
|---|---|---|
| MCP joints | Symmetrical, sparing the thumb | Tenderness, palpable synovial bogginess, eventual ulnar deviation, palmar subluxation |
| PIP joints | Symmetrical | Spindle-shaped (fusiform) swelling; distinguish from Heberden nodes (DIP, OA) and Bouchard nodes (PIP, OA) |
| Wrists | Bilateral | Radiocarpal and distal radioulnar joint involvement; eventual dorsal subluxation of the ulnar head (caput ulnae), extensor tenosynovitis |
| MTP joints | Symmetrical, especially 4th and 5th | "Lateral compression pain" — squeeze across the MTP heads (MTP squeeze test); early metatarsalgia and eventual hallux valgus, claw toes |
| Cervical spine | C1-C2 | Atlantoaxial subluxation (anterior translation of C1 on C2); also atlantoaxial impaction (vertical subluxation of the odontoid) and subaxial subluxation |
Morning stiffness lasting more than one hour (and frequently several hours) is the key discriminating feature from osteoarthritis, in which stiffness is brief (less than 30 minutes) and worsens with use. The stiffness in RA improves with activity — this is the "gelling phenomenon": the joint gels with inactivity and loosens with movement. [1]
Joints typically SPARED in RA: distal interphalangeal joints (DIPs), the thoracolumbar spine, and the sacroiliac joints. DIP involvement should prompt reconsideration of the diagnosis (osteoarthritis, psoriatic arthritis, gout). [1]
Late hand deformities (DCE short-case territory)
These deformities are exam favourites because they are visually diagnostic: [1]
- Ulnar deviation of the fingers — the MCP joints sublux and the fingers drift ulnarward.
- Palmar subluxation of the MCP joints — the phalanx slides palmarward off the metacarpal head.
- Swan-neck deformity — PIP hyperextension with DIP flexion. Mechanism: flexor tendon tightness or intrinsic muscle tightness pulling the PIP into hyperextension.
- Boutonniere deformity — PIP flexion with DIP hyperextension. Mechanism: central slip extensor tendon rupture at the PIP, allowing the lateral bands to slip palmarward, acting as flexors at the PIP.
- Z-deformity of the thumb — MCP flexion, IP hyperextension.
- Dorsal subluxation of the ulnar head (caput ulnae) — prominent ulnar styloid with piano-key movement on pressing the wrist.
- Extensor tendon ruptures — especially extensor digitorum communis and extensor digiti minimi, from friction over a dorsal-subluxed ulnar head. Present as sudden inability to extend a finger. [1]
Constitutional and systemic features
RA is a systemic disease. Patients commonly describe fatigue, low-grade fever, weight loss and generalised malaise proportional to disease activity. These are driven by cytokine release (TNF, IL-1, IL-6) — the same mechanism that drives the acute-phase response (elevated CRP, elevated ESR, thrombocytosis) and anaemia of chronic disease (hepcidin-mediated iron sequestration). [1]
Extra-articular manifestations
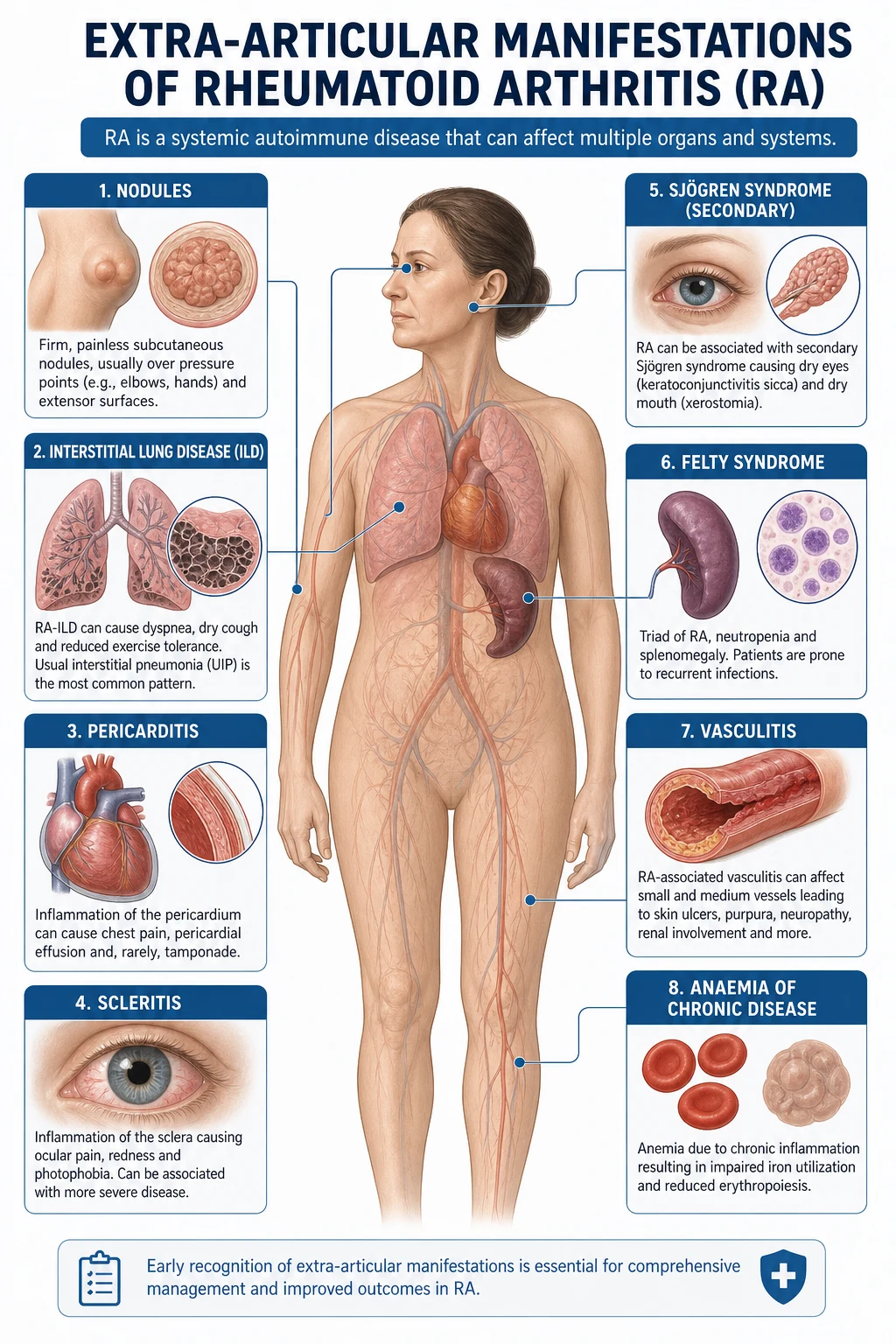
Extra-articular involvement occurs in approximately 40 per cent of patients over the disease course, almost exclusively in seropositive (RF and/or anti-CCP positive) disease. These manifestations predict mortality and are the substance of a DCE long case. [1]
Rheumatoid nodules
The most common extra-articular feature. Firm, non-tender, mobile subcutaneous nodules on extensor surfaces — classically the olecranon, the proximal ulna, the knuckles and the Achilles tendon. Histologically, they are granulomatous with a central area of fibrinoid necrosis surrounded by palisading histiocytes. They correlate with seropositive disease and more aggressive articular disease. Nodules over the vocal cords (in the larynx) can cause hoarseness and stridor. Pulmonary and cardiac nodules also occur. [1]
Exam trap: Methotrexate can cause accelerated nodulosis (methotrexate-induced nodulosis) — multiple small nodules on the fingers that appear despite disease control. This is a paradoxical reaction, not treatment failure. [1]
Pulmonary involvement
Pulmonary disease is the leading extra-articular cause of death in RA. The spectrum includes: [1]
- Interstitial lung disease (RA-ILD) — the most clinically important pulmonary manifestation. The usual pattern is usual interstitial pneumonia (UIP) — basal, reticulonodular changes with honeycombing on HRCT — identical radiologically to idiopathic pulmonary fibrosis, but in the setting of RA. Less common patterns include nonspecific interstitial pneumonia (NSIP) and organising pneumonia. Risk factors: male sex, smoking, older age, anti-CCP positivity. Methotrexate itself can cause pneumonitis — always distinguish drug-induced pneumonitis from RA-ILD.
- Pleural disease — pleural effusion (exudative, characteristically very low glucose, often below 1.4 mmol/L, and low pH), pleural nodules, pleuritic chest pain. The very low pleural fluid glucose is an exam favourite. [1]- Rheumatoid (Caplan) nodules — well-defined pulmonary nodules that may cavitate. Caplan syndrome is the combination of rheumatoid nodules and pneumoconiosis (coal workers' pneumoconiosis, silicosis, asbestosis) — rapidly progressive pulmonary nodules in a dust-exposed worker with RA.
- Obstructive airways disease — bronchiectasis and bronchiolitis are increased in frequency in RA.
- Drug-induced pneumonitis — methotrexate, leflunomide and biologics can all cause interstitial pneumonitis, which can be clinically and radiologically indistinguishable from RA-ILD. This distinction is critical because treatment differs (stop the drug versus treat the disease). [1]
Cardiovascular involvement
- Pericarditis — the most common cardiac manifestation. Usually clinically silent; effusions are common on echocardiography but rarely cause tamponade.
- Coronary artery disease — RA is an independent cardiovascular risk factor equivalent to diabetes mellitus [10]. Chronic systemic inflammation accelerates atherosclerosis.
- Myocarditis and cardiac nodules — rare.
- Aortic and mitral regurgitation — from nodular involvement of valve leaflets.
Ocular involvement
- Keratoconjunctivitis sicca — secondary Sjogren syndrome (dry eyes, dry mouth) occurs in 10 to 15 per cent of RA patients. Schirmer test is positive. Distinguish from primary Sjogren syndrome (which occurs without another autoimmune disease and is anti-Ro/anti-La positive).
- Episcleritis — mild, self-limiting, does not threaten sight. Treated with topical lubricants.
- Scleritis — severe, painful, sight-threatening. Diffuse anterior scleritis causes deep boring eye pain with redness. Scleromalacia perforans (necrotising scleritis without inflammation) is the feared complication — thinning of the sclera with visible uveal tissue. Requires urgent ophthalmology and systemic immunosuppression.
- Peripheral ulcerative keratitis — corneal melting; a rheumatoid emergency. [1]
Haematological involvement
- Anaemia of chronic disease — the most common haematological abnormality. Driven by IL-6-mediated hepcidin upregulation, which sequestures iron in macrophages. Normocytic, normochromic, low iron, low transferrin, high ferritin. Treat the underlying disease, not the iron.
- Felty syndrome — the triad of RA, splenomegaly and neutropenia (neutrophil count below 1.5 x 10^9/L). Occurs in long-standing, seropositive, nodular RA. Complicated by recurrent bacterial infections and leg ulcers. Treatment: methotrexate, rituximab, or splenectomy. Large granular lymphocyte (LGL) syndrome overlaps with Felty and is associated with T-cell large granular lymphocytic leukaemia.
- Thrombocytosis — reactive, proportional to disease activity.
- Lymphadenopathy — reactive, can mimic lymphoma. [1]
Vasculitis
Rheumatoid vasculitis is now uncommon (it was more prevalent in the pre-biologic era) but remains a serious complication of long-standing, poorly controlled seropositive RA. The spectrum includes: [1]
- Nail-fold infarcts and digital pulp infarcts (mild).
- Digital gangrene — requires urgent treatment.
- Mononeuritis multiplex — vasculitic neuropathy; presents as foot drop, wrist drop or sensory loss in a nerve distribution. Confirmed by nerve conduction studies and nerve biopsy. This is a medical emergency.
- Mesenteric vasculitis — bowel ischaemia and perforation.
- Cutaneous vasculitis — palpable purpura, leg ulcers, pyoderma gangrenosum-like lesions. [1]
Rheumatoid vasculitis is treated with high-dose glucocorticoids and cyclophosphamide or rituximab. [1]
Neurological involvement
- Cervical spine subluxation — the most feared neurological complication. Atlantoaxial subluxation (anterior displacement of the atlas on the axis, anterior atlantodental interval above 3 mm on lateral cervical spine flexion view) can compress the spinal cord, causing myelopathy, progressive quadriparesis, and even sudden death from brainstem compression. Atlantoaxial impaction (vertical subluxation — the odontoid migrates superiorly through the foramen magnum) can compress the vertebrobasilar circulation. Any RA patient scheduled for surgery or intubation needs a lateral cervical spine flexion view or MRI to rule out atlantoaxial instability. Symptoms: occipital headache, sensory changes in the hands, progressive weakness, gait disturbance. Signs: pyramidal signs, sensory level, urinary retention.
- Peripheral neuropathy — from vasculitis, cervical root compression, or entrapment (carpal tunnel syndrome is common in RA from wrist synovitis compressing the median nerve).
- Cervical cord compression — a rheumatological emergency; requires urgent MRI and neurosurgical or spinal orthopaedic opinion. [1]
Diagnosis and classification

The 2010 ACR/EULAR classification criteria
The 2010 criteria replaced the 1987 ACR criteria, which were insensitive for early disease (they required features like erosions and nodules that develop later). The 2010 system is designed to identify patients with early, active, inflammatory synovitis who are at risk for persistent and erosive disease [1].
Prerequisite: confirmed synovitis in at least one joint, not better explained by another disease. [1]
Scoring (score of 6 or more out of 10 classifies definite RA): [1]
| Domain | Score 0 | Score 1 | Score 2 | Score 3 | Score 5 |
|---|---|---|---|---|---|
| Joint involvement (count of swollen or tender joints, excluding DIPs, first CMC, first MTP) | 1 large joint | 2 to 10 large joints | 1 to 3 small joints (with or without large joints) | 4 to 10 small joints | Above 10 joints (at least 1 small joint) |
| Serology (RF and anti-CCP) | Negative | — | Low-positive | High-positive (above 3 times ULN) | — |
| Acute-phase reactants (CRP and ESR) | Normal | Abnormal | — | — | — |
| Symptom duration | Under 6 weeks | 6 weeks or more | — | — | — |
Large joints: shoulders, elbows, hips, knees, ankles. Small joints: MCPs, PIPs, second to fifth MTPs, thumb IP, wrists. [1]
Exam trap: The 2010 criteria are classification criteria, not diagnostic criteria. They identify patients likely to have RA for research and early-treatment purposes. A patient can score 6 and have a mimic (psoriatic arthritis, SLE with arthropathy, polyarticular gout). Clinical judgment is always the final arbiter. Conversely, a seronegative patient with short symptom duration may score below 6 and still have RA — this is why the criteria include the phrase "not better explained by another disease." [1]
Serology — RF and anti-CCP
| Feature | Rheumatoid Factor (RF) | Anti-CCP (ACPA) |
|---|---|---|
| Target | Fc portion of IgG | Citrullinated peptides |
| Sensitivity for RA | 60 to 80 per cent | 60 to 70 per cent |
| Specificity for RA | 70 to 80 per cent | 90 to 98 per cent |
| Appears early | Sometimes late | Yes — years before symptoms |
| Predicts erosive disease | Moderately | Strongly |
| False positives | Sjogren, SLE, chronic hepatitis, endocarditis, cryoglobulinaemia, healthy elderly | Rare — very specific |
The Nishimura meta-analysis confirmed that anti-CCP is more specific than RF for RA and is a better predictor of erosive disease [2]. Always send both tests. Anti-CCP positivity is the single strongest serological predictor of aggressive, erosive disease and is therefore an indication to treat aggressively from the outset.
About 20 to 30 per cent of RA patients are seronegative for both RF and anti-CCP — "seronegative RA." This subset tends to be less erosive but still requires DMARD therapy. [1]
Acute-phase reactants
CRP and ESR are markers of systemic inflammation and are useful for monitoring disease activity. They are incorporated into composite scores (DAS28 uses ESR or CRP). Note that ESR is affected by immunoglobulin levels (which may be elevated in seropositive RA) and by anaemia, while CRP is not. Some patients have active clinical disease with normal CRP and ESR — particularly the seronegative subset. Use a clinical composite score (CDAI or SDAI, which do not require laboratory data) in these patients. [1]
Imaging
Plain X-rays of hands, wrists and feet remain the first-line imaging modality. The classical sequence of radiographic changes: [1]
- Soft tissue swelling and periarticular osteopenia (earliest findings, often non-specific).
- Marginal erosions — the hallmark. Best seen at the ulnar styloid, the radial aspect of the second and third MCP heads, and the MTP heads (especially the fifth).
- Joint space narrowing — uniform, concentric (unlike the asymmetric, compartmental narrowing of OA).
- Late changes — subluxation, deformity, ankylosis. [1]
Plain X-rays are insensitive for early disease — erosions appear on X-ray months to years after they are present on MRI or ultrasound. This is why early RA can have normal X-rays, and why ultrasound or MRI is recommended when clinical suspicion is high but X-rays are normal. [1]
Ultrasound detects synovial hypertrophy (grey-scale), synovial vascularity (power Doppler), erosions and tenosynovitis. Power Doppler is particularly valuable — active synovial hyperaemia predicts erosive progression and response to treatment. [1]
MRI detects synovitis, bone marrow oedema (the strongest predictor of future erosion), erosions and tenosynovitis. It is the most sensitive modality for early disease but is rarely needed in routine practice if ultrasound is available. [1]
Differential diagnosis of inflammatory polyarthritis
The question "is this RA or something else?" must always be asked. The key differentials: [1]
| Condition | Discriminating features |
|---|---|
| Psoriatic arthritis | Asymmetrical, DIP involvement, enthesitis, dactylitis (sausage digit), nail changes (pitting, onycholysis), psoriasis rash, negative RF and anti-CCP |
| Ankylosing spondylitis / axial spondyloarthritis | Inflammatory back pain, sacroiliitis, enthesitis, HLA-B27 positive, asymmetrical large-joint oligoarthritis |
| Systemic lupus erythematosus | Non-erosive arthropathy (Jaccoud arthropathy — reducible deformities), malar rash, renal disease, ANA and anti-dsDNA positive |
| Polyarticular gout | Podagra, tophi, hyperuricemia; joint aspiration shows negatively birefringent monosodium urate crystals; can mimic RA closely in late disease |
| Polyarticular pseudogout (CPPD) | Wrists, MCPs, knees; chondrocalcinosis on X-ray; positively birefringent calcium pyrophosphate crystals |
| Reactive arthritis | Asymmetrical oligoarthritis, preceding infection (GI or GU), enthesitis, conjunctivitis, urethritis |
| Osteoarthritis (erosive/inflammatory) | DIP and PIP involvement (Heberden and Bouchard nodes), brief morning stiffness, crepitus, non-inflammatory synovial fluid |
| Viral arthropathy (parvovirus B19, hepatitis B/C, rubella, chikungunya) | Acute onset, symmetrical, usually self-limiting; check parvovirus IgM, hepatitis serology in the right context |
| Polymyalgia rheumatica | Age above 50, proximal stiffness (shoulders and hips) more than peripheral arthritis, very high ESR, rapid steroid response |
The single most important investigation in any mono- or oligo-articular presentation is synovial fluid analysis — to exclude infection and crystal arthropathy. Never assume an inflamed joint in an RA patient is a flare without considering septic arthritis, which is 5 to 10 times more common in RA than in the general population. [1]
The treat-to-target management paradigm
Why treat-to-target works
The TICORA trial (Grigor et al., 2004) was the landmark evidence: patients managed with intensive, protocolised tight control — monthly assessment with DAS, and escalation of DMARD therapy if DAS remained above 2.4 — had significantly better outcomes (more remission, less radiographic damage, better function) than patients managed with routine, unstructured care [4]. This established that the strategy matters as much as the drugs: measure, set a target, escalate if not met.
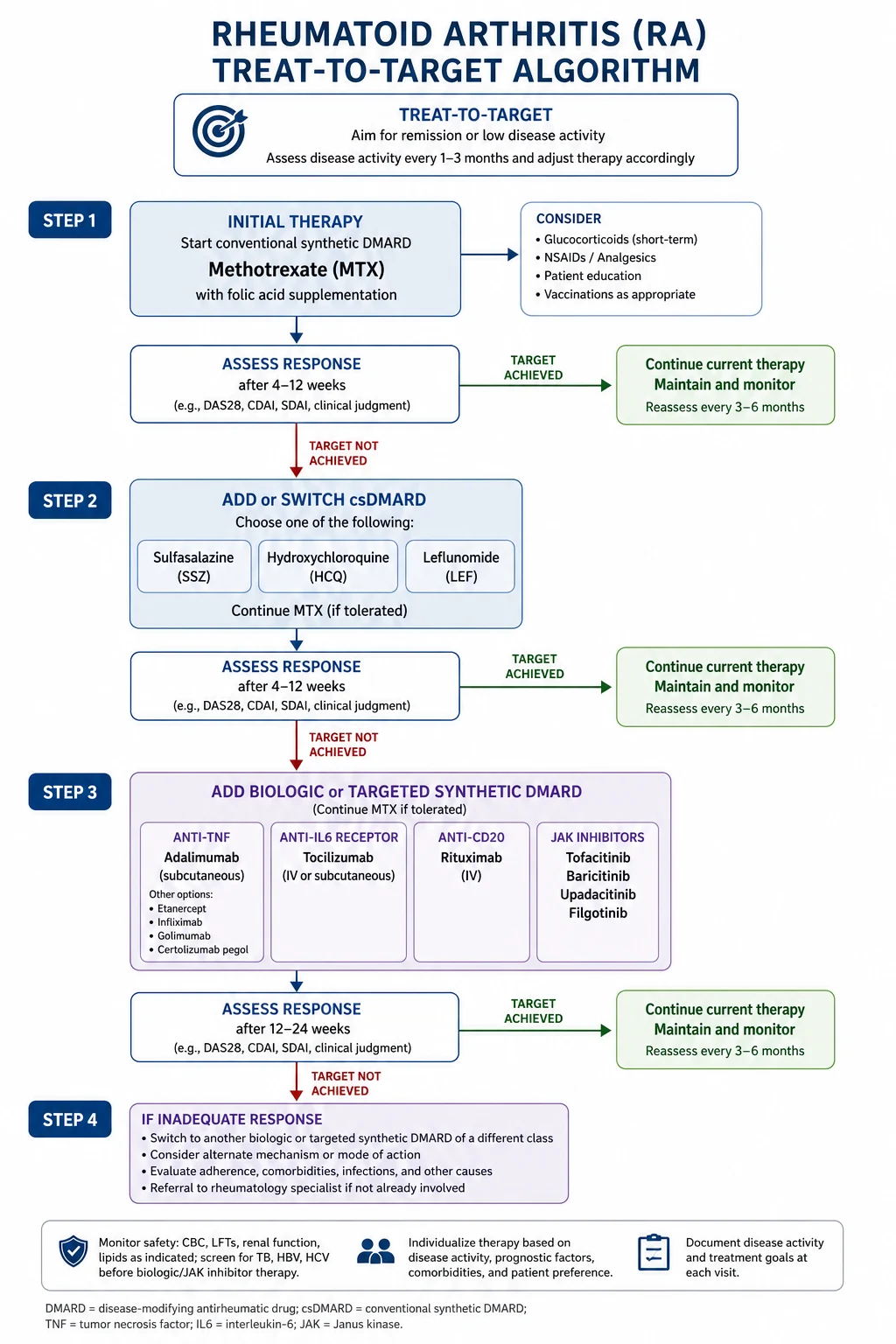
The international treat-to-target recommendations specify [3]:
- Target: remission (preferred) or low disease activity (acceptable, particularly in long-standing disease).
- Assessment: every 1 to 3 months during active disease, using a composite measure of disease activity that includes joint counts (DAS28, CDAI or SDAI).
- Escalation window: if the target is not reached within 3 months, or low disease activity is not reached within a maximum of 6 months, escalate therapy.
- Beyond the joints: comorbidity management (cardiovascular risk, osteoporosis, infection, psychological health) is integrated into every visit. [1]
Disease activity scores
| Score | Components | Interpretation |
|---|---|---|
| DAS28 (ESR or CRP) | 28 tender joints, 28 swollen joints, ESR/CRP, patient global (0 to 100 VAS) | Remission: below 2.6; Low: 2.6 to 3.2; Moderate: 3.2 to 5.1; High: above 5.1 |
| CDAI | Tender/s swollen count (28 joints), patient and physician global (0 to 10 VAS each) — no labs | Remission: 2.8 or below; Low: 2.9 to 10; Moderate: 10.1 to 22; High: above 22 |
| SDAI | Same as CDAI plus CRP | Remission: 3.3 or below; Low: 3.4 to 11; Moderate: 11.1 to 26; High: above 26 |
The newer Boolean remission definition is the strictest: tender joint count 1 or below, swollen joint count 1 or below, CRP 10 mg/L or below, patient global 1 or below (0 to 10 scale). [1]
Pharmacological management
Conventional synthetic DMARDs (csDMARDs)
Methotrexate is the anchor DMARD and first-line therapy for virtually all RA patients. It is given once weekly (this is critical — daily dosing causes fatal toxicity), starting at 10 to 15 mg orally once weekly, titrating up by 5 mg every 2 to 4 weeks to a target of 20 to 25 mg weekly (oral, or subcutaneous if oral absorption is poor or gastrointestinal side effects are limiting). Folate supplementation (5 mg once weekly, given on a different day to methotrexate, or 1 to 2 mg daily) reduces mucosal, hepatic and gastrointestinal toxicity without reducing efficacy. [1]
Why methotrexate first-line: it has the best efficacy-to-toxicity ratio of any DMARD, works within 4 to 8 weeks, can be combined with all biologics, and is inexpensive. The ATTRACT trial and decades of observational data show that methotrexate combined with a biologic is superior to either alone [5]. Approximately 30 per cent of patients achieve the treat-to-target goal on methotrexate monotherapy.
Monitoring methotrexate: full blood count, liver function tests and creatinine every 2 to 4 weeks for the first 3 months, then every 8 to 12 weeks. The main toxicities are:
- Hepatic: transaminitis; risk of fibrosis and cirrhosis with long-term use (monitor LFTs, consider transient elastography if persistent transaminase elevation). Avoid in significant alcohol intake or pre-existing liver disease.
- Haematological: marrow suppression (macrocytosis is an early warning). More common in renal impairment (methotrexate is renally cleared), folate deficiency and hypoalbuminaemia.
- Pulmonary: methotrexate pneumonitis — dry cough, dyspnoea, fever, diffuse infiltrates. This is an idiosyncratic reaction; stop the drug immediately and do not rechallenge.
- Mucosal: stomatitis, oral ulcers — mitigated by folate.
- Renal: reduced clearance in renal impairment increases toxicity; dose-reduce.
- Teratogenic: contraindicated in pregnancy. Both men and women must use reliable contraception and discontinue 3 to 6 months before conception. [1]
Other csDMARDs: [1]
| Drug | Dose | Key points | Monitoring |
|---|---|---|---|
| Sulfasalazine | 2 to 3 g orally daily (start low, titrate) | Useful in mild disease or combined with methotrexate; first-line in males (avoid in G6PD deficiency); can cause reversible male infertility (oligospermia) | FBC and LFTs every 1 to 2 months initially |
| Hydroxychloroquine | 200 to 400 mg orally daily | Mildest DMARD; ideal for mild disease or combination therapy; retinal toxicity (bull's-eye maculopathy) requires annual ophthalmology screening from 5 years (earlier if risk factors) | Annual ophthalmology review (baseline then annual after 5 years) |
| Leflunomide | 10 to 20 mg orally daily (loading dose 100 mg daily for 3 days optional but causes GI upset) | Similar efficacy to methotrexate; alternative if methotrexate not tolerated; very long half-life (active metabolite persists for up to 2 years); teratogenic — need washout with cholestyramine before pregnancy | FBC and LFTs and blood pressure regularly |
Triple therapy (methotrexate plus sulfasalazine plus hydroxychloroquine) is an evidence-based alternative to adding a biologic in patients with inadequate response to methotrexate monotherapy. The TEAR and RACAT trials showed triple therapy is non-inferior to anti-TNF plus methotrexate in many patients, though onset is slower. In ANZ practice, triple therapy is a reasonable option for patients with moderate disease activity, though many rheumatologists prefer biologic or JAK inhibitor escalation for higher disease activity. [1]
Biologic DMARDs (bDMARDs)
Biologics are added to (not substituted for) methotrexate when the treat-to-target goal is not met on csDMARD therapy. They transform disease control but are expensive (though now off-patent biosimilars are reducing cost) and carry infection risk. [1]
Anti-TNF agents (first-line biologic class): [1]
| Drug | Structure | Dose |
|---|---|---|
| Adalimumab | Fully human anti-TNF monoclonal antibody | 40 mg subcutaneously every 2 weeks |
| Infliximab | Chimeric anti-TNF monoclonal antibody | 3 mg/kg IV at weeks 0, 2, 6, then every 8 weeks |
| Certolizumab pegol | PEGylated anti-TNF Fab fragment (minimal placental transfer) | 400 mg subcutaneously at weeks 0, 2, 4, then 200 mg every 2 weeks |
| Golimumab | Fully human anti-TNF monoclonal antibody | 50 mg subcutaneously monthly |
The ATTRACT trial established infliximab's efficacy in methotrexate-inadequate responders [5]. Anti-TNF agents are broadly equivalent in efficacy; the choice depends on patient preference (self-injected versus infusion), comorbidities (certolizumab is preferred in pregnancy because it does not cross the placenta), and local funding.
Anti-TNF adverse effects and screening:
- Reactivation of latent tuberculosis — all patients need an IGRA (interferon-gamma release assay) and chest X-ray before starting. If latent TB, treat with prophylaxis (usually 3 to 4 months of rifampicin or 9 months of isoniazid) for at least 1 month before starting anti-TNF.
- Hepatitis B reactivation — screen for HBsAg and anti-HBc; treat prophylactically if positive.
- Hepatitis C — screen; co-management with hepatology.
- Serious infections — including atypical ( Legionella, Listeria, Pneumocystis) and opportunistic.
- Heart failure — avoid or use with caution in New York Heart Association class III or IV heart failure (TNF blockade can worsen heart failure).
- Demyelination — rare reports of multiple-sclerosis-like demyelinating events; avoid in patients with pre-existing demyelinating disease.
- Lupus-like syndrome — rare drug-induced lupus.
- Injection-site or infusion reactions. [1]
Anti-IL-6 receptor:
- Tocilizumab — humanised monoclonal antibody against the IL-6 receptor. Given as 8 mg/kg IV every 4 weeks or 162 mg subcutaneously every 1 to 2 weeks. The RADIATE trial demonstrated efficacy in patients refractory to anti-TNF [7]. Monitor for neutropenia, thrombocytopenia, hyperlipidaemia (check lipids 4 to 8 weeks after starting), elevated transaminases and bowel perforation (caution in patients with diverticular disease). Sarilumab is a similar subcutaneous agent.
- Key advantage: effective as monotherapy (methotrexate not required), useful when methotrexate is contraindicated.
Anti-CD20:
- Rituximab — chimeric monoclonal antibody against CD20 on B cells, causing B-cell depletion. Given as two 1000 mg IV infusions 2 weeks apart (with methylprednisolone premedication to reduce infusion reactions), repeated every 6 to 12 months. The REFLEX trial demonstrated efficacy in patients with inadequate response to anti-TNF [6].
- Key advantage: lower infection reactivation risk than anti-TNF — preferred in patients with latent TB, chronic hepatitis B (with antiviral prophylaxis), or previous lymphoma. Also the biologic of choice in RA-associated interstitial lung disease.
- Monitoring: CD19/CD20 B-cell counts (optional); immunoglobulins (monitor for hypogammaglobulinaemia with repeated courses); response to vaccines (reduced — vaccinate before treatment).
T-cell co-stimulation blockade:
- Abatacept — fusion protein (CTLA-4 extracellular domain fused to Fc of IgG1) that blocks CD28-CD80/86 co-stimulation, preventing T-cell activation. Given IV or subcutaneously. Useful in patients who have failed anti-TNF; also used as a first biologic in some guidelines. Generally well tolerated. [1]
Targeted synthetic DMARDs (tsDMARDs) — JAK inhibitors
JAK inhibitors are oral small molecules that block the JAK-STAT intracellular signalling pathway, thereby inhibiting multiple cytokine receptors simultaneously. [1]
| Drug | Target | Dose |
|---|---|---|
| Tofacitinib | JAK1/JAK3 (and to a lesser extent JAK2) | 5 mg orally twice daily (with methotrexate or as monotherapy); extended-release 11 mg once daily available |
| Baricitinib | JAK1/JAK2 | 2 to 4 mg orally daily |
| Upadacitinib | JAK1 selective | 15 mg orally daily |
The ORAL Solo trial demonstrated that tofacitinib monotherapy is effective in patients with inadequate response to DMARDs [8]. JAK inhibitors have rapid onset (days to weeks) and are as effective as anti-TNF agents. They are oral, which is an advantage for patients who dislike injections or infusions.
Safety — the ORAL Surveillance study: This is a critical exam topic. The ORAL Surveillance trial (Ytterberg et al., 2022) was a post-authorisation safety study comparing tofacitinib with anti-TNF in RA patients aged 50 or above with at least one cardiovascular risk factor. Tofacitinib did not meet non-inferiority for major adverse cardiovascular events (MACE) or malignancy — both were numerically higher with tofacitinib than with anti-TNF [9]. The study also showed increased rates of herpes zoster (including disseminated and CNS involvement), serious infections, and venous thromboembolism, particularly with the 10 mg twice-daily dose. This led to FDA and TGA boxed warnings for all JAK inhibitors (considered a class effect), and the recommendation to:
- Use JAK inhibitors with caution in patients above 50 years with cardiovascular or malignancy risk factors.
- Prefer anti-TNF or other biologics in this group.
- Offer herpes zoster vaccination (Shingrix, the non-live recombinant vaccine) before starting.
- Monitor lipids, full blood count, and liver function.
Tofacitinib is contraindicated in active serious infection, and should be avoided in chronic or recurrent infections. Shingrix (recombinant zoster vaccine) should be offered at least 2 weeks before initiation. [1]
Glucocorticoids — bridging, not backbone
Glucocorticoids are not disease-modifying — they suppress inflammation rapidly while waiting for DMARDs to take effect (typically 4 to 12 weeks for methotrexate). The role is strictly bridging therapy: [1]
- Intra-articular (triamcinolone, methylprednisolone) — for a single or few persistently active joints.
- Intramuscular (depot methylprednisolone 80 to 120 mg) — for a flare, or as bridge for 4 to 6 weeks.
- Oral (prednisolone 5 to 10 mg daily, or up to 30 mg for flares, tapered over 4 to 8 weeks) — short-term bridge.
- Intravenous pulse (methylprednisolone 500 mg to 1 g daily for 1 to 3 days) — for severe disease, organ-threatening vasculitis or scleritis. [1]
The exam trap: Long-term oral glucocorticoids cause osteoporosis (glucocorticoid-induced osteoporosis — offer a bisphosphonate or denosumab with calcium and vitamin D), diabetes, hypertension, cataracts, weight gain, skin thinning, adrenal suppression and increased infection risk. Every effort should be made to taper and stop glucocorticoids. The EULAR recommendation is to use the lowest dose for the shortest duration possible, and to aim for glucocorticoid-free remission. [1]
NSAIDs and simple analgesics
NSAIDs (e.g., naproxen 500 mg twice daily, ibuprofen 400 to 600 mg three times daily, celecoxib 100 to 200 mg twice daily) provide symptomatic relief of pain and stiffness but have no disease-modifying effect. They should be used at the lowest dose for the shortest time. Choose based on gastrointestinal, cardiovascular and renal risk: [1]- High GI risk: prefer a COX-2 selective (celecoxib) or add a proton pump inhibitor.
- High cardiovascular risk: avoid COX-2 selective and high-dose non-selective NSAIDs; naproxen has the best cardiovascular safety profile.
- Renal impairment: avoid or use with caution; NSAIDs reduce renal blood flow and can precipitate AKI. [1]
Paracetamol is less effective than NSAIDs for inflammatory pain but is safe for long-term use. [1]
Pre-biologic screening
Before starting any biologic DMARD or JAK inhibitor, perform the following screen: [1]
| Screen | Rationale |
|---|---|
| IGRA (QuantiFERON-TB Gold or T-SPOT.TB) and chest X-ray | Latent TB reactivation is the most feared biologic complication; anti-TNF carries the highest risk. Treat latent TB for at least 1 month before starting (rifampicin 4 months or isoniazid 9 months). Rituximab and JAK inhibitors have lower reactivation risk but screening is still recommended. |
| Hepatitis B serology (HBsAg, anti-HBs, anti-HBc) | Reactivation of chronic or resolved HBV is a risk with all biologics (especially rituximab, which can reactivate resolved HBV through profound B-cell depletion). Prophylactic antivirals (entecavir or tenofovir) if HBsAg positive; monitor if anti-HBc positive alone. |
| Hepatitis C serology (anti-HCV, and HCV RNA if positive) | Screen; co-manage with hepatology. Direct-acting antivirals can cure HCV, after which biologics are safe. |
| HIV | Screen. HIV is not an absolute contraindication to biologics if viral load is suppressed on antiretrovirals. |
| FBC, U&E, LFTs | Baseline; identify cytopenias, renal or hepatic dysfunction that affect drug choice. |
| Vaccinations | Ensure vaccinations are up to date BEFORE starting (biologics reduce vaccine immunogenicity). Specifically: influenza annually, pneumococcal (23-valent polysaccharide plus 13-valent conjugate), hepatitis B if non-immune, recombinant zoster (Shingrix) for those above 50 or about to start JAK inhibitors, COVID-19 boosters. Avoid live vaccines (MMR, yellow fever, oral polio, live zoster — Zostavax) once on biologics. |
| Cardiac assessment | Echocardiogram if heart failure suspected (anti-TNF caution in NYHA III/IV). |
| Lipids and HbA1c | Baseline, particularly before JAK inhibitors (which raise lipids). |
Comorbidities — the long-game
RA is not just about joints. The leading causes of death in RA are cardiovascular disease, infection, respiratory disease (RA-ILD) and malignancy (lymphoma). A DCE long case in an RA patient must address every comorbidity. [1]
Cardiovascular disease
RA is a coronary risk equivalent — patients with RA have approximately 50 per cent higher cardiovascular risk than the general population, comparable to diabetes mellitus [10]. This is driven by chronic systemic inflammation (atherosclerosis is an inflammatory disease), traditional risk factors (physical inactivity from joint disease, NSAID-related hypertension), and some treatments (glucocorticoids, NSAIDs, JAK inhibitors).
Management:
- Calculate cardiovascular risk at least annually using a validated risk calculator (Framingham, ASCVD or QRISK — note QRISK incorporates RA as a risk multiplier; Australian Absolute Cardiovascular Risk calculator includes "moderate or severe CKD and diabetes with albuminuria" but not RA explicitly, so clinical adjustment upward is needed).
- Treat hypertension aggressively (target 130/80 or below).
- Manage lipids to target (statin therapy for most RA patients over 40 with additional risk factors).
- Encourage smoking cessation — smoking both increases RA risk and severity, and is a conventional CV risk factor.
- Minimise glucocorticoid and NSAID exposure. [1]
Osteoporosis
RA patients have increased fracture risk from three sources: disease activity (osteoclast activation, systemic inflammation), immobility, and glucocorticoids. Glucocorticoid-induced osteoporosis is particularly important. All patients on glucocorticoids for 3 months or more should have:
- FRAX assessment (with glucocorticoid adjustment — the tool underestimates risk at prednisolone doses above 7.5 mg daily). [1]- Baseline and interval DEXA scans.
- Calcium (1000 mg daily) and vitamin D (800 to 1000 IU daily) supplementation.
- A bisphosphonate (e.g., alendronate 70 mg weekly, zoledronic acid 5 mg IV annually) or denosumab 60 mg subcutaneously every 6 months if at moderate or high fracture risk. Denosumab is preferred in renal impairment and glucocorticoid-induced osteoporosis by some guidelines. [1]
Infection risk
RA patients have increased infection risk from the disease itself (immunosuppression from chronic inflammation) and from immunosuppressive therapy. The risk is proportional to disease activity and to the intensity of immunosuppression. Biologics (especially anti-TNF and JAK inhibitors) increase the risk of serious bacterial infections, opportunistic infections (Pneumocystis, Listeria, Legionella, Salmonella), herpes zoster and TB. Every RA patient should have:
- Up-to-date vaccinations (as above, before biologics).
- A low threshold for investigating infection — RA patients may not mount a normal fever or inflammatory response.
- Always aspirate a disproportionately inflamed joint to exclude septic arthritis. [1]
Malignancy
RA is associated with a modestly increased risk of lymphoma (particularly diffuse large B-cell lymphoma) proportional to disease activity and duration — the inflammation drives lymphomagenesis. The relationship between biologics and malignancy is less clear — registry data have not consistently shown increased solid tumour risk with anti-TNF. The ORAL Surveillance study showed increased malignancy with tofacitinib in older patients with CV risk factors [9].
Psychological health
Depression and anxiety are 2 to 3 times more common in RA than in the general population, driven by chronic pain, fatigue, functional limitation and the psychological burden of a chronic disease. Screen at every visit (PHQ-9, GAD-7) and treat. [1]
Cervical spine in RA — the hidden danger
Atlantoaxial subluxation deserves special emphasis because it is the most commonly missed life-threatening complication of RA. It occurs in 10 to 20 per cent of patients with long-standing disease. [1]
When to suspect:
- Occipital headache (C2 nerve root).
- Lhermitte sign (electric shock down the spine on neck flexion).
- Progressive weakness or gait disturbance.
- Sensory changes in the hands (not explained by peripheral neuropathy or carpal tunnel).
- Urinary urgency or retention (early cord compression).
- Respiratory compromise from brainstem compression (late and dangerous). [1]
Assessment:
- Lateral cervical spine flexion and extension views: anterior atlantodental interval above 3 mm suggests subluxation; above 9 mm correlates with cord compression.
- MRI is the gold standard — it shows cord compression, signal change (myelomalacia) and pannus behind the dens. [1]
Management:
- Neurologically asymptomatic, mild subluxation: monitor with serial imaging; advise the patient to report neurological symptoms; avoid high-impact activities.
- Symptomatic or progressive subluxation: urgent neurosurgical or spinal orthopaedic referral for occipitocervical fusion.
- Before any general anaesthetic or intubation: lateral cervical spine flexion view or MRI to assess stability; use in-line stabilisation during intubation. [1]
Regional guideline deltas
| Aspect | ANZ (ARA) | UK (BSR, NICE) | US (ACR) |
|---|---|---|---|
| First-line DMARD | Methotrexate | Methotrexate | Methotrexate |
| Escalation | Triple therapy or biologic/JAK; bDMARD after csDMARD failure | Biologic (anti-TNF preferred) after csDMARD failure; triple therapy alternative | Triple therapy or biologic/JAK; JAK inhibitors with caution above 50 with CV risk |
| JAK inhibitor caution | TGA boxed warning; caution above 50 with CV/malignancy risk | MHRA guidance; prefer biologic in over-65s | FDA boxed warning; prefer anti-TNF in over-50 with CV risk |
| Biosimilars | Widely used for anti-TNF (reducing cost) | Mandated switch to biosimilars in many NHS trusts | Increasingly used |
The Australian Rheumatology Association (ARA) and NICE NG100 (Rheumatoid arthritis in adults: management) are broadly concordant with the EULAR recommendations. The ACR 2021 guideline prefers triple therapy to biologics as the first escalation step in some patients (unlike EULAR, which is more biologic-forward), but this is a nuance rather than a fundamental disagreement. [1]
Communication and shared decision-making
RA management is a lifelong partnership. Key communication points: [1]
-
Setting expectations: RA is a chronic disease that is now treatable but not curable. With modern therapy, 30 to 50 per cent of patients achieve sustained remission, and the majority achieve low disease activity. The goals are to prevent joint damage, maintain function and quality of life, and manage comorbidities. [1]
-
Explaining methotrexate: Address the "chemotherapy" misconception head-on — methotrexate is used in much lower doses for RA than for cancer, and it is the safest and most effective DMARD. Address the weekly dosing explicitly. Address folic acid. Address the alcohol question (low-risk drinking is acceptable; heavy drinking is not). [1]
-
Explaining biologics: Frame biologics as "targeted immunotherapies," not "immunosuppression." Discuss the infection risk, the need for screening, and the vaccinations. Discuss the route (self-injection versus infusion) and the cost/funding (PBS authority in ANZ; NHS in UK; insurance in US). [1]
-
Pregnancy: Address early — ideally before conception. Methotrexate and leflunomide are contraindicated in pregnancy (teratogenic — stop 3 to 6 months before). Sulfasalazine and hydroxychloroquine are safe. Anti-TNF (especially certolizumab, which does not cross the placenta, and adalimumab and infliximab, which are cleared from the neonatal circulation by 6 months) can be continued through pregnancy. Rituximab is avoided in the third trimester. JAK inhibitors are contraindicated. Maternal disease control in pregnancy is essential — active disease is worse for the baby than most well-chosen drugs. [1]
-
Flare plan: Give the patient a written flare plan — when to increase the DMARD, when to use glucocorticoids, when to call the rheumatology team, when to seek urgent care (for infection, new neurological symptoms, disproportionate joint pain suggesting sepsis). [1]
High-yield exam discriminators
- Anti-CCP is more specific than RF and predicts erosive disease. Always send both. Anti-CCP can be positive years before clinical disease [2].
- Morning stiffness more than one hour distinguishes inflammatory from mechanical arthritis (OA has stiffness lasting less than 30 minutes).
- DIPs are spared in RA. DIP involvement suggests osteoarthritis, psoriatic arthritis or gout.
- The 2010 ACR/EULAR criteria require a score of 6 or more out of 10, not a list of four-out-of-seven criteria (that was the 1987 version) [1].
- Methotrexate is given once weekly, not daily. Folic acid is given to reduce mucosal and hepatic toxicity.
- Always screen for latent TB (IGRA) before anti-TNF. Rituximab has lower TB reactivation risk.
- Rheumatoid pleural effusion has very low glucose (often below 1.4 mmol/L) — an exam favourite.
- ORAL Surveillance: tofacitinib carries higher MACE and malignancy risk than anti-TNF in patients above 50 with CV risk factors — prefer anti-TNF in this group [9].
- Felty syndrome = RA plus splenomegaly plus neutropenia. Recurrent sepsis is the danger.
- Caplan syndrome = rheumatoid pulmonary nodules plus pneumoconiosis.
- Secondary Sjogren syndrome (dry eyes, dry mouth in a patient with another autoimmune disease) is anti-Ro/anti-La negative, unlike primary Sjogren.
- RA is a coronary risk equivalent — cardiovascular risk management is mandatory, not optional [10].
- Atlantoaxial subluxation: always check the cervical spine before intubation in long-standing RA. Anterior atlantodental interval above 3 mm is abnormal; above 9 mm suggests cord compression.
- Pannus is invasive synovium — it destroys cartilage and bone through osteoclast activation (RANKL-driven) and MMPs.
- Treat-to-target with tight control (TICORA evidence) — measure every 1 to 3 months, escalate if target not met within 3 to 6 months [3][4].
Summary: the RA consultation in one paragraph
RA is a symmetrical small-joint polyarthritis driven by autoimmune synovitis (T-cell, B-cell, macrophage-mediated; TNF, IL-6, IL-1), producing pannus that erodes cartilage and bone. Diagnose using the 2010 ACR/EULAR criteria (joint count plus serology — RF and anti-CCP — plus acute-phase reactants plus duration, scoring 6 out of 10 or more), recognising that anti-CCP is the more specific serological marker. Image the hands, wrists and feet for erosions; use ultrasound or MRI for early disease. Manage with treat-to-target: methotrexate first-line, add sulfasalazine and hydroxychloroquine or escalate to a biologic (anti-TNF, anti-IL-6 receptor, anti-CD20, abatacept) or a JAK inhibitor if the target is not met within 3 to 6 months. Bridge with glucocorticoids but aim to stop them. Screen for TB, hepatitis and infection before biologics. Manage comorbidities proactively — cardiovascular disease (RA is a coronary risk equivalent), osteoporosis (glucocorticoid-induced), infection, interstitial lung disease, and cervical spine instability. Do not forget the patient as a whole: psychological health, function, work, pregnancy planning and shared decision-making are integrated into every consultation. [1]
References
- [1]Aletaha D, Neogi T, Silman AJ, et al. The 2010 American College of Rheumatology/European League Against Rheumatism classification criteria for rheumatoid arthritis: Phase 2 methodological report Arthritis Rheum, 2010.PMID 20872596
- [2]Nishimura K, Sugiyama D, Kogata Y, et al. Meta-analysis: diagnostic accuracy of anti-cyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritis Ann Intern Med, 2007.PMID 17548411
- [3]Smolen JS, Aletaha D, Bijlsma JW, et al. Treating rheumatoid arthritis to target: recommendations of an international task force Ann Rheum Dis, 2010.PMID 20215140
- [4]Grigor C, Capell H, Stirling A, et al. Effect of a treatment strategy of tight control for rheumatoid arthritis (the TICORA study): a single-blind randomised controlled trial Lancet, 2004.PMID 15262104
- [5]Maini R, St Clair EW, Breedveld F, et al. Infliximab (chimeric anti-tumour necrosis factor alpha monoclonal antibody) versus placebo in rheumatoid arthritis patients receiving concomitant methotrexate: a randomised phase III trial. ATTRACT Study Group Lancet, 1999.PMID 10622295
- [6]Cohen SB, Emery P, Greenwald MW, et al. Rituximab for rheumatoid arthritis refractory to anti-tumor necrosis factor therapy: Results of a multicenter, randomized, double-blind, placebo-controlled, phase III trial evaluating primary efficacy and safety at twenty-four weeks Arthritis Rheum, 2006.PMID 16947627
- [7]Emery P, Keystone E, Tony HP, et al. IL-6 receptor inhibition with tocilizumab improves treatment outcomes in patients with rheumatoid arthritis refractory to anti-tumour necrosis factor biologicals: results from a 24-week multicentre randomised placebo-controlled trial Ann Rheum Dis, 2008.PMID 18625622
- [8]Fleischmann R, Kremer J, Cush J, et al. Placebo-controlled trial of tofacitinib monotherapy in rheumatoid arthritis N Engl J Med, 2012.PMID 22873530
- [9]Ytterberg SR, Bhatt DL, Mikuls TR, et al. Cardiovascular and Cancer Risk with Tofacitinib in Rheumatoid Arthritis N Engl J Med, 2022.PMID 35081280
- [10]Avina-Zubieta JA, Thomas J, Sadatsafavi M, et al. Risk of incident cardiovascular events in patients with rheumatoid arthritis: a meta-analysis of observational studies Ann Rheum Dis, 2012.PMID 22425941
- [11]Klareskog L, Malmstrom V, Lundberg K, et al. Smoking, citrullination and genetic variability in the immunopathogenesis of rheumatoid arthritis Semin Immunol, 2011.PMID 21376627