Phys · rheumatological
Spondyloarthropathies
Also known as spondyloarthritis · spondyloarthropathy · ankylosing spondylitis · axial spondyloarthritis · non-radiographic axial spondyloarthritis · seronegative spondyloarthropathy · psoriatic arthritis · reactive arthritis · enteropathic arthritis · Reiter syndrome · SpA · axSpA · nr-axSpA
Consultant-physician-depth guide to the seronegative spondyloarthropathies — axial spondyloarthritis (ankylosing spondylitis, non-radiographic axSpA), psoriatic arthritis, reactive arthritis, and enteropathic arthritis — covering enthesitis-driven pathophysiology (HLA-B27, IL-23/IL-17 axis), inflammatory back pain recognition (Calin criteria, ASAS classification, MRI sacroiliitis), the modified New York criteria, BASDAI/BASFI/ASDAS, NSAIDs first-line, physiotherapy core, biologic DMARDs (TNF inhibitors, IL-17 inhibitors) and JAK inhibitors, plus extra-articular manifestations (uveitis, aortic regurgitation, apical fibrosis, amyloidosis) and the CASPAR/DAPSA framework for psoriatic arthritis — structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Spondyloarthropathies


The one-minute consultant answer
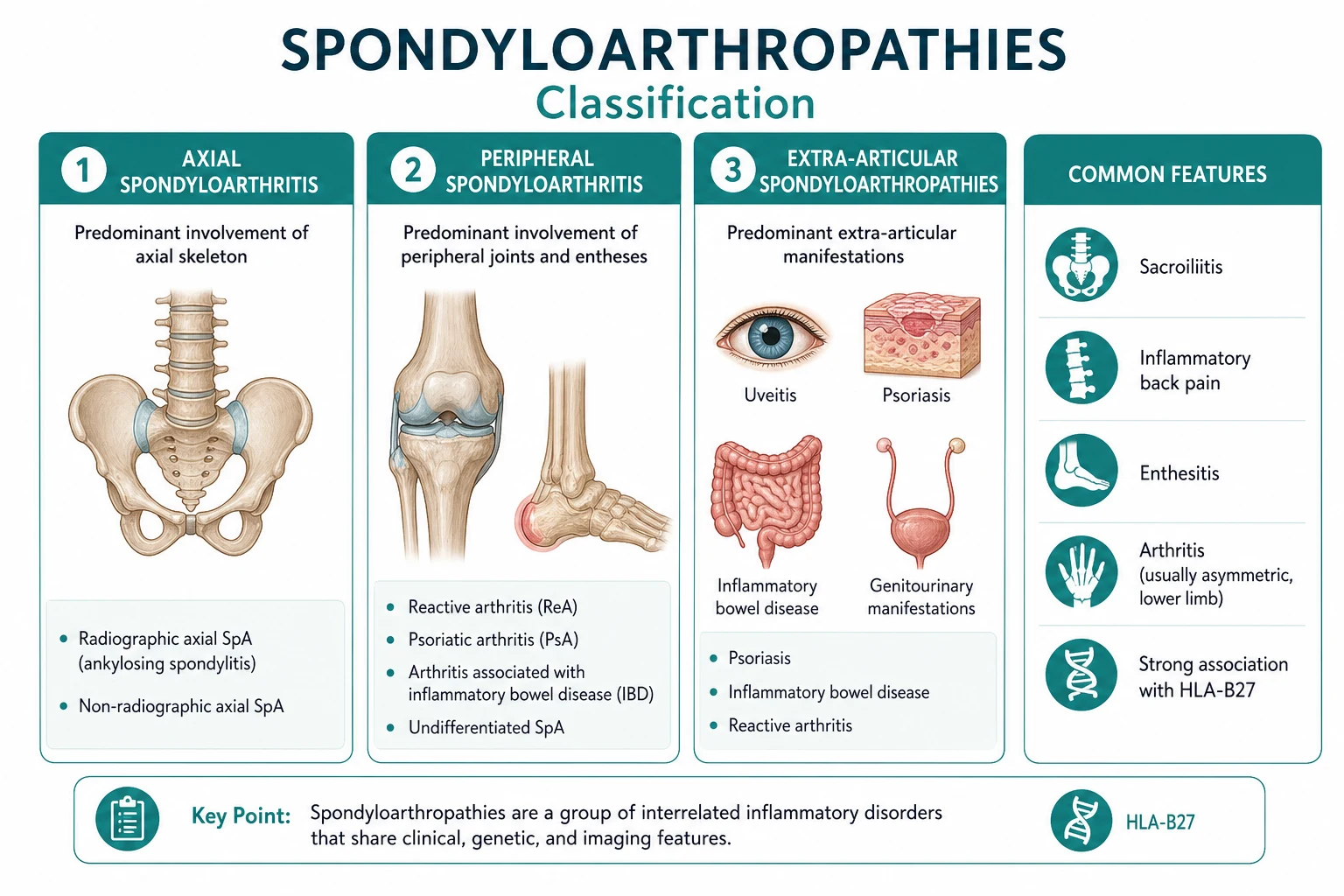
The spondyloarthropathies (SpA) are a family of interrelated inflammatory rheumatic diseases unified by four core features: inflammatory back pain, enthesitis (inflammation at the bone-tendon/ligament junction), the genetic marker HLA-B27, and an absence of rheumatoid factor (hence seronegative). The family includes ankylosing spondylitis (AS) and non-radiographic axial SpA (the axial subgroup), psoriatic arthritis (PsA), reactive arthritis, and enteropathic arthritis (associated with inflammatory bowel disease). The clinical hallmark is inflammatory back pain — insidious onset, age under 45, improving with exercise but not rest, alternating buttock pain, and morning stiffness over 30 minutes [6]. Diagnosis rests on the modified New York criteria for established AS (radiographic sacroiliitis plus one clinical criterion) [1] and the ASAS classification criteria for axial SpA (the imaging arm or the clinical arm, applied to chronic back pain with onset under 45) [2]. Management follows the ASAS-EULAR 2022 recommendations: NSAIDs at full dose are first-line, physiotherapy and exercise are the non-pharmacological core, and biologic DMARDs (TNF inhibitors or IL-17 inhibitors) are indicated when disease activity (ASDAS at least 2.1 or BASDAI at least 4) persists despite at least two NSAIDs [5]. JAK inhibitors (tofacitinib, upadacitinib) are approved after biologic failure [10]. Conventional synthetic DMARDs (sulfasalazine, methotrexate) are ineffective for pure axial disease but useful for peripheral arthritis.
Pathophysiology — why SpA does what it does
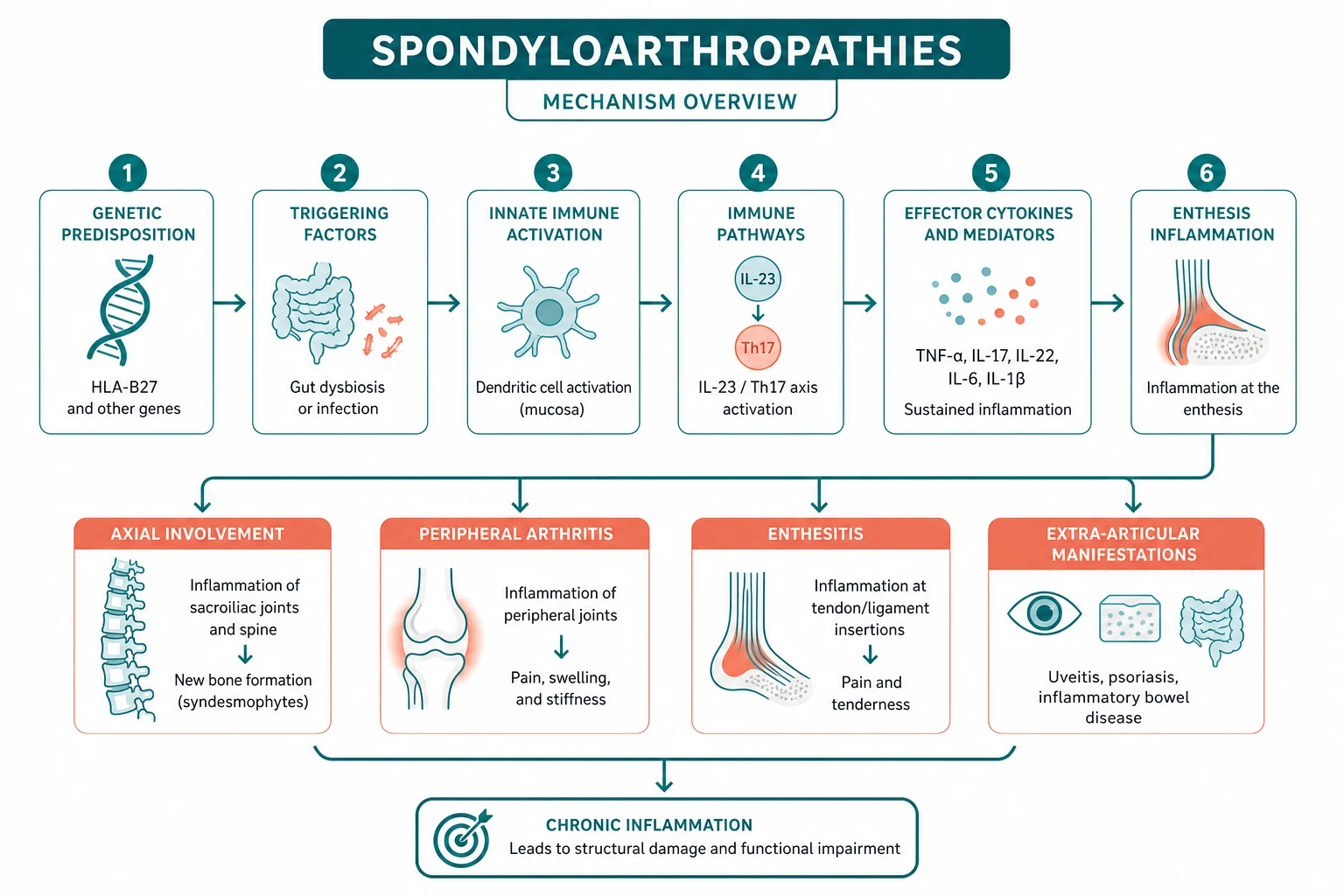
Understanding the immunopathogenesis transforms every management decision — from NSAID selection to biologic class choice. The key insight: the primary lesion in SpA is enthesitis, not synovitis. This is the fundamental distinction from rheumatoid arthritis. [1]
The enthesis — where it all begins
The enthesis is the site where tendon, ligament or joint capsule inserts into bone. In SpA, this is where inflammation starts. Enthesitis produces the characteristic heel pain (Achilles tendon insertion and plantar fascia origin), the dactylitis (sausage digit from combined enthesitis and synovitis along a digit), and the syndesmophytes (new bone formation at the vertebral enthesis). The enthesis is rich in fibrocartilage and subject to mechanical stress, which may explain why SpA targets the axial skeleton and lower limbs. [1]
The inflammatory process follows a predictable cycle: acute inflammation produces erosion at the enthesis, followed by repair with fibrocartilage, and then enchondral ossification — new bone formation. This is why the spine stiffens over years: the same inflammatory cascade that causes pain also produces syndesmophytes that eventually bridge vertebrae to form the bamboo spine [6].
HLA-B27 — the dominant genetic factor
HLA-B27 is the strongest genetic association in any rheumatic disease. It is present in approximately 90 per cent of patients with ankylosing spondylitis, 70 per cent of reactive arthritis, and 50 per cent of psoriatic arthritis with axial involvement — compared with about 8 per cent of the general population. Two leading hypotheses explain the association: [1]
- The arthritogenic peptide hypothesis: HLA-B27 presents specific peptides (from bacteria or self) to CD8+ cytotoxic T cells, triggering an autoimmune response against joint tissues.
- The unfolded protein response (UPR) hypothesis: HLA-B27 misfolds in the endoplasmic reticulum, activating the UPR and promoting IL-23 production and inflammation. [1]
HLA-B27 is necessary but not sufficient — only a minority of HLA-B27-positive individuals develop SpA, indicating that additional genetic and environmental factors (gut microbiome, mechanical stress, infection) are required. [1]
The IL-23/IL-17 immune axis
The IL-23/IL-17 axis is the central cytokine pathway in SpA [6]. IL-23, produced by dendritic cells and macrophages, activates Th17 cells and innate immune cells (gamma-delta T cells, MAIT cells, group 3 innate lymphoid cells) to produce IL-17A. IL-17A drives enthesitis, inflammation, and pathological new bone formation.
This pathway explains the efficacy of both drug classes that target it:
- IL-17 inhibitors (secukinumab, ixekizumab) block IL-17A directly, providing dramatic relief of both axial and peripheral symptoms and skin disease (in PsA) [4].
- TNF inhibitors block upstream amplification but do not fully suppress IL-17-driven new bone formation — this may explain why syndesmophytes can continue to form even on effective TNF blockade.
Triggering infections in reactive arthritis
Reactive arthritis follows a triggering infection 1 to 4 weeks before onset. The classical triggers:
- Genitourinary: Chlamydia trachomatis (the most common, typically post-STI)
- Gastrointestinal: Salmonella, Shigella, Campylobacter jejuni, Yersinia enterocolitica (post-enteric); occasionally Clostridioides difficile and Giardia lamblia [1]
The mechanism involves molecular mimicry (bacterial antigens cross-reacting with self) and persistent antigen in the joint. The Reiter triad of urethritis, conjunctivitis and arthritis (formerly called Reiter syndrome) is now uncommon — most patients present with asymmetrical oligoarthritis alone. [1]
Clinical features — the full spectrum
Inflammatory back pain — the cardinal axial symptom
The recognition of inflammatory back pain is the single most important clinical skill in SpA. The Calin criteria screen for it using five features (4 of 5 gives approximately 75 per cent sensitivity and specificity in a rheumatology clinic): [1]
- Age of onset under 40 years
- Insidious onset (over weeks to months)
- Improvement with exercise
- No improvement with rest
- Night pain (often second half of the night, improving on rising) [1]
The Berlin criteria add alternating buttock pain as a sixth feature. The key discriminating point from mechanical back pain: SpA pain improves with activity and worsens with rest, the opposite of mechanical pain. [1]
Exam trap: Inflammatory back pain is commonly missed for years — the average diagnostic delay is 6 to 8 years. Any young person with chronic back pain that improves with exercise and has morning stiffness should be evaluated for SpA, not dismissed as muscular. [1]
Enthesitis and dactylitis — the SpA signatures
Enthesitis — tenderness at tendon or ligament insertions — is the pathological hallmark. The most clinically important sites:
- Achilles tendon insertion — posterior heel pain, tenderness, sometimes swelling
- Plantar fascia origin (calcaneal tuberosity) — plantar heel pain, worst on first steps in the morning
- Tibial tuberosity, patellar tendon, iliac crest, ischial tuberosity, greater trochanter — less common but identifiable [1]
Dactylitis — diffuse swelling of an entire digit (finger or toe), producing the classic sausage digit — results from simultaneous enthesitis and synovitis along the digit. It is pathognomonic for SpA, particularly psoriatic and reactive arthritis. [1]
Peripheral arthritis — the asymmetrical lower-limb pattern
The peripheral arthritis of SpA is characteristically asymmetrical and oligoarticular, targeting the lower limbs (knees, ankles, hips). This is the mirror image of rheumatoid arthritis (symmetrical, polyarticular, small joints of hands, upper limbs). In psoriatic arthritis, the pattern is more diverse (see below). [1]
Extra-articular manifestations — SpA is a systemic disease
| System | Manifestation | Key features |
|---|---|---|
| Eye | Acute anterior uveitis (iritis) | Unilateral, painful red eye, photophobia, blurred vision; 25 to 40 per cent of AS; recurrent; urgent ophthalmology |
| Cardiac | Aortic regurgitation, conduction disease | Aortitis of the aortic root (1 to 10 per cent); first-degree AV block; may need valve replacement |
| Pulmonary | Apical pulmonary fibrosis | Upper-lobe interstitial disease with cavitation; mimics TB; occurs in advanced disease |
| Renal | AA amyloidosis, IgA nephropathy | Nephrotic syndrome from chronic inflammation; less common with biologic therapy |
| Bone | Osteoporosis, vertebral fracture | Inflammatory and immobility-driven; the fused spine is brittle |
| Neurological | Atlantoaxial subluxation, cauda equina | Rare but serious; dural ectasia can compress nerve roots |
| Skin/nails | Psoriasis, nail dystrophy (PsA) | Pitting, onycholysis, hyperkeratosis, oil-drop sign |
Psoriatic arthritis — a distinct subtype
Psoriatic arthritis occurs in approximately 30 per cent of patients with psoriasis. It is the most heterogeneous of the SpA subtypes, with five classical patterns (the Moll and Wright classification): [1]
- Asymmetrical oligoarthritis (most common, 70 per cent) — fewer than five joints, often DIPs, PIPs, MCPs, knees; with dactylitis
- Symmetrical polyarthritis (RA-like, 15 per cent) — clinically indistinguishable from RA except RF is negative and DIPs are involved
- DIP-predominant (5 per cent) — with nail changes; highly characteristic
- Arthritis mutilans (rare) — destructive, opera-glass hand, telescoping digits
- Spondylitis (5 to 20 per cent) — axial disease with or without peripheral arthritis [1]
CASPAR classification criteria
The CASPAR criteria (Taylor et al., 2006) classify PsA in a patient with established inflammatory articular disease (joint, spine or entheseal) using a point system — a score of 3 or more classifies PsA [3]:
| Feature | Points |
|---|---|
| Current psoriasis | 2 |
| Personal history of psoriasis (if current not present) | 1 |
| Family history of psoriasis (if current/personal not present) | 1 |
| Psoriatic nail dystrophy (pitting, onycholysis, hyperkeratosis) | 1 |
| Negative rheumatoid factor | 1 |
| Dactylitis (current or history) | 1 |
| Radiographic juxta-articular new bone formation | 1 |
The CASPAR criteria have a sensitivity of 91 per cent and specificity of 99 per cent — the highest of any SpA classification system. Current psoriasis is the only feature worth 2 points. [1]
Nail changes — the diagnostic clue
Psoriatic nail changes are present in over 80 per cent of patients with PsA and are a key diagnostic clue. The patterns:
- Pitting — small depressions in the nail plate (most common)
- Onycholysis — separation of the nail plate from the nail bed (oil-drop sign)
- Hyperkeratosis — thickening under the nail (subungual)
- Nail dystrophy — ridging, crumbling, destruction [1]
Always examine the nails of any patient with inflammatory arthritis — and look for hidden psoriasis in the scalp (behind the ears), umbilicus, natal cleft, and extensor surfaces (elbows, knees). [1]
DAPSA — disease activity in PsA
The Disease Activity index for Psoriatic Arthritis (DAPSA) is the preferred composite score for peripheral PsA activity. It sums: tender joint count (0 to 68), swollen joint count (0 to 66), patient pain VAS (0 to 10), patient global activity VAS (0 to 10), and CRP (mg/dL). [1]
| DAPSA score | Category |
|---|---|
| 0 to 3.9 | Remission |
| 4.0 to 13.9 | Low disease activity |
| 14.0 to 27.9 | Moderate disease activity |
| 28 or above | High disease activity |
A DAPSA of 4 or below is the treatment target (remission or low disease activity). [1]
Reactive arthritis — the post-infectious subtype
Reactive arthritis is sterile arthritis occurring 1 to 4 weeks after a genitourinary or gastrointestinal infection. The classical Reiter triad of urethritis, conjunctivitis and arthritis (can't see, can't pee, can't climb a tree) is now uncommon — most patients present with asymmetrical oligoarthritis of the lower limbs, with or without enthesitis and dactylitis. [1]
Triggering organisms:
- GU: Chlamydia trachomatis (most common)
- GI: Salmonella, Shigella, Campylobacter jejuni, Yersinia enterocolitica
- Less common: Clostridioides difficile, Giardia lamblia, Ureaplasma [1]
Clinical features:
- Asymmetrical lower-limb oligoarthritis (knees, ankles) — the key pattern
- Enthesitis (Achilles, plantar fascia)
- Dactylitis (sausage digits)
- Mucocutaneous: circinate balanitis (painless penile lesions), keratoderma blennorrhagicum (pustular lesions on palms and soles)
- Ocular: conjunctivitis (usually mild), acute anterior uveitis (less common than in AS)
- Urethritis (in chlamydia-triggered disease) [1]
Course: Reactive arthritis is usually self-limiting, resolving within 3 to 12 months in the majority. However, approximately 30 to 50 per cent develop chronic or recurrent disease, and some progress to ankylosing spondylitis. HLA-B27 positivity predicts a more severe and chronic course. [1]
Management: Treat the triggering infection (if identified — e.g., chlamydia with azithromycin or doxycycline, though antibiotic treatment after the arthritis has begun does not clearly alter the course). NSAIDs for symptom control. Intra-articular corticosteroid injections for persistent monoarthritis. Sulfasalazine for persistent disease over 6 months. Biologics (TNFi) for refractory disease. [1]
Enteropathic arthritis — the IBD-associated subtype
Inflammatory bowel disease (Crohn disease, ulcerative colitis) is associated with two distinct arthritis patterns: [1]
Type 1 peripheral arthritis — pauciarticular (fewer than five joints), asymmetrical, involving large joints (knees, ankles). It mirrors bowel disease activity — flares with gut inflammation and resolves with effective IBD treatment. Self-limiting, usually non-erosive. [1]
Type 2 peripheral arthritis — polyarticular, symmetrical, involving small joints of the hands. It is independent of bowel disease activity — does not resolve with IBD treatment. More chronic and potentially erosive. [1]
Axial disease — sacroiliitis and spondylitis. Independent of bowel disease activity. Clinically and radiographically identical to primary AS. Occurs in 10 to 20 per cent of IBD patients. [1]
Management: TNF inhibitors are the key therapy — but choose carefully. Monoclonal antibody TNFi (adalimumab, infliximab, certolizumab, golimumab) treat both gut and joints. Etanercept (fusion protein) is effective for joints but ineffective for IBD and may even exacerbate gut inflammation. IL-17 inhibitors may worsen IBD and should be avoided. [1]
Diagnosis and classification
The modified New York criteria (1984) — for established AS
The modified New York criteria (van der Linden et al., 1984) remain the standard for diagnosing established (radiographic) ankylosing spondylitis [1]:
Diagnosis requires: radiographic sacroiliitis (grade 2 bilateral or grade 3 to 4 unilateral) plus at least one clinical criterion: [1]
- Low back pain and stiffness for more than 3 months that improves with exercise but not rest
- Limited lumbar spine motion in sagittal and frontal planes
- Limited chest expansion relative to normal values corrected for age and sex
- History of iritis, psoriasis, or chronic inflammatory bowel disease (or evidence of these on examination) [1]
The limitation: the mNY criteria require radiographic sacroiliitis, which develops years after symptom onset. This is why the average diagnostic delay is 6 to 8 years. [1]
The ASAS classification criteria (2009) — for early and non-radiographic disease
The ASAS axial SpA criteria (Rudwaleit et al., 2009) were developed to enable earlier diagnosis, before radiographic damage appears [2]. They apply to patients with chronic back pain (over 3 months) and onset under 45 years.
A patient is classified as having axial SpA if they satisfy either arm: [1]
Imaging arm: Sacroiliitis on imaging (radiography — grade 2 bilateral or grade 3 to 4 unilateral; OR MRI showing active inflammation) plus at least 1 SpA feature. [1]
Clinical arm: HLA-B27 positive plus at least 2 SpA features. [1]
SpA features (common to both arms): inflammatory back pain, arthritis, enthesitis (heel), uveitis, dactylitis, psoriasis, Crohn disease or ulcerative colitis, good response to NSAIDs, family history of SpA, HLA-B27, elevated CRP. [1]
Exam trap: The ASAS criteria are classification criteria, not strict diagnostic criteria. They perform well in early SpA populations but have reduced specificity in back pain clinics. Clinical judgment and rheumatology referral remain essential. [1]
MRI — the key investigation for non-radiographic axSpA
MRI of the sacroiliac joints detects active inflammatory sacroiliitis years before it appears on plain radiographs. The key finding is bone marrow oedema — high signal on STIR (short tau inversion recovery) or T2 fat-saturated sequences, indicating osteitis. The ASAS definition requires bone marrow oedema on at least two consecutive slices or more than one lesion on a single slice. [1]
MRI has transformed the diagnostic landscape — patients who would have waited years for radiographic changes can now be diagnosed and treated early. The modified New York criteria require X-ray sacroiliitis; the ASAS criteria allow MRI sacroiliitis (in the imaging arm). [1]
Plain radiographs — the classical progression
The radiographic sequence of AS is examinable and follows a predictable course: [1]
- Sacroiliitis — the earliest finding: blurring of the subchondral bone plate, erosions ("pseudo-widening" of the joint space), sclerosis (especially iliac side), and eventually complete fusion (ankylosis). Graded 0 to 4 bilaterally.
- Vertebral body squaring — erosion of the anterior corners of vertebral bodies, producing a squared profile (loss of the normal concave anterior surface).
- Syndesmophytes — delicate bony bridges forming at the margins of the discovertebral junction, growing vertically along the annulus fibrosus. These are distinct from the bulky, horizontal osteophytes of degenerative disease.
- Bamboo spine — syndesmophytes bridging consecutive vertebrae, giving the spine a bamboo-like appearance on lateral X-ray. This is the classical late finding.
- Dagger sign — ossification of the interspinous and supraspinous ligaments, producing a central vertical density on the AP view. [1]
HLA-B27 — supportive but never diagnostic alone
HLA-B27 testing supports the diagnosis (the ASAS clinical arm) but should never be used as a stand-alone test. It has a sensitivity of approximately 90 per cent for AS but a specificity of only about 25 per cent (because 8 per cent of the general population are positive). A positive result in a patient with inflammatory back pain increases the post-test probability; a negative result reduces it but does not exclude AS. [1]
Inflammatory markers
CRP is elevated in approximately 50 to 70 per cent of patients with active AS and is a better predictor of radiographic progression than ESR. However, normal inflammatory markers do not exclude active SpA — a significant proportion of patients with active disease have normal CRP and ESR. Use composite clinical scores (ASDAS, BASDAI) for disease activity assessment. [1]
Disease activity assessment
| Score | Components | Interpretation |
|---|---|---|
| BASDAI | 6 VAS questions (fatigue, spinal pain, joint pain, enthesitis, morning stiffness duration, morning stiffness severity) | 0 to 10 scale; 4 or above indicates active disease (threshold for biologic) |
| BASFI | 10 VAS questions on functional ability (reaching, bending, dressing, stairs) | 0 to 10 scale; measures functional limitation |
| ASDAS | Back pain, duration of morning stiffness, patient global, peripheral pain/swelling, plus CRP (ASDAS-CRP) or ESR (ASDAS-ESR) | Below 1.3 inactive; 1.3 to 2.1 moderate; 2.1 to 3.5 high; above 3.5 very high |
| DAPSA (PsA) | Tender joints, swollen joints, patient pain, patient global, CRP | Below 4 remission/low; 4 to 14 low; 14 to 28 moderate; 28+ high |
ASDAS is preferred over BASDAI because it incorporates CRP/ESR and correlates better with radiographic progression. The ASAS-EULAR 2022 recommendations use ASDAS 2.1 or above as the threshold for biologic escalation [5].
Management — the treatment ladder
Step 1: NSAIDs — the foundation
NSAIDs are the first-line and most important pharmacological treatment for axial SpA, as confirmed by the ASAS-EULAR 2022 and ACR 2019 recommendations [5][12]. Use at full anti-inflammatory dose (not analgesic dose):
| NSAID | Anti-inflammatory dose | Key points |
|---|---|---|
| Naproxen | 500 mg twice daily | Best cardiovascular safety profile |
| Celecoxib | 200 mg twice daily | COX-2 selective; better GI profile; cardiovascular caution |
| Ibuprofen | 400 to 800 mg three times daily | Often under-dosed; needs 2.4 g/day for anti-inflammatory effect |
| Indomethacin | 25 to 50 mg three times daily | Historically first-line; effective but poorly tolerated (GI, CNS) |
| Meloxicam | 15 mg daily | Once daily; moderate COX-2 selectivity |
The Poddubnyy cohort study showed that high NSAID intake over 2 years is associated with retarded radiographic progression in AS, particularly in patients with baseline syndesmophytes and elevated CRP [9]. This provides a rationale for continuous (rather than on-demand) dosing in active disease, even though the evidence is observational.
Choosing the right NSAID: Assess gastrointestinal risk (consider a proton pump inhibitor or COX-2 selective), cardiovascular risk (naproxen preferred), and renal function (avoid or caution in CKD). If one NSAID is ineffective, try another — there is individual variation in response. [1]
Step 2: Physiotherapy and exercise — the non-pharmacological core
Physiotherapy and exercise are as essential as any drug in SpA management. The ASAS-EULAR recommendations state that all patients should have access to physiotherapy [5]. Evidence shows:
- Supervised group exercise is superior to home exercise for spinal mobility and function
- Strengthening and stretching exercises maintain posture and reduce stiffness
- Swimming is ideal — low-impact, promotes extension and rotation
- Daily postural exercises prevent the progressive flexion deformity of advanced AS [1]- Deep breathing exercises maintain chest expansion
Patients should understand that exercise is treatment, not optional. This is one of the most important messages in the SpA consultation. [1]
Step 3: Conventional DMARDs — only for peripheral disease
Conventional synthetic DMARDs (csDMARDs) are ineffective for pure axial disease — this is one of the most important exam points in SpA. The ASAS-EULAR recommendations explicitly state that csDMARDs are not recommended for axial symptoms [5]. They may be used for:
- Peripheral arthritis (especially knee or hip involvement) — sulfasalazine 2 to 3 g daily is the first choice
- Psoriatic arthritis with polyarticular disease — methotrexate 15 to 25 mg weekly, sulfasalazine, or leflunomide
- Persistent reactive arthritis over 6 months — sulfasalazine
Exam trap: Prescribing methotrexate or sulfasalazine for a patient with pure axial SpA (no peripheral arthritis) is a classic error. csDMARDs will not help the spinal symptoms. [1]
Step 4: Biologic DMARDs — TNF inhibitors and IL-17 inhibitors
Biologics are indicated when disease activity (ASDAS at least 2.1 or BASDAI at least 4) persists despite a therapeutic trial of at least two NSAIDs over 4 weeks [5][12].
TNF inhibitors (first-line biologic class): [1]
| Drug | Structure | Dose | Key points |
|---|---|---|---|
| Adalimumab | Fully human anti-TNF mAb | 40 mg SC every 2 weeks | Effective for axial, peripheral, uveitis, PsA, IBD; preferred in pregnancy (certolizumab preferred) |
| Infliximab | Chimeric anti-TNF mAb | 5 mg/kg IV at weeks 0, 2, 6, then every 6 to 8 weeks | Effective for all manifestations; infusion reactions |
| Certolizumab pegol | PEGylated anti-TNF Fab fragment | 400 mg SC weeks 0, 2, 4, then 200 mg every 2 weeks | Minimal placental transfer (preferred in pregnancy) |
| Golimumab | Fully human anti-TNF mAb | 50 mg SC monthly | Once monthly dosing convenience |
The landmark trials: Gorman et al. (2002) showed etanercept's efficacy in AS [7]; Braun et al. (2002) showed infliximab's efficacy [8]. These two NEJM/Lancet papers established the TNF-blockade paradigm in SpA.
TNF inhibitor adverse effects and screening: The same as for RA — latent TB screening (IGRA plus chest X-ray), HBV/HCV serology, vaccination update, and counselling on infection risk. Etanercept is specifically ineffective for uveitis and may paradoxically worsen it — use a monoclonal antibody TNFi (adalimumab, infliximab) or an IL-17i for patients with recurrent uveitis. [1]
IL-17 inhibitors (alternative first-line biologic): [1]
| Drug | Structure | Dose | Key points |
|---|---|---|---|
| Secukinumab | Fully human anti-IL-17A mAb | 150 mg SC weekly for 4 weeks, then monthly | MEASURE 1: ASAS20 in 60 per cent at week 16 vs 29 per cent placebo [4]; also for PsA; caution in IBD |
| Ixekizumab | Humanised anti-IL-17A mAb | 160 mg SC loading, then 80 mg every 2 weeks for 6 weeks, then monthly | COAST trials in AS; also for PsA; caution in IBD |
IL-17 inhibitors are as effective as TNFi for axial and peripheral SpA, and are particularly useful in patients with co-existing psoriasis (where they also clear skin disease). However, they can exacerbate inflammatory bowel disease — avoid in patients with Crohn disease or ulcerative colitis. [1]
IL-23 inhibitors in PsA: Ustekinumab (anti-IL-12/23 p40) and guselkumab (anti-IL-23 p19) are effective for psoriatic arthritis and psoriasis but are NOT approved for axial SpA. This is an important distinction — IL-23 blockade works for the skin and peripheral joints of PsA but not for the axial skeleton, despite IL-23 being central to SpA pathogenesis. The failure of IL-23i in axial SpA trials is one of the great paradoxes of modern rheumatology. [1]
Step 5: JAK inhibitors — after biologic failure
JAK inhibitors are approved for AS after inadequate response to at least one biologic. The Deodhar et al. phase 3 trial (2021) showed tofacitinib 5 mg twice daily achieved ASAS20 in 56 per cent versus 29 per cent placebo at week 16 [10]. Upadacitinib is also approved.
Caution: Apply the same cardiovascular and malignancy caution as in RA (ORAL Surveillance data) for patients over 50 with cardiovascular risk factors. Screen for herpes zoster and offer Shingrix before starting. [1]
Glucocorticoids — limited role
Unlike RA, glucocorticoids have a very limited role in SpA. Systemic glucocorticoids are not recommended for axial SpA — the ASAS-EULAR recommendations explicitly discourage long-term systemic glucocorticoid use [5]. Local (intra-articular or intralesional) corticosteroid injections are useful for:
- Persistent peripheral monoarthritis (e.g., a single inflamed knee)
- Enthesitis injections (though evidence is limited)
- Intraocular corticosteroids for uveitis (ophthalmology-managed)
Exam trap: Prescribing oral prednisolone for axial SpA is a classic error. Unlike RA, where bridging glucocorticoids are standard, they have no role in pure axial disease. [1]
Pre-biologic screening
The pre-biologic screen is the same as for RA biologics and is non-negotiable: [1]
| Screen | Rationale |
|---|---|
| IGRA + chest X-ray | Latent TB reactivation is highest with monoclonal antibody TNFi; treat with rifampicin 4 months or isoniazid 9 months for at least 1 month before starting |
| HBV serology (HBsAg, anti-HBs, anti-HBc) | Reactivation risk, especially with rituximab; prophylactic antivirals if positive |
| HCV serology | Screen; co-manage with hepatology |
| HIV | Screen |
| FBC, U&E, LFTs | Baseline |
| Vaccinations | Up to date BEFORE starting — influenza, pneumococcal, hepatitis B, recombinant zoster (Shingrix), COVID-19; avoid live vaccines once on biologics |
| Cardiac assessment | TNFi caution in NYHA III/IV heart failure |
Extra-articular management — the multisystem disease
Acute anterior uveitis
Uveitis is the most common extra-articular manifestation of AS (25 to 40 per cent). It presents as a unilateral, painful, red eye with photophobia, lacrimation and blurred vision. It is not conjunctivitis (which is painless, bilateral and gritty). The patient needs same-day ophthalmology for slit-lamp examination and topical corticosteroids. Recurrent attacks cause posterior synechiae, cataract, and glaucoma. [1]
Pharmacological prevention: Monoclonal antibody TNFi (adalimumab, infliximab) reduce uveitis recurrence. Etanercept does not prevent uveitis and may worsen it. IL-17i (secukinumab) have a modest uveitis-reducing effect. [1]
Aortic regurgitation and conduction disease
Aortitis involving the aortic root produces aortic regurgitation in 1 to 10 per cent of patients with long-standing AS. Conduction abnormalities (first-degree AV block, occasionally higher-grade block requiring pacing) occur. A routine echocardiogram and ECG should be part of the long-term assessment in established disease, with a low threshold for cardiology referral if a new murmur or conduction abnormality is detected. [1]
Apical pulmonary fibrosis
Upper-lobe interstitial disease with pleural thickening, cavitation and nodularity occurs in advanced long-standing AS. It mimics tuberculosis and can produce restrictive lung disease. The mechanism is pleuropulmonary inflammation analogous to the enthesitis of the axial skeleton. Baseline and periodic pulmonary function tests and chest imaging are appropriate in advanced disease. [1]
Amyloidosis
Secondary (AA) amyloidosis, from decades of untreated chronic inflammation, causes nephrotic syndrome and progressive renal failure. It is now much less common with effective biologic therapy but remains a risk in long-standing, poorly controlled disease. Check urinalysis for proteinuria at least annually in established AS. [1]
Osteoporosis and spinal fracture
The fused spine is osteoporotic and brittle. Even minor trauma — a fall from standing height — can cause an unstable three-column fracture, typically at the cervicothoracic or thoracolumbar junction. These fractures have a high rate of neurological deficit and mortality. Always image the full spine (CT then MRI) after any significant trauma in a patient with known AS, even if the patient appears well. DEXA may underestimate fracture risk in the fused spine; consider vertebral fracture assessment (VFA) and bone-protective therapy. [1]
Smoking — a modifiable prognostic factor
Smoking is the single most important modifiable prognostic factor in SpA. Smokers have:
- Faster radiographic progression (more syndesmophytes)
- Worse spinal mobility
- Reduced response to TNF inhibitors
- Higher disease activity scores
- Higher cardiovascular risk [1]
Counsel every patient on smoking cessation at every visit. This is a treatable factor that the patient controls, and it has a real impact on disease outcomes. [1]
Regional guideline deltas
| Aspect | ANZ (ARA) | UK (BSR, NICE) | US (ACR) |
|---|---|---|---|
| First-line pharmacological | NSAIDs at full dose | NSAIDs at full dose | NSAIDs at full dose |
| Physiotherapy | Core treatment | Core treatment | Core treatment |
| csDMARD for axial disease | Not recommended | Not recommended | Not recommended |
| Biologic threshold | ASDAS at least 2.1 or BASDAI at least 4 after 2 NSAIDs | BASDAI at least 4 after 2 NSAIDs | Active disease despite NSAIDs (physician assessment) |
| First biologic choice | TNFi or IL-17i (equal preference) | TNFi or IL-17i | TNFi preferred; IL-17i if contraindication to TNFi |
| JAK inhibitor | After biologic failure | After biologic failure | After biologic failure; caution over 50 with CV risk |
| Treat-to-target | ASDAS-based target | BASDAI-based target | Physician assessment (not formal treat-to-target) |
The ASAS-EULAR 2022 update and the ACR 2019 recommendations are broadly concordant on the treatment ladder but differ on the biologic threshold (ASDAS-based vs physician assessment) [5][12].
Communication and shared decision-making
-
Setting expectations: SpA is a chronic but treatable disease. With modern therapy — NSAIDs, physiotherapy, and biologics for those who need them — the majority of patients maintain good function and quality of life. The prognosis has been transformed in the biologic era. [1]
-
Exercise is treatment: Explain that daily exercise is not optional — it is as important as any medication. Postural exercises, swimming, and stretching maintain mobility and prevent the progressive flexion of advanced disease. [1]
-
Smoking cessation: Counsel explicitly that smoking accelerates spinal damage, worsens mobility, and reduces biologic response. This is a modifiable factor with real impact. [1]
-
Uveitis warning: Explain the symptoms of acute anterior uveitis (painful red eye, photophobia, blurred vision) and the need for same-day ophthalmology review. This is a sight-threatening complication that patients must recognise. [1]
-
Spinal fracture warning: Explain that the fused spine is fragile. After any fall or significant trauma — even if they feel well — they must present for full spine imaging. This is a safety-critical message. [1]
-
Biologic choice: Discuss the TNFi vs IL-17i decision. TNFi is preferred if there is co-existing IBD (IL-17i may worsen it); IL-17i is preferred if there is prominent psoriasis. Both are effective for the axial skeleton. [1]
-
Pregnancy: NSAIDs are relatively contraindicated in the third trimester (premature ductus arteriosus closure). Certolizumab (minimal placental transfer) is the preferred biologic in pregnancy. IL-17i and JAKi safety data are limited. [1]
High-yield exam discriminators
- Inflammatory back pain improves with exercise, worsens with rest — the opposite of mechanical back pain. Use Calin criteria (4 of 5) to screen [6].
- NSAIDs are first-line for axial SpA, not DMARDs — sulfasalazine and methotrexate are ineffective for pure axial disease; this is the most commonly tested point [5].
- Modified New York criteria require radiographic sacroiliitis — grade 2 bilateral or grade 3 to 4 unilateral, plus one clinical criterion [1].
- ASAS criteria allow MRI or HLA-B27 — enabling diagnosis of non-radiographic axSpA before X-ray changes appear [2].
- HLA-B27 is supportive but never diagnostic alone — 8 per cent of the general population are positive; 90 per cent of AS patients are positive.
- Enthesitis is the primary lesion — not synovitis. This distinguishes SpA from RA pathologically.
- CASPAR criteria for PsA — inflammatory articular disease plus 3 points (current psoriasis is worth 2). Sensitivity 91 per cent, specificity 99 per cent [3].
- Etanercept is ineffective for uveitis and may worsen it — use a monoclonal antibody TNFi (adalimumab) or IL-17i for patients with recurrent uveitis.
- IL-17 inhibitors can exacerbate IBD — avoid in Crohn disease or ulcerative colitis; use a TNFi monoclonal antibody instead.
- IL-23 inhibitors work for PsA but not axial SpA — ustekinumab and guselkumab treat skin and peripheral joints but are not approved for the axial skeleton.
- The bamboo spine is brittle — always image the full spine after any significant trauma in AS; spinal fractures have high neurological morbidity.
- Reactive arthritis is usually self-limiting but 30 to 50 per cent develop chronic or recurrent disease; HLA-B27 predicts a worse course.
- Acute anterior uveitis needs same-day ophthalmology — it is not conjunctivitis (which is painless, bilateral and gritty).
- DAPSA of 4 or below is the treatment target for PsA — remission or low disease activity.
- Smoking accelerates radiographic progression and reduces biologic response — counsel cessation at every visit.
Summary: the SpA consultation in one paragraph
The spondyloarthropathies are a family of seronegative inflammatory arthritides unified by inflammatory back pain, enthesitis, HLA-B27, and extra-articular features. Diagnose axial disease using the ASAS criteria (imaging arm: sacroiliitis on X-ray or MRI plus 1 SpA feature; clinical arm: HLA-B27 plus 2 SpA features) for early disease, or the modified New York criteria (radiographic sacroiliitis plus 1 clinical criterion) for established AS. Diagnose psoriatic arthritis using the CASPAR criteria (inflammatory articular disease plus 3 points, with current psoriasis worth 2). Manage with NSAIDs at full anti-inflammatory dose as first-line, physiotherapy and exercise as the non-pharmacological core, and biologic DMARDs (TNF inhibitors or IL-17 inhibitors) when disease activity (ASDAS at least 2.1 or BASDAI at least 4) persists despite at least two NSAIDs. csDMARDs are for peripheral arthritis only — they do not work for pure axial disease. Screen for and manage extra-articular features: uveitis (same-day ophthalmology, prefer monoclonal TNFi or IL-17i), aortic regurgitation (echo, cardiology), apical fibrosis (PFTs, chest imaging), and osteoporosis (the fused spine is brittle — always image after trauma). Counsel on smoking cessation (modifiable prognostic factor), exercise as treatment, and the fracture and uveitis warnings. The prognosis is good with early, sustained treatment in the biologic era. [1]
References
- [1]van der Linden S, Valkenburg HA, Cats A Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria Arthritis Rheum, 1984.PMID 6231933
- [2]Rudwaleit M, van der Heijde D, Landewe R, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection Ann Rheum Dis, 2009.PMID 19297344
- [3]Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new criteria from a large international study Arthritis Rheum, 2006.PMID 16871531
- [4]Baeten D, Sieper J, Braun J, et al. Secukinumab, an Interleukin-17A Inhibitor, in Ankylosing Spondylitis N Engl J Med, 2015.PMID 26699169
- [5]Ramiro S, Nikiphorou E, Sepriano A, et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update Ann Rheum Dis, 2023.PMID 36270658
- [6]Sieper J, Braun J, Dougados M, Baeten D Axial spondyloarthritis Nat Rev Dis Primers, 2015.PMID 27188328
- [7]Gorman JD, Sack KE, Davis JC Treatment of ankylosing spondylitis by inhibition of tumor necrosis factor alpha N Engl J Med, 2002.PMID 11986408
- [8]Braun J, Brandt J, Listing J, et al. Treatment of active ankylosing spondylitis with infliximab: a randomised controlled multicentre trial Lancet, 2002.PMID 11955536
- [9]Poddubnyy D, Rudwaleit M, Haibel H, et al. Effect of non-steroidal anti-inflammatory drugs on radiographic spinal progression in patients with axial spondyloarthritis: results from the German Spondyloarthritis Inception Cohort Ann Rheum Dis, 2012.PMID 22459541
- [10]Deodhar A, van der Heijde D, Sieper J, et al. Tofacitinib for the treatment of ankylosing spondylitis: a phase III, randomised, double-blind, placebo-controlled study Ann Rheum Dis, 2021.PMID 33906853
- [11]Mease PJ, Gladman DD, Ritchlin CT, et al. Adalimumab for the treatment of patients with moderately to severely active psoriatic arthritis: results of a double-blind, randomized, placebo-controlled trial Arthritis Rheum, 2005.PMID 16200601
- [12]Ward MM, Deodhar A, Gensler LS, et al. 2019 Update of the American College of Rheumatology/Spondylitis Association of America/Spondyloarthritis Research and Treatment Network Recommendations for the Treatment of Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis Arthritis Care Res (Hoboken), 2019.PMID 31436026