Phys · rheumatological
Systemic Lupus Erythematosus
Also known as systemic lupus erythematosus · SLE · lupus · lupus nephritis · discoid lupus · neonatal lupus · drug-induced lupus · antiphospholipid syndrome · APS · Libman-Sacks endocarditis
Consultant-physician-depth guide to systemic lupus erythematosus (SLE) — loss of immune tolerance, type I interferon signature, autoantibody profiling (ANA, anti-dsDNA, anti-Smith, anti-Ro/La, antiphospholipid), multisystem clinical features, lupus nephritis (ISN/RPS classes I to VI), ACR/EULAR 2019 classification, antiphospholipid syndrome, pregnancy and neonatal lupus, and evidence-based immunosuppression from hydroxychloroquine to belimumab, anifrolumab and voclosporin. Structured for FRACP DWE and DCE preparation.
On this page & tools
Your progress
Saved locally on this device.
Practise this topic
Target exams
Red flags
Systemic Lupus Erythematosus
The answer first
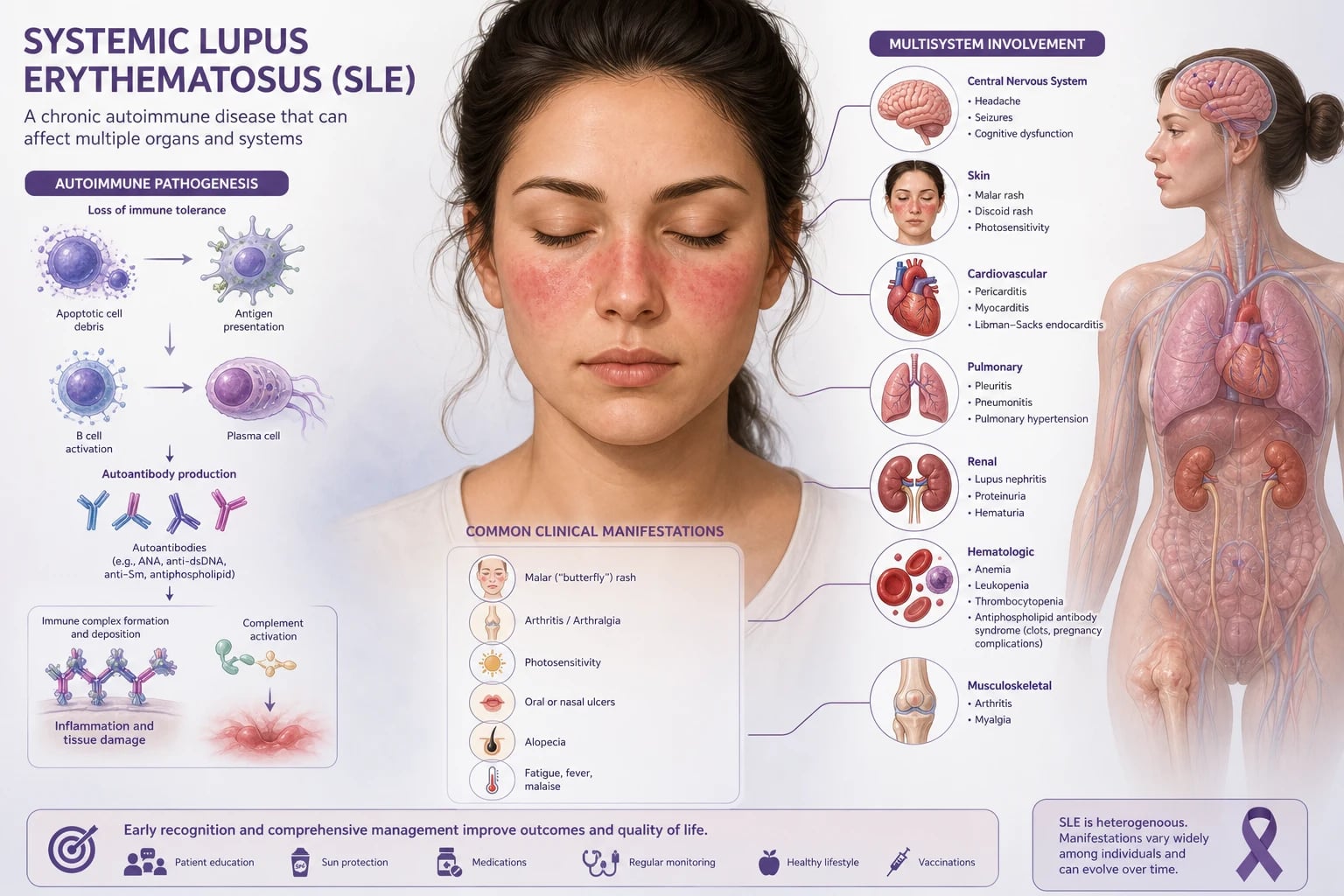
Systemic lupus erythematosus (SLE) is a chronic, relapsing-remitting autoimmune disease in which loss of immune tolerance drives autoantibody production, immune complex formation and deposition, and multi-organ inflammation. It predominantly affects women of childbearing age (female-to-male ratio about 9 to 1) and runs a highly variable course from mild cutaneous and joint disease to life-threatening renal, neurological or haematological involvement. [1]
Three ideas frame everything else on this page: [1]
-
SLE is a clinical diagnosis built on a positive ANA plus cumulative weighted criteria. A positive antinuclear antibody (ANA) is the obligatory entry criterion for the 2019 EULAR/ACR classification. From there, the diagnosis rests on accumulating 10 points or more across weighted clinical and immunological domains, after a more likely alternative explanation has been excluded [1]. ANA alone never makes the diagnosis; a negative ANA (on a competent immunofluorescence assay) makes classification very unlikely.
-
The two organs that decide prognosis are the kidney and the brain. Lupus nephritis is the strongest predictor of mortality and the commonest route to end-stage kidney disease in SLE. Neuropsychiatric lupus and catastrophic antiphospholipid syndrome are the other major killers. Every patient needs a urinalysis at every visit, and any new neurological symptom in a lupus patient is lupus-related until proven otherwise (after infection is excluded). [1]
-
Hydroxychloroquine is the backbone of management for nearly every patient. It reduces flares, improves survival, protects against renal and cutaneous disease, lowers thrombosis risk, and is safe in pregnancy. The LUMINA cohort showed a clear survival benefit [2]. Stopping it is almost always the wrong answer.
DWE high-yield: The single most discriminating antibody panel in SLE is anti-dsDNA (sensitive for activity and nephritis, low specificity) and anti-Smith (anti-Sm) (high specificity, low sensitivity). Anti-Sm is the most specific antibody for SLE — its presence essentially confirms the diagnosis. A rising anti-dsDNA titre with falling C3 and C4 often heralds a flare, particularly a renal flare. [1]
Pathophysiology: why the immune system turns on itself
Understanding the mechanism explains the serology, the organ pattern, and the treatment targets. [1]
Loss of immune tolerance and the type I interferon signature
SLE begins with a failure to clear apoptotic debris. Nuclear material from apoptotic cells is normally removed quickly by macrophages and the complement system. When clearance is defective — through inherited complement deficiency (early classical pathway components C1q, C2, C4), impaired DNase activity, or monocyte dysfunction — nucleic acids accumulate and stimulate innate immune receptors. [1]
The result is sustained activation of plasmacytoid dendritic cells, which produce large amounts of type I interferon (interferon-alpha). This "interferon signature" is one of the most consistent molecular abnormalities in SLE. Type I interferon does three harmful things: it lowers the threshold for B-cell activation (promoting autoantibody production), it drives monocyte differentiation and antigen presentation, and it upregulates the molecules that present nuclear antigens to T cells. The therapeutic proof of this concept is anifrolumab, a monoclonal antibody to the type I interferon receptor, which works precisely because it blocks this central pathway [11].
Autoantibody production
B cells, activated by excess T-cell help and by BAFF (B-cell activating factor, also called BLyS), produce a characteristic family of autoantibodies directed against nuclear antigens: [1]
- ANA — present in 95 to 98 percent of patients; the screening test and the 2019 entry criterion.
- Anti-dsDNA — present in 50 to 70 percent; correlates with disease activity, nephritis, and low complement.
- Anti-Smith (anti-Sm) — present in 20 to 30 percent; the most specific antibody for SLE.
- Anti-Ro (SSA) and anti-La (SSB) — associated with photosensitive rash, subacute cutaneous lupus, sicca symptoms, and neonatal lupus with congenital heart block.
- Antiphospholipid antibodies (lupus anticoagulant, anticardiolipin, anti-beta-2 glycoprotein I) — associated with thrombosis and pregnancy loss.
- Anti-RNP — high titre suggests mixed connective tissue disease overlap.
- Anti-ribosomal P — associated with lupus psychosis (modest predictive value). [1]
Immune complex deposition and complement consumption
Pathogenic antigen-antibody complexes (particularly those containing anti-dsDNA) circulate and deposit in tissues — glomeruli, blood vessel walls, serosal surfaces, and the skin. Deposition activates the classical complement pathway, generating inflammation and consuming C3 and C4. This is why active SLE, and active lupus nephritis in particular, shows low C3 and low C4 together — a classical pathway pattern. A falling C3 and C4 with a rising anti-dsDNA is the classic serological signature of an impending flare. [1]
Mechanism to clinical logic: Because immune complexes activate the classical pathway, both C3 and C4 fall in active lupus. This distinguishes lupus from ANCA vasculitis and IgA nephropathy (normal complement) and from post-streptococcal GN and C3 glomerulopathy (isolated low C3 with normal C4). Memorise this complement pattern — it is tested relentlessly. [1]
Clinical features by system
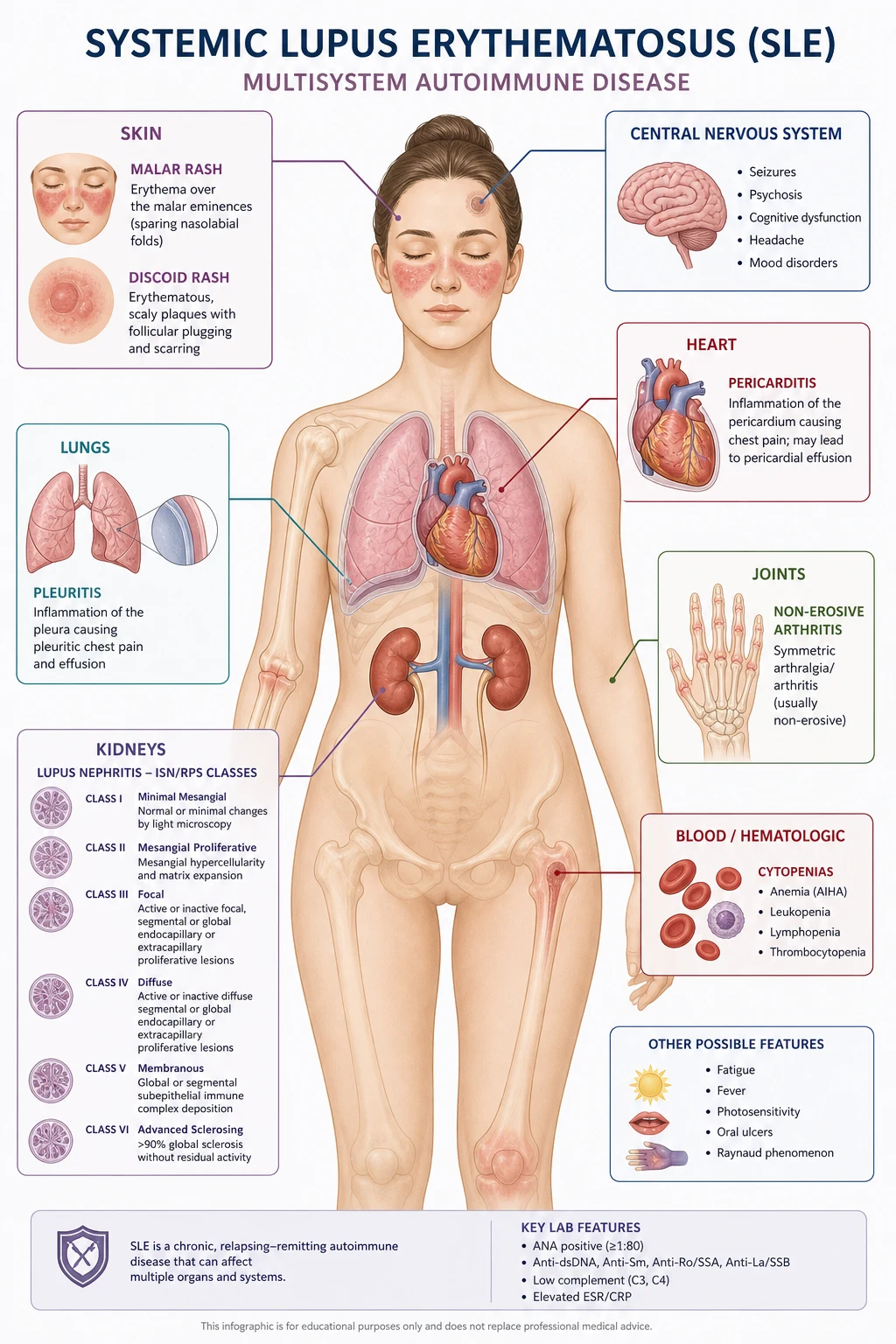
SLE can involve almost any organ. The pattern of involvement varies between patients and over time within the same patient. Approach every patient system by system. [1]
Constitutional
Fatigue is the most common and most disabling symptom in SLE — present in 80 percent or more of patients and often disproportionate to measurable disease activity. Fever and weight loss can occur during flares, but always exclude infection first: immunosuppressed lupus patients are far more likely to have fever from infection than from active lupus. Lymphadenopathy and splenomegaly occur but should prompt consideration of infection or lymphoma. [1]
Cutaneous
The skin is involved in 70 to 85 percent of patients. Learn the specific lesions because they are high-yield in both MCQ and short-case settings: [1]
- Malar (butterfly) rash — the classic fixed erythematous rash over the cheeks and bridge of nose, sparing the nasolabial folds. This fold-sparing distinguishes it from seborrhoeic dermatitis and rosacea (which involve the folds). It is photosensitive, often triggered by sun exposure, and does not scar.
- Discoid rash — coin-shaped, scaly, follicular plaques, usually on the face, scalp and ears; scarring with central atrophy and depigmentation. Discoid lesions are strongly associated with scarring alopecia. A patient with discoid lupus may have isolated cutaneous disease (chronic cutaneous lupus) rather than systemic disease.
- Subacute cutaneous lupus erythematosus (SCLE) — annular or papulosquamous, photosensitive, non-scarring rash on the upper trunk and arms; strongly associated with anti-Ro antibodies and, importantly, with drug exposure (especially terbinafine, calcium-channel blockers, TNF inhibitors).
- Photosensitivity — an exaggerated sunburn-type reaction; one of the clinical criteria.
- Oral and nasal ulcers — usually painless (unlike aphthous ulcers or Behcet ulcers, which are painful), found on the hard palate and nasal septum.
- Alopecia — non-scarring, diffuse hair thinning during active disease (reversible); or scarring alopecia from discoid lesions on the scalp (irreversible).
- Livedo reticularis — a lacelike purplish discoloration, associated with antiphospholipid syndrome.
- Vasculitic lesions — palpable purpura, digital ulcers, nailfold infarcts. [1]
DCE short-case discriminator: The malar rash of SLE spares the nasolabial folds. This single fact is tested repeatedly. Discoid rash scars; malar rash does not. [1]
Musculoskeletal
Arthralgia and arthritis affect more than 90 percent of patients and are often the presenting complaint. The arthritis is typically symmetrical, involving the small joints of the hands, wrists and knees, and is non-erosive and non-deforming. This distinguishes it from rheumatoid arthritis, which is erosive and deforming. However, some patients develop Jaccoud arthropathy — a reducible, non-erosive deforming arthropathy with ulnar deviation and swan-neck deformities caused by tendon and ligament laxity rather than joint destruction. The radiographs show no erosions, which is the key distinction from rheumatoid arthritis. Myalgia and myositis (less commonly) also occur. [1]
Renal — lupus nephritis
Lupus nephritis develops in 40 to 70 percent of patients and is the strongest predictor of poor outcome. Up to 10 to 20 percent of patients with severe proliferative lupus nephritis progress to end-stage kidney disease within 10 years. Every patient with SLE must have a urinalysis and blood pressure measured at every review — renal involvement can be silent early on. [1]
Clinical clues: proteinuria (foamy urine), oedema, hypertension, haematuria, and a rising creatinine. New or worsening proteinuria, microscopic haematuria with dysmorphic red cells or red cell casts, or a falling eGFR mandate urgent renal biopsy and serological assessment (anti-dsDNA, C3, C4). See the lupus nephritis classification section below for the ISN/RPS classes and management. [1]
Cardiopulmonary
The heart and lungs are commonly involved and the manifestations are clinically important: [1]
- Pericarditis is the most common cardiac manifestation — typically sharp positional chest pain with a rub. Tamponade is uncommon but must be excluded.
- Pleuritis and pleural effusion are the most common pulmonary manifestations — usually exudative, often bilateral, with a low complement and low glucose relative to serum.
- Myocarditis is uncommon but serious — presenting with heart failure, arrhythmia, or a globally impaired ejection fraction.
- Libman-Sacks endocarditis — non-bacterial (sterile) verrucous vegetations, classically on the mitral and aortic valves; often clinically silent but can cause valvular regurgitation or embolism, and predisposes to infective endocarditis. Antiphospholipid antibodies add further thrombotic risk to the valves.
- Pulmonary hypertension — may complicate long-standing disease or antiphospholipid syndrome.
- Shrinking lung syndrome — a rare but distinctive manifestation: progressive dyspnoea with elevated hemidiaphragms and reduced lung volumes on imaging, with no parenchymal disease. Thought to reflect diaphragmatic myopathy/dysfunction.
- Acute lupus pneumonitis and diffuse alveolar haemorrhage — rare but life-threatening pulmonary-renal presentations needing urgent immunosuppression. [1]
Neuropsychiatric
The 1999 ACR nomenclature defines 19 neuropsychiatric syndromes in SLE, ranging from the common (headache, mood disorder, cognitive dysfunction) to the severe (seizure, psychosis, transverse myelitis, acute confusional state, chorea, cranial neuropathy, aseptic meningitis, cerebrovascular disease, peripheral neuropathy). [1]
The high-yield severe manifestations to know: [1]
- Seizures — generalised or focal; may be from lupus cerebritis, antiphospholipid-related infarct, or posterior reversible encephalopathy syndrome (PRES) from hypertension or immunosuppression.
- Psychosis — rare but classic; associated with anti-ribosomal P antibodies. Must be distinguished from steroid-induced psychosis.
- Acute confusional state — a medical emergency; exclude infection, metabolic derangement and drug effects first.
- Transverse myelitis — an acute paraparesis with a spinal cord sensory level; associated with antiphospholipid antibodies; needs urgent pulse steroids and often plasma exchange or cyclophosphamide.
- Chorea — rare movement disorder, strongly associated with antiphospholipid antibodies.
- Cranial neuropathy — especially optic neuritis and the Miller Fisher pattern.
- Cognitive dysfunction — common and often subtle; ranges from "brain fog" to overt dementia over years. [1]
Exam trap — neuropsychiatric lupus diagnosis: There is no single diagnostic test for neuropsychiatric lupus. MRI may show white-matter lesions, atrophy, or acute inflammatory changes but can be normal. Cerebrospinal fluid is typically done to exclude infection (raised white cells, normal or low glucose in active lupus cerebritis). The diagnosis is clinical, made after excluding infection, drug effects, metabolic causes and primary psychiatric disease. Always exclude infection before attributing a neurological change to active lupus and giving more immunosuppression. [1]
Haematological
Cytopenias are extremely common and are themselves weighted criteria: [1]
- Anaemia of chronic disease — normocytic, normochromic; the most common anaemia.
- Autoimmune haemolytic anaemia — Coombs (direct antiglobulin test) positive; a reticulocytosis, raised LDH and unconjugated bilirubin. One of the more severe haematological manifestations.
- Leukopenia (below 4.0) and lymphopenia (below 1.0) — lymphopenia is the most common cytopenia and a helpful diagnostic clue.
- Thrombocytopenia — may be immune (ITP-like) or part of antiphospholipid syndrome; severe thrombocytopenia (below 20) with bleeding is a haematological emergency.
- Antiphospholipid syndrome — thrombocytopenia is common, paradoxically coexisting with a prothrombotic state. [1]
High-yield haematology fact: Lymphopenia is the most common cytopenia in SLE. A young woman with unexplained lymphopenia, a malar rash and joint pains has SLE until proven otherwise. [1]
Diagnosis: the 2019 EULAR/ACR classification criteria
The 2019 EULAR/ACR criteria replaced the 1997 ACR and 2012 SLICC criteria. They are the framework examiners expect you to know [1].
How the criteria work
- Entry criterion: a positive ANA (immunofluorescence titre of 1:80 or higher) at least once. If ANA is negative on a competent assay, classification as SLE is not made.
- Additive weighted criteria: each criterion is given a weight (from 2 to 10 points) across seven clinical domains and three immunological domains. Only the highest-scoring criterion within each domain is counted.
- Threshold: a patient is classified as having SLE when they accumulate 10 points or more, provided at least one clinical criterion is present.
- Attribution rule: each criterion counts only if no more likely alternative explanation exists. This is critical — for example, a seizure from known epilepsy, or haemolytic anaemia from a drug, should not be attributed to SLE. [1]
In the validation cohort, these criteria achieved a sensitivity of 96.1 percent and specificity of 93.4 percent — better than both prior criteria sets. [1]
The weighted domains
| Domain | Criterion | Points |
|---|---|---|
| Constitutional | Fever | 2 |
| Haematological | Leukopenia | 3 |
| Thrombocytopenia | 4 | |
| Autoimmune haemolysis | 4 | |
| Neuropsychiatric | Delirium | 2 |
| Psychosis | 3 | |
| Seizure | 5 | |
| Mucocutaneous | Non-scarring alopecia | 2 |
| Oral ulcers | 2 | |
| Subacute cutaneous or discoid lupus | 4 | |
| Acute cutaneous lupus (e.g., malar rash) | 6 | |
| Serosal | Pleural or pericardial effusion | 5 |
| Acute pericarditis | 6 | |
| Musculoskeletal | Joint involvement (synovitis or tenderness on motion) | 6 |
| Renal | Proteinuria above 0.5 g/day (or PCR or ACR equivalent) | 4 |
| Class III or IV lupus nephritis on biopsy | 10 | |
| Antiphospholipid antibodies | Anti-cardiolipin or anti-beta-2 glycoprotein I or lupus anticoagulant | 2 |
| Complement | Low C3 or low C4 | 3 |
| Low C3 and low C4 | 4 | |
| SLE-specific antibodies | Anti-dsDNA or anti-Smith | 6 |
Examiner logic: Notice that a renal biopsy showing class III or IV lupus nephritis alone earns 10 points — enough by itself, with the ANA entry criterion, to classify SLE. This reflects the high diagnostic weight of the biopsy. Similarly, anti-Smith or anti-dsDNA carries 6 points. The criteria reward the high-specificity findings. [1]
What is NOT in the criteria
Raynaud phenomenon, sicca symptoms, and non-specific fatigue are common in SLE but carry no points — they are not discriminating. Discoid lupus is captured under mucocutaneous (4 points for subacute cutaneous or discoid lupus). Neurological criteria are deliberately narrow (only delirium, psychosis, seizure), excluding the broader 1999 NP-SLE syndromes, because the broader syndromes are hard to attribute reliably. [1]
Lupus nephritis: the classification and management framework
Lupus nephritis is the most feared organ manifestation. Its classification, biopsy interpretation, and treatment are tested at every level. [1]
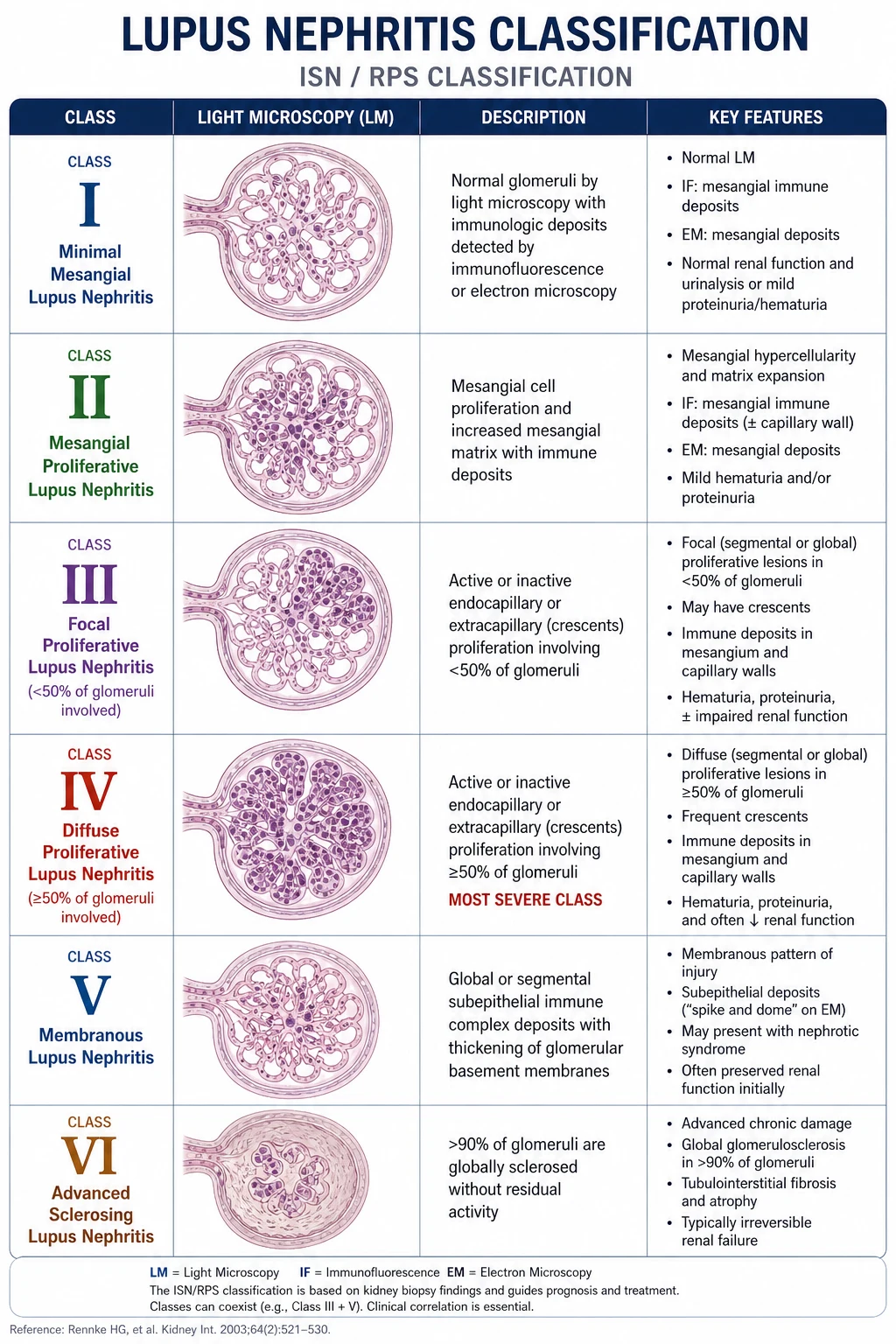
The ISN/RPS classification (2003, revised 2018)
| Class | Name | Key features | Clinical behaviour |
|---|---|---|---|
| I | Minimal mesangial | Immune deposits on immunofluorescence or EM, normal light microscopy | Asymptomatic; no treatment needed |
| II | Mesangial proliferative | Mesangial hypercellularity or expansion | Mild; microscopic haematuria and/or low-grade proteinuria |
| III | Focal proliferative | Active or inactive endocapillary or extracapillary involvement of less than 50 percent of glomeruli; subendothelial deposits | Significant; often nephritic; treat if active |
| IV | Diffuse proliferative | Involvement of 50 percent or more of glomeruli; segmental (IV-S) or global (IV-G); wire-loop lesions, karyorrhexis, crescents | Most severe and most common severe class; highest risk of ESKD; always treat |
| V | Membranous | Global or segmental subepithelial immune deposits; "full house" IF | Nephrotic-range proteinuria; thrombosis risk; may coexist with III or IV |
| VI | Advanced sclerosing | 90 percent or more globally sclerosed glomeruli | End-stage; immunosuppression futile; prepare for renal replacement |
The 2018 revision (Bajema) clarified lesion definitions and introduced a modified NIH activity index (active, potentially reversible lesions: endocapillary hypercellularity, karyorrhexis/fibrinoid necrosis, cellular crescents, hyaline deposits) and chronicity index (irreversible: glomerular sclerosis, fibrous crescents, interstitial fibrosis, tubular atrophy) [3]. The activity/chronicity split guides the intensity of immunosuppression — high activity with low chronicity justifies aggressive treatment; high chronicity means much of the damage is irreversible.
Immunofluorescence and electron microscopy
Lupus nephritis produces a characteristic "full house" immunofluorescence pattern — granular deposition of IgG, IgA, IgM, C3 and C1q — reflecting polyclonal immune complex deposition with classical and alternative pathway activation. Electron microscopy shows deposits in mesangial, subendothelial (class III/IV) and subepithelial (class V) locations. [1]
Approach to suspected lupus nephritis
- Confirm proteinuria and active sediment — urine protein-to-creatinine ratio (PCR) or albumin-to-creatinine ratio; urine microscopy for dysmorphic red cells and red cell casts.
- Serology — anti-dsDNA, C3 and C4 (low in active proliferative disease).
- Renal biopsy — essential before committing to immunosuppression. The class determines the regimen: class III/IV proliferative disease needs aggressive induction; class V membranous disease needs a different approach; class VI needs renal replacement planning.
- Baseline assessment — eGFR, blood pressure, proteinuria, and screening for hepatitis B, hepatitis C and HIV before immunosuppression. [1]
Induction and maintenance of class III/IV lupus nephritis
KDIGO 2021 and the 2019 EULAR/ERA-EDTA recommendations define the standard regimen [8] [9]:
Induction (3 to 6 months):
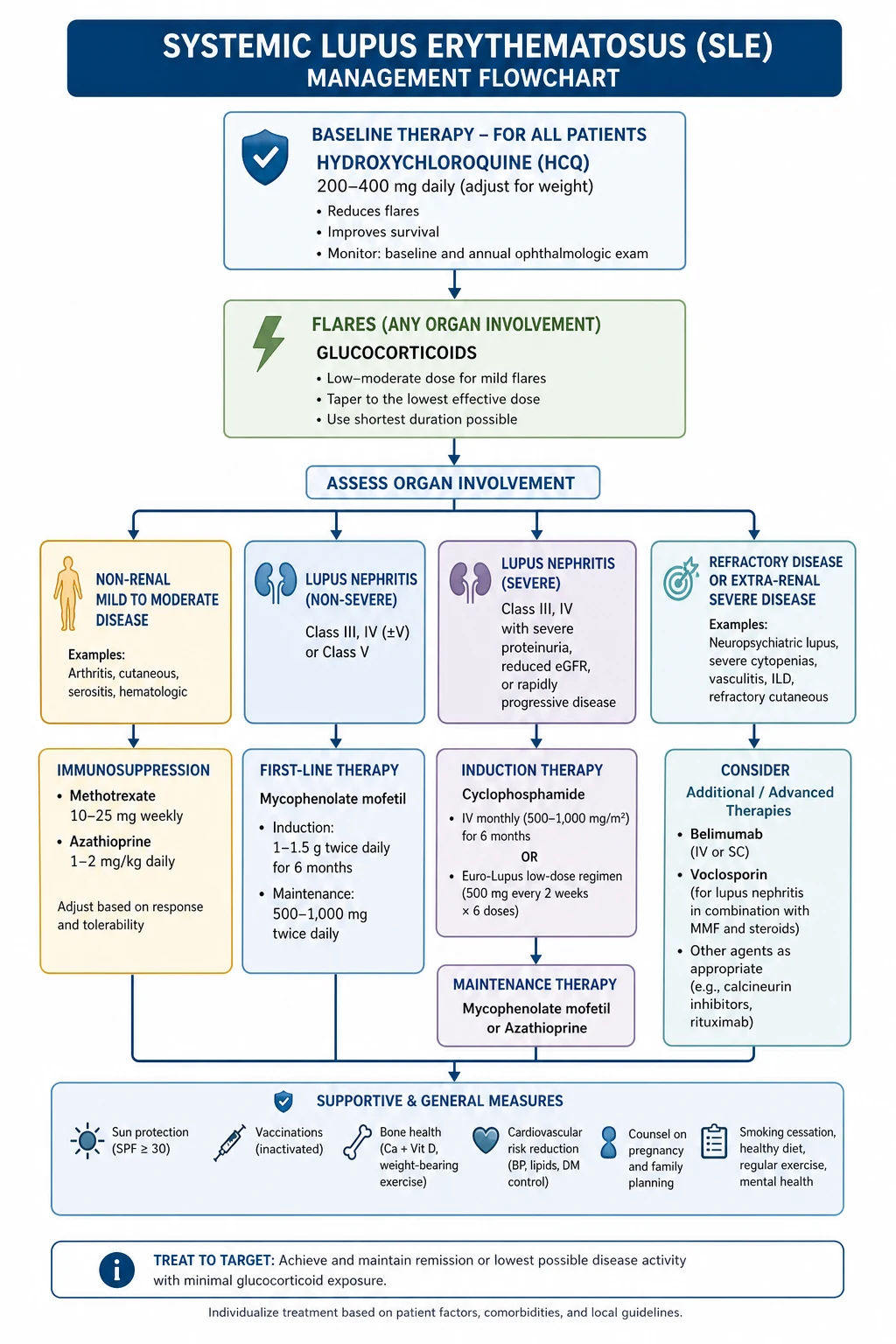
- Glucocorticoids: methylprednisolone pulses (250 to 1000 mg IV daily for 1 to 3 days), then oral prednisone 0.3 to 0.5 mg/kg/day (the EULAR-preferred lower starting dose, reflecting modern steroid-sparing practice), tapering to below 5 to 7.5 mg by 6 months.
- Plus one of:
- Mycophenolate mofetil (MMF) — target 2 to 3 g/day (the ALMS induction trial established MMF as equivalent to IV cyclophosphamide for induction) [5].
- Low-dose IV cyclophosphamide (Euro-Lupus regimen) — 500 mg IV every 2 weeks for 6 doses. The Euro-Lupus Nephritis Trial showed this is as effective as high-dose NIH cyclophosphamide with far less toxicity [4].
- Add-on options for high-risk disease (nephrotic-range proteinuria, adverse prognostic factors): MMF plus a calcineurin inhibitor (especially tacrolimus), or voclosporin. The AURORA 1 trial showed that adding voclosporin 23.7 mg twice daily to MMF and low-dose steroids more than doubled the complete renal response rate at 52 weeks (41 percent versus 23 percent) [12]. Voclosporin does not require therapeutic drug monitoring, unlike tacrolimus or cyclosporin.
Maintenance (after response, for years):
- MMF or azathioprine, with low-dose or no glucocorticoid. The ALMS maintenance trial showed MMF was superior to azathioprine for preventing treatment failure and renal flare (hazard ratio 0.44) [6]. Azathioprine is preferred when pregnancy is planned, because MMF is teratogenic.
- Calcineurin inhibitor continuation is reasonable where voclosporin or tacrolimus was part of induction.
Biologics and refractory disease:
- Rituximab is not first-line — the LUNAR trial did not meet its primary endpoint when rituximab was added to MMF and steroids for induction (56.9 percent versus 45.8 percent, not significant) [7]. It has a role in refractory disease, contraindications to MMF/cyclophosphamide, and as maintenance in relapsing disease.
- Belimumab (anti-BAFF) is approved as add-on therapy; there is emerging evidence for its use in lupus nephritis.
- Non-response: switch induction regimen (MMF to cyclophosphamide or vice versa) and consider rituximab; re-biopsy if the response is incomplete to reassess activity versus chronicity.
Pregnancy pharmacology rule: Mycophenolate mofetil and cyclophosphamide are teratogenic and absolutely contraindicated in pregnancy. A woman planning conception must switch from MMF to azathioprine at least 3 months beforehand. This is a guaranteed exam point and a high-stakes real-world safety issue. [1]
Antiphospholipid syndrome (APS)
About 30 to 40 percent of SLE patients carry antiphospholipid antibodies, and roughly half of those develop clinical APS. APS is defined by the Sydney (2006) criteria [13] — at least one clinical event (vascular thrombosis or pregnancy morbidity) plus at least one laboratory criterion (lupus anticoagulant, medium-high titre anticardiolipin, or anti-beta-2 glycoprotein I), present on two occasions at least 12 weeks apart.
Clinical features of APS
- Venous and arterial thrombosis — deep vein thrombosis and pulmonary embolism are commonest, but arterial thrombosis (stroke, transient ischaemic attack, mesenteric) is disproportionately common compared with other prothrombotic states. A young person with an unexplained stroke must be screened for antiphospholipid antibodies.
- Pregnancy morbidity — recurrent early miscarriage (three or more losses before 10 weeks), one or more unexplained late fetal death (beyond 10 weeks), or severe pre-eclampsia or placental insufficiency necessitating delivery before 34 weeks.
- Thrombocytopenia — paradoxical: a prothrombotic state with a low platelet count.
- Livedo reticularis, valvular heart disease (Libman-Sacks), nephropathy (thrombotic microangiopathy pattern on biopsy). [1]
Catastrophic antiphospholipid syndrome (CAPS)
A rare, feared manifestation defined by thrombosis in three or more organs over days to weeks, with histological evidence of microvascular thrombosis and confirmed antiphospholipid antibodies. Mortality is 30 to 50 percent. Treatment combines anticoagulation, corticosteroids, plasma exchange and intravenous immunoglobulin, plus treatment of any precipitant (infection is the commonest trigger). [1]
Management of APS
- Lifelong anticoagulation for those who have thrombosed — warfarin remains the mainstay for most patients (the direct oral anticoagulants are not preferred for triple-positive or arterial APS, per the TRAPS and ASTRO-APS evidence). Target INR 2 to 3 for venous disease; 3 to 4 for arterial disease in some patients.
- Hydroxychloroquine reduces thrombosis risk and should be continued.
- Aspirin is used for obstetric APS and for primary thromboprophylaxis in high-risk antibody carriers.
- Pregnancy requires combined low-dose aspirin plus prophylactic or treatment-dose low-molecular-weight heparin, managed jointly with obstetric medicine. [1]
Management overview
Hydroxychloroquine for every patient
Hydroxychloroquine (HCQ) is the foundation of SLE management and is indicated in essentially every patient unless contraindicated. The usual dose is 5 mg/kg/day (about 200 to 400 mg daily for most adults). Its benefits: [1]
- Reduces disease activity and flare frequency.
- Improves survival — the LUMINA cohort demonstrated a survival benefit in patients taking HCQ [2].
- Protects against renal and cutaneous flares and reduces cumulative organ damage.
- Lowers thrombosis risk (relevant in antiphospholipid-positive patients).
- Reduces the risk of congenital heart block in anti-Ro positive mothers.
- Is safe in pregnancy and breastfeeding.
The principal toxicity is retinopathy, which is dose- and duration-dependent. All patients should have a baseline ophthalmological assessment (including spectral-domain OCT) and annual screening from five years of therapy (or earlier with higher risk). Do not stop HCQ reflexively — the survival and flare-reduction benefits almost always outweigh the small retinopathy risk. [1]
Corticosteroids for flares
Corticosteroids control acute inflammation rapidly but are toxic with long-term use, contributing substantially to cumulative damage (osteoporosis, avascular necrosis, diabetes, hypertension, cataracts, infection). Use the lowest effective dose for the shortest possible time: [1]
- Mild to moderate flares — oral prednisone 0.5 mg/kg/day or less, tapering to a maintenance dose below 5 to 7.5 mg/day by 3 to 6 months.
- Severe flares (proliferative nephritis, neuropsychiatric, severe cytopenia, alveolar haemorrhage) — IV methylprednisolone pulses 250 to 1000 mg daily for 1 to 3 days, then oral prednisone tapering.
- The modern trend is a lower, faster taper (mirroring the PEXIVAS steroid-sparing principle) to minimise infection and cumulative damage. [1]
Immunosuppressives for organ-threatening disease
When disease threatens a major organ (kidney, brain, haematological, severe serositis or vasculitis), a steroid-sparing immunosuppressive is added: [1]
- Mycophenolate mofetil (MMF) — first-line for lupus nephritis induction and maintenance, and for non-renal disease. Target 2 to 3 g/day. Teratogenic — stop 3 months before pregnancy.
- Azathioprine — 1 to 2 mg/kg/day; the preferred immunosuppressive in pregnancy. Check thiopurine methyltransferase (TPMT) activity before starting to predict myelosuppression risk. [1]- Methotrexate — useful for musculoskeletal and cutaneous disease; avoid in pregnancy and renal impairment.
- Cyclophosphamide — reserved for severe organ-threatening disease (Euro-Lupus regimen for nephritis; high-dose NIH for neuropsychiatric lupus or rapidly progressive disease). Gonadotoxic; consider fertility preservation.
- Calcineurin inhibitors — tacrolimus or voclosporin as add-on for lupus nephritis, especially with nephrotic-range proteinuria.
- Leflunomide — an alternative for musculoskeletal disease; teratogenic with a long washout. [1]
Biologics for refractory disease
When conventional therapy fails or is not tolerated, biologic agents are added: [1]
- Belimumab (anti-BAFF/BLyS) — the first biologic approved for SLE. The BLISS-52 trial showed a higher SLE Responder Index response versus placebo (51 to 58 percent versus 44 percent) [10]. Useful for musculoskeletal and cutaneous disease and reducing steroid exposure; now also has renal indications.
- Anifrolumab (anti-type I interferon receptor) — the TULIP-2 trial showed a BILAG-based Composite Lupus Assessment response of 47.8 percent versus 31.5 percent for placebo [11]. Particularly effective for cutaneous disease and steroid tapering. Watch for herpes zoster reactivation.
- Rituximab (anti-CD20) — used off-label for refractory disease, cytopenias and nephritis despite LUNAR being negative.
Supportive and preventive care
- Vaccination — pneumococcal, influenza, hepatitis B and COVID-19 should be up to date before immunosuppression. Live vaccines (e.g., zoster live, MMR) are avoided during immunosuppression.
- Infection prophylaxis — Pneumocystis jirovecii prophylaxis (trimethoprim-sulfamethoxazole 800/160 mg three times weekly) during high-dose corticosteroids (prednisone 20 mg or more for 4 weeks or longer) and with rituximab. [1]- Bone protection — calcium and vitamin D, DEXA-guided bisphosphonate, during prolonged glucocorticoids.
- Cardiovascular risk — SLE patients have markedly increased cardiovascular risk; manage lipids, blood pressure, diabetes, smoking aggressively.
- Sun protection — broad-spectrum sunscreen, sun avoidance, for photosensitive disease.
- Screening for drug-induced lupus — consider in patients on procainamide, hydralazine, isoniazid, minocycline, anti-TNF agents; characteristic anti-histone antibodies and sparing of the kidney and central nervous system. [1]
Pregnancy and neonatal lupus
Pregnancy in SLE requires careful planning and shared care with obstetric medicine. The principles: [1]
- Plan conception during disease quiescence. Aim for at least 6 months of inactive disease (especially nephritis) before conception to reduce the risk of flare, pre-eclampsia and fetal loss.
- Continue hydroxychloroquine throughout pregnancy — it reduces flares, improves pregnancy outcomes, and reduces the risk of congenital heart block in anti-Ro positive mothers. Stopping HCQ in pregnancy is a common and avoidable error.
- Stop teratogenic drugs before conception — mycophenolate mofetil and cyclophosphamide must be stopped at least 3 months before; switch to azathioprine. Methotrexate and leflunomide are also contraindicated. ACE inhibitors and ARBs are stopped (proteinuria and hypertension are managed with labetalol, methyldopa and nifedipine).
- Assess antiphospholipid and anti-Ro/La status.
- Monitor closely — disease activity markers (anti-dsDNA, complement) each trimester; low-dose aspirin for all to reduce pre-eclampsia; heparin for those with APS. [1]
Neonatal lupus and congenital heart block
Anti-Ro (SSA) and anti-La (SSB) antibodies cross the placenta and can affect the fetus. The two main manifestations: [1]
- Congenital heart block — the most serious complication. Anti-Ro antibodies damage the fetal cardiac conduction tissue (especially the atrioventricular node), producing third-degree heart block. The risk in an anti-Ro positive mother is about 1 to 2 percent for a first affected child, rising to about 15 to 20 percent recurrence in a subsequent pregnancy. It typically develops between 16 and 24 weeks' gestation. It is irreversible — most affected infants need a permanent pacemaker. Serial fetal echocardiography between 16 and 26 weeks is essential in anti-Ro positive mothers. Maternal HCQ reduces the risk. Fluorinated steroids (dexamethasone) are sometimes used for early first- or second-degree block detected on surveillance, but are not beneficial once third-degree block is established.
- Neonatal lupus rash and cytopenias — annular, photosensitive rash (often around the eyes and scalp) and transient cytopenias; these resolve as maternal antibody clears over the first 6 to 8 months, usually without sequelae. [1]
SLE flare versus pre-eclampsia in pregnancy
This is a classic and difficult discriminator. Both cause hypertension, oedema, proteinuria and renal dysfunction in a pregnant lupus patient. Features that favour SLE flare over pre-eclampsia: active urinary sediment, falling complement, rising anti-dsDNA, extra-renal lupus activity (rash, arthritis), and a stable platelet count. Features that favour pre-eclampsia: raised serum urate, low platelets, abnormal liver function, hyperreflexia, and a placental growth factor pattern. A rising anti-dsDNA with falling complement is the single most discriminating finding pointing to lupus flare. Delivery is the treatment for pre-eclampsia; immunosuppression is the treatment for lupus flare — so the distinction changes management fundamentally. [1]
Differential diagnosis
SLE mimics many diseases and many diseases mimic SLE. The broad groups: [1]
- Other connective tissue diseases — mixed connective tissue disease (high-titre anti-U1-RNP), systemic sclerosis, Sjogren syndrome, dermatomyositis, rheumatoid arthritis. Features such as Raynaud, sclerodactyly, myositis, sicca and erosive arthritis point toward overlap syndromes.
- Systemic vasculitis — ANCA-associated vasculitis, cryoglobulinaemia, polyarteritis nodosa. Complement, ANCA and biopsy differentiate these.
- Infection — subacute bacterial endocarditis, viral infections (EBV, HIV, parvovirus B19) can cause a positive ANA, cytopenias and constitutional symptoms. Always exclude infection before escalating immunosuppression.
- Malignancy — lymphoma can present with B symptoms, cytopenias and autoantibodies.
- Drug-induced lupus — anti-histone positive, kidney and CNS spared, resolves on withdrawal of the culprit drug (procainamide, hydralazine, isoniazid, minocycline, anti-TNF).
- Fibromyalgia — overlapping fatigue and pain with a normal serology and inflammatory profile; commonly coexists with SLE and confounds disease activity assessment. [1]
DWE high-yield discriminators
- Malar rash spares the nasolabial folds. Discoid rash scars; malar does not. This is the most tested cutaneous fact.
- SLE arthritis is non-erosive and non-deforming. Jaccoud arthropathy is reducible and non-erosive — distinguished from rheumatoid arthritis radiographically.
- Anti-Smith is the most specific antibody for SLE. Anti-dsDNA tracks disease activity and nephritis. Both carry 6 points in the 2019 criteria.
- Both C3 and C4 are low in active lupus (classical pathway). Normal complement in ANCA vasculitis, IgA nephropathy, anti-GBM. Isolated low C3 in post-strep GN and C3 glomerulopathy.
- ANA is the entry criterion for the 2019 classification. A negative ANA makes classification very unlikely; a positive ANA alone is never diagnostic.
- Class IV lupus nephritis is the most severe and most common severe class and carries 10 points — enough, with ANA, to classify SLE.
- Hydroxychloroquine improves survival and reduces flares and should be continued in pregnancy. Stopping it is almost always wrong.
- Mycophenolate and cyclophosphamide are teratogenic — switch to azathioprine 3 months before conception.
- Anti-Ro causes neonatal lupus and congenital heart block (irreversible third-degree AV block; risk 1 to 2 percent, recurrence 15 to 20 percent). Maternal HCQ reduces the risk.
- Always exclude infection before attributing fever or a new neurological change to active lupus and escalating immunosuppression.
- Lymphopenia is the most common cytopenia in SLE.
- APS requires lifelong anticoagulation after thrombosis. A young person with an unexplained stroke must be screened for antiphospholipid antibodies. [1]
DCE long-case integration
An SLE long case is typically a young or middle-aged woman with multisystem disease — lupus nephritis on immunosuppression, complicated by hypertension, CKD, antiphospholipid syndrome, recurrent infections, or pregnancy planning. The structured approach: [1]
- Opening statement (SASPOP) — Symptoms, Age, Sex, Presentation, Occupation, Problems. Lead with the integrated picture, not a list of test results.
- Problem list — prioritised: the active disease (e.g., class IV lupus nephritis in partial remission), the complications of treatment (e.g., steroid-induced osteoporosis, prior PJP), the comorbidities (hypertension, CKD, APS on warfarin), and the psychosocial (fertility, employment, adherence, contraception).
- Investigation interpretation — serology (ANA, anti-dsDNA, anti-Sm, complement trend), urinalysis and proteinuria trend, biopsy class with activity and chronicity indices, antiphospholipid profile.
- Integrated management plan — disease control (HCQ, maintenance immunosuppression, steroid-sparing), organ protection (RAAS blockade, blood pressure, cardiovascular risk), prevention (vaccination, bone protection, infection prophylaxis, sun protection), and pregnancy planning.
- Communication — fertility and contraception, teratogenicity of drugs, prognosis (overall survival now above 90 percent at 10 years, but ESKD, cardiovascular disease and infection are the main causes of death), and shared decision-making around immunosuppression intensity. [1]
The demonstration of integrated medicine — rheumatology, nephrology, haematology, obstetric medicine and general medicine working together — is what distinguishes a strong long-case answer. [1]
DCE short-case examination
In a rheumatology short case you may be asked to examine the hands and face of a patient with SLE: [1]
- General inspection: a young woman, possibly Cushingoid from steroids, with a malar rash, facial puffiness or thinning hair.
- Hands: look for palmar erythema, nailfold erythema or infarcts, Raynaud phenomenon, non-erosive synovitis of the metacarpophalangeal and proximal interphalangeal joints, Jaccoud deformity (reducible ulnar deviation, swan-neck), discoid lesions on the fingers, livedo, vasculitic ulcers, and digital pulp infarcts.
- Face: malar (butterfly) rash sparing the nasolabial folds, discoid lesions, oral ulcers (hard palate), alopecia (especially temporal), livedo on the ears.
- Systemic extension: blood pressure (hypertension from nephritis), heart sounds (pericardial rub, murmur of Libman-Sacks), chest (pleural effusion, crackles), abdomen (organomegaly), legs (oedema, palpable purpura), and a neurological screen. [1]
Presentation template: "These findings are a non-erosive symmetrical small-joint arthropathy with a photosensitive malar rash sparing the nasolabial folds and oral ulceration, consistent with systemic lupus erythematosus. I would like to confirm the diagnosis with ANA, anti-dsDNA, anti-Smith and complement levels, screen for renal involvement with urinalysis and proteinuria, and assess for antiphospholipid antibodies." [1]
Discussion questions would then cover the differential (rheumatoid arthritis, other connective tissue diseases), the classification criteria, the significance of the antibody profile, and the management including the role of hydroxychloroquine and the approach to nephritis. See the viva and case artifacts for full model presentations. [1]
Key references and evidence summary
| Trial / Guideline | PMID | Key finding |
|---|---|---|
| ACR/EULAR 2019 classification | 31385462 | ANA entry criterion; weighted additive criteria; threshold 10 points; sensitivity 96.1 percent, specificity 93.4 percent [1] |
| LUMINA — hydroxychloroquine survival | 17389655 | HCQ improves survival in SLE [2] |
| ISN/RPS 2018 revision (Bajema) | 29459092 | Clarified lupus nephritis class definitions and NIH activity/chronicity indices [3] |
| Euro-Lupus Nephritis Trial | 12209517 | Low-dose cyclophosphamide (500 mg q2weekly x6) as effective as high-dose for proliferative lupus nephritis [4] |
| ALMS induction | 19369404 | MMF equivalent to cyclophosphamide for lupus nephritis induction [5] |
| ALMS maintenance | 22087680 | MMF superior to azathioprine for lupus nephritis maintenance [6] |
| LUNAR | 22231479 | Rituximab did not meet primary endpoint in lupus nephritis induction [7] |
| EULAR/ERA-EDTA lupus nephritis 2019 | 32220834 | Treatment targets, CNI use, steroid-sparing recommendations [8] |
| KDIGO 2021 Glomerular Diseases | 34556256 | Comprehensive guidance including lupus nephritis [9] |
| BLISS-52 (belimumab) | 21296403 | First biologic approved for SLE; higher SRI response versus placebo [10] |
| TULIP-2 (anifrolumab) | 31851795 | Type I interferon receptor blockade; BICLA response 47.8 percent versus 31.5 percent [11] |
| AURORA 1 (voclosporin) | 33971155 | Voclosporin added to MMF doubled complete renal response in lupus nephritis [12] |
| Miyakis — APS Sydney criteria | 16420554 | Revised classification criteria for definite antiphospholipid syndrome [13] |
ACR/EULAR 2019 Classification Criteria for SLE; EULAR/ERA-EDTA Lupus Nephritis Recommendations (2019 update); KDIGO 2021 Glomerular Diseases Guideline; Australian Rheumatology Association guidance on SLE; ANZSN clinical practice statements on lupus nephritis. [1]
References
- [1]Aringer M, Costenbader K, Daikh D, et al. 2019 European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus Arthritis Rheumatol, 2019.PMID 31385462
- [2]Alarcon GS, McGwin G, Bertoli AM, et al. Effect of hydroxychloroquine on the survival of patients with systemic lupus erythematosus: data from LUMINA, a multiethnic US cohort (LUMINA L) Ann Rheum Dis, 2007.PMID 17389655
- [3]Bajema IM, Wilhelmus S, Alpers CE, et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: clarification of definitions, and modified National Institutes of Health activity and chronicity indices Kidney Int, 2018.PMID 29459092
- [4]Houssiau FA, Vasconcelos C, D'Cruz D, et al. Immunosuppressive therapy in lupus nephritis: the Euro-Lupus Nephritis Trial, a randomized trial of low-dose versus high-dose intravenous cyclophosphamide Arthritis Rheum, 2002.PMID 12209517
- [5]Appel GB, Contreras G, Dooley MA, et al. Mycophenolate mofetil versus cyclophosphamide for induction treatment of lupus nephritis J Am Soc Nephrol, 2009.PMID 19369404
- [6]Dooley MA, Jayne D, Ginzler EM, et al. Mycophenolate versus azathioprine as maintenance therapy for lupus nephritis N Engl J Med, 2011.PMID 22087680
- [7]Rovin BH, Furie R, Latinis K, et al. Efficacy and safety of rituximab in patients with active proliferative lupus nephritis: the Lupus Nephritis Assessment with Rituximab study Arthritis Rheum, 2012.PMID 22231479
- [8]Fanouriakis A, Kostopoulou M, Cheema K, et al. 2019 Update of the Joint European League Against Rheumatism and European Renal Association-European Dialysis and Transplant Association (EULAR/ERA-EDTA) recommendations for the management of lupus nephritis Ann Rheum Dis, 2020.PMID 32220834
- [9]Kidney Disease: Improving Global Outcomes (KDIGO) Glomerular Diseases Work Group KDIGO 2021 Clinical Practice Guideline for the Management of Glomerular Diseases Kidney Int, 2021.PMID 34556256
- [10]Navarra SV, Guzman RM, Gallacher AE, et al. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: a randomised, placebo-controlled, phase 3 trial Lancet, 2011.PMID 21296403
- [11]Morand EF, Furie R, Tanaka Y, et al. Trial of Anifrolumab in Active Systemic Lupus Erythematosus N Engl J Med, 2020.PMID 31851795
- [12]Rovin BH, Teng YKO, Ginzler EM, et al. Efficacy and safety of voclosporin versus placebo for lupus nephritis (AURORA 1): a double-blind, randomised, multicentre, placebo-controlled, phase 3 trial Lancet, 2021.PMID 33971155
- [13]Miyakis S, Lockshin MD, Atsumi T, et al. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS) J Thromb Haemost, 2006.PMID 16420554