Psych · Addiction psychiatry
Addiction in older adults
Also known as Substance use disorder in older adults · Geriatric addiction · Late-life alcohol use disorder · Elderly substance misuse · Late-onset substance use disorder · Prescription drug misuse older adults
Exam-exhaustive fellowship topic on addiction and substance misuse in older adults — early- vs late-onset phenotypes, age-related PK/PD, alcohol binge trends, benzodiazepine and opioid iatrogenic dependence, atypical presentation (falls, confusion, self-neglect), SMAST-G and AUDIT-C screening, withdrawal and Wernicke traps, SBIRT/BRITE, naltrexone and acamprosate, EMPOWER/Beers deprescribing, dual diagnosis with late-life depression and suicide. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
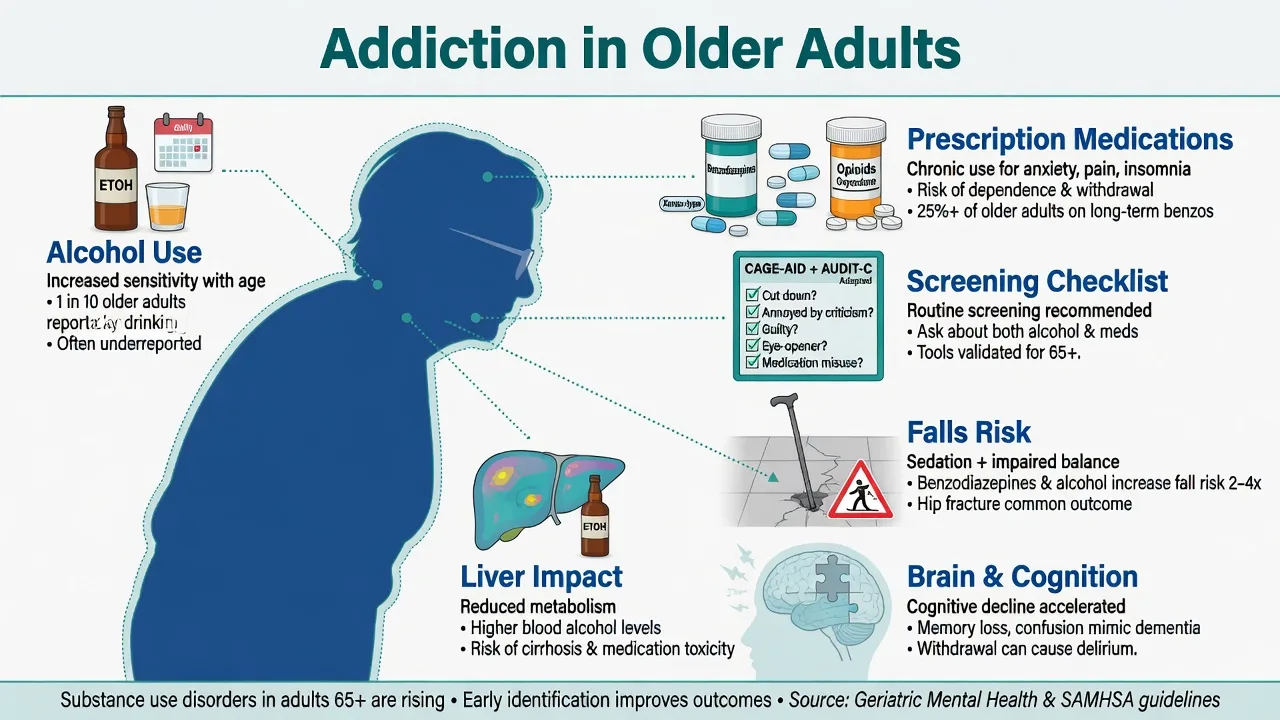
Population ageing and the Baby Boom cohort moving through later life mean absolute numbers of older adults with hazardous substance use and substance use disorders (SUDs) are rising, while clinical services still under-screen and under-treat.[1][2][5] Fellowship answers must hold two truths: older adults may meet full DSM-5-TR SUD criteria, and many more experience medically important harm at volumes that would look modest in a 30-year-old.
Overview and definition
Substance use disorder criteria (impaired control, social impairment, risky use, pharmacological criteria) apply across the lifespan. In geriatrics the same criterion count defines severity, but harm thresholds shift downward because of lower lean mass, higher CNS sensitivity, polypharmacy, falls risk, and medical comorbidity.[1][2]
ICD-11 language of hazardous use, harmful pattern of use, and dependence is often more clinically honest for older adults who do not fit a young polysubstance stereotype yet still need intervention.[1][4]
Physiological dependence (tolerance/withdrawal) on prescribed benzodiazepines or opioids is not a moral diagnosis and can coexist with, or occur without, full behavioural use-disorder criteria.[1][13]
Operational age cut-offs in the literature commonly use ≥50, ≥60, or ≥65 years — state your operational definition in viva answers.[2][4]
Classification
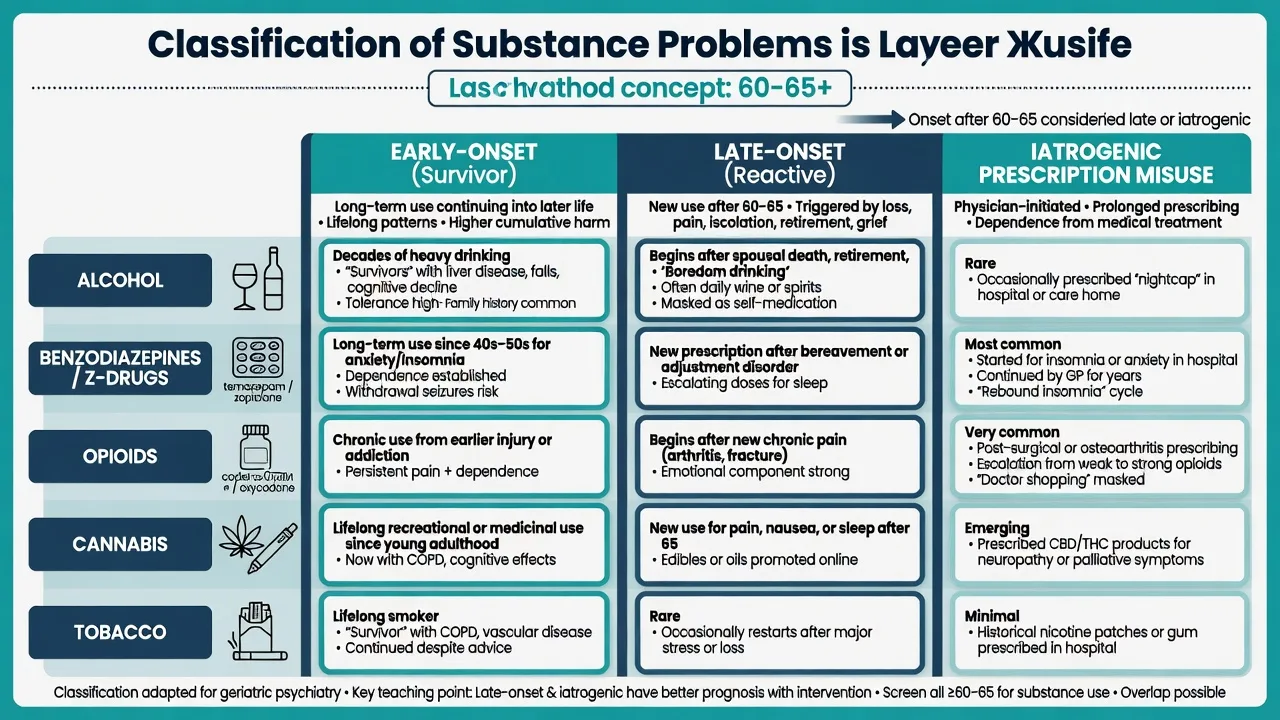
Early-onset (survivor)
- Onset earlier in life; continues into old age
- Higher cumulative organ and cognitive harm
- More lifetime dual diagnosis and stigma history
Late-onset (reactive)
- New problem after ~60–65
- Often grief, retirement, pain, isolation
- Less antisocial history; depression common
Iatrogenic prescription
- BZD/Z-drug, opioids, sometimes gabapentinoids
- Started for insomnia, anxiety, or pain
- Deprescribing + treat the driver
Epidemiology and risk factors
Alcohol is the dominant substance of misuse in later life. Binge drinking and AUD signals have increased in older US cohorts across the 2000s–2010s, including important signals among older women — do not treat “old male drinker only” as the mental model.[5][6][7]
NESARC-III and related epidemiology establish the population burden of DSM-5 AUD across adulthood and underscore the treatment gap; geriatric services inherit that gap with additional ageism.[7][1]
Risk anchors: male sex (alcohol, still), widowhood and social isolation, chronic pain, insomnia, anxiety and late-life depression, prior SUD, easy multi-prescriber access, and residential-care boredom or “PRN culture.”[2][4][15]
Harms that examiners expect named: falls and fractures, delirium, cognitive impairment, liver disease, drug–drug interactions, overdose (especially opioids ± benzodiazepines), and suicide.[1][12][16]
High-yield anchors
Pathophysiology
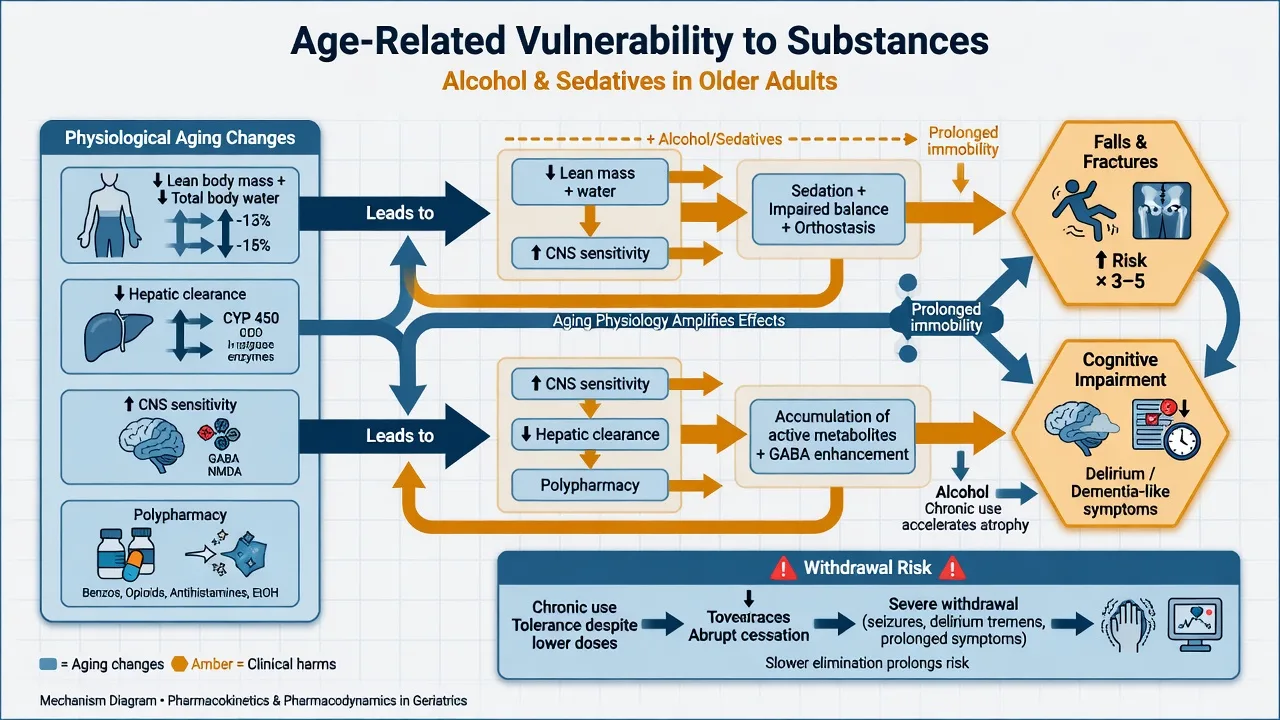
Pharmacokinetics: reduced lean body mass and total body water raise blood alcohol concentration for a given drink; hepatic mass/flow and renal clearance decline, prolonging exposure to many psychotropics and active metabolites.[1][2]
Pharmacodynamics: greater CNS sensitivity to alcohol, benzodiazepines, Z-drugs, and opioids; orthostasis and balance impairment amplify fall risk.[1][12][13]
Addiction circuits (reward, salience, habit, impaired control) do not vanish at retirement. Malnutrition and thiamine depletion still drive Wernicke–Korsakoff risk in older drinkers, often without the classic “skid-row” stereotype.[1][4]
Reinforcing loops: pain → opioids → depression/sedation; insomnia → BZD/Z-drug → tolerance → rebound insomnia; grief → alcohol → depression → more alcohol.[2][15]
Clinical presentation
Atypical presentations dominate exam stems: recurrent falls and fractures, fluctuating confusion and self-neglect, treatment-resistant hypertension or diabetes, new insomnia or depression after loss, unexplained macrocytosis or raised GGT, and family concern with empty bottles or stockpiled tablets.[1][2][4]
Withdrawal may present as delirium on a medical ward after alcohol or benzodiazepines stop on admission. Intoxication may present as falls with head injury rather than “party excess.” Collateral from GP, pharmacy, family, and carers is not optional in older adults who minimise use.[1][13]
Differential diagnosis
| Presentation | Favours substance-related | Favours alternative |
|---|---|---|
| Confusion | Tempo with last drink/dose cut; autonomic signs; drug chart | Infection, stroke, metabolic, primary dementia progression |
| Falls | Night sedatives, alcohol, orthostasis on chart | Parkinsonism, visual loss, environment alone |
| Low mood | Daily drinking, early-morning relief drinking | Primary late-life depression without substance driver |
| Cognitive decline | Heavy alcohol years, BZD load, nutritional neglect | Alzheimer/vascular without substance contribution |
| Chronic pain opioids | Loss of control, craving, multiple prescribers | Stable therapeutic opioid without OUD criteria |
Bedside assessment
History that scores marks: standard drinks per day/week, binge pattern, last drink time, all benzodiazepines/Z-drugs/opioids (prescribed and actual), OTC codeine/antihistamine sedatives, cannabis, tobacco, prior seizures/DT/Wernicke, suicide attempts, driving, living alone, carers, and what the substance is “solving” (pain, grief, sleep, boredom).[1][2][4]
Screens:
- AUDIT-C / AUDIT for alcohol risk
- SMAST-G / MAST-G — geriatric-sensitive alcohol screens
- CAGE — still taught but can miss at-risk older drinkers who do not feel “guilty” or “annoyed”; do not rely on CAGE alone
- Full medication reconciliation and prescription-monitoring review where available
Risk: suicide (alcohol + late-life depression is high-yield), falls, elder abuse/neglect, capacity for detox and deprescribing decisions, fire risk if smoking with oxygen, driving.[15][16]
Investigations
Baseline work-up includes FBC (MCV), LFT (GGT, AST/ALT pattern), U&E, magnesium, phosphate, glucose, B12/folate, and coags if liver disease; ECG if QT-risk polypharmacy, syncope, or overdose; cognitive screen when planning detox or sedative taper; imaging/LP only for differential (trauma, focal neurology, meningitis suspicion). Drug screens are adjuncts — many benzodiazepines are missed; history first. Do not delay parenteral thiamine for laboratory confirmation when Wernicke risk is present.[1][4]
Management — resuscitation and emergencies
- Intoxication/overdose: ABCDE, airway protection, co-ingestant awareness (opioids + BZD), naloxone for opioids with observation for renarcotisation.[1]
- Alcohol/BZD withdrawal: symptom-guided benzodiazepine cover with falls and oversedation monitoring; prefer agents with cleaner hepatic pathways (e.g. lorazepam teaching) when cirrhosis or severe frailty is present — still treat adequately to prevent seizures.[1][13]
- Wernicke risk: give thiamine promptly (parenteral high-dose regimens per local protocol); Caine criteria teaching — do not wait for the full classic triad.[1][4]
- Delirium: parallel medical work-up — never attribute everything to “the alcohol history” alone.[1]
- Suicide and vulnerability: safety plan, means restriction, carer involvement, urgent old-age psychiatry when needed.[16][15]
Management — definitive and stepped care
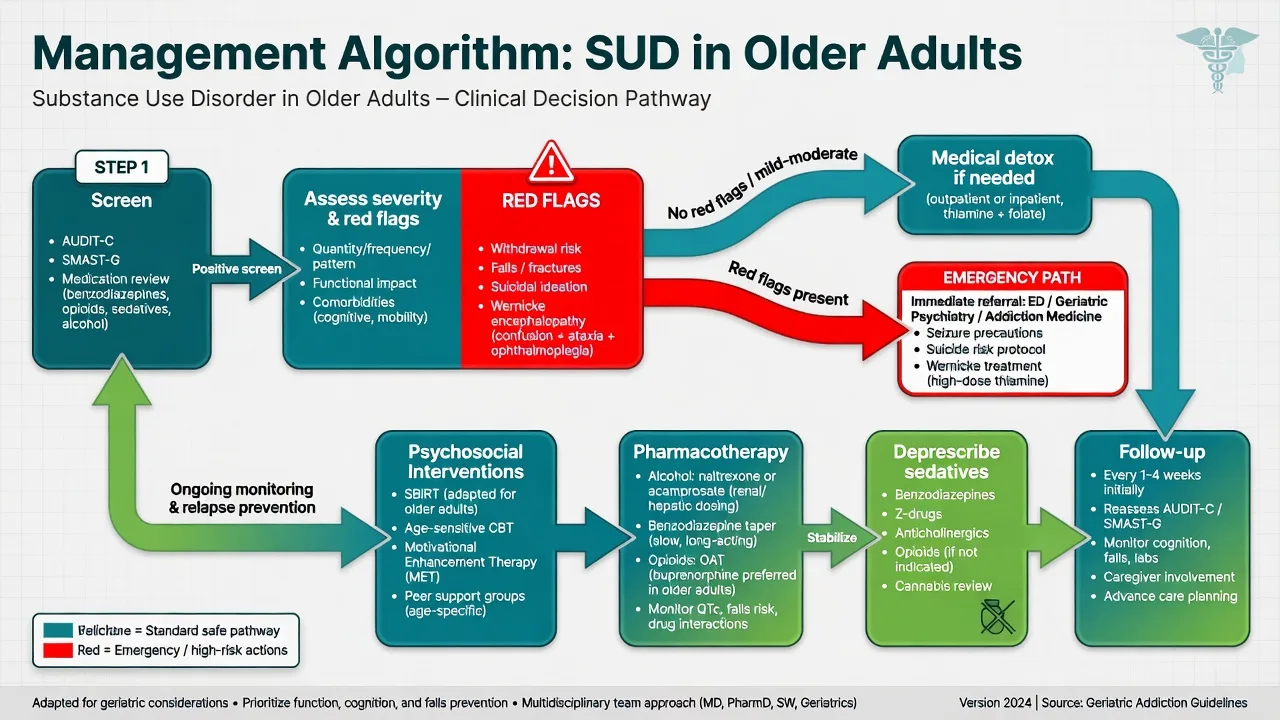
Step 1 — Identify and engage (SBIRT)
Screening, brief intervention, and referral to treatment models extend to older adults. The Florida BRITE project is a named exemplar of older-adult-specific screening and brief intervention with reductions in substance misuse at follow-up.[10][2][4]
Motivational interviewing, non-stigmatising language, and treating the presenting medical problem (falls, insomnia, mood) as the engagement hook beat moral lectures.[3][1]
Step 2 — Psychosocial care
Age-sensitive CBT/MET elements, case management, grief work, social prescribing for isolation, and — when available — age-peer group settings that many older adults prefer over mixed-age youth-heavy programmes.[3][2] Treatment reviews suggest older adults can achieve outcomes as good as or better than younger adults when retained in care.[3]
Step 3 — Alcohol pharmacotherapy (doses examiners expect)
After detoxification or when medically appropriate, anti-craving agents used in general adult practice remain relevant with geriatric caution. Naltrexone oral typically 50 mg once daily if the patient is opioid-free, not in acute hepatitis failure pathways that contraindicate use, and with LFT monitoring — older-adult trial data support naltrexone as an adjunct (Oslin et al.); COMBINE supports naltrexone with medical management in broader AUD populations.[8][9][1] Acamprosate typically 666 mg three times daily (reduce in renal impairment — check eGFR and product information) as a glutamate-modulating relapse-prevention option post-detox.[9][1] Disulfiram requires reliable cognition, supervision, and alcohol education; frailty, cognitive impairment, and unsupervised use make it a high-caution choice in later life.[1][4] Always verify current product information and local formulary; start with shared decision-making and monitoring for dizziness, hepatic signals (naltrexone), and adherence.[1][8]
Step 4 — Benzodiazepines and Z-drugs
Beers Criteria list benzodiazepines and non-benzodiazepine hypnotics as potentially inappropriate in older adults for most chronic insomnia/anxiety scripts.[14] Glass meta-analysis: modest sleep benefit versus cognitive and adverse-event harm.[12] Markota review: dangers, management, alternatives.[13]
Never abrupt-stop continuous users. Negotiate gradual taper (often ~5–10% reductions every 1–2 weeks, slower near the end, individualised), consider diazepam substitution for awkward multi-agent regimens, and use EMPOWER-style patient education, which reduced inappropriate benzodiazepine use in a cluster RCT of older adults.[11][13][1]
Step 5 — Opioids and other substances
Apply OUD criteria carefully (dependence alone on long-term analgesia is not automatically OUD). Offer naloxone where overdose risk exists, multimodal pain care, and addiction pathways when compulsive use, lost control, or harm criteria are met — without abandoning pain.[1][2] Cannabis and tobacco need explicit enquiry; smoking cessation remains disease-modifying in COPD and vascular disease common in this age group.[2][4]
Step 6 — Dual diagnosis and follow-up
Integrate treatment of late-life depression, anxiety, PTSD, and cognitive impairment with substance care — sequential “fix-pong” between services fails this population.[15][3] Plan early review after any taper start, post-detox, or new anti-craving medicine; involve GPs, pharmacists, and carers.[1][10]
Specific subtypes and scenarios
Late-onset alcohol after bereavement. Screen depression and suicide; brief intervention plus grief support; pharmacotherapy if dependence criteria met.[4][15][16]
Long-term night BZD with falls. EMPOWER education, CBT-I pathway, gradual taper, Beers framing without abandoning the patient to rebound insomnia alone.[11][12][14]
Ward alcohol withdrawal. CIWA-style protocols with geriatric sedation vigilance; thiamine; discharge plan that includes addiction follow-up, not only “home with GP.”[1][4]
Residential aged care. Hidden alcohol, PRN sedatives for behavioural disturbance, and capacity/guardianship interfaces — treat the person, not only the chart.[1][2]
Chronic pain and opioids. Multimodal analgesia, OUD assessment, naloxone, specialist pain–addiction interface.[1]
Complications and pitfalls
- Ageist nihilism (“leave them to drink”)
- Under-screening because the patient is “respectable”
- Missing Wernicke called dementia
- Abrupt inpatient BZD cessation
- Standard adult detox doses causing falls/aspiration
- Starting naltrexone while opioids continue
- Ignoring suicide in early abstinence
- Deprescribing without treating pain, grief, or insomnia drivers
Prognosis and disposition
Engaged older adults often do as well as younger adults; late-onset alcohol problems sometimes carry a more favourable psychosocial profile if isolation and mood are addressed.[3][2]
Disposition ladder: opportunistic SBIRT in primary care and ED → GP shared care with brief intervention → specialist addiction and/or old-age psychiatry → inpatient detox when prior seizures/DT, severe medical comorbidity, unstable housing, high suicide risk, or failed ambulatory attempts.[1][10][3]
Special populations
Very old and frail: extreme PK, capacity assessment, carer burden, advance-care planning honesty about goals of care.[1]
Women: under-detection, lower absolute consumption with similar or greater harm, widowhood risk, binge-trend signals in recent epidemiology.[5][6]
Cultural diversity and Indigenous elders: culturally safe enquiry; avoid both under-asking and stereotyping.[2]
LGBTQ+ older adults: minority stress, chosen-family collateral, historical trauma with institutions.[2]
Evidence, guidelines, and regional differences
| Source | Exam take-home |
|---|---|
| Lehmann and Fingerhood NEJM 2018 | Core later-life SUD review |
| Kuerbis 2013/2014 | Epidemiology, phenotypes, treatment evidence |
| Barry and Blow 2016 | Lifespan alcohol focus on older adults |
| Han binge papers | Rising binge/AUD signals |
| Oslin naltrexone; COMBINE | Pharmacotherapy anchors |
| BRITE / SBIRT | Brief intervention works in older adults |
| EMPOWER; Beers 2023; Glass; Markota | Sedative deprescribing and harm |
ANZ: FRANZCP addiction and old-age interfaces; Australian Guidelines for the Treatment of Alcohol Problems principles; local real-time prescription monitoring; mental health acts for involuntary care when capacity and risk criteria met — state principles, do not invent section numbers. UK: NICE alcohol pathways and medicines optimisation for limited hypnotic duration; CASC skills for non-stigmatising engagement of older drinkers. US: AGS Beers Criteria, ABPN items on geriatric PK and opioid–BZD synergy, SBIRT/BRITE programme logic, EMPOWER-style deprescribing education.[1][4][14][11][10]
Exam pearls
Last drink plus full sedative list before predicting withdrawal timing; SMAST-G / AUDIT-C plus medication review every comprehensive older-adult assessment; Caine for Wernicke — incomplete triad still treats; naltrexone 50 mg daily if opioid-free; acamprosate 666 mg TDS with renal adjustment; EMPOWER = education deprescribes BZD in older adults; Beers: avoid chronic BZD/Z-drug for insomnia when possible; late-life suicide plus alcohol = act, do not minimise; early- vs late-onset changes formulation, not compassion.[1][8][9][11][14][16]
OLDER-SUD
References
- [1]Lehmann SW, Fingerhood M. Substance-Use Disorders in Later Life N Engl J Med, 2018.PMID 30575463
- [2]Kuerbis A, Sacco P, Blazer DG, et al. Substance abuse among older adults Clin Geriatr Med, 2014.PMID 25037298
- [3]Kuerbis A, Sacco P. A review of existing treatments for substance abuse among the elderly and recommendations for future directions Subst Abuse, 2013.PMID 23471422
- [4]Barry KL, Blow FC. Drinking Over the Lifespan: Focus on Older Adults Alcohol Res, 2016.PMID 27159818
- [5]Han BH, Moore AA, Sherman S, et al. Demographic trends of binge alcohol use and alcohol use disorders among older adults in the United States, 2005-2014 Drug Alcohol Depend, 2017.PMID 27979428
- [6]Han BH, Moore AA, Ferris R, et al. Binge Drinking Among Older Adults in the United States, 2015 to 2017 J Am Geriatr Soc, 2019.PMID 31364159
- [7]Grant BF, Goldstein RB, Saha TD, et al. Epidemiology of DSM-5 Alcohol Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions III JAMA Psychiatry, 2015.PMID 26039070
- [8]Oslin D, Liberto JG, O'Brien J, et al. Naltrexone as an adjunctive treatment for older patients with alcohol dependence Am J Geriatr Psychiatry, 1997.PMID 9363289
- [9]Anton RF, O'Malley SS, Ciraulo DA, et al. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial JAMA, 2006.PMID 16670409
- [10]Schonfeld L, King-Kallimanis BL, Duchene DM, et al. Screening and brief intervention for substance misuse among older adults: the Florida BRITE project Am J Public Health, 2010.PMID 19443821
- [11]Tannenbaum C, Martin P, Tamblyn R, et al. Reduction of inappropriate benzodiazepine prescriptions among older adults through direct patient education: the EMPOWER cluster randomized trial JAMA Intern Med, 2014.PMID 24733354
- [12]Glass J, Lanctôt KL, Herrmann N, et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits BMJ, 2005.PMID 16284208
- [13]Markota M, Rummans TA, Bostwick JM, et al. Benzodiazepine Use in Older Adults: Dangers, Management, and Alternative Therapies Mayo Clin Proc, 2016.PMID 27814838
- [14]By the 2023 American Geriatrics Society Beers Criteria Update Expert Panel American Geriatrics Society 2023 updated AGS Beers Criteria for potentially inappropriate medication use in older adults J Am Geriatr Soc, 2023.PMID 37139824
- [15]Blow FC, Serras AM, Barry KL. Late-life depression and alcoholism Curr Psychiatry Rep, 2007.PMID 17257508
- [16]Blow FC, Brockmann LM, Barry KL. Role of alcohol in late-life suicide Alcohol Clin Exp Res, 2004.PMID 15166636