Psych · Addiction psychiatry
Alcohol-related brain injury and Korsakoff syndrome
Also known as ARBI · ARBD · Alcohol-related brain damage · Wernicke encephalopathy · Wernicke-Korsakoff syndrome · Korsakoff psychosis · Alcohol-induced amnestic disorder · Thiamine deficiency encephalopathy
Exam-exhaustive fellowship topic on alcohol-related brain injury and Korsakoff syndrome — ARBI umbrella versus Wernicke–Korsakoff continuum, Caine criteria, thiamine prevention and treatment doses with EFNS/RCP regional deltas, MRI support patterns, neuropsychology of diencephalic amnesia and confabulation, differentials from other dementias, acute emergency care, and long-term rehabilitation, capacity, and supported living. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Alcohol-related brain injury is a high-yield addiction–neuropsychiatry interface. Examiners punish three failures: waiting for the classic Wernicke triad, vague thiamine dosing without route and intensity, and collapsing all ARBI into “Korsakoff” or primary degenerative dementia.[1][2][5][8]
Overview and definition
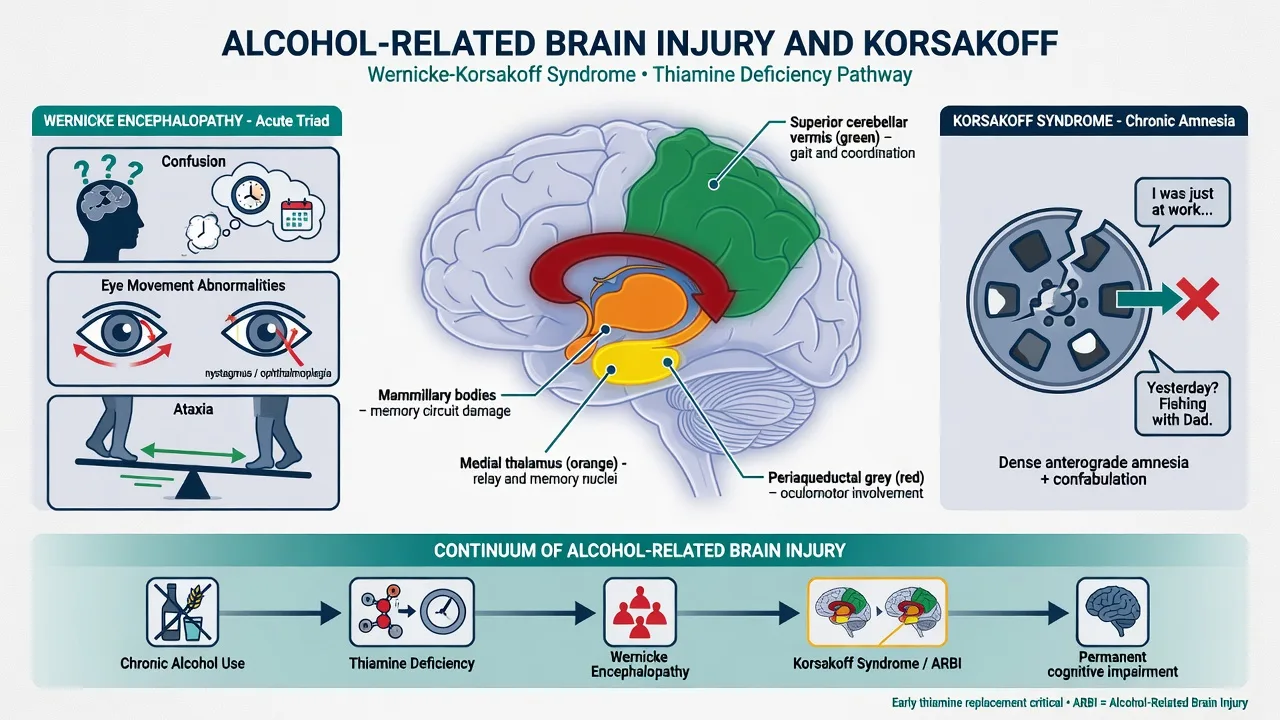
Alcohol-related brain injury / damage (ARBI/ARBD) describes structural and functional brain sequelae of chronic heavy alcohol use, spanning executive dysfunction, cerebellar–motor impairment, and diencephalic amnesia, with or without a documented Wernicke episode.[8][9]
Wernicke encephalopathy (WE) is an acute, potentially reversible neuropsychiatric emergency of thiamine (vitamin B1) deficiency — most often in alcohol dependence with malnutrition, but also in non-alcoholic starvation states (hyperemesis, bariatric surgery, malignancy, dialysis).[2][5]
Korsakoff syndrome (KS) is a chronic amnestic syndrome — disproportionate memory impairment relative to other cognitive domains — classically residual after WE, though some presentations evolve more insidiously.[6][7][13]
The Wernicke–Korsakoff continuum is therefore a subset of ARBI, not a synonym for every alcohol-related cognitive problem.[8][9]
Classification — spectrum and nosology
Practical clinical buckets
| Bucket | Core feature | Time course | Reversibility |
|---|---|---|---|
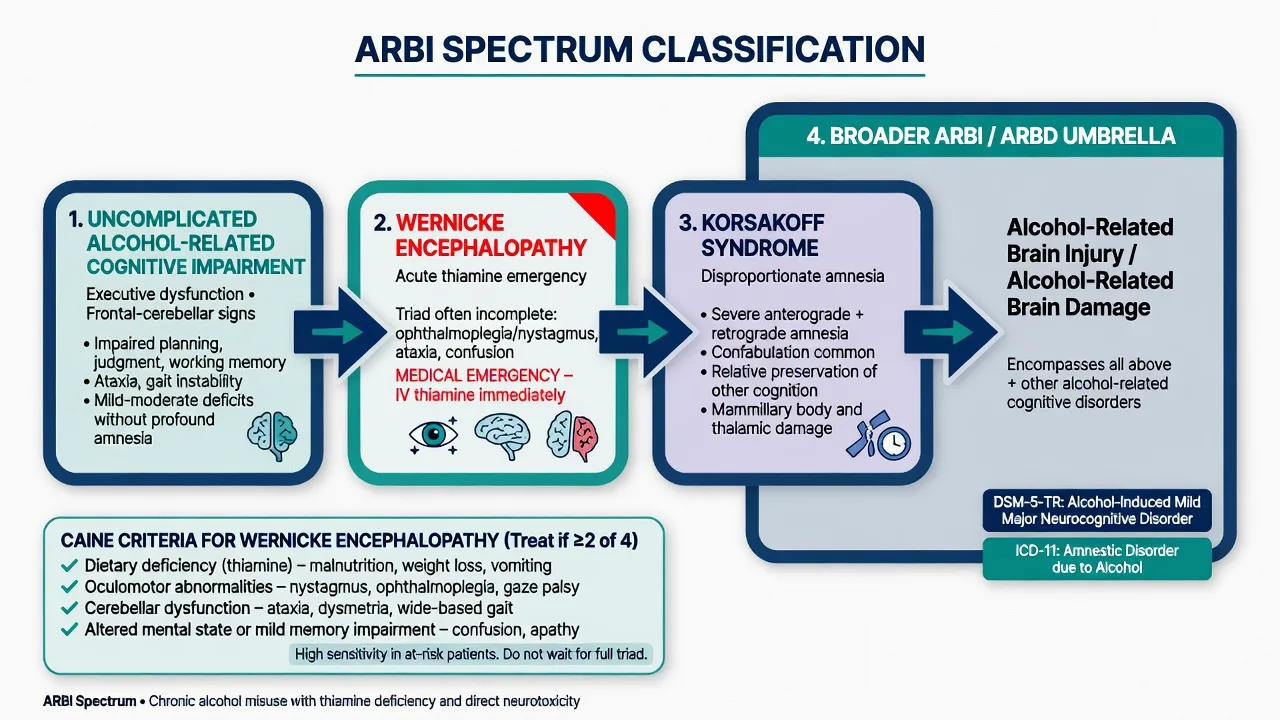
| Uncomplicated ARBI | Executive, frontal–cerebellar, social cognition | Chronic, may improve with abstinence | Partial over months |
| Wernicke encephalopathy | Confusion ± oculomotor ± ataxia ± malnutrition | Hours–days | Often partial if treated early |
| Korsakoff syndrome | Dense anterograde amnesia ± confabulation | Residual after WE | Often limited once structural |
| Other alcohol syndromes | Cerebellar degeneration, Marchiafava–Bignami, hepatic encephalopathy | Variable | Cause-specific |
DSM-5-TR and ICD-11 framing
- DSM-5-TR: alcohol-induced major or mild neurocognitive disorder (specify whether persisting); specify amnestic–confabulatory phenotype when present.
- ICD-11: amnestic disorder due to psychoactive substances including alcohol; separate coding for acute WE/thiamine deficiency where systems allow.
Always name the system you are using in viva answers.[8][12]
Caine operational criteria (must reproduce)
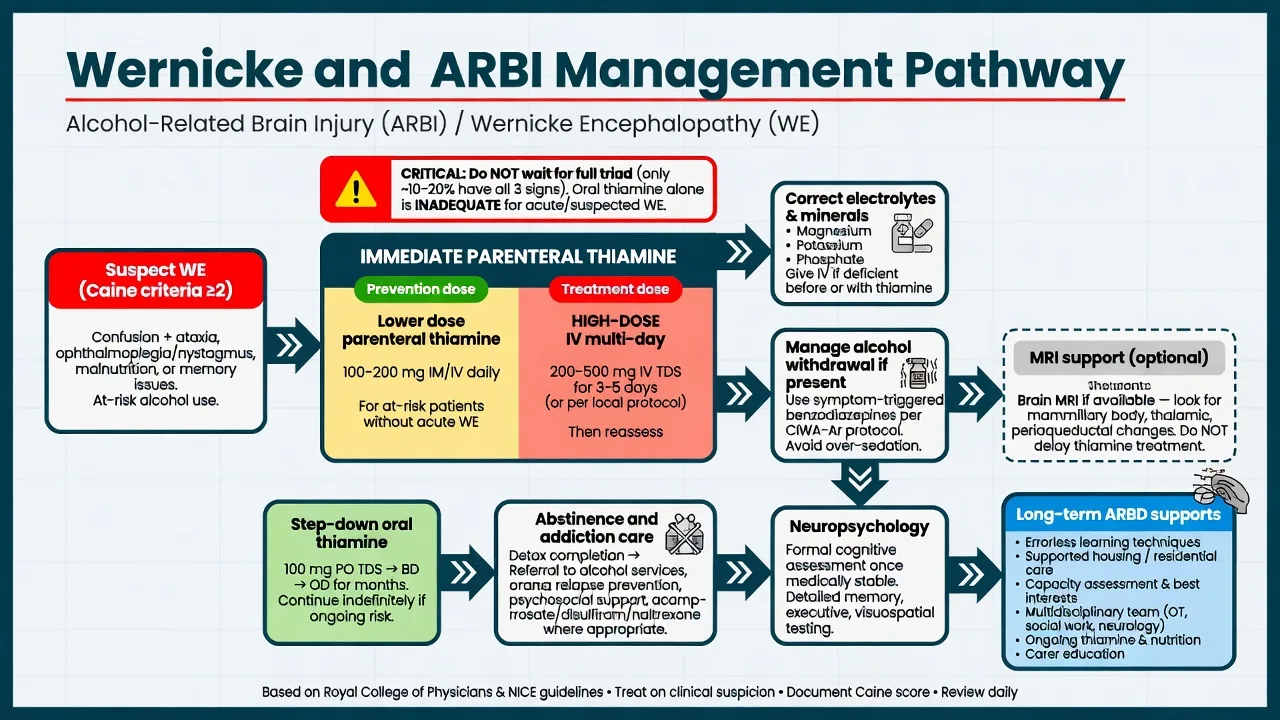
Treat as WE if any two of four are present in a person at risk: (1) dietary deficiencies; (2) oculomotor abnormalities; (3) cerebellar dysfunction; (4) altered mental state or mild memory impairment.[1]
The classic triad (confusion, ophthalmoplegia, ataxia) is incomplete in most cases — waiting for all three is an exam-failing delay.[1][2][5]
Epidemiology and risk factors
WE remains under-recognised in life; neuropathology series historically show higher prevalence than clinical diagnosis, driving the low treatment threshold.[2][5][9] KS most often follows WE in alcohol-dependent populations; residual amnesia is a major cause of long-term disability and institutional care needs in working-age adults.[6][7][8]
Risk amplifiers: severe alcohol use disorder with poor diet; repeated vomiting; homelessness; GI disease; high carbohydrate loads without thiamine cover; magnesium depletion; non-alcoholic thiamine deficiency states (bariatric surgery, hyperemesis gravidarum, cancer cachexia, dialysis, eating disorders, AIDS).[2][5][12]
Pathophysiology
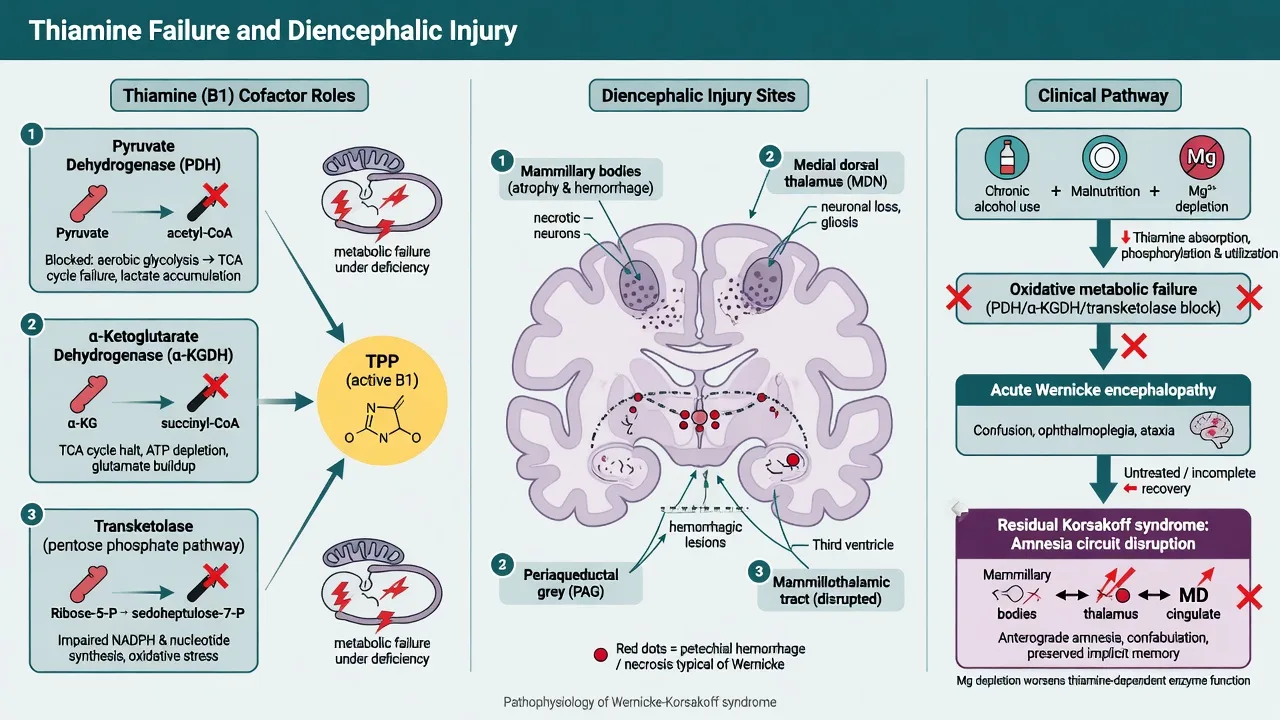
Thiamine is an essential cofactor for pyruvate dehydrogenase, alpha-ketoglutarate dehydrogenase, and transketolase. Deficiency collapses oxidative metabolism in high-demand neurons and glia.[2][5]
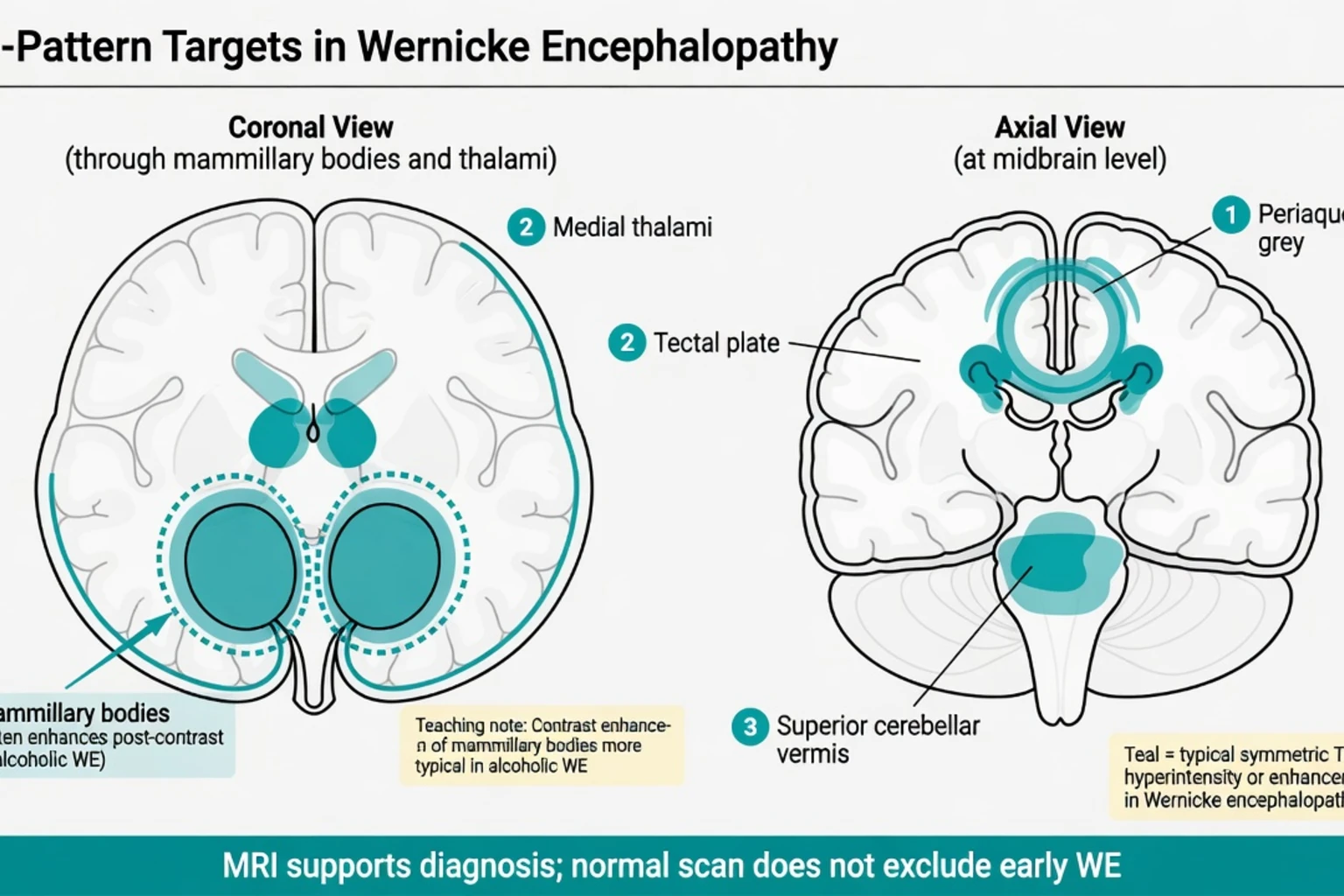
Selective vulnerability: mammillary bodies, medial dorsal thalamus, periaqueductal grey, floor of the fourth ventricle, and superior cerebellar vermis — explaining oculomotor signs, ataxia, and diencephalic amnesia.[5][9][10]
Alcohol multiplies risk through poor intake, gastrointestinal losses, reduced hepatic storage, and magnesium depletion that impairs thiamine-dependent enzyme function. Direct alcohol neurotoxicity and white-matter injury (especially frontal–cerebellar circuits) explain non-Wernicke ARBI even when classic KS is absent.[8][9][12]
KS memory failure reflects disruption of diencephalic–hippocampal networks rather than isolated “hippocampal Alzheimer” pathology; confabulation can be spontaneous (more florid, often frontal–diencephalic) or provoked (common on testing).[6][7][13]
Clinical presentation
Wernicke encephalopathy
- Altered mental state: confusion, apathy, drowsiness, or agitation
- Oculomotor: nystagmus, bilateral abducens weakness, conjugate gaze palsy
- Cerebellar: gait ataxia, dysmetria
- Autonomic instability and hypothermia can occur in severe disease
MSE: inattention may mimic delirium; document last drink timing because WE and alcohol withdrawal delirium can coexist.[1][2][5]
Korsakoff syndrome
- Dense anterograde amnesia (failure of new episodic learning)
- Variable retrograde amnesia, often temporally graded
- Relatively preserved early attention and procedural learning in classic cases
- Confabulation may be prominent but is neither necessary nor sufficient for diagnosis
- Insight often impaired; personality change, apathy, or irritability common
Broader ARBI phenotype
Executive dysfunction, poor planning, disinhibition, social cognition deficits, slowed processing, cerebellar motor signs, and peripheral neuropathy — with or without a clear KS amnestic core.[8][9]
Differential diagnosis
Discriminators matter more than lists — WE and withdrawal can coexist, and trauma or hepatic encephalopathy frequently mimic “behavioural” presentations in dependent drinkers.[2][5][12]
| Competing diagnosis | Why it confuses | Discriminators |
|---|---|---|
| Delirium tremens | Confusion + autonomic surge after stopping | Timing 48–72 h; severe autonomics; still give thiamine — can coexist with WE |
| Hepatic encephalopathy | Confusion in drinker | Asterixis, ammonia context, liver failure signs |
| Subdural / trauma | Falls in dependent drinkers | Focal signs, imaging for trauma — does not replace thiamine |
| Alzheimer disease | Memory complaints | Age, gradual multi-domain course, less abrupt WE history, different imaging |
| Vascular cognitive impairment | Stepwise decline | Vascular risks, infarct pattern |
| HSV encephalitis | Acute confusion/amnesia | Fever, seizures, temporal MRI/EEG — different emergency |
| Primary psychiatric illness | Behaviour change | Organic amnesia and oculomotor/ataxia signs redirect |
Assessment
- History: quantity/frequency alcohol, last drink, diet, weight loss, vomiting, housing, head injury, prior WE, other substances.
- Exam: nystagmus/gaze palsy, gait, neuropathy, nutritional status, trauma signs.
- Cognition: orientation, delayed recall, confabulation probes, executive bedside tasks; formal neuropsychology when medically stable.
- Risk: self-neglect, wandering, exploitation, fire, driving, suicide/depression, carer burnout.
- Capacity: treatment, discharge, finances — dense amnesia often fails to retain and weigh information; use supported decision-making and least-restrictive legal frameworks jurisdictionally.
- Collateral: essential when confabulation and amnesia distort self-report.
Investigations
- Do not delay thiamine for laboratory confirmation. If blood thiamine/erythrocyte transketolase is available, draw before the first dose when practical, then treat.[2]
- Baseline: FBC, U and E, magnesium, phosphate, glucose, LFTs, coagulation, B12/folate, TSH.
- MRI brain supports acute WE (EFNS Level B): T2/FLAIR hyperintensity in mammillary bodies, medial thalami, periaqueductal grey; contrast enhancement of mammillary bodies is particularly associated with alcoholic WE in series, and non-alcoholic WE can show more atypical patterns.[2][10][11]
- CT often normal and is mainly for trauma differentials.
- EEG/LP only when alternative diagnoses (encephalitis, non-convulsive status) are plausible.
- Neuropsychology maps KS versus broader ARBI once delirium and acute WE are treated.[6][7][14]
Acute / emergency management
Thiamine — the exam core
Principle: parenteral thiamine for suspected WE and high-risk malnourished drinkers; oral regimens are for lower-risk prophylaxis or step-down, not for treating established WE.[2][3][4]
EFNS guidance (Galvin 2010): thiamine for suspected or manifest WE; give before carbohydrate; a cited regimen is 200 mg three times daily, preferably intravenously (Level C evidence for exact dose), with parenteral thiamine for at-risk emergency presentations as good practice.[2]
UK RCP / Thomson A and E teaching and many hospital protocols emphasise high-dose parenteral B vitamins (often taught as approximately 500 mg thiamine IV three times daily for days in established WE, commonly as paired high-dose Pabrinex preparations, then step-down) because under-dosing oral/“banana bag” approaches fail to optimise CNS delivery.[3][16]
Practical fellowship answer (state both and follow local protocol): use multi-day high-dose parenteral thiamine for WE, then step down, with glucose and magnesium co-management as below.[2][3][16]
| Scenario | Typical teaching regimen | Notes |
|---|---|---|
| Suspected / established WE | High-dose IV thiamine multi-day: EFNS-style 200 mg IV TDS minimum teaching; many UK protocols ~500 mg IV TDS for 2–3+ days then step-down | Parenteral; resusc facilities for rare anaphylaxis |
| High-risk prevention (dependent drinker, poor diet, admission) | Parenteral thiamine daily for several days (protocolised lower than full treatment intensity) then oral | Do not rely on oral alone if high risk |
| Step-down / ongoing risk | Oral thiamine commonly 100 mg three times daily while drinking risk/malnutrition persists | Pair with nutrition and Mg |
| Hypoglycaemia | Give glucose with thiamine cover; do not withhold urgent glucose if thiamine co-administered | Classic trap is glucose without thiamine in at-risk patients |
Cochrane review evidence for precise optimal thiamine dosing in alcohol-related WKS is limited; guidelines and pharmacokinetic reasoning still drive high-dose parenteral practice for WE.[4][16]
Concurrent measures
- Replete magnesium, potassium, phosphate.
- Manage alcohol withdrawal with benzodiazepines when indicated (see alcohol use disorder topic) — antipsychotics are not first-line for withdrawal physiology.
- Protect airway, prevent falls/aspiration, continuous monitoring.
- Treat coexistent head injury, infection, and hepatic failure as found.
Definitive and long-term management
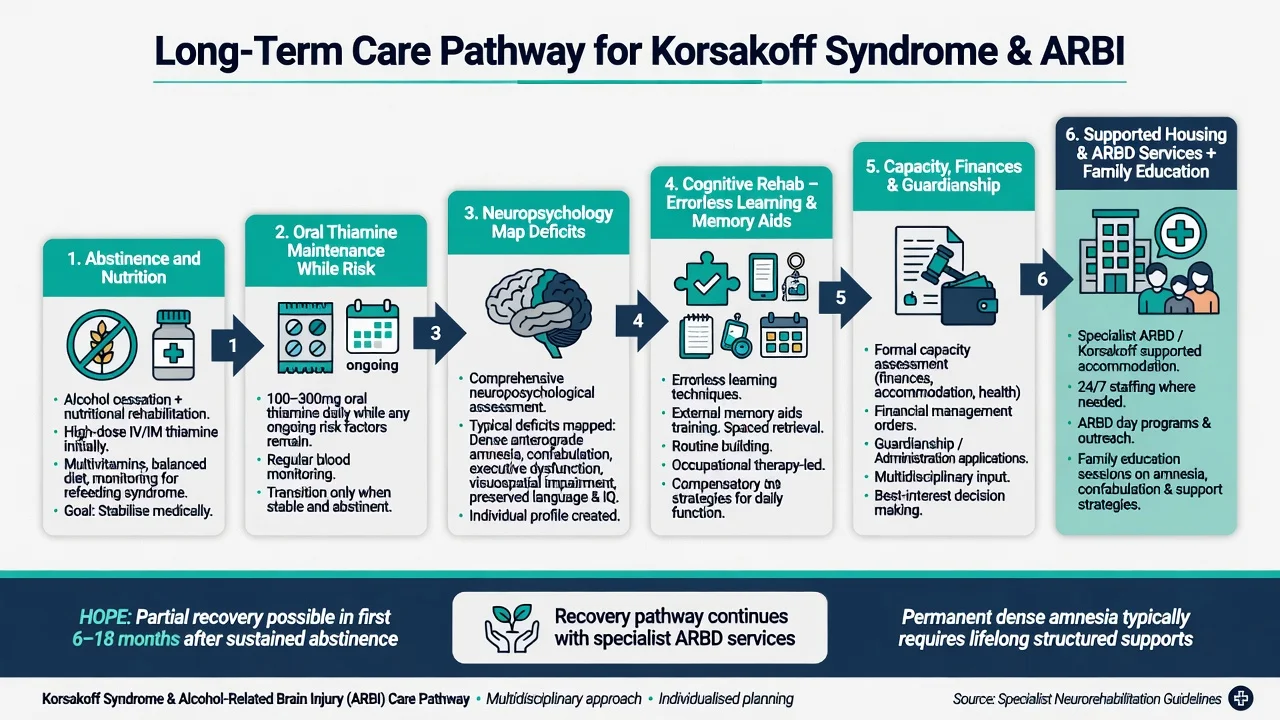
- Complete the thiamine course and continue oral maintenance while risk remains.
- Abstinence is the main disease-modifying intervention for progressive ARBI; integrate addiction treatment (motivational work, relapse-prevention medicines when appropriate, mutual aid, residential options).
- No specific pharmacological cure for established KS amnesia — avoid reflex cholinesterase-inhibitor pathways unless a separate neurodegenerative diagnosis is justified. Treat depression, psychosis, seizures, and sleep disturbance carefully.
- Cognitive rehabilitation: errorless learning, spaced retrieval, external memory aids, structured routines, environmental modification; evidence base for ARBD rehab is modest but clinically essential.[6][7][14]
- Psychosocial rehabilitation and housing: specialist ARBD community teams, supported accommodation, carer education, safeguarding.[15]
- Legal/capacity: financial administration, guardianship/substitute decision-making when needed; least restrictive option; reassess as cognition improves with abstinence.
- Secondary prevention: nutrition, thiamine, fall prevention, treat concurrent liver disease, vaccinate/hepatitis screening as indicated, dual-diagnosis mental health care.[12][15]
EFNS publishes IV thiamine 200 mg TDS as a key cited treatment figure with MRI as supportive Level B. UK RCP/Thomson-influenced ED pathways and many Australasian hospital protocols use higher multi-pair parenteral B-vitamin regimens (often taught near 500 mg thiamine IV TDS for established WE). In FRANZCP answers: name Caine threshold, parenteral route, multi-day course, local protocol dose, and Mg/glucose co-management — do not invent a single global tablet dose for acute WE.[2][3][16]
Subtypes and high-yield scenarios
- ED WE: incomplete triad, intoxicated masking, give parenteral thiamine early.[3]
- WE + DT: treat both — thiamine plus high-dose benzos/ICU, not antipsychotics-first.
- Non-alcoholic WE: bariatric, hyperemesis, malignancy — same thiamine urgency.[5]
- Insidious KS: hostel resident with confabulation and lost weeks of memory.
- Executive ARBI without dense KS: still needs abstinence and functional supports.[8]
- Older adult mixed picture: ARBI plus vascular/Alzheimer — dual pathology common; thiamine still if risk.
Complications and pitfalls
- Waiting for the full triad
- Oral thiamine only for nystagmus + ataxia + malnutrition
- Assuming normal CT excludes WE
- Missing concurrent subdural after falls
- Calling KS “Alzheimer” and missing treatable nutrition/addiction factors
- Ignoring capacity and unsafe discharge
- Over-sedation without airway/fall precautions
- Rare anaphylaxis fear delaying life-saving parenteral thiamine (have resusc readiness; still treat)
Prognosis and disposition
Ocular signs often improve fastest with thiamine; ataxia and cognitive deficits recover more slowly and often incompletely.[2][5] Established KS amnesia frequently persists, though modest gains over months can occur with abstinence, nutrition, and rehabilitation.[6][7] Broader ARBI may show meaningful recovery over months of sustained abstinence — counsel realistic hope with structured supports.[8][14][15]
Disposition ladder: medical stabilisation → exclude ongoing WE risk → addiction and nutrition plan → neuropsychology → community ARBD/rehab pathway or supported residential care if needed → capacity and safeguarding review.[7][14][15]
Special populations
- Older adults: falls, polypharmacy, mixed dementia.
- Pregnancy/hyperemesis: non-alcoholic WE — parenteral thiamine.
- Homeless and prison populations: high risk, fragmented follow-up.
- Intellectual disability: dual vulnerability; collateral critical.
- Indigenous and culturally diverse communities: access barriers, stigma, culturally safe addiction and disability supports.
Evidence and guidelines
Landmark anchors examiners expect by name: Caine 1997 operational criteria; EFNS Galvin 2010 WE diagnosis/therapy/prevention; Thomson RCP 2002 ED Wernicke guidance; Sechi and Serra 2007 modern WE review; Kopelman KS clinical psychology reviews; Arts 2017 KS critical review; Zahr/Harper ARBD neuropathology; Sullivan/Pfefferbaum and Zuccoli neuroimaging patterns; Day Cochrane on thiamine evidence limits; ICU “banana bag” critiques favouring higher-dose thiamine strategies.[1][2][3][4][5][6][7][8][10][11][16]
Exam pearls
CAINE WE
- Classic triad present in a minority — treat earlier.
- Parenteral for WE; know EFNS 200 mg IV TDS teaching versus common UK ~500 mg IV TDS treatment protocols.
- MRI supports; clinical diagnosis rules.
- KS = disproportionate memory deficit; confabulation is optional.
- ARBI ≠ automatically Korsakoff.
- Long-term wins: abstinence + structure + capacity-aware supports.
References
- [1]Caine D, Halliday GM, Kril JJ, et al. Operational criteria for the classification of chronic alcoholics: identification of Wernicke's encephalopathy. J Neurol Neurosurg Psychiatry, 1997.PMID 9010400
- [2]Galvin R, Bråthen G, Ivashynka A, et al. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur J Neurol, 2010.PMID 20642790
- [3]Thomson AD, Cook CC, Touquet R, et al. The Royal College of Physicians report on alcohol: guidelines for managing Wernicke's encephalopathy in the accident and Emergency Department. Alcohol Alcohol, 2002.PMID 12414541
- [4]Day E, Bentham PW, Callaghan R, et al. Thiamine for prevention and treatment of Wernicke-Korsakoff Syndrome in people who abuse alcohol. Cochrane Database Syst Rev, 2013.PMID 23818100
- [5]Sechi G, Serra A Wernicke's encephalopathy: new clinical settings and recent advances in diagnosis and management. Lancet Neurol, 2007.PMID 17434099
- [6]Kopelman MD, Thomson AD, Guerrini I, et al. The Korsakoff syndrome: clinical aspects, psychology and treatment. Alcohol Alcohol, 2009.PMID 19151162
- [7]Arts NJ, Walvoort SJ, Kessels RP Korsakoff's syndrome: a critical review. Neuropsychiatr Dis Treat, 2017.PMID 29225466
- [8]Zahr NM, Kaufman KL, Harper CG Clinical and pathological features of alcohol-related brain damage. Nat Rev Neurol, 2011.PMID 21487421
- [9]Harper C The neuropathology of alcohol-related brain damage. Alcohol Alcohol, 2009.PMID 19147798
- [10]Sullivan EV, Pfefferbaum A Neuroimaging of the Wernicke-Korsakoff syndrome. Alcohol Alcohol, 2009.PMID 19066199
- [11]Zuccoli G, Santa Cruz D, Bertolini M, et al. MR imaging findings in 56 patients with Wernicke encephalopathy: nonalcoholics may differ from alcoholics. AJNR Am J Neuroradiol, 2009.PMID 18945789
- [12]Connor JP, Haber PS, Hall WD Alcohol use disorders. Lancet, 2016.PMID 26343838
- [13]Kopelman MD The Korsakoff syndrome. Br J Psychiatry, 1995.PMID 7728359
- [14]Svanberg J, Evans JJ Neuropsychological rehabilitation in alcohol-related brain damage: a systematic review. Alcohol Alcohol, 2013.PMID 23955833
- [15]Wilson K, Halsey A, Macpherson H, et al. The psycho-social rehabilitation of patients with alcohol-related brain damage in the community. Alcohol Alcohol, 2012.PMID 22278316
- [16]Flannery AH, Adkins DA, Cook AM Unpeeling the Evidence for the Banana Bag: Evidence-Based Recommendations for the Management of Alcohol-Associated Vitamin and Electrolyte Deficiencies in the ICU. Crit Care Med, 2016.PMID 27002274