Psych · Addiction psychiatry
Alcohol use disorder
Also known as Alcohol dependence · Alcoholism · AUD · Alcohol withdrawal · Delirium tremens · Wernicke encephalopathy alcohol · CIWA-Ar
Exam-exhaustive fellowship topic on alcohol use disorder — DSM-5-TR versus ICD-11 nosology, epidemiology, neurobiology of dependence and withdrawal, AUDIT and CIWA-Ar, withdrawal seizures and delirium tremens, Wernicke–Korsakoff and parenteral thiamine, detox algorithms, naltrexone/acamprosate/disulfiram doses, psychosocial interventions, dual diagnosis, special populations, and multi-board guideline deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Alcohol use disorder (AUD) is the most examinable substance-use presentation in psychiatry fellowship. Examiners punish three failures: thin nosology (DSM versus ICD), incomplete withdrawal/Wernicke emergencies, and vague pharmacology without agent, dose, route, monitoring, and contraindications.[4][6][12]
Overview and definition
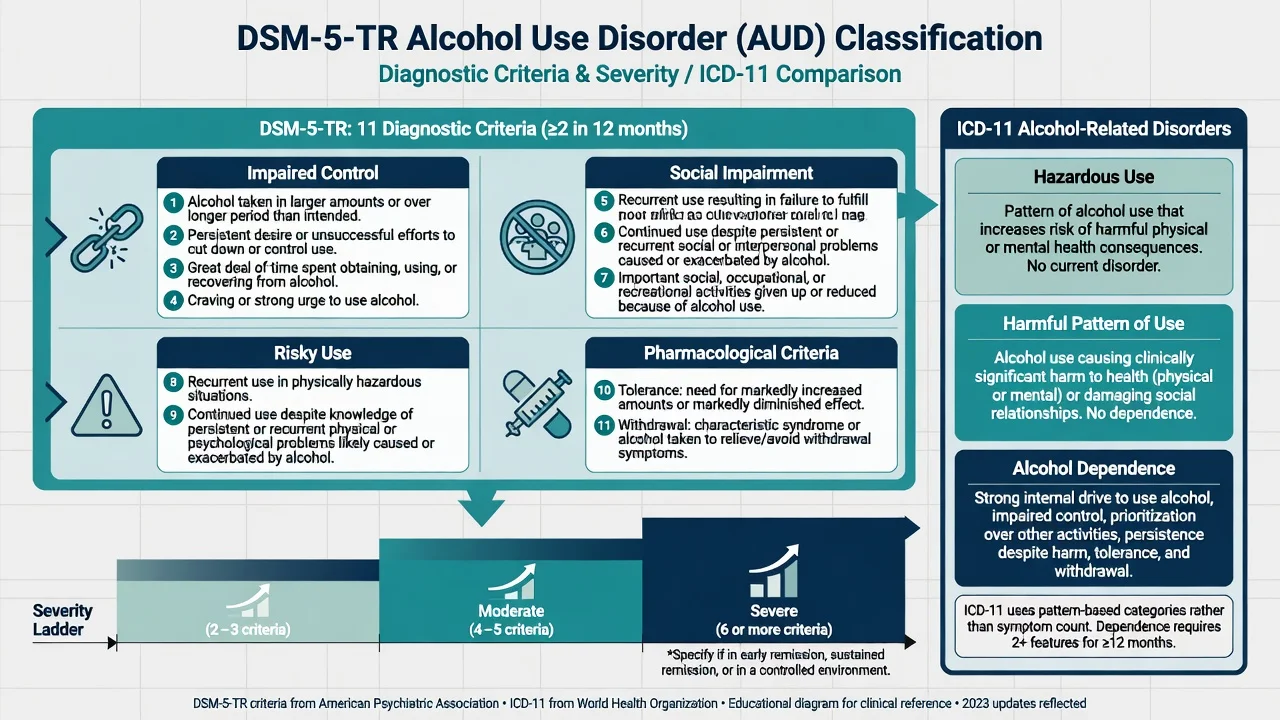
AUD is a maladaptive pattern of alcohol use leading to clinically significant impairment or distress. DSM-5-TR collapsed older abuse/dependence categories into a single spectrum disorder with eleven criteria spanning impaired control, social impairment, risky use, and pharmacological features (tolerance, withdrawal).[6][8][12]
ICD-11 keeps a more traditional public-health ladder: hazardous alcohol use, harmful pattern of use, and alcohol dependence (impaired control, alcohol taking precedence, physiological features). In viva answers, name the system you are using — examiners mark candidates who mix severity counts with ICD dependence language carelessly.[6][12]
Classification — DSM-5-TR and ICD-11
DSM-5-TR (reproduce for exam)
At least two of eleven criteria within a twelve-month period, with severity:[8][12]
| Severity | Criteria met |
|---|---|
| Mild | 2–3 |
| Moderate | 4–5 |
| Severe | 6 or more |
Domains (paraphrased accurately for teaching): 1. Impaired control — larger/longer use; desire/unsuccessful cut-down; time spent; craving; 2. Social impairment — role failure; continued use despite interpersonal problems; activities given up; 3. Risky use — hazardous situations; continued use despite physical/psychological harm; 4. Pharmacological — tolerance; withdrawal (or alcohol to relieve/avoid withdrawal).[8][12]
Specifiers include early/sustained remission and controlled environment when relevant.[12]
ICD-11 contrast (high-yield divergence)
- Hazardous use — risk-elevating pattern without established disorder.
- Harmful pattern of use — alcohol causing physical or mental harm without full dependence.
- Alcohol dependence — strong internal drive, impaired control, prioritisation, persistence despite harm, often with tolerance/withdrawal.
Related coded states examiners still ask: alcohol intoxication, alcohol withdrawal (with/without perceptual disturbance), alcohol-induced mental disorders, and amnestic syndromes (Korsakoff).[12]
Epidemiology and risk factors
In NESARC-III, twelve-month DSM-5 AUD prevalence was approximately 13.9% and lifetime approximately 29.1% among US adults, with higher rates in men, younger adults, and substantial comorbidity with other mental and substance disorders.[8] Global patterns vary by culture, policy, and availability, but the clinical message is consistent: AUD is common, undertreated, and a major driver of injury, liver disease, cancer risk, cardiovascular harm, suicide, and health-system use.[6][12]
Risk amplifiers: family history and substantial heritability; early onset of heavy drinking; trauma and adverse childhood experiences; other substance use; mood/anxiety/psychotic disorders; social isolation; high availability and low price environments.[6][12] Genetic variants affecting alcohol metabolism (for example ALDH2*2-associated flushing in East Asian populations) modulate risk and can shape culturally informed counselling.[12]
Pathophysiology
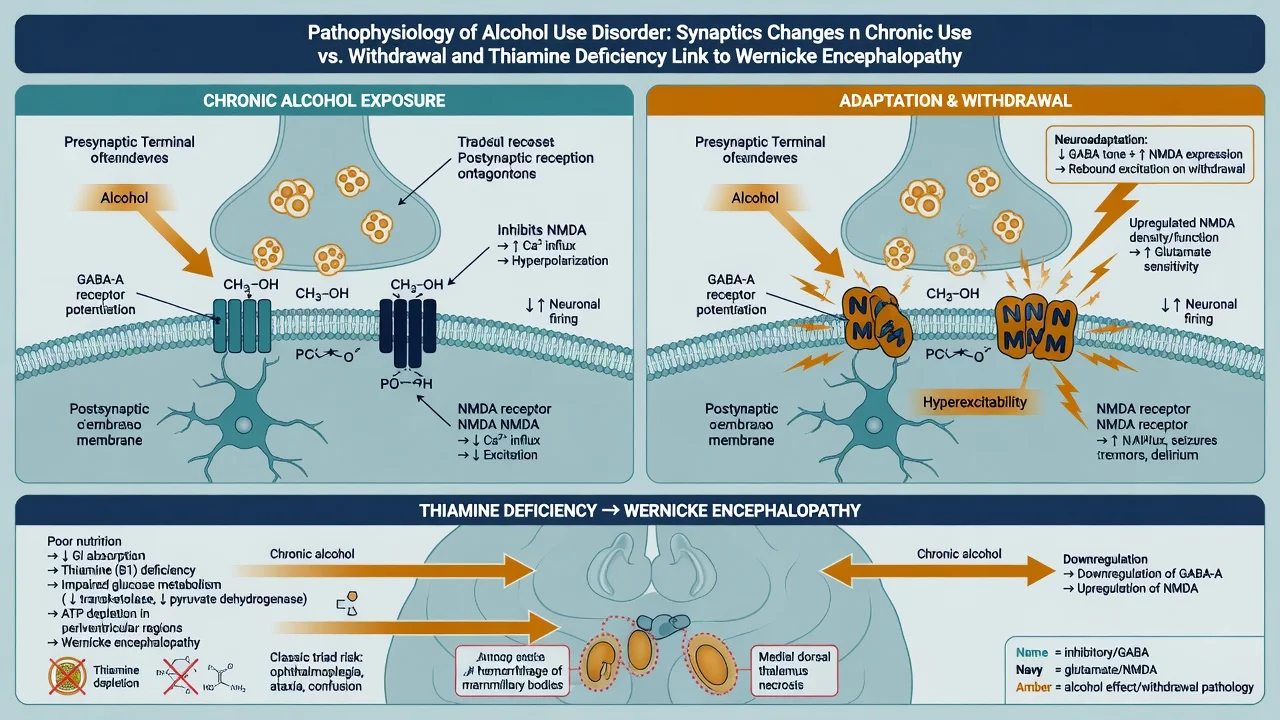
Intoxication/reinforcement. Alcohol facilitates GABA-A signalling and inhibits NMDA glutamatergic transmission; mesolimbic dopamine contributes to rewarding and habit-forming effects.[12]
Neuroadaptation. With sustained heavy use, GABAergic tone is relatively downregulated and glutamatergic/NMDA systems upregulated. Abrupt cessation produces CNS hyperexcitability — tremor, anxiety, seizures, autonomic surge, and risk of delirium tremens.[9][12]
Thiamine and Wernicke. Poor intake, gastrointestinal losses, reduced hepatic storage, and increased metabolic demand deplete thiamine (vitamin B1). Critical regions (mammillary bodies, medial thalamus, periaqueductal grey) fail oxidative metabolism → Wernicke encephalopathy; incomplete recovery yields Korsakoff amnestic syndrome.[3][11][17]
Clinical presentation
Use history that examiners want
- Quantity, frequency, binge pattern, beverage type, time of last drink
- Previous withdrawal severity, seizures, DT, detox failures
- Morning drinking, relief drinking, blackouts, drink-driving, occupational impact
- Other substances (especially benzodiazepines — dual withdrawal)
- Psychiatric comorbidity and suicide attempts
Intoxication
Disinhibition, impaired judgement, ataxia, dysarthria, nystagmus, progressive CNS and respiratory depression at high levels. Trauma and aspiration risk are part of the assessment, not afterthoughts.[12]
Withdrawal spectrum and timing
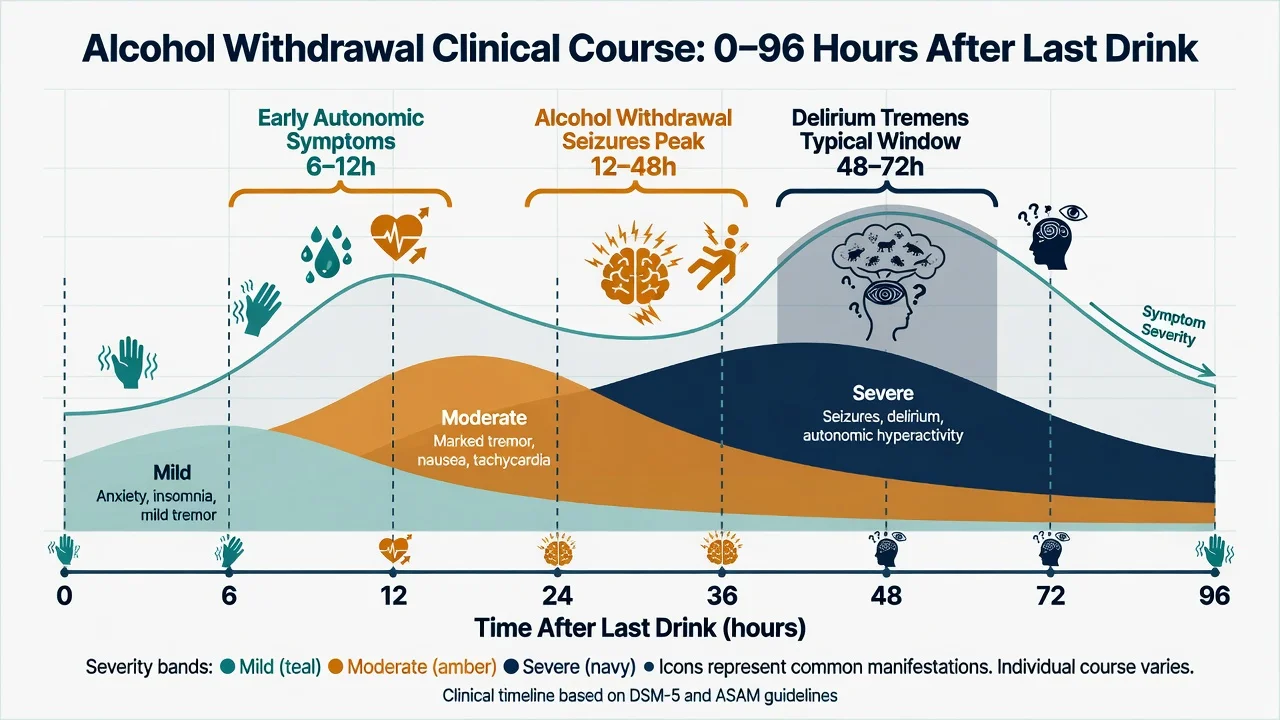
| Window after last drink (typical) | Features |
|---|---|
| ~6–12 h | Anxiety, insomnia, tremor, nausea, mild autonomic rise |
| ~12–48 h | Peak risk of withdrawal seizures (often generalised tonic-clonic) |
| ~48–72 h (can later) | Delirium tremens — fluctuating consciousness, severe autonomic hyperactivity, hallucinations |
Hallucinosis without full delirium can occur earlier. DT mortality is material if untreated — this is a medical emergency.[9][12]
Atypical presentations
Older adults with falls, confusion, or "failure to thrive"; perioperative patients whose dependence is unrecognised until day two; women and some cultural groups under-detected by quantity-focused history; dual diagnosis masking primary mood/psychosis timelines.[6][12]
Differential diagnosis
- Last drink timing fits
- Autonomic hyperactivity
- Tremor, seizures, hallucinations
- History of heavy dependence
- Responds to adequate benzodiazepines
- Malnutrition + oculomotor ± ataxia ± confusion
- Caine: any 2 of 4 features
- May coexist with withdrawal
- Needs parenteral thiamine urgently
- Do not wait for full classic triad
- Asterixis, known liver failure
- Infection, metabolic, trauma, stroke
- Drug toxicity (including benzos themselves)
- Work-up when features atypical
- May coexist with AUD
Also separate: benzodiazepine or GHB withdrawal; primary anxiety/panic; primary psychotic disorders versus alcohol-induced psychotic disorder; post-ictal states; head injury; thyrotoxicosis/sepsis mimics of autonomic surge.[9][12]
Clinical and bedside assessment
- ABCDE, vitals, glucose, SpO2; trauma survey if intoxicated.[12]
- Structured alcohol and substance history + psychiatric + medical + forensic/social.[6][12]
- AUDIT (10 items) for screening/severity signal in clinic and ED interfaces.[16]
- CIWA-Ar for symptomatic withdrawal severity when the patient can be assessed reliably.[1]
- MSE: intoxication versus withdrawal versus delirium; hallucinations; insight; capacity.[12]
- Risk: suicide, violence, vulnerability, driving, childcare, occupational safety.[6][12]
- Motivation and goals (abstinence versus reduction) — honest negotiation, not moralising.[6]
- Collateral and pharmacy/GP records when history is incomplete.[12]
- Legal status if incapacity or acute risk requires jurisdiction-specific mental health or guardianship pathways — do not invent section numbers across countries.[6][12]
AUDIT (what it is)
The WHO Alcohol Use Disorders Identification Test is a ten-item screen developed for early detection of hazardous and harmful drinking. Interpret thresholds using local protocol cut-points; higher scores increase the probability of dependence-range problems and need for full assessment.[16]
CIWA-Ar (reproduce accurately)
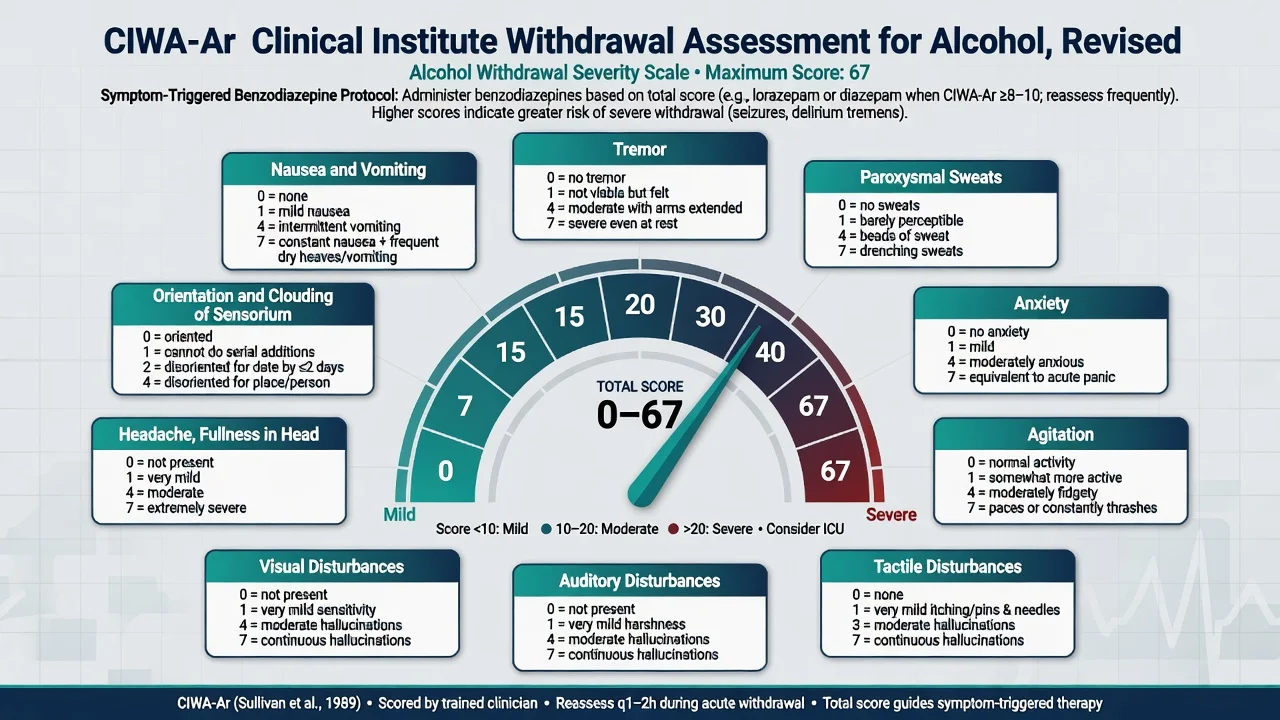
The revised Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) rates ten items (nausea/vomiting, tremor, paroxysmal sweats, anxiety, agitation, tactile/auditory/visual disturbances, headache, orientation and clouding of sensorium). Maximum total 67.[1] Local protocols map score bands to PRN benzodiazepine dosing and reassessment frequency (commonly every 1–2 hours in active withdrawal).[1][18]
Limitations: not validated as a stand-alone tool in severe medical illness, inability to communicate, or concurrent delirium of other cause — treat the physiology and do not withhold benzos solely because a score cannot be completed.[1][9]
DETACH
Investigations
There is no single lab that diagnoses AUD. Labs risk-stratify and find reversible drivers of delirium.[12]
| Priority | Tests | Why |
|---|---|---|
| Immediate | Glucose, vitals, ECG if indicated | Hypoglycaemia, instability, QT/drug context |
| Core bloods | FBC (MCV), U and E, Mg, phosphate, LFTs (GGT, AST/ALT pattern), coags | Malnutrition, electrolyte risk, liver disease |
| Adjuncts | B12/folate; beta-hCG; infection screen | Common comorbidities |
| Biomarkers (selected) | CDT, PEth, urine EtG/EtS | Monitoring/honesty adjuncts — not sole diagnosis |
| Imaging/LP | Only if focal neurology, trauma, meningitis concern | Alternative delirium causes |
Do not delay parenteral thiamine for a thiamine level when Wernicke is clinically plausible.[11][13][17]
Management — resuscitation and withdrawal
Immediate priorities
- Airway/breathing/circulation, recovery position if vomiting/intoxicated, aspiration precautions.[9][12]
- Thiamine early — parenteral when malnourished, confused, ataxic, oculomotor signs, or otherwise high Wernicke risk. Classic teaching: do not give glucose without thiamine cover in this population; if hypoglycaemia requires glucose, give thiamine concurrently/promptly.[11][13][17]
- Benzodiazepines — first-line for alcohol withdrawal (meta-analytic and guideline support).[9][19]
- Correct magnesium, potassium, phosphate and dehydration carefully.[9][12]
- Seizure management: protect airway, benzodiazepines; investigate alternative causes if first seizure or focal features.[9]
Benzodiazepine strategy
Symptom-triggered regimens guided by CIWA-Ar reduce total benzodiazepine exposure and treatment duration compared with fixed schedules in appropriate monitored settings, without loss of efficacy for preventing severe withdrawal when protocols are followed.[18][9] Fixed schedules remain useful when CIWA-Ar is impractical or risk is very high.
Agent choice (exam standard): Diazepam — long-acting; common front-line oral/IV agent where liver function allows; symptom-triggered PRN dosing per local CIWA-Ar band (example teaching band: treat when CIWA-Ar is elevated, often from around 8–10 upward depending on protocol). Lorazepam — preferred when advanced liver disease, elderly, or risk of diazepam accumulation; typical intermittent IV/oral PRN doses in protocols (commonly 1–2 mg increments, titrated). Chlordiazepoxide — still used in some UK protocols as fixed or triggered regimens.[9][18][19]
Always cite local protocol for exact milligram bands; fellowship answers must still name agents and the symptom-triggered principle.[9][18]
Setting of detox
Inpatient/supervised if: history of withdrawal seizures or DT; significant medical or psychiatric comorbidity; pregnancy; unstable housing or lack of support; polydrug dependence; failed ambulatory attempts; high suicide risk.[4][6][12]
Ambulatory detox only with reliable supports, daily review capacity, lower predicted severity, and clear escalation plan.[6][12]
Management — definitive and stepwise (post-detox)
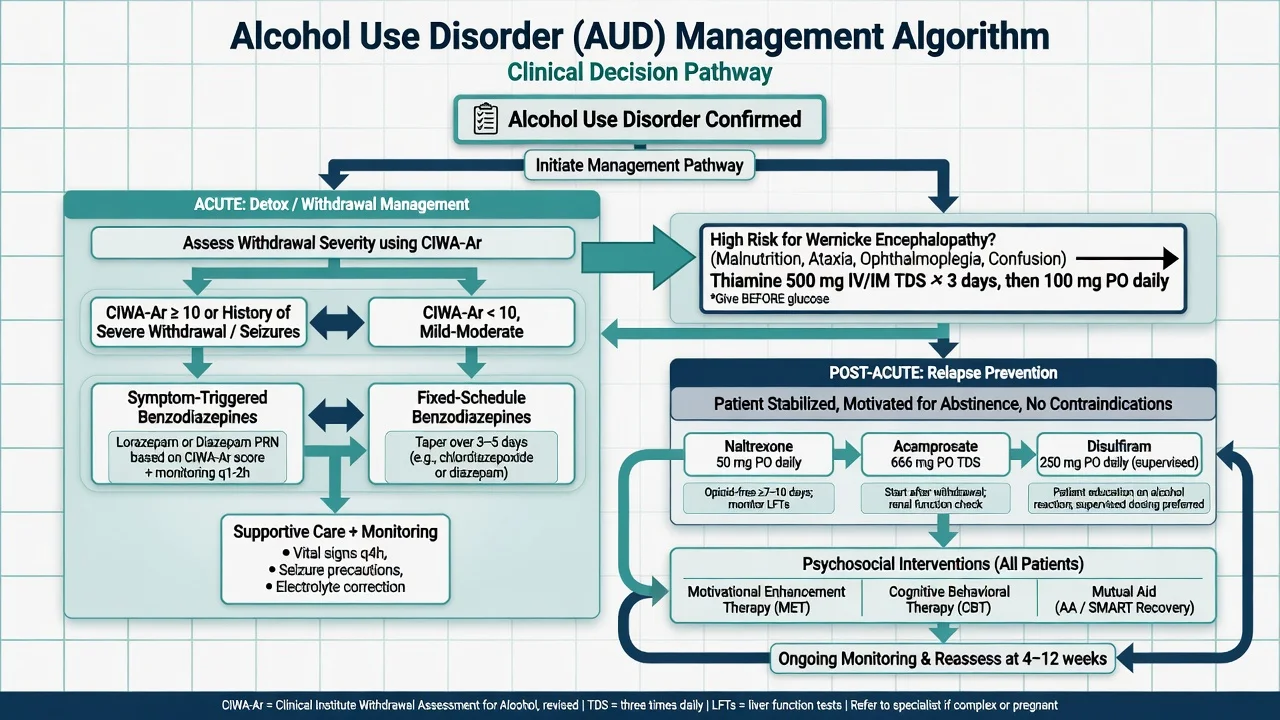
Pharmacotherapy for relapse prevention
APA pharmacological guidance supports offering evidence-based medications; naltrexone and acamprosate have the strongest overall evidence base for reducing return to heavy drinking or supporting abstinence depending on goal and population.[4][5][7]
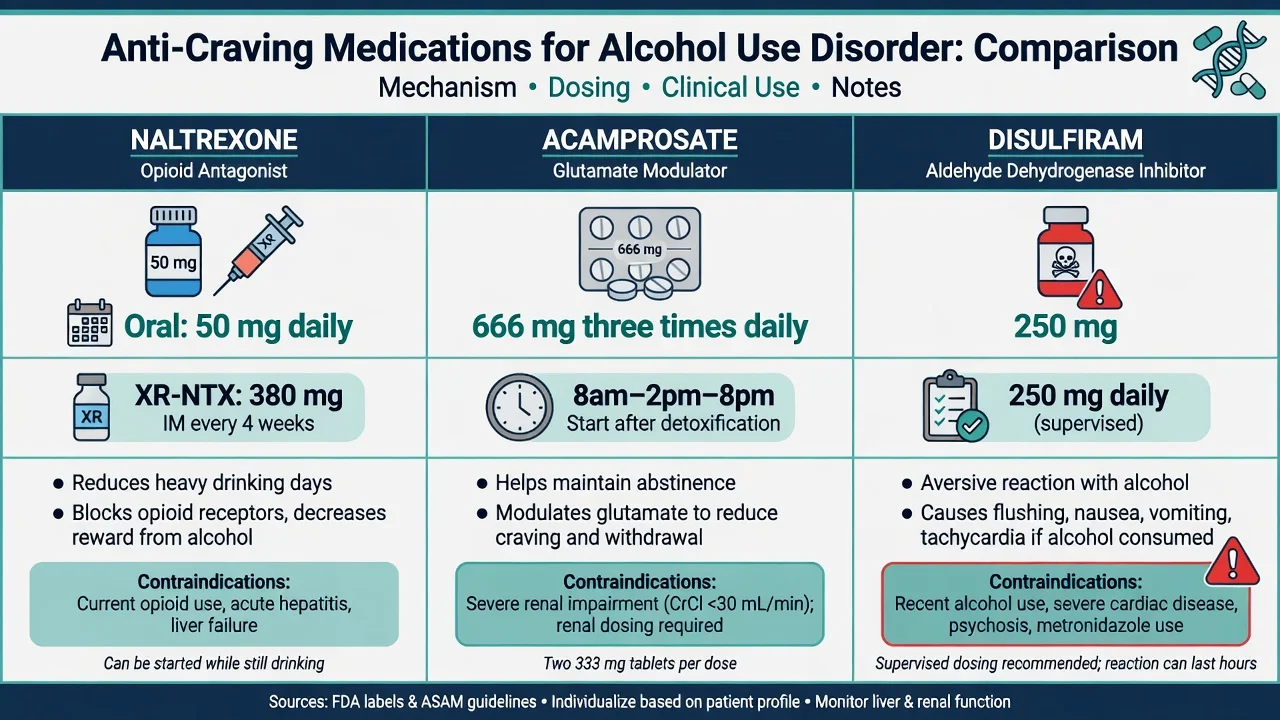
Naltrexone
- Mechanism: mu-opioid receptor antagonist; reduces alcohol reward/heavy drinking days.[10][5]
- Oral dose (standard teaching): 50 mg once daily (some start 25 mg for a few days if tolerability concern).[4][7][10]
- Long-acting injectable naltrexone (XR-NTX): monthly IM formulation improves adherence for selected patients (classic trial evidence for efficacy/tolerability).[15]
- Prerequisites: opioid-free (risk of precipitated withdrawal); counsel that opioids will not work as usual in emergency analgesia — medical alert; baseline and follow-up LFTs; avoid in acute hepatitis/liver failure per product guidance.[4][7]
- COMBINE: naltrexone with medical management improved outcomes; interpret alongside behavioural platforms.[2]
Acamprosate
- Mechanism: modulates glutamatergic (NMDA-related) hyperactivity; supports abstinence maintenance after detox.[14][5]
- Dose (standard adult with normal renal function): 666 mg three times daily (two 333 mg tablets TDS).[4][7][14]
- Renal impairment: dose-reduce or avoid in severe renal failure per product information — always check eGFR before prescribing.[4][14]
- Start: typically after detoxification when abstinence is established; does not treat acute withdrawal.[4][14]
- COMBINE nuance: acamprosate did not show expected benefit in COMBINE’s specific design — quote the trial carefully rather than over-generalising that acamprosate "does not work". Meta-analyses still support efficacy in appropriate abstinence-oriented samples.[2][5][14]
Disulfiram
- Mechanism: aldehyde dehydrogenase inhibition → aversive acetaldehyde reaction with alcohol (flushing, nausea, tachycardia, hypotension risk).[20]
- Dose: commonly 200–250 mg daily after specialist assessment (regional product strengths differ; UK often discusses 200 mg, US product teaching often 250 mg).[4][20]
- Mandatory: informed consent; supervised dosing when possible; absolute alcohol education (including some mouthwashes/foods); not for impulsive patients or those likely to drink through the reaction; caution/contraindication in significant cardiac disease, psychosis, and when adherence/supervision impossible.[4][20]
- Evidence is strongest in supervised contexts; unsupervised use underperforms.[20][7]
Other agents (know, do not over-claim)
Baclofen and nalmefene (marketed in some European settings for reduction) appear in stems as controversies or regional options — not universal first-line replacements for naltrexone/acamprosate in ANZ teaching. State evidence uncertainty and local approval status.[4][6][7]
Psychosocial interventions
Medication is adjunctive, not a complete treatment. Evidence-aligned packages include:[2][6][12]
- Motivational enhancement therapy (MET) / motivational interviewing
- Cognitive behavioural therapy for alcohol (urge surfing, high-risk planning, cognitive restructuring)
- Contingency management where available
- Twelve-step facilitation and mutual aid (AA, SMART Recovery) — offer, do not coerce ideology
- Residential rehabilitation for high severity, unstable environment, or failed community treatment
- Family interventions and social work (housing, employment, legal)
- Brief intervention for hazardous use that does not meet full dependence thresholds
Specific subtypes and scenarios
Alcohol withdrawal seizures
Usually generalised tonic-clonic within the 12–48 hour window; prior seizures predict recurrence. Benzodiazepines are the cornerstone; chronic antiepileptic drugs are not routine substitutes for adequate withdrawal management unless another epilepsy diagnosis exists.[9][19]
Delirium tremens
Fluctuating consciousness, severe autonomic hyperactivity, vivid hallucinations, global disturbance — typically day 2–3 after cessation. High-dose benzodiazepines, medical/ICU support, thiamine, electrolytes, infection and metabolic work-up.[9][12]
Wernicke encephalopathy and Korsakoff
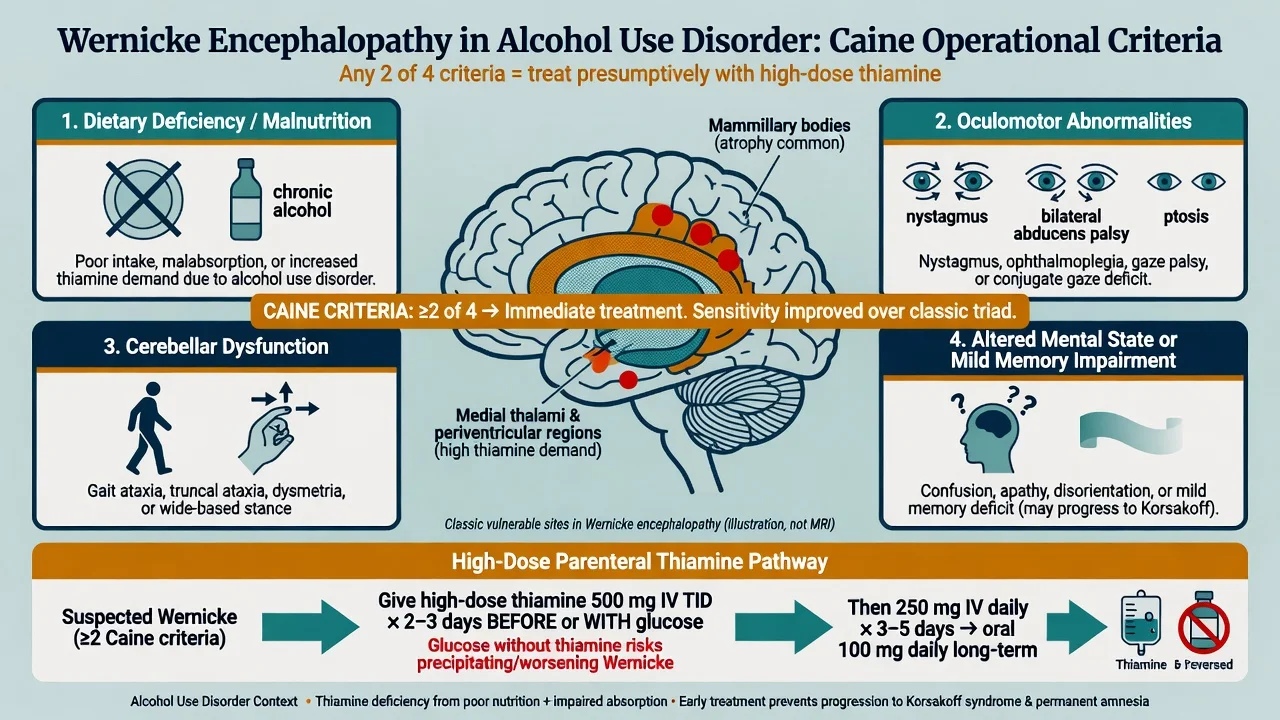
Caine operational criteria (any two of four) improve identification over waiting for the incomplete classic triad of ophthalmoplegia, ataxia, and confusion:[3]
- Dietary deficiency / malnutrition
- Oculomotor abnormalities
- Cerebellar dysfunction
- Altered mental state or mild memory impairment
Treatment intensity: EFNS and RCP-linked emergency guidance support high-dose parenteral thiamine for suspected Wernicke (commonly taught regimens use 500 mg IV three times daily for several days, then step-down — follow local product-compatible protocol and EFNS/RCP sources).[13][17] Oral thiamine alone is inadequate for established Wernicke. Prevention doses for lower-risk admitted drinkers are lower but still systematic — local protocols apply.[11][13][17]
Korsakoff syndrome: dense anterograde amnesia, confabulation variable, poor insight — rehabilitation and long-term support after the acute thiamine emergency.[3][11]
Alcohol-induced psychotic disorder / hallucinosis
Hallucinations (often auditory) with clearer sensorium than DT; still exclude medical delirium. Manage withdrawal physiology and safety; antipsychotic short-term if needed after medical stabilisation; reassess for primary psychosis after sustained abstinence.[12]
Dual diagnosis pointer
Depression, anxiety, PTSD, bipolar disorder, schizophrenia, and personality disorders commonly co-occur. Integrated care outperforms sequential "treat one then the other" in principle — see the dual-diagnosis topic for full models. Acute safety and withdrawal come first; restart or adjust psychotropics with hepatic status and interaction awareness.[6][12]
Liver disease and transplant interface
Prefer lorazepam over long-acting diazepam when cirrhosis risks accumulation. Avoid disulfiram in significant liver disease. Naltrexone needs careful LFT review. Addiction psychiatry input improves transplant candidacy processes in specialised centres.[4][12]
Complications and pitfalls
- Missing Wernicke because the classic triad is incomplete.[3][17]
- Underdosing benzodiazepines → seizure/DT; oversedation → aspiration and respiratory failure.[9][19]
- Glucose without thiamine cover in malnutrition.[13][17]
- Naltrexone started on ongoing opioids.[4]
- Unsupervised disulfiram and covert drinking.[20]
- Calling DT "behavioural" and under-treating medically.[9]
- Ignoring suicide risk in early recovery and intoxication.[6][12]
- Fixed belief that one medication works for all goals (reduction vs abstinence phenotypes differ).[5][7]
Prognosis and disposition
AUD is typically relapsing–remitting. Many people improve substantially with engagement; severity, comorbidity, social capital, and treatment adherence predict course.[6][12] After detox, default disposition packages medication plus psychosocial follow-up within days to weeks, not "discharge and good luck". Step up to residential or intensive outpatient when community care fails or risk remains high.[4][6]
Special populations
Pregnancy. Alcohol is teratogenic (FASD spectrum). Detox is specialist (obstetric + addiction); avoid disulfiram; individualise other pharmacotherapy with extreme caution; prioritise psychosocial support and safeguarding.[4][12]
Older adults. Lower consumption may still be hazardous; falls, cognitive impairment, polypharmacy, and atypical withdrawal presentations.[6][12]
Adolescents. Family-based interventions; developmental framing; careful off-label pharmacology thresholds.[6][12]
Indigenous and culturally diverse communities. Stigma, access, and historical trauma shape engagement — culturally safe care and local services matter as much as the script.[12]
Intellectual disability. Collateral history, simplified interventions, capacity assessment for treatment decisions.[6][12]
Evidence, guidelines, and regional differences
Australian Guidelines for the Treatment of Alcohol Problems and local health-service protocols drive detox setting, thiamine regimens, and prescribing. RANZCP addiction training expects CIWA-Ar competence, Wernicke prevention, and first-line anti-craving literacy (naltrexone/acamprosate/disulfiram) with psychosocial care.[12][13]
Landmark anchors to name in viva: Volpicelli naltrexone; COMBINE; Jonas outpatient pharmacotherapy meta-analysis; Maisel naltrexone/acamprosate meta-analysis; Rösner acamprosate Cochrane; Sullivan CIWA-Ar; Caine Wernicke criteria; Galvin EFNS Wernicke guideline; Daeppen/Saitz symptom-triggered detox trials.[1][2][3][5][7][10][14][17][18]
Exam pearls
- Last drink time drives the seizure/DT prediction window.[9]
- DSM severity = count of criteria; ICD-11 dependence = pattern features — do not conflate.[8][12]
- CIWA-Ar max 67; ten items; symptom-triggered benzos.[1]
- Caine: any two of four → treat as Wernicke.[3]
- Naltrexone 50 mg daily; acamprosate 666 mg TDS; disulfiram supervised 200–250 mg range.[4][7][20]
- DT is medical, not "just psych".[9]
- Dual diagnosis: stabilise withdrawal/safety, then integrated care — do not dump one disorder for the other.[6][12]
Self-test: 54-year-old day-2 post-admission
A man with decades of heavy drinking, last drink 48 hours ago, becomes agitated, sweaty, HR 128, BP 178/100, disoriented, pulling at lines, describing insects on the walls. CIWA-Ar is high. What is the working diagnosis and first-line treatment ladder?[9]
Answer. Working diagnosis: delirium tremens (timing, autonomic hyperactivity, fluctuating sensorium, hallucinations). Immediate: medical emergency pathway — IV access, monitoring, high-dose benzodiazepines titrated to control agitation/autonomics, parenteral thiamine, electrolytes (Mg/K/phosphate), exclude infection/metabolic/head injury, ICU/HDU if refractory. Not antipsychotics-first. Not "behavioural specialling" alone.[9][13][19]
References
- [1]Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict, 1989.PMID 2597811
- [2]Anton RF, O'Malley SS, Ciraulo DA, et al. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial. JAMA, 2006.PMID 16670409
- [3]Caine D, Halliday GM, Kril JJ, et al. Operational criteria for the classification of chronic alcoholics: identification of Wernicke's encephalopathy. J Neurol Neurosurg Psychiatry, 1997.PMID 9010400
- [4]Reus VI, Fochtmann LJ, Bukstein O, et al. The American Psychiatric Association Practice Guideline for the Pharmacological Treatment of Patients With Alcohol Use Disorder. Am J Psychiatry, 2018.PMID 29301420
- [5]Maisel NC, Blodgett JC, Wilbourne PL, et al. Meta-analysis of naltrexone and acamprosate for treating alcohol use disorders: when are these medications most helpful? Addiction, 2013.PMID 23075288
- [6]Knox J, Hasin DS, Larson FRR, et al. Prevention, screening, and treatment for heavy drinking and alcohol use disorder. Lancet Psychiatry, 2019.PMID 31630982
- [7]Jonas DE, Amick HR, Feltner C, et al. Pharmacotherapy for adults with alcohol use disorders in outpatient settings: a systematic review and meta-analysis. JAMA, 2014.PMID 24825644
- [8]Grant BF, Goldstein RB, Saha TD, et al. Epidemiology of DSM-5 Alcohol Use Disorder: Results From the National Epidemiologic Survey on Alcohol and Related Conditions III. JAMA Psychiatry, 2015.PMID 26039070
- [9]Mayo-Smith MF Pharmacological management of alcohol withdrawal. A meta-analysis and evidence-based practice guideline. American Society of Addiction Medicine Working Group on Pharmacological Management of Alcohol Withdrawal. JAMA, 1997.PMID 9214531
- [10]Volpicelli JR, Alterman AI, Hayashida M, et al. Naltrexone in the treatment of alcohol dependence. Arch Gen Psychiatry, 1992.PMID 1345133
- [11]Day E, Bentham PW, Callaghan R, et al. Thiamine for prevention and treatment of Wernicke-Korsakoff Syndrome in people who abuse alcohol. Cochrane Database Syst Rev, 2013.PMID 23818100
- [12]Connor JP, Haber PS, Hall WD Alcohol use disorders. Lancet, 2016.PMID 26343838
- [13]Thomson AD, Cook CC, Touquet R, et al. The Royal College of Physicians report on alcohol: guidelines for managing Wernicke's encephalopathy in the accident and Emergency Department. Alcohol Alcohol, 2002.PMID 12414541
- [14]Rösner S, Hackl-Herrwerth A, Leucht S, et al. Acamprosate for alcohol dependence. Cochrane Database Syst Rev, 2010.PMID 20824837
- [15]Garbutt JC, Kranzler HR, O'Malley SS, et al. Efficacy and tolerability of long-acting injectable naltrexone for alcohol dependence: a randomized controlled trial. JAMA, 2005.PMID 15811981
- [16]Saunders JB, Aasland OG, Babor TF, et al. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption--II. Addiction, 1993.PMID 8329970
- [17]Galvin R, Bråthen G, Ivashynka A, et al. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur J Neurol, 2010.PMID 20642790
- [18]Daeppen JB, Gache P, Landry U, et al. Symptom-triggered vs fixed-schedule doses of benzodiazepine for alcohol withdrawal: a randomized treatment trial. Arch Intern Med, 2002.PMID 12020181
- [19]Amato L, Minozzi S, Vecchi S, et al. Benzodiazepines for alcohol withdrawal. Cochrane Database Syst Rev, 2010.PMID 20238336
- [20]Fuller RK, Gordis E Does disulfiram have a role in alcoholism treatment today? Addiction, 2004.PMID 14678055