Psych · Addiction psychiatry
Alcohol withdrawal and delirium tremens
Also known as Alcohol withdrawal syndrome · AWS · Delirium tremens · DT · Alcohol withdrawal seizure · CIWA-Ar · PAWSS · Alcohol withdrawal delirium
Exam-exhaustive fellowship topic on alcohol withdrawal and delirium tremens — timeline after last drink, DSM-5-TR/ICD-11 nosology, GABA/NMDA neuroadaptation, CIWA-Ar and PAWSS, symptom-triggered versus fixed-schedule benzodiazepine protocols with named agents, seizure and DT emergencies, parenteral thiamine and Wernicke prevention, electrolytes, disposition, and ASAM/NICE/ANZ practice points.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Alcohol withdrawal and delirium tremens (DT) are among the highest-stakes addiction presentations in FRANZCP MEQs, MRCPsych papers and CASC stations, ABPN items, and MD/DNB vivas. Examiners punish three failures: wrong timeline after last drink, underpowered benzodiazepine cover for evolving DT, and missing Wernicke while chasing psychiatric labels.[7][8][14]
Overview and definition
Alcohol withdrawal syndrome (AWS) is the cluster of autonomic, neuropsychiatric, and (in severe forms) seizing or delirious features that follow cessation or marked reduction of heavy, prolonged alcohol use. It is a medical emergency spectrum on the background of alcohol use disorder (AUD) / alcohol dependence — not a behavioural problem and not synonymous with intoxication.[7][11][14]
DT (alcohol withdrawal delirium) is the severe end: fluctuating consciousness, severe autonomic hyperactivity, agitation, and often vivid hallucinations. Untreated historical mortality was substantial; modern supportive care and adequate sedative-hypnotic treatment lower mortality, but risk remains if recognition is late or cover is timid.[3][8]
Classification — DSM-5-TR and ICD-11
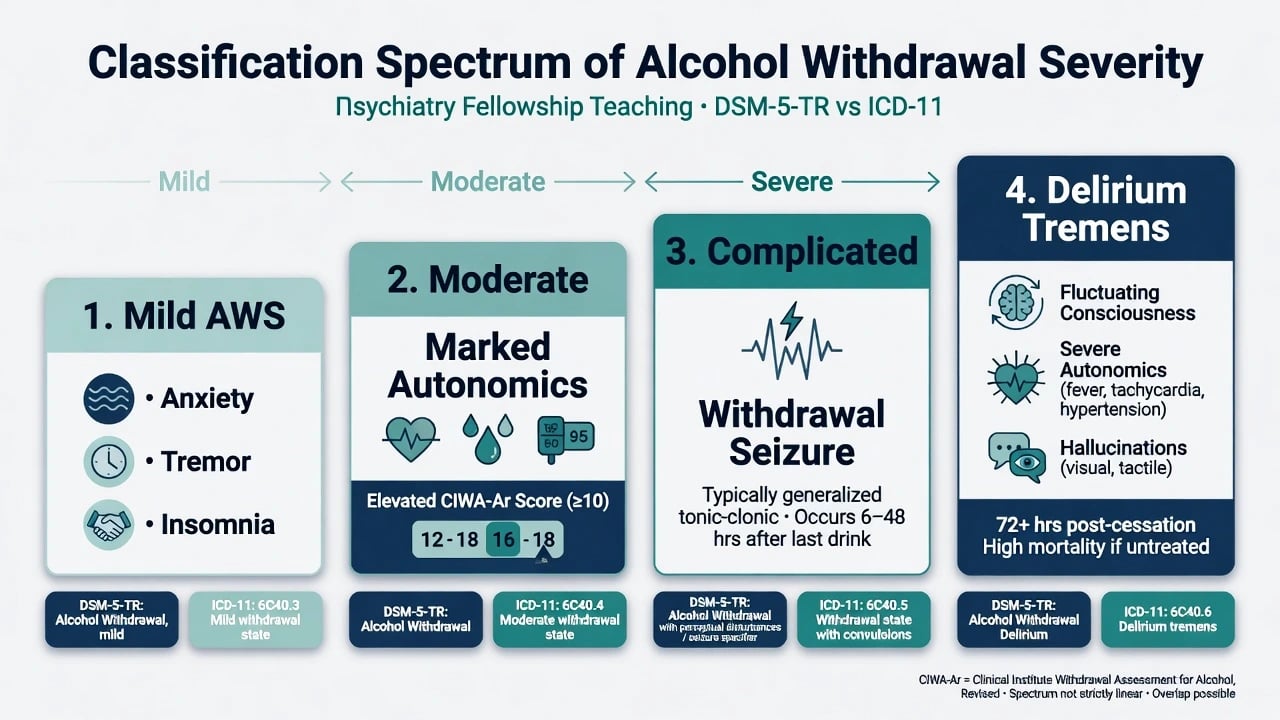
DSM-5-TR Alcohol Withdrawal (exam-ready structure)
After cessation/reduction of heavy prolonged alcohol use, two or more of: autonomic hyperactivity (e.g. sweating, pulse greater than 100); increased hand tremor; insomnia; nausea or vomiting; transient visual, tactile, or auditory hallucinations or illusions; psychomotor agitation; anxiety; generalised tonic-clonic seizures — causing distress or impairment and not better explained by another medical or mental disorder or other substance.[8][14]
Specify with perceptual disturbances when hallucinations/illusions occur with intact reality testing in the absence of delirium. Full delirium in this context is managed as withdrawal delirium / DT.[8]
ICD-11 contrast
ICD-11 codes alcohol withdrawal with or without perceptual disturbances and separately frames alcohol-induced delirium. State the manual you are using; do not mix DSM criterion counts with ICD labels carelessly.[14]
Clinical severity ladder (teaching frame)
| Band | Typical features | Setting bias |
|---|---|---|
| Mild | Anxiety, tremor, insomnia, mild autonomics | May be ambulatory if low risk |
| Moderate | Marked autonomics, elevated CIWA-Ar | Often inpatient monitoring |
| Complicated | Withdrawal seizure | Inpatient; treat physiology + work-up |
| DT | Fluctuating consciousness + severe autonomics ± hallucinations | Monitored bed / ICU |
Epidemiology and risk
Alcohol is a leading global contributor to disease, injury, and economic cost; withdrawal is the acute inpatient face of that burden among dependent drinkers.[15][14] Most AWS is mild–moderate; a minority escalate to seizures or DT. Prior complicated withdrawal is the strongest clinical predictor that the next episode may also be complicated.[11][13]
Risk amplifiers for complicated withdrawal / DT: prior seizures or DT; high daily consumption and long duration of dependence; concurrent acute medical illness; greater number of days since last drink at presentation; older age; electrolyte and nutritional depletion; concurrent sedative-hypnotic dependence; unstable housing and failed prior outpatient detox.[11][12][13] In Ferguson and colleagues' inpatient series, concurrent medical illness and longer time since last drink predicted DT development; risk rose when both factors were present.[13]
Pathophysiology
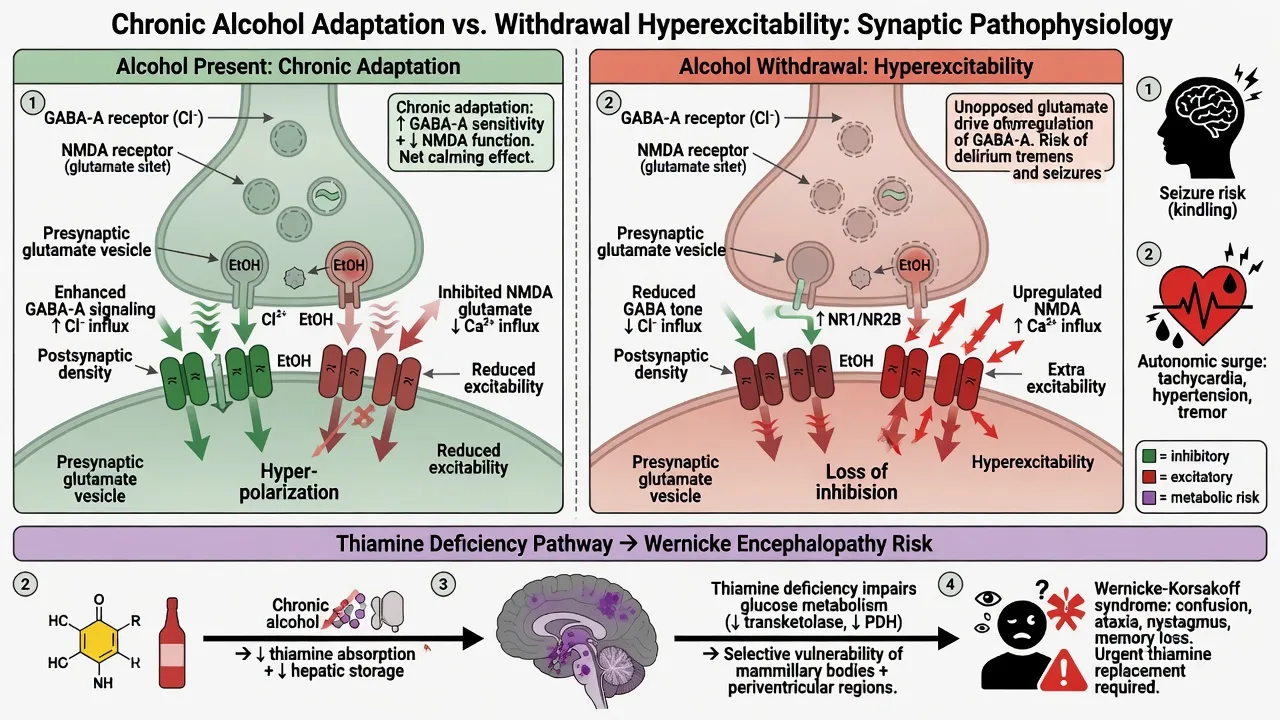
During heavy use. Alcohol facilitates GABA-A signalling and inhibits NMDA glutamatergic transmission; mesolimbic dopamine contributes to reinforcement of drinking.[7][14]
Neuroadaptation. Sustained exposure downregulates relative GABAergic tone and upregulates NMDA/glutamate systems, with hypothalamic–pituitary–adrenal and autonomic set-point change. Abrupt cessation produces CNS hyperexcitability (tremor, anxiety, seizures) and sympathetic surge (tachycardia, hypertension, sweating, hyperthermia in severe cases).[7][8]
Kindling (viva nuance). Repeated untreated or severe withdrawals may sensitize subsequent episodes — clinical implication: take prior complicated withdrawal seriously even if the current early exam looks mild.[7][11]
Why benzodiazepines work. Benzodiazepines are cross-tolerant GABA-A agonists that restore inhibitory tone and remain first-line pharmacotherapy for AWS and DT across meta-analyses and guidelines.[2][6][11]
Thiamine intersection. Poor intake, gastrointestinal losses, and reduced hepatic storage deplete thiamine; high-demand diencephalic structures fail oxidative metabolism → Wernicke encephalopathy, which may coexist with withdrawal and must not wait for the classic triad.[9][10]
Clinical presentation and timeline

| Typical window after last drink | Features |
|---|---|
| ~6–12 h | Anxiety, insomnia, tremor, nausea, mild tachycardia/hypertension, sweating |
| ~12–48 h | Peak risk of generalised tonic-clonic withdrawal seizures (often single; can cluster) |
| ~48–72 h (can later) | DT — fluctuating consciousness, severe autonomics, agitation, hallucinations |
| Variable earlier | Hallucinosis with clearer sensorium (not full delirium) |
History that scores marks: quantity and frequency, beverage pattern, exact last drink time, prior seizures/DT/detox failures, morning relief drinking, other substances (especially benzodiazepines), medical comorbidity (liver, infection, trauma), nutrition, housing and supports, psychiatric comorbidity and suicide risk.[11][14]
Atypical presentations. Older adults with falls or isolated confusion; perioperative patients decompensating on day two; women under-detected by male-normed quantity heuristics; dual diagnosis masking timelines.[14]
Differential diagnosis
- Last drink timing fits course
- Autonomic hyperactivity and tremor
- Seizures and/or fluctuating consciousness
- History of heavy dependence
- Improves with adequate benzodiazepines
- Malnutrition + oculomotor ± ataxia ± confusion
- Caine: any 2 of 4 features
- May coexist with withdrawal
- Needs parenteral thiamine urgently
- Do not wait for full classic triad
- Infection, hypoxia, metabolic, stroke, subdural
- Hepatic encephalopathy if cirrhotic
- Benzodiazepine or GHB withdrawal
- Primary psychosis with clearer sensorium
- NMS / serotonin syndrome / thyrotoxicosis when history incomplete
Discriminators examiners love: clouded fluctuating consciousness favours DT or medical delirium over pure alcoholic hallucinosis; asterixis and known decompensated liver disease raise hepatic encephalopathy; fever always forces infection work-up even when DT is likely; focal neurology forces neuroimaging.[8][13]
Bedside assessment
- ABCDE, vitals, glucose, SpO2; trauma survey if intoxicated, post-ictal, or after a fall.[7][11]
- Structured alcohol/substance history with last drink time and prior complicated withdrawal.[11][14]
- MSE: level of consciousness, fluctuation, orientation, hallucination modality, insight, capacity (especially self-discharge).[8]
- Risk: suicide, violence, vulnerability, absconding to drink, driving/childcare when relevant.[14]
- Scales: CIWA-Ar for severity when assessable; PAWSS for prediction of moderate–severe AWS in hospitalised adults where protocolised; AUDIT for broader AUD screening context.[1][12][16]
- Collateral, GP/pharmacy records, and legal status if incapacity or acute risk requires jurisdiction-specific pathways — use least-restrictive principles; do not invent foreign statute numbers.[11][14]
CIWA-Ar (must-know scale)
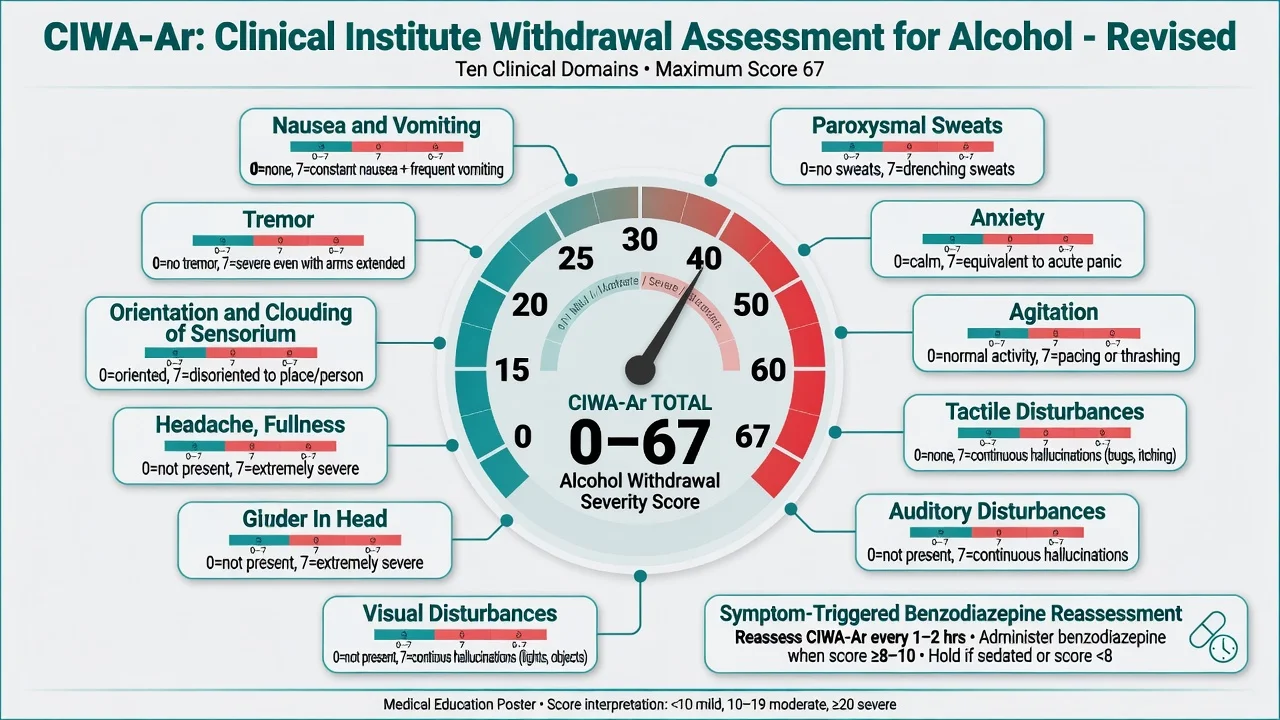
The revised Clinical Institute Withdrawal Assessment for Alcohol (CIWA-Ar) rates ten items: nausea/vomiting; tremor; paroxysmal sweats; anxiety; agitation; tactile, auditory, and visual disturbances; headache; orientation and clouding of sensorium. Maximum total 67.[1] Local protocols map score bands to PRN benzodiazepine dosing and reassessment frequency (commonly every 1–2 hours while actively withdrawing).[1][5][11]
Limits: do not use CIWA-Ar as a sole decision tool when the patient cannot communicate, is intubated, or has severe concurrent medical illness — treat physiology and do not withhold benzos for a falsely low or unobtainable score.[1][11]
PAWSS (prediction, not severity alone)
The Prediction of Alcohol Withdrawal Severity Scale (PAWSS) is a validated tool to identify medically ill inpatients at elevated risk of moderate-to-severe AWS (including seizures and DT). A score of 4 or higher indicates high risk and supports proactive monitoring and prophylaxis protocols where used.[12] Pair PAWSS risk stratification with clinical judgement; it complements rather than replaces CIWA-Ar monitoring of established withdrawal.[11][12]
LAST-DRINK
Investigations
Always consider: FBC (MCV), U and E, magnesium, phosphate, glucose, LFTs, coagulation; ECG if arrhythmia risk or QT-prolonging co-medication; pregnancy test when relevant.[11][14]
Selective: CT head for trauma, first seizure with red flags, focal neurology, or unexplained prolonged low GCS; septic work-up when fever or medical illness is present — DT and infection coexist.[8][13] Blood ethanol documents recent use but a still-detectable level does not exclude evolving withdrawal as the level falls.[7]
Do not delay thiamine for laboratory confirmation of deficiency.[9][10]
Acute management — resuscitation and protocols
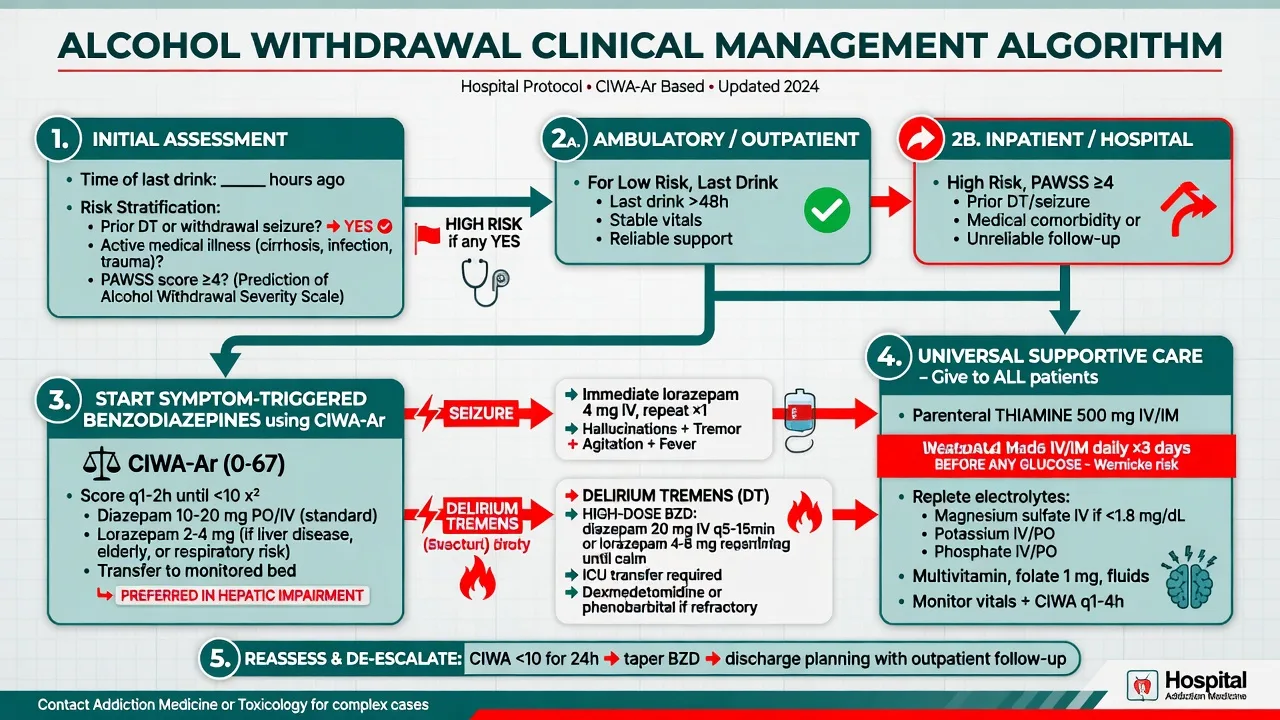
Setting selection
Ambulatory / community detox only when risk is low: no prior seizures/DT, medical stability, reliable support and follow-up, ability to take oral medication, and no major polydrug or housing crisis. Inpatient default for prior complicated withdrawal, high PAWSS, rising CIWA trajectory, acute medical illness, pregnancy, unstable housing, failed outpatient attempts, or inability to engage safely.[7][11]
Benzodiazepines — first-line
Benzodiazepines reduce withdrawal severity and protect against seizures versus placebo; they are the evidence-backed cornerstone of AWS pharmacotherapy.[2][6]
Agent choice (name it): diazepam for many long-acting/loading protocols in medically suitable adults; lorazepam (or oxazepam in some formularies) when significant hepatic impairment or elderly frailty risks metabolite accumulation.[2][7][11]
| Agent | Typical teaching role | Pearls |
|---|---|---|
| Diazepam | Long-acting; common for symptom-triggered or loading regimens in medically suitable adults | Active metabolites; avoid accumulation in severe liver disease/elderly |
| Lorazepam | Preferred when significant hepatic impairment, elderly frailty, or need for more predictable intermediate action | No active metabolites; oral/IM/IV per local protocol |
| Oxazepam | Alternative short/intermediate agent in liver disease in some regions | Local formulary dependent |
Illustrative symptom-triggered starting ranges taught in many hospital protocols (always follow local CIWA order set): diazepam 10–20 mg oral (or IV when protocol allows) for elevated CIWA scores, repeated on reassessment; or lorazepam 1–4 mg oral/IV depending on severity and route availability, titrated to control of autonomics and agitation.[2][5][7][11] Fixed-schedule regimens remain acceptable when CIWA cannot be applied or staffing cannot deliver frequent reassessment.[4][5][11]
Symptom-triggered versus fixed-schedule
Saitz and colleagues showed that individualised / symptom-triggered dosing reduced total benzodiazepine exposure and treatment duration versus fixed schedules without loss of safety in appropriate candidates.[4] Daeppen and colleagues similarly found symptom-triggered diazepam used less drug and shorter treatment than fixed-schedule dosing.[5] ASAM guidance supports structured assessment-driven treatment within a monitored protocol.[11]
Alcohol withdrawal seizures
- Protect airway, abort ongoing seizure with benzodiazepines per emergency protocol, then treat the underlying withdrawal with adequate ongoing benzo cover.[2][6][7]
- Typical timing ~12–48 h after last drink; often generalised tonic-clonic.[8]
- Investigate alternative causes when first seizure, focal features, prolonged post-ictal state, head trauma, or metabolic derangement are present.[8][11]
- Phenytoin is not first-line for pure alcohol withdrawal seizures; fix GABA deficiency and electrolytes.[2][7]
Delirium tremens
Evidence-based DT care emphasises rapid control of agitation with parenteral rapid-acting sedative-hypnotic agents cross-tolerant with alcohol — benzodiazepines are standard — plus supportive ICU-capable care.[3][8] Large cumulative doses may be required; underdosing leaves the patient at risk of injury, rhabdomyolysis, arrhythmias, and death. Antipsychotics may sometimes be added for severe perceptual agitation after adequate GABA cover, but they are not monotherapy for DT physiology.[3][8][11] Specialist ICU pathways may use adjunctive agents (e.g. phenobarbital or dexmedetomidine) in refractory cases under critical-care governance.[11]
Thiamine and Wernicke prevention
For suspected Wernicke or high risk, give high-dose parenteral thiamine urgently. EFNS-aligned teaching commonly cites thiamine 500 mg IV three times daily for several days, then step-down to lower parenteral then oral dosing per local protocol; oral thiamine alone is inadequate when absorption and severity are uncertain.[10] Give thiamine promptly when glucose is administered in malnourished patients (co-administration practice — do not withhold needed glucose).[10][11]
Supportive care
Quiet low-stimulation environment; fall and seizure precautions; aspiration risk management; IV fluids as needed; replete magnesium, potassium, and phosphate; treat hypoglycaemia; monitor for refeeding issues in severely malnourished patients.[7][11] Multivitamins and folate are adjunctive; they do not replace high-dose thiamine when Wernicke is suspected.[10]
Definitive care after stabilisation and disposition
Once CIWA trajectory falls and medical stability returns, plan addiction follow-up rather than celebrating detox alone. Link to AUD pharmacotherapy (e.g. naltrexone, acamprosate, supervised disulfiram when appropriate) and psychosocial care — detailed in the alcohol use disorder atlas leaf — and address dual diagnosis, housing, and mutual-aid options.[14] Document capacity discussions if the patient seeks premature discharge; high-risk self-discharge after early complicated withdrawal is a classic systems failure.[11][14]
Subtypes and high-yield scenarios
- Uncomplicated mild–moderate AWS — CIWA-guided benzos, thiamine risk assessment, ambulatory only if criteria met.[4][5][11]
- Withdrawal seizure — GABA cover + seizure first aid + selective work-up.[2][6]
- DT — high-dose benzos, monitoring/ICU, exclude co-delirium causes.[3][8]
- Perceptual disturbance without delirium — still treat withdrawal; safety nursing.[8]
- Perioperative unrecognised dependence — day-1–3 ward crisis; PAWSS/history screening helps.[12]
- Cirrhosis — prefer lorazepam (or oxazepam) over accumulating diazepam.[7][11]
- Dual alcohol–benzodiazepine withdrawal — prolonged course; do not strip GABA cover abruptly.[7]
- Pregnancy — maternal–fetal risk of severe untreated withdrawal; specialist obstetric-addiction care; thiamine; protocolised benzos when indicated.[11][14]
Complications and pitfalls
Other complications: injuries from agitation or seizures, rhabdomyolysis, arrhythmias, aspiration pneumonia, residual cognitive injury if Wernicke or trauma coexist, and iatrogenic prolonged sedation.[3][8]
Prognosis and course
Most uncomplicated AWS settles over days with adequate treatment. DT lasts longer and needs sustained monitoring. Prior complicated withdrawal, medical illness, high consumption, and delayed presentation predict worse courses.[8][13] Prognosis after discharge hinges on engagement with AUD care, social supports, and comorbidity treatment — detox without a plan is a revolving door.[14]
Special populations
Older adults. Atypical confusion and falls; lower benzo doses; polypharmacy interactions; higher delirium risk from medical illness.[8][11]
Liver disease. Prefer lorazepam/oxazepam; avoid heavy diazepam loading without senior oversight.[7][11]
ICU / ventilated patients. CIWA is limited; use RASS or ICU-specific AWS protocols.[11]
Cultural safety. Reduce stigma, use interpreters, and address access barriers; Indigenous and other priority populations need trauma-informed, non-punitive pathways.[14]
Youth. Less common severe AWS than adults but high-stakes when present; involve family and specialist youth addiction services.[14]
Evidence and regional guideline deltas
[2] [3] [10] [11]Landmark evidence stack for viva name-drops: Mayo-Smith 1997 (benzodiazepines for AWS); Saitz 1994 and Daeppen 2002 (symptom-triggered regimens); Amato Cochrane 2010 (benzos, seizure protection); Mayo-Smith 2004 (DT management); Kosten and O'Connor 2003 and Schuckit 2014 (clinical reviews); Sullivan CIWA-Ar; Maldonado PAWSS; Caine and Galvin for Wernicke.[1][2][3][4][5][6][7][8][9][10][12]
Exam pearls
- Last drink time predicts seizure (~12–48 h) and DT (~48–72 h) windows.[8]
- CIWA-Ar: ten items, max 67; symptom-triggered benzos when assessable.[1][5]
- PAWSS ≥4: high risk of moderate–severe AWS in hospitalised patients.[12]
- DT: benzos first, high dose if needed, ICU-capable care; not antipsychotics monotherapy.[3][8]
- Caine any 2 of 4 → treat as Wernicke; thiamine 500 mg IV TDS-style high-dose parenteral regimens per EFNS/local protocol.[9][10]
- Liver disease → lorazepam (or oxazepam) over diazepam accumulation.[7][11]
- Prior DT/seizure → inpatient default.[11][13]
- Dual BZD–alcohol dependence → expect a longer, riskier course.[7]
References
- [1]Sullivan JT, Sykora K, Schneiderman J, et al. Assessment of alcohol withdrawal: the revised clinical institute withdrawal assessment for alcohol scale (CIWA-Ar). Br J Addict, 1989.PMID 2597811
- [2]Mayo-Smith MF Pharmacological management of alcohol withdrawal. A meta-analysis and evidence-based practice guideline. JAMA, 1997.PMID 9214531
- [3]Mayo-Smith MF, Beecher LH, Fischer TL, et al. Management of alcohol withdrawal delirium. An evidence-based practice guideline. Arch Intern Med, 2004.PMID 15249349
- [4]Saitz R, Mayo-Smith MF, Roberts MS, et al. Individualized treatment for alcohol withdrawal. A randomized double-blind controlled trial. JAMA, 1994.PMID 8046805
- [5]Daeppen JB, Gache P, Landry U, et al. Symptom-triggered vs fixed-schedule doses of benzodiazepine for alcohol withdrawal: a randomized treatment trial. Arch Intern Med, 2002.PMID 12020181
- [6]Amato L, Minozzi S, Vecchi S, et al. Benzodiazepines for alcohol withdrawal. Cochrane Database Syst Rev, 2010.PMID 20238336
- [7]Kosten TR, O'Connor PG Management of drug and alcohol withdrawal. N Engl J Med, 2003.PMID 12724485
- [8]Schuckit MA Recognition and management of withdrawal delirium (delirium tremens). N Engl J Med, 2014.PMID 25427113
- [9]Caine D, Halliday GM, Kril JJ, et al. Operational criteria for the classification of chronic alcoholics: identification of Wernicke's encephalopathy. J Neurol Neurosurg Psychiatry, 1997.PMID 9010400
- [10]Galvin R, Bråthen G, Ivashynka A, et al. EFNS guidelines for diagnosis, therapy and prevention of Wernicke encephalopathy. Eur J Neurol, 2010.PMID 20642790
- [11]The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management The ASAM Clinical Practice Guideline on Alcohol Withdrawal Management. J Addict Med, 2020.PMID 32511109
- [12]Maldonado JR, Sher Y, Das S, et al. Prospective Validation Study of the Prediction of Alcohol Withdrawal Severity Scale (PAWSS) in Medically Ill Inpatients: A New Scale for the Prediction of Complicated Alcohol Withdrawal Syndrome. Alcohol Alcohol, 2015.PMID 25999438
- [13]Ferguson JA, Suelzer CJ, Eckert GJ, et al. Risk factors for delirium tremens development. J Gen Intern Med, 1996.PMID 8842933
- [14]Connor JP, Haber PS, Hall WD Alcohol use disorders. Lancet, 2016.PMID 26343838
- [15]Rehm J, Mathers C, Popova S, et al. Global burden of disease and injury and economic cost attributable to alcohol use and alcohol-use disorders. Lancet, 2009.PMID 19560604
- [16]Saunders JB, Aasland OG, Babor TF, et al. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on Early Detection of Persons with Harmful Alcohol Consumption-II. Addiction, 1993.PMID 8329970