Psych · Addiction psychiatry
Benzodiazepine dependence
Also known as Benzodiazepine use disorder · Sedative hypnotic anxiolytic use disorder · BZD dependence · Benzodiazepine withdrawal · Z-drug dependence · Benzodiazepine deprescribing
Exam-exhaustive fellowship topic on benzodiazepine dependence — DSM-5-TR/ICD-11 nosology, GABA-A tolerance and withdrawal including seizures, half-life classification, Z-drugs, structured taper and diazepam substitution, elderly falls and cognition, legitimate short-term use, alcohol and opioid interactions, deprescribing evidence (EMPOWER, Canadian BRZA, joint tapering CPG). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
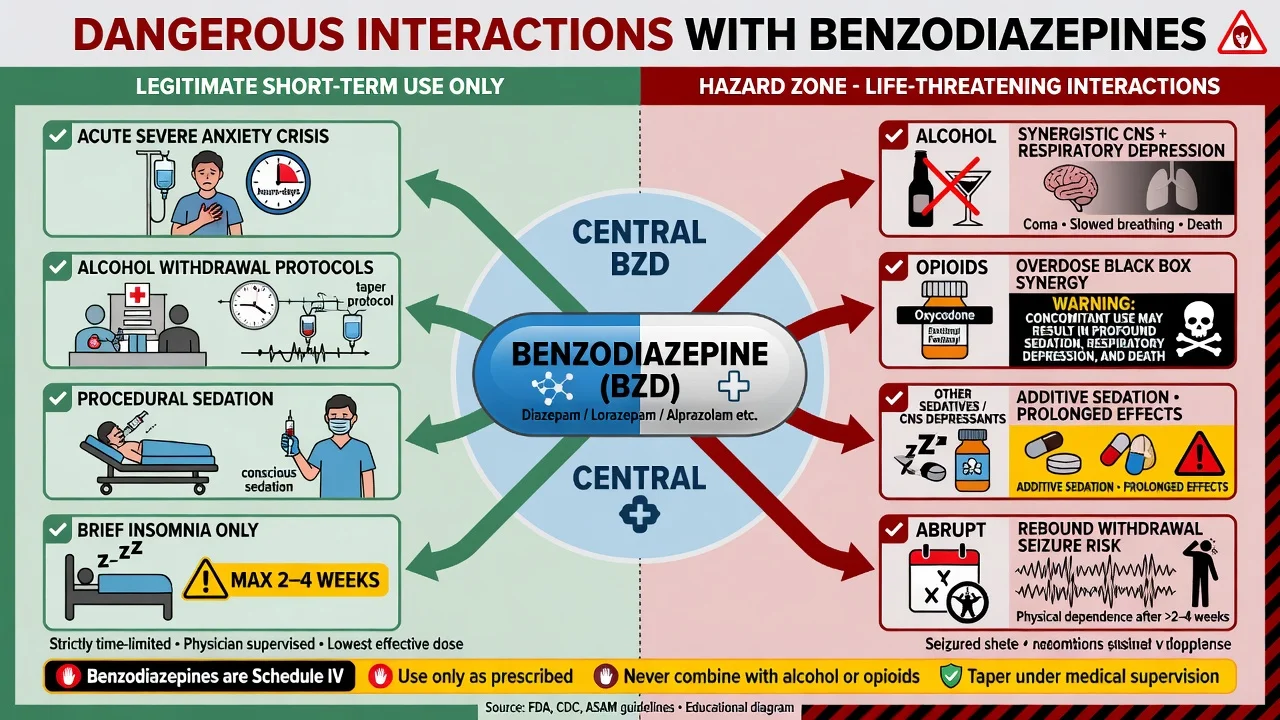
Benzodiazepines remain among the most widely prescribed psychotropics and among the most examined substances in addiction and consultation-liaison viva. Fellowship candidates must hold two truths at once: short-term, indication-limited use can be legitimate and life-saving (severe acute anxiety, alcohol withdrawal protocols, procedural sedation), and chronic unsupervised use drives falls, cognitive harm, dependence, and overdose synergy with other depressants.[1][8][16]
Overview and definition
Physiological dependence means tolerance and/or a characteristic withdrawal syndrome after dose reduction or cessation. It can develop even when the original prescription was appropriate. Sedative, hypnotic, or anxiolytic use disorder (DSM-5-TR language) adds the behavioural syndrome of impaired control, social impairment, risky use, and pharmacological criteria — severity by criterion count. ICD-11 frames disorders due to use of sedatives, hypnotics, or anxiolytics along a similar harmful-use to dependence spectrum. Examiners mark candidates who conflate “any long-term script” with “use disorder” without assessing control and harm, and those who dismiss iatrogenic dependence because the patient is “not a recreational user.”[1][3][16]
Therapeutic (prescribed) long-term use, high-dose misuse, and illicit alprazolam markets are different clinical phenotypes that share receptor biology but differ in risk of diversion, trauma, and dual diagnosis.[2][15]
Classification
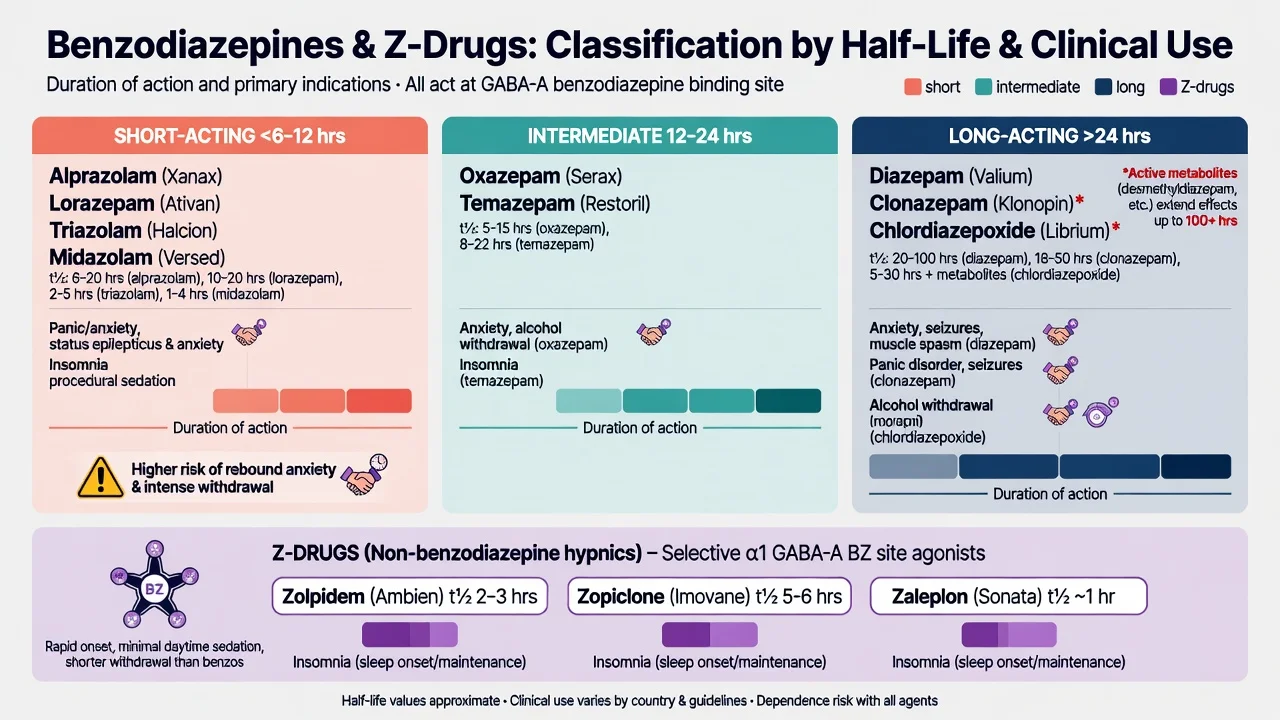
Short / high-potency
- Alprazolam, lorazepam, midazolam, triazolam
- Earlier rebound and often more intense withdrawal
- Alprazolam frequently appears in misuse stems
Long-acting / active metabolites
- Diazepam, chlordiazepoxide, clonazepam (long)
- Useful for substitution taper flexibility
- Delayed withdrawal peak possible
Z-drugs
- Zolpidem, zopiclone/eszopiclone, zaleplon
- Not non-addictive safe sleeping pills
- Dependence, complex sleep behaviours, elderly harm
Hepatic teaching point: agents relying heavily on oxidative metabolism accumulate in liver disease and older adults; lorazepam and oxazepam (glucuronidation pathway teaching) are often preferred when a benzodiazepine is still required in hepatic impairment — still not a licence for chronic insomnia scripts.[2]
Epidemiology and risk factors
Long-term community use clusters in middle-aged and older adults, chronic insomnia and anxiety pathways, and polypharmacy. Women are over-represented in many primary-care cohorts. Prior substance use disorder, high starting dose, longer duration, and short-acting high-potency agents increase dependence and withdrawal severity risk.[1][8][9]
Harms extend beyond “addiction labels”: falls and fractures, cognitive slowing, road traffic risk, paradoxical agitation in some patients, and fatal overdose — especially when combined with opioids or alcohol. Dementia-association signals exist in observational data and must be discussed with confounding caveats rather than as proven pure causation.[9][10][11][17]
High-yield risk anchors
Pathophysiology
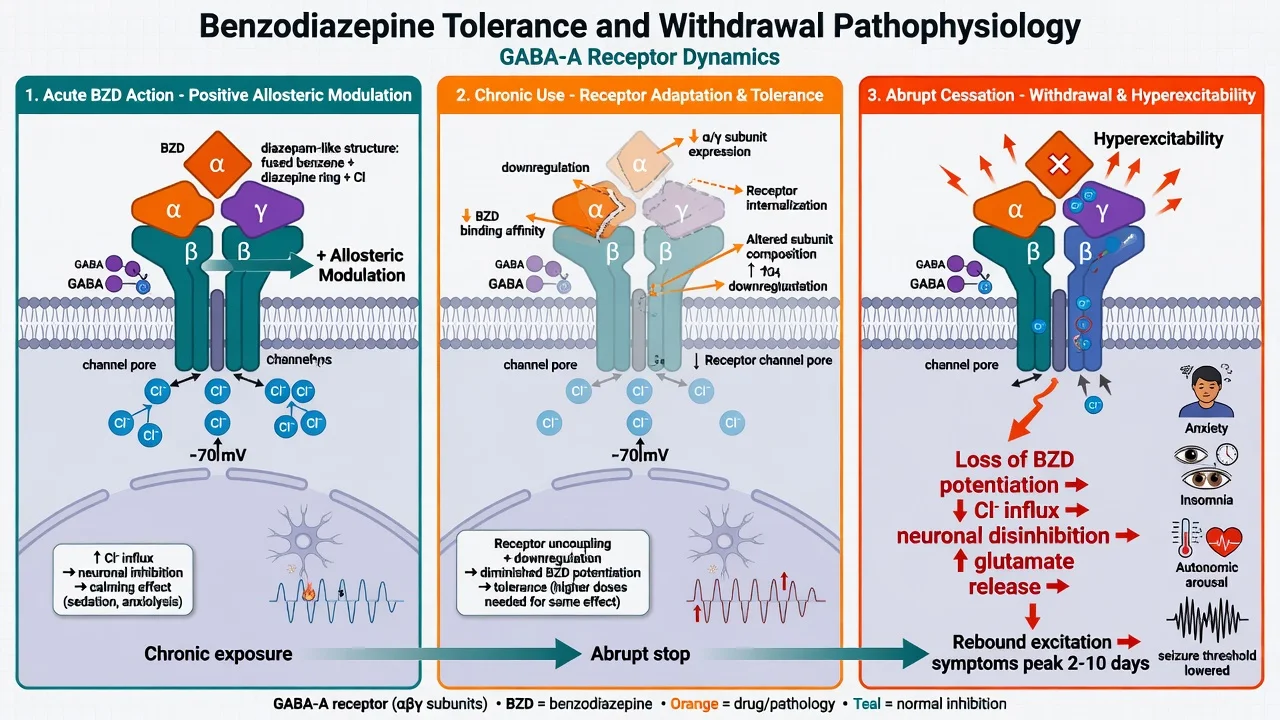
Benzodiazepines are positive allosteric modulators of GABA-A receptors: they increase the effect of GABA without opening the channel alone at usual concentrations. Teaching models map α1-containing receptors more to sedation and amnesia, and α2/α3 more to anxiolysis — useful for viva, not for ordering a “subunit blood test.”[1][16]
Tolerance reflects receptor uncoupling, subunit expression shifts, and reduced allosteric efficacy. Sedative and hypnotic effects often attenuate faster than anxiolysis, which is why patients escalate night doses for sleep while still reporting daytime anxiety.[1][3][15]
Withdrawal is rebound CNS hyperexcitability: anxiety, insomnia, irritability, tremor, sweating, tachycardia, nausea, perceptual disturbance (hyperacusis, photophobia, depersonalisation), and in severe cases seizures and delirium. Cross-tolerance with alcohol and other GABA-A agents explains both alcohol-withdrawal treatment protocols and the danger of stacking depressants.[1][3][18]
Clinical presentation
Intoxication: sedation, dysarthria, ataxia, nystagmus, impaired judgement, anterograde amnesia; respiratory depression mainly when combined with other depressants or in extreme dose.[1][16]
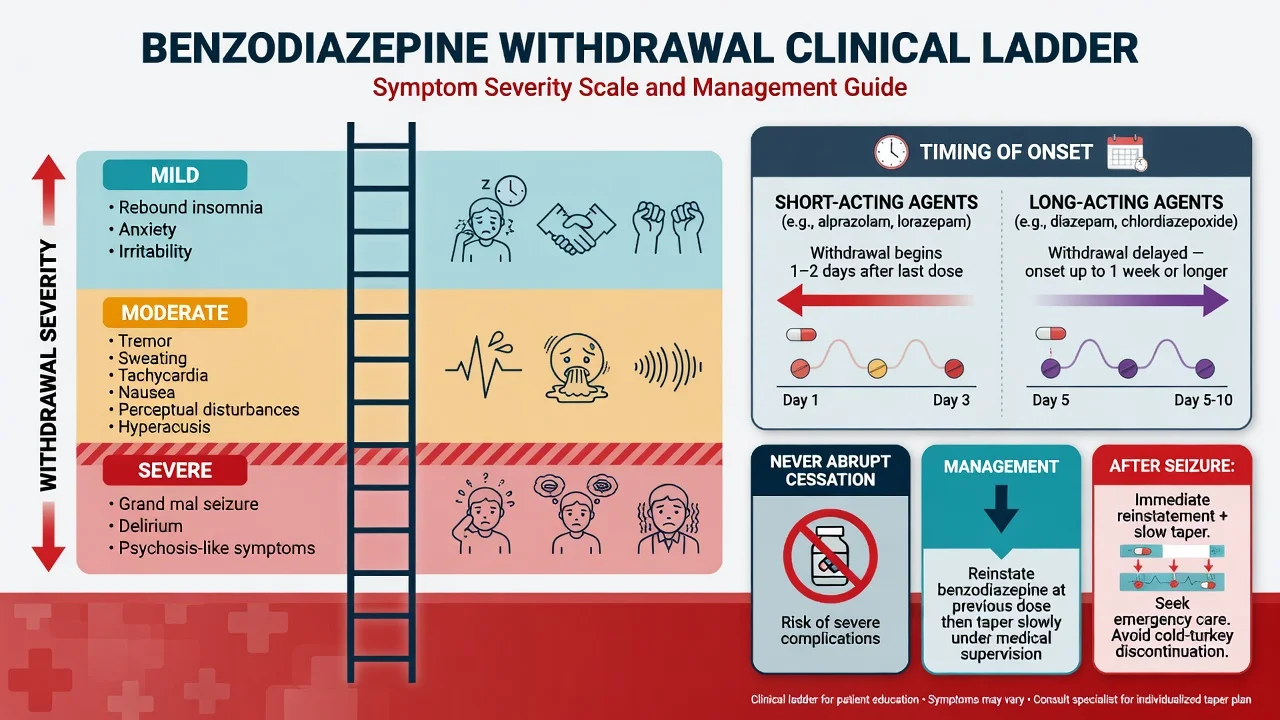
Acute withdrawal ladder:
- Mild — rebound insomnia, anxiety, irritability
- Moderate — tremor, diaphoresis, tachycardia, nausea, sensory hyperacusis, perceptual change
- Severe — generalised tonic-clonic seizures, delirium, psychosis-like states
Onset tempo tracks pharmacokinetics: short-acting agents often within 1–2 days; long-acting agents may peak later in the first week or beyond. Protracted withdrawal (weeks to months of fluctuating anxiety, insomnia, sensory symptoms) is real in some patients and must be distinguished from relapse of primary anxiety disorder and from secondary gain narratives that examiners dislike when they replace a careful differential.[3][7][15][18]
Use-disorder MSE content: craving, unsuccessful cut-downs, time spent obtaining, continued use despite falls or relationship harm, tolerance, withdrawal relief dosing.[1][2]
Differential diagnosis
| Mimic | Favours BZD withdrawal / dependence | Favours alternative |
|---|---|---|
| Primary panic / GAD relapse | Tempo tightly linked to dose cut or missed doses; autonomic plus sensory hyperacusis | Anxiety independent of stable dose for months |
| Alcohol withdrawal | BZD history clear; isolated BZD cessation | Heavy alcohol, CIWA trajectory, liver stigma clues |
| Serotonin toxicity / NMS | BZD context, no serotonergic rigidity package | Clonus/hyperthermia pattern or antipsychotic rigidity |
| Thyrotoxicosis / hypoglycaemia | Normal metabolic work-up | Abnormal glucose/TFT, different systemic signs |
| Primary seizure disorder | First seizure after abrupt BZD stop | Prior epilepsy, focal onset, structural lesion |
| Dementia / delirium (elderly) | Recent BZD start/stop or accumulation | Infection, stroke, other drugs |
Clinical and bedside assessment
History that scores marks: exact agent(s), prescribed versus actual dose, duration, source (single GP, multiple, online, illicit), prior withdrawal seizures, alcohol and opioid co-use, gabapentinoids, driving, occupation safety-critical work, pregnancy possibility, suicide risk, and what problem the tablet is “solving” tonight (sleep, panic, grief, pain).[2][1][14]
Examination: vitals, tremor, gait/ataxia, nystagmus, consciousness, injuries from falls or seizures, signs of alcohol use disorder, injection marks if polysubstance.[2]
Risk and capacity: withdrawal delirium abolishes capacity for complex decisions; document emergency treatment rationale. Assess suicide and accidental overdose risk when stockpiles exist. Driving advice during intoxication, early taper, and after seizures is mandatory counselling content.[2][8]
Investigations
- Clinical diagnosis first — immunoassay urine drug screens miss many benzodiazepines and cannot quantify dependence; use as adjunct, not gatekeeper.[2]
- Baseline FBC, U&E, LFT, glucose; ECG if polypharmacy, syncope, or overdose.[2]
- CT head if first seizure with trauma, focal neurology, or prolonged post-ictal state.[1]
- Cognitive screen in older adults as baseline for deprescribing conversations.[9][12]
- Pregnancy test when relevant.[2]
Routine serum benzodiazepine levels are not a community taper tool.[2]
Management — resuscitation and emergencies
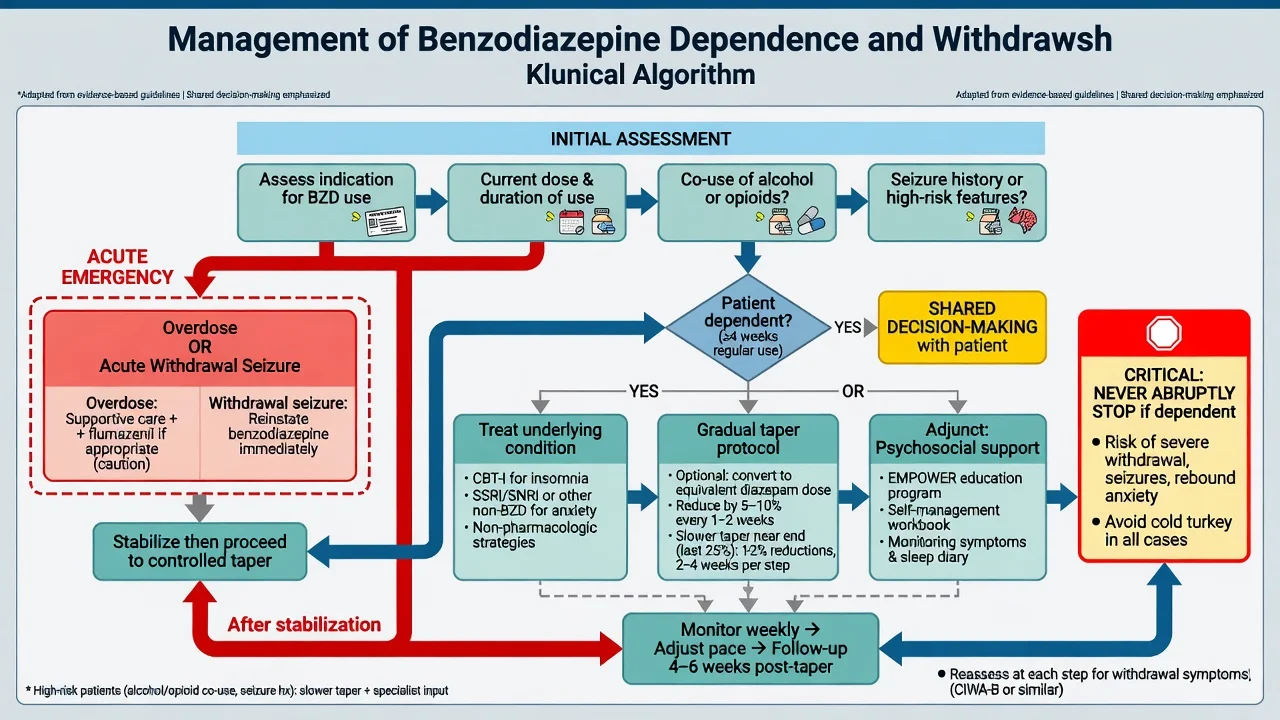
- Overdose: ABC support, airway protection, oxygen, monitoring; co-ingestant work-up. Flumazenil is a competitive antagonist that can precipitate seizures in chronic users, mixed overdoses, or epileptogenic co-ingestants — reserve for highly selected settings with seizure preparedness, not as a default “naloxone equivalent.”[1][2][15]
- Withdrawal seizure: terminate seizure per emergency protocol, protect airway, then reinstate benzodiazepine cover and plan a controlled taper — “cold turkey after a fit” fails exams and patients.[1][3][14]
- Delirium tremens-spectrum BZD withdrawal: medical ward or HDU capability, exclude other causes, reinstate long-acting agent, supportive care.[1][15]
- Alcohol plus BZD withdrawal: higher acuity; protocolised medical management; do not under-dose fearfully into seizures.[2]
Management — definitive and stepwise
Step 1 — Revisit the indication
If the original problem was insomnia or anxiety, first-line long-term answers are usually CBT-I / CBT for anxiety, sleep scheduling, and where indicated SSRI/SNRI or other non-benzodiazepine pharmacotherapy — not indefinite hypnotic scripts.[7][12][16]
Step 2 — Negotiate a taper (core skill)
Structured approaches improve cessation versus minimal intervention. Meta-analysis supports supervised discontinuation strategies; psychosocial interventions help harmful use pathways; pharmacological adjuncts for discontinuation have mixed, limited evidence and are not magic bullets.[4][5][6]
Principles (Brett and Murnion; Ashton-informed clinical tradition; modern tapering CPG):
- Agree goals, pace, and crisis plan in writing where possible
- Prefer one long-acting agent (commonly diazepam) when multiple short-acting agents or awkward tablet strengths impede smooth reductions
- Reduce gradually — common outpatient teaching bands are about 5–10% of the daily dose every 1–2 weeks, slower at low doses, individualised to withdrawal severity
- Hold or step back if severe withdrawal, major life stress, or destabilising mental illness
- Inpatient faster tapers only with observation and when risk demands (high dose, seizures, unstable social context)[2][3][14][1]
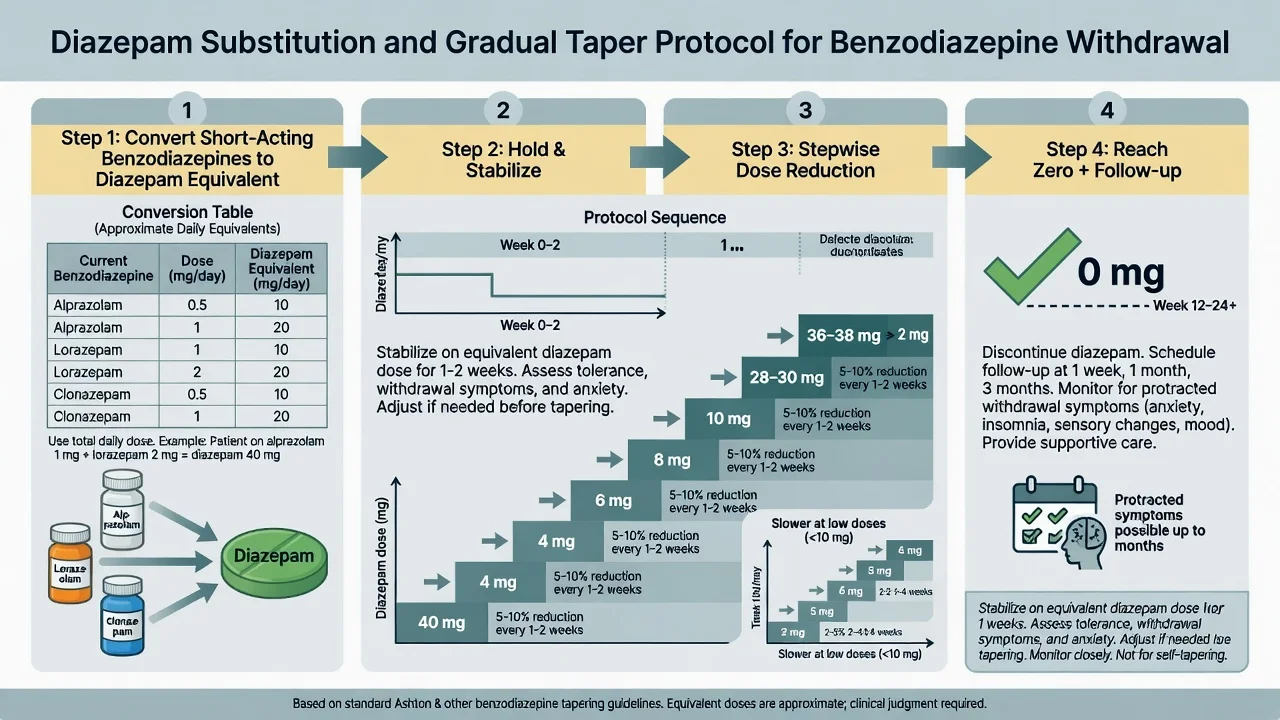
Approximate diazepam equivalences (order-of-magnitude teaching aids — always check a current local conversion table and clinical response; do not treat as rigid laws):
- Diazepam 5 mg ≈ alprazolam 0.25–0.5 mg ≈ lorazepam 0.5–1 mg ≈ clonazepam 0.25–0.5 mg ≈ oxazepam 15 mg ≈ temazepam 10 mg (ranges vary by source)
Stabilise on the equivalent, then reduce. Ashton’s clinical narrative remains historically important for describing protracted symptoms and slow flexible tapering; modern practice integrates shared decision-making and deprescribing evidence rather than a single rigid manual for every patient.[2][3][18][14]
Step 3 — Adjuncts and psychosocial care
- EMPOWER-style patient education about risks and taper options increases cessation in older adults in cluster RCT evidence.[13]
- Canadian deprescribing BRZA guideline supports structured deprescribing conversations for benzodiazepine receptor agonists.[12]
- 2025 joint clinical practice guideline on benzodiazepine tapering emphasises when risks outweigh benefits and how to taper safely — use as contemporary multi-society framing alongside local policy.[14]
- Motivational interviewing, CBT elements, supervised dispensing, and prescription-monitoring review when diversion is suspected.[5][2]
- Adjunctive medicines (carbamazepine, antidepressants, melatonin, etc.) may be considered case-by-case; Cochrane-level evidence does not crown a universal pharmacological fix for discontinuation.[6][15]
Step 4 — Monitoring
Track withdrawal symptoms, mood and suicidality, alcohol/opioid substitution, sleep, falls, and driving. After the last dose, plan follow-up for protracted symptoms and primary disorder care so the patient does not drift back to the first GP who will re-prescribe under pressure.[7][2][14]
Specific subtypes and scenarios
Iatrogenic primary-care insomnia scripts. Deprescribe with education + CBT-I pathway; EMPOWER logic.[13][12]
High-dose alprazolam misuse. Expect difficult withdrawal, diversion, and dual diagnosis; consider inpatient stabilisation and diazepam conversion.[2][15]
Z-drug nightly dependence. Same receptor-family story; taper and sleep therapy — do not switch forever from temazepam to zolpidem as a “solution.”[12][16]
Opioid–BZD co-prescribing. Overdose synergy is a public-health red flag; prioritise risk reduction and deprescribing one or both under specialist advice.[8][16]
Inherited inpatient chronic BZD. Do not strip cover on day one of admission without a plan; convert and taper collaboratively with the community prescriber.[2][14]
Complications and pitfalls
- Abrupt cessation → seizure/delirium
- Flumazenil as routine reversal → seizure
- Too-fast taper → dropout and illicit sourcing
- Moralising “weak will” without offering CBT-I / anxiety treatment
- Missing alcohol co-dependence
- Blaming age alone for falls while continuing night Z-drugs
- Re-labelling protracted withdrawal as “personality” without assessment
Prognosis and disposition
Many patients achieve long-term cessation with structured support; predictors include motivation, lower dose, psychosocial stability, and effective treatment of the original symptom driver. Relapse is common if insomnia and anxiety are untreated. Outpatient taper suits stable, lower-dose, good-support cases. Inpatient or residential pathways suit high dose, prior seizures, unstable housing, severe dual diagnosis, or failed community attempts.[4][1][2]
Special populations
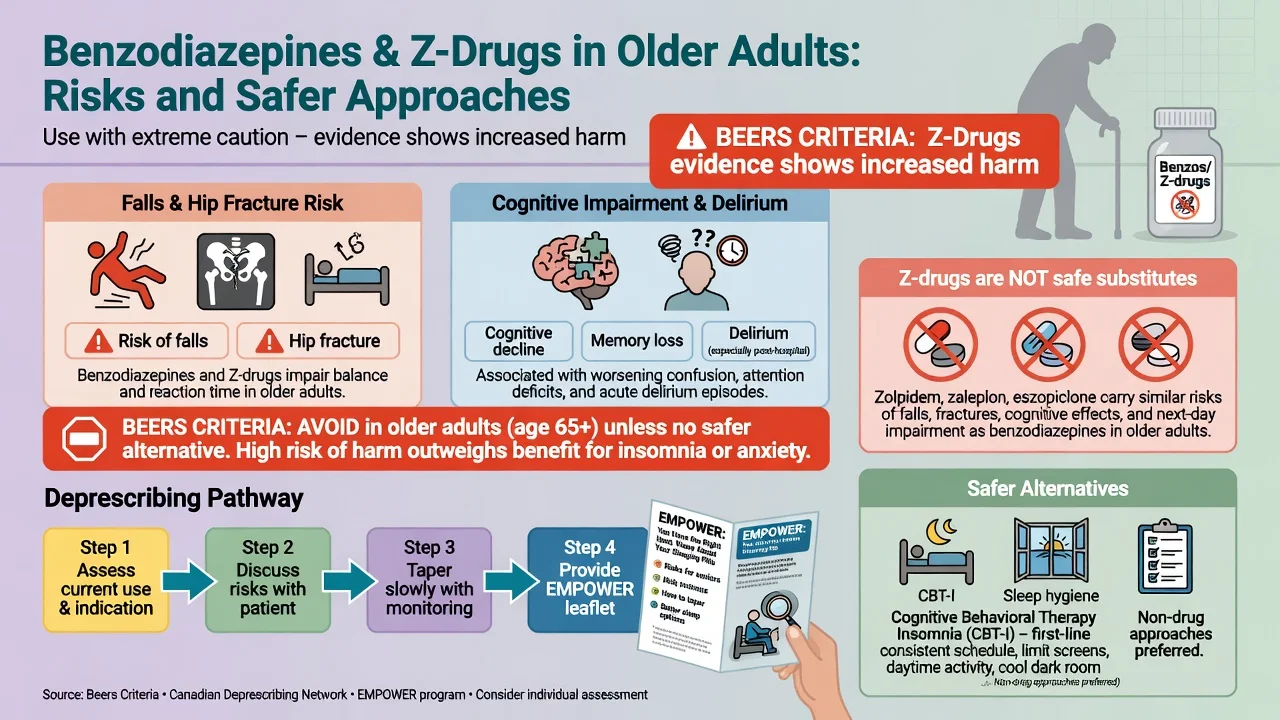
Older adults. Prefer avoidance (Beers-type guidance logic). Glass meta-analysis: sedative-hypnotics yield small sleep gains with meaningful cognitive and adverse-event harm. Markota review: dangers, management, alternatives. Cognitive effects of long-term use are supported in meta-analysis. Dementia association data (Billioti de Gage) should be taught with residual confounding awareness.[9][10][11][17][12]
Pregnancy and lactation. Prefer non-drug strategies; neonatal adaptation/withdrawal and floppy-infant-type concerns exist with late exposure; decisions are specialist and individualised — do not invent fixed teratogen absolute rules beyond evidence.[2]
Youth. Diversion and learning impact; avoid chronic anxiolytic scripts.[8]
Hepatic impairment. Prefer lorazepam/oxazepam when a BZD is unavoidable; still time-limit.[2]
Evidence, guidelines, and regional differences
| Source | Exam take-home |
|---|---|
| Soyka NEJM 2017 | Comprehensive treatment framework |
| Brett and Murnion Aust Prescr 2015 | Practical ANZ management and taper principles |
| Voshaar 2006 meta-analysis | Structured discontinuation strategies work |
| Darker Cochrane 2015 | Psychosocial interventions for harmful use |
| Baandrup Cochrane 2018 | Pharmacological adjuncts for discontinuation — limited |
| Pottie et al. 2018 Canadian BRZA deprescribing | Primary-care deprescribing standard |
| EMPOWER RCT 2014 | Direct patient education reduces inappropriate use |
| Joint tapering CPG 2025 | Contemporary multi-stakeholder taper guidance |
| Ashton 1984/2005 | Clinical phenomenology of withdrawal; slow flexible taper tradition |
ANZ: Australian Prescriber guidance (Brett and Murnion) is high-yield for FRANZCP; use local real-time prescription monitoring programs where available; mental health acts and controlled-drug rules are jurisdiction-specific — state principles, do not invent section numbers. UK: NICE-aligned substance-misuse and medicines-optimisation pathways emphasise limited duration for anxiety/insomnia benzodiazepines and structured withdrawal support; MRCPsych expects half-life and seizure risk fluency. US: ABPN-style items stress Beers criteria logic in elderly, opioid–BZD black-box synergy, and deprescribing; 2025 joint tapering CPG is contemporary multi-society language.[2][14][9]
Legal frameworks for involuntary treatment of withdrawal delirium or comorbid risk are jurisdiction-specific — describe capacity, duty of care, and local mental health legislation principles without fabricating statutes.[2][14]
Exam pearls
- Short half-life + high potency (alprazolam stems) = harder withdrawal and misuse signal
- Withdrawal seizure → reinstate, then taper — not moral lectures alone
- Z-drugs share GABA-A BZ-site dependence potential
- Alcohol + BZD = synergistic respiratory depression
- Flumazenil ≠ naloxone for street use-disorder care
- EMPOWER education is a named trial examiners like
- Convert to diazepam when tablet maths blocks a smooth outpatient taper
- Treat the insomnia/anxiety disorder or the taper fails
TAPER-BZD
References
- [1]Soyka M. Treatment of Benzodiazepine Dependence N Engl J Med, 2017.PMID 28614686
- [2]Brett J, Murnion B. Management of benzodiazepine misuse and dependence Aust Prescr, 2015.PMID 26648651
- [3]Ashton H. The diagnosis and management of benzodiazepine dependence Curr Opin Psychiatry, 2005.PMID 16639148
- [4]Voshaar RC, Couvée JE, van Balkom AJ, et al. Strategies for discontinuing long-term benzodiazepine use: meta-analysis Br J Psychiatry, 2006.PMID 16946355
- [5]Darker CD, Sweeney BP, Barry JM, et al. Psychosocial interventions for benzodiazepine harmful use, abuse or dependence Cochrane Database Syst Rev, 2015.PMID 26106751
- [6]Baandrup L, Ebdrup BH, Rasmussen JØ, et al. Pharmacological interventions for benzodiazepine discontinuation in chronic benzodiazepine users Cochrane Database Syst Rev, 2018.PMID 29543325
- [7]Lader M, Kyriacou A. Withdrawing Benzodiazepines in Patients With Anxiety Disorders Curr Psychiatry Rep, 2016.PMID 26733324
- [8]Lader M. Benzodiazepine harm: how can it be reduced? Br J Clin Pharmacol, 2014.PMID 22882333
- [9]Markota M, Rummans TA, Bostwick JM, et al. Benzodiazepine Use in Older Adults: Dangers, Management, and Alternative Therapies Mayo Clin Proc, 2016.PMID 27814838
- [10]Glass J, Lanctôt KL, Herrmann N, et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits BMJ, 2005.PMID 16284208
- [11]Barker MJ, Greenwood KM, Jackson M, et al. Cognitive effects of long-term benzodiazepine use: a meta-analysis CNS Drugs, 2004.PMID 14731058
- [12]Pottie K, Thompson W, Davies S, et al. Deprescribing benzodiazepine receptor agonists: Evidence-based clinical practice guideline Can Fam Physician, 2018.PMID 29760253
- [13]Tannenbaum C, Martin P, Tamblyn R, et al. Reduction of inappropriate benzodiazepine prescriptions among older adults through direct patient education: the EMPOWER cluster randomized trial JAMA Intern Med, 2014.PMID 24733354
- [14]Brunner E, Chen CA, Klein T, et al. Joint Clinical Practice Guideline on Benzodiazepine Tapering: Considerations When Risks Outweigh Benefits J Gen Intern Med, 2025.PMID 40526204
- [15]Fluyau D, Revadigar N, Manobianco BE. Challenges of the pharmacological management of benzodiazepine withdrawal, dependence, and discontinuation Ther Adv Psychopharmacol, 2018.PMID 29713452
- [16]Guina J, Merrill B. Benzodiazepines I: Upping the Care on Downers: The Evidence of Risks, Benefits and Alternatives J Clin Med, 2018.PMID 29385731
- [17]Billioti de Gage S, Bégaud B, Bazin F, et al. Benzodiazepine use and risk of dementia: prospective population based study BMJ, 2012.PMID 23045258
- [18]Ashton H. Benzodiazepine withdrawal: an unfinished story Br Med J (Clin Res Ed), 1984.PMID 6143582