Psych · Addiction psychiatry — cannabis and psychosis
Cannabis use and psychosis
Also known as Cannabis-induced psychosis · Marijuana psychosis · THC psychosis · Skunk and psychosis · High-potency cannabis · Cannabis use disorder and psychosis · Substance-induced psychotic disorder cannabis · Dual diagnosis cannabis · Cannabis FEP
Exam-exhaustive fellowship reference on the cannabis–psychosis interface: THC potency and dose–response, adolescent risk, substance-induced versus primary psychosis, conversion after SIP, CUD treatment, early intervention dual care, dual formulation, CBD evidence and regional guideline framing. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Cannabis is the most examinable substance–psychosis interface in fellowship psychiatry. The viva is not "is cannabis bad?" — it is whether you can quantify potency and frequency, distinguish intoxication, substance-induced psychotic disorder (SIP), and primary psychosis with comorbidity, run a dual formulation, integrate CUD treatment with early intervention, and counsel without moralising while holding risk. This topic is the cannabis–psychosis monograph; full FEP pathway depth lives in the related early-psychosis topic.[4][19][20]
Overview and definition
Cannabis products deliver variable delta-9-tetrahydrocannabinol (THC) (partial CB1 agonist; psychotomimetic) and cannabidiol (CBD) (often framed as relatively non-psychotomimetic, sometimes counterbalancing in research settings). "High-potency" or "skunk-type" products are high-THC, often low-CBD. Street names change; potency, frequency, age of onset, and last use are the clinical variables that matter.[6][13]
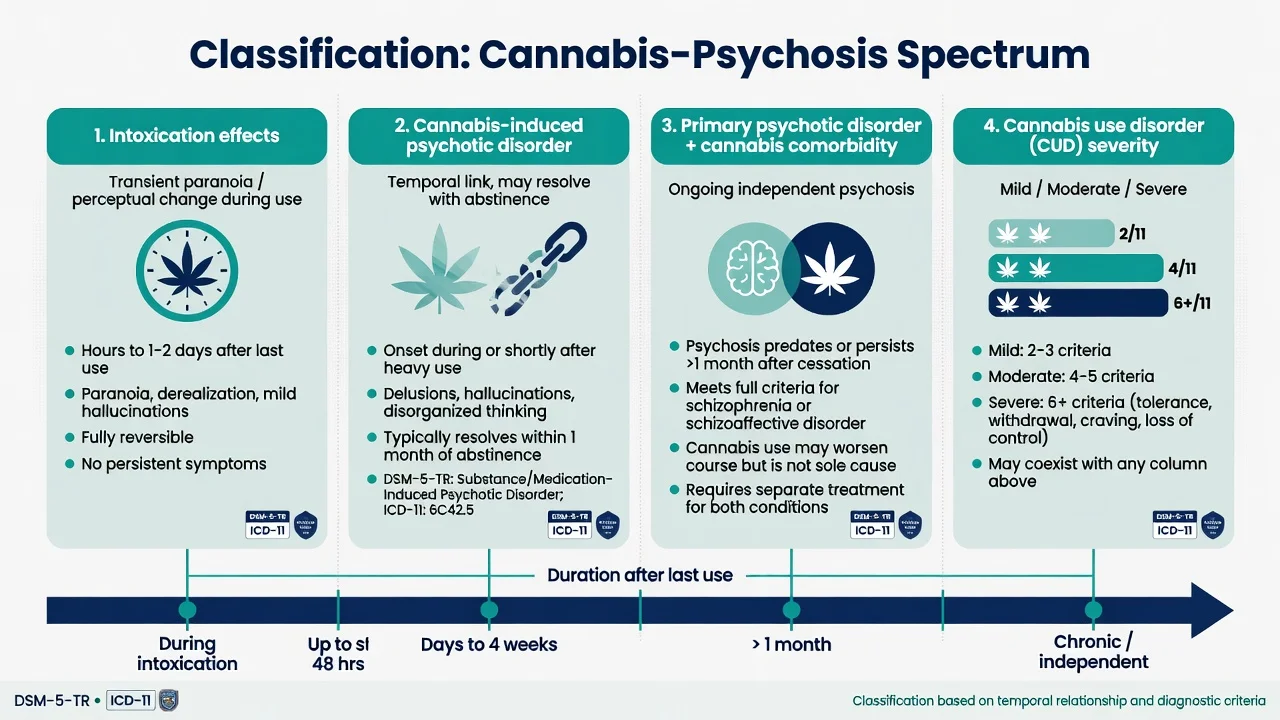
Three clinical layers examiners expect you to name separately: intoxication effects, cannabis-induced psychotic disorder, and primary psychotic disorder with cannabis comorbidity.[4][19]
- Intoxication effects — paranoia, perceptual distortion, anxiety, tachycardia during use; usually time-limited.[13]
- Cannabis-induced (substance/medication-induced) psychotic disorder — delusions or hallucinations with temporal link to intoxication or withdrawal, not better explained by a primary psychotic disorder, not exclusively during delirium.[4][19]
- Primary psychotic disorder with cannabis comorbidity — schizophrenia-spectrum or affective psychosis that continues independently; cannabis may have precipitated, advanced onset, or worsened course.[4][19]
Cannabis use disorder (CUD) is diagnosed by DSM-5-TR criteria (control, craving, use despite harm, tolerance, withdrawal, social/role impact, hazardous use, etc.). Severity is by criterion count (commonly taught as mild 2–3, moderate 4–5, severe 6+). CUD can exist with or without psychosis; psychosis can exist with use below CUD threshold — assess both axes every time.[14][15]
Classification
Intoxication
- During/shortly after use
- Insight often partial but recovers
- Supportive care usually enough
- Still assess risk and other substances
Cannabis-induced psychotic disorder
- Temporal link to intoxication/withdrawal
- Prominent delusions/hallucinations
- May need antipsychotic short-term
- High conversion risk — follow-up mandatory
Primary psychosis + cannabis
- Psychosis independent of recent use window
- Premorbid decline, family history common
- EIS/FEP multi-element care
- CUD treatment is secondary prevention
CUD (any severity)
- Criteria-based dependence pattern
- Withdrawal is real and treatable
- MI/CBT/CM psychosocial package
- Not cured by an antipsychotic alone
DSM-5-TR vs ICD-11. Both allow substance-induced psychotic disorder when psychosis is judged secondary to the substance with a temporal relationship. ICD-11 cannabis-induced psychotic disorder sits in the substance-induced mental disorders chapter. State which manual you are using in multi-board answers. Neither manual lets a single positive urine test replace longitudinal formulation.[19]
Epidemiology and risk factors
Headline numbers examiners expect
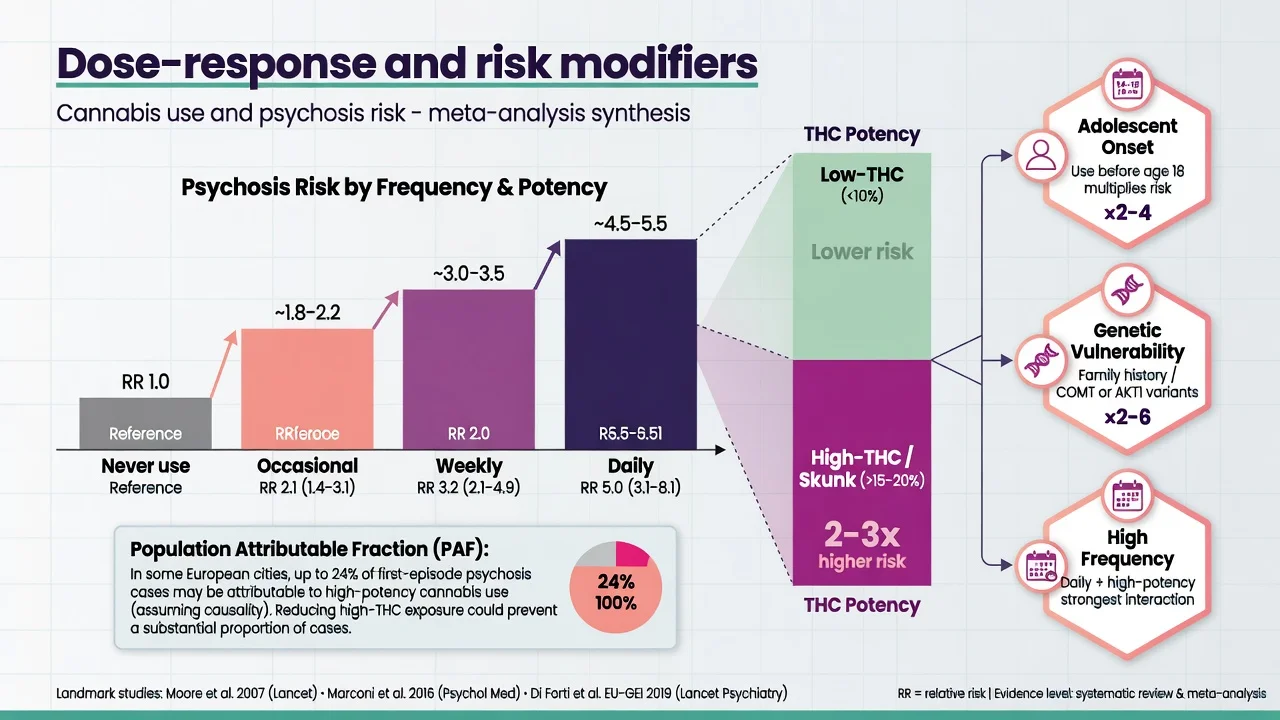
Andréasson longitudinal Swedish conscript data linked cannabis use, especially heavier use, with later schizophrenia diagnosis — the classic epidemiology stem still cited in fellowship teaching.[1] Moore and colleagues synthesised observational evidence showing increased risk of psychotic outcomes with cannabis use and a dose relationship in the literature of that era.[2] Marconi meta-analysis quantified association between level of cannabis use and psychosis risk — "ever tried once" is not the same as daily high-THC use.[5]
Potency matters. Di Forti and colleagues estimated a substantial population attributable fraction of first-episode psychosis in south London linked to high-potency cannabis patterns, and EU-GEI linked daily and high-potency use to variation in psychotic disorder incidence across Europe.[6][7] Petrilli systematic review associates higher potency with greater mental ill-health and addiction risk signals.[13]
Adolescent window. Dunedin-linked work (Arseneault) associated adolescent cannabis use with later psychotic outcomes, with stronger signals for earlier use; the broader causal-evidence review remains a viva staple.[3][4] Large meta-analysis associates cannabis use with earlier age at onset of psychosis — clinically: young heavy users present earlier into services.[11] Myles meta-analysis documents high rates of cannabis use and CUD patterns around FEP, with initiation often preceding frank psychosis.[12]
Causality debate (examinable honesty). Confounding (shared genetics, trauma, urbanicity), reverse causation (prodromal self-medication), and residual bias exist. Mendelian randomisation work (Vaucher) supports a causal pathway from cannabis liability toward schizophrenia risk in genetic instrumental designs — use it as evidence synthesis, not as proof that every user will become psychotic.[18][19]
Pathophysiology
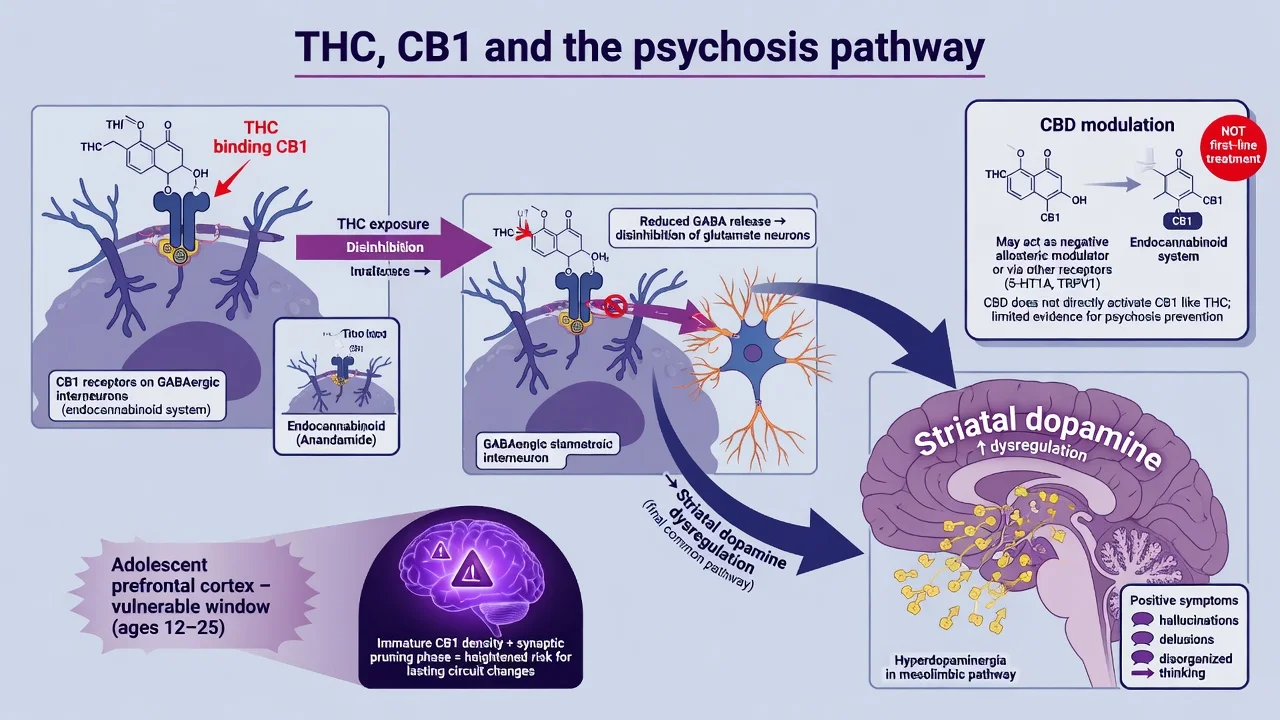
THC acts as a partial agonist at CB1 receptors, densely expressed on GABAergic interneurons and other circuits that gate cortical and midbrain signalling. Net effects include altered inhibitory control and downstream influence on striatal dopamine dynamics — the same final common pathway targeted by antipsychotic D2 blockade (dopamine hypothesis version III framing for positive symptoms).[19] Adolescent prefrontal maturation is incomplete; early heavy THC exposure hits a plastic developmental window, aligning epidemiology with mechanism teaching without overclaiming a single gene test.[3][11]
THC vs CBD. High-THC low-CBD products dominate modern risk discussions. CBD as adjunctive therapy in schizophrenia showed symptom benefit versus placebo in a multicentre RCT (McGuire) — research/specialist context, not a licence to market over-the-counter CBD as CUD or psychosis cure, and not a substitute for antipsychotics when they are indicated.[17][13]
Clinical presentation
Intoxication. Anxiety, suspiciousness, depersonalisation, time distortion, mild perceptual changes, conjunctival injection, tachycardia, dry mouth, impaired attention. Severe intoxication can look like an acute behavioural emergency.[13]
Cannabis-associated psychosis. Persecutory or referential delusions, auditory hallucinations, thought disorder, fear, sleep collapse. Mood can be elevated, irritable or depressed. Synthetic cannabinoids may produce more extreme agitation and medical instability.[19]
Primary psychosis unmasked by cannabis. Psychosis continues or re-emerges without ongoing use; premorbid decline, negative symptoms, and family history raise the primary-illness probability — but course after abstinence is the decider, not a single MSE snapshot.[9][10]
Atypical stems. Edibles with delayed onset and accidental high dose; "medical cannabis" patient with new paranoia; late-onset first use in older adults (intensify organic work-up); perinatal presentations; adolescent "just weed" minimisation with daily skunk use on collateral.[13]
Differential diagnosis
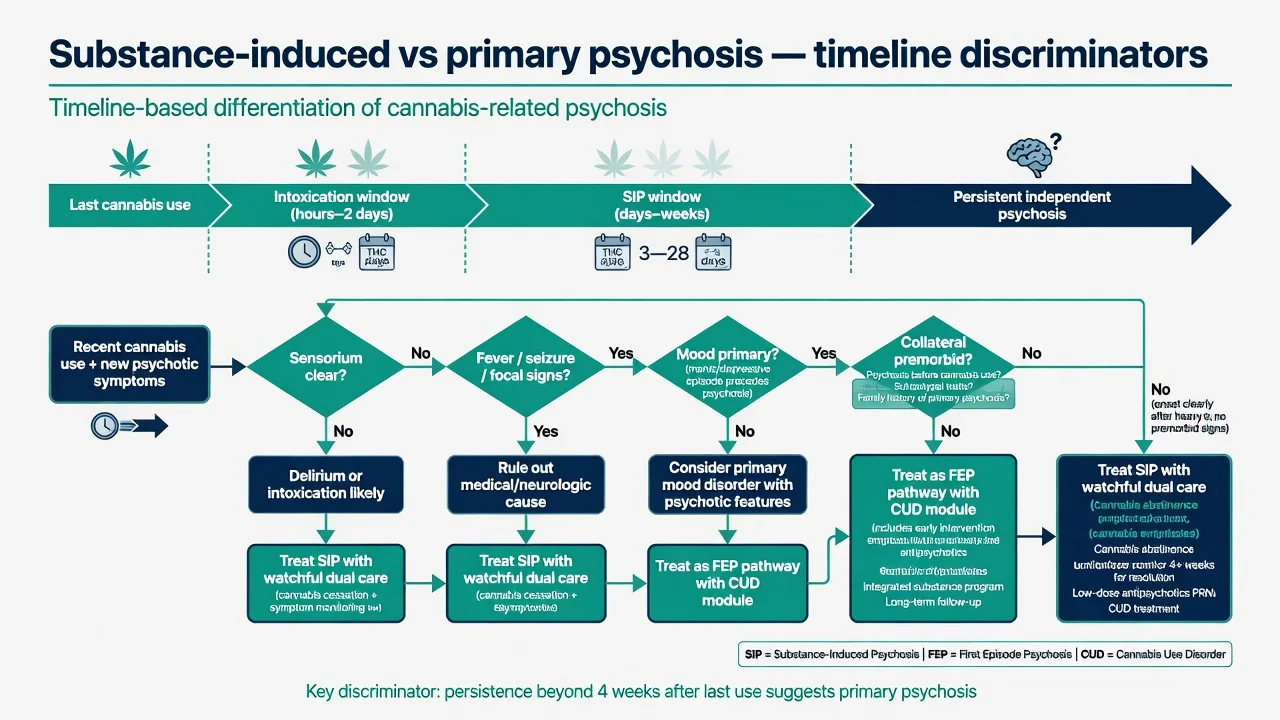
Win the differential on timeline after last use, attention/sensorium, medical signs, mood chronology, and premorbid trajectory — not on urine colour.[19]
Delirium
- Inattention and fluctuation core
- Medical driver or polypharmacy
- Visual hallucinations more common
- Treat cause first
Stimulant psychosis
- Methamphetamine, cocaine
- Often severe paranoia, formication
- Other substance timeline
- UDS panel broader than cannabis alone
Primary schizophrenia spectrum
- Persistence beyond substance window
- Negative/cognitive load
- Family history, premorbid decline
- EIS pathway
Affective psychosis
- Mood episode primary and persistent
- Psychosis often mood-congruent (not absolute)
- Treat mood and psychosis
- Cannabis may still worsen course
Also keep PTSD with dissociative phenomena, OCD with poor insight, autism-related atypical beliefs, and personality (paranoid, schizotypal, borderline) on the board. Organic can't-miss: encephalitis, seizure, intracranial mass, HIV, syphilis, B12, thyroid, steroid psychosis.[20]
Clinical and bedside assessment
Structure every assessment so a CASC examiner can mark you — safety, cannabis timeline with potency and frequency, CUD criteria, psychosis chronology, collateral, MSE, risk, motivation, capacity/legal status, and physical exam.[12][14][20]
- Safety and observations (including capillary glucose when behavioural emergency).[20]
- Cannabis timeline — age of first use, current frequency, estimated amount, potency (skunk/high-THC if known), route (smoke, vape, edible, oil), last use time, other substances, prior SIP episodes.[12][13]
- CUD criteria — control, craving, withdrawal, harm, roles, hazardous use.[14][15]
- Psychosis history — first symptom date, content with examples, duration relative to use.[4]
- Collateral — parents, partners, flatmates, GP, school; premorbid function.[20]
- MSE with quoted delusional and hallucinatory content.[20]
- Risk — suicide, self-harm, violence, vulnerability, driving, weapons, childcare, absconding.[20]
- Motivation to change (stages of change) and previous quit attempts.[14]
- Capacity for specific decisions; legal status under local Mental Health Act principles (least restrictive; do not invent foreign section numbers).[20]
- Physical examination — medical red flags force work-up intensification.[12][20]
Investigations
Urine immunoassay supports recent cannabis exposure within a detection window that varies with chronicity; it does not measure potency, does not timestamp the moment psychosis began, and a negative screen does not exclude synthetic cannabinoids or very recent oral use patterns. Blood THC levels are rarely available acutely for routine psychiatric decision-making.[13]
Before antipsychotics when treating psychosis: weight/BMI, BP, glucose or HbA1c, lipids, FBC, U&E, LFT, ECG with QTc, pregnancy test when relevant. Image/EEG/autoimmune pathway when red flags fire (late onset, fever, seizure, focal neurology, rapid cognitive decline).[20]
Management — resuscitation of the acute crisis
De-escalate; reduce stimulation; offer oral medication first. For severe agitation use local rapid tranquillisation protocols (oral preference; IM when needed for safety; monitor airway, respiration, QTc, consciousness; avoid intramuscular olanzapine plus parenteral benzodiazepine). Benzodiazepines may settle severe intoxication-related agitation when medical review supports safety. Exclude hypoglycaemia and other organic drivers. Choose community versus admission by risk, support, insight and medical need — least restrictive setting that is still safe.[20]
Do not delay indicated antipsychotic treatment solely because cannabis is present on history or UDS. Abstinence is a treatment goal, not a prerequisite for treating frank psychosis.[8][20]
Management — definitive and stepwise
Integrated dual-diagnosis care
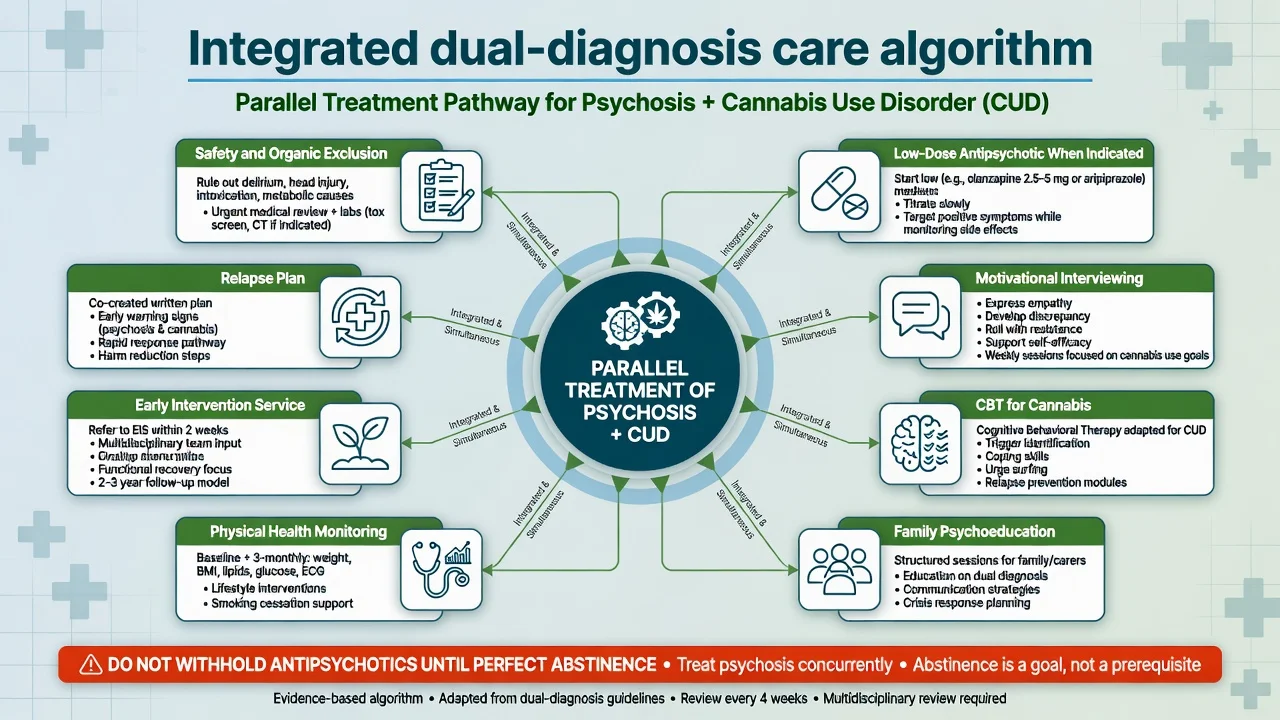
Parallel, not sequential. Treat psychotic symptoms and CUD together in one coordinated plan. Fragmented "psychosis team ignores cannabis / addiction team ignores psychosis" care is an exam fail.[8][20]
When psychosis needs medication
Use first-episode principles if this is a first presentation: start low, educate about side effects, monitor metabolically. Examples of oral starts used in FEP pathways (adjust to local formulary and product information) follow RANZCP-aligned comprehensive care principles.[20]
| Agent (oral) | Typical cautious start | Notes |
|---|---|---|
| Aripiprazole | 10 mg daily (often 5–15 mg range) | Metabolic-friendlier; watch akathisia |
| Risperidone | 1–2 mg daily; titrate carefully | Prolactin and EPS rise with dose |
| Olanzapine | 5–10 mg at night | Effective; high metabolic burden |
| [20] |
Plan an adequate trial of roughly 4–6 weeks at a therapeutic dose with adherence support. LAIs are adherence tools when oral adherence fails and psychosis is established — not a substitute for CUD work. Physical health monitoring is mandatory.[20]
Cannabis use disorder treatment
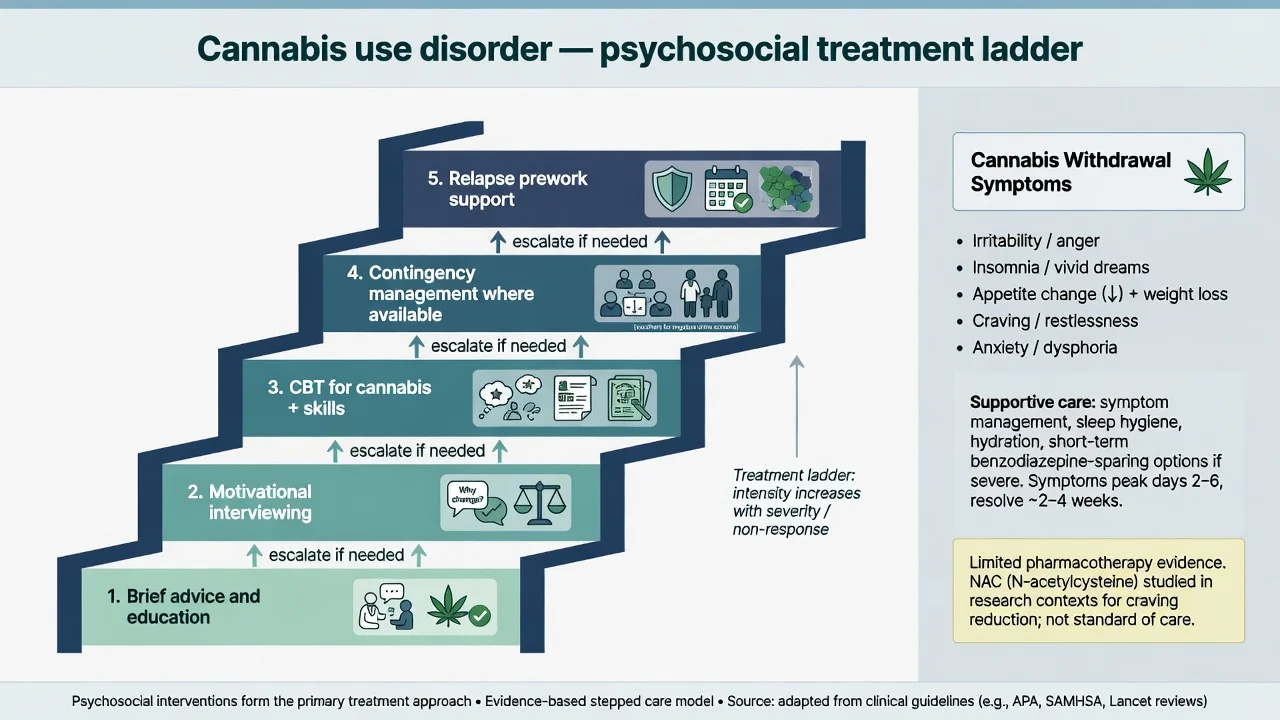
Psychosocial interventions are the core of CUD care. Cochrane review evidence supports structured psychosocial approaches (including CBT, motivational enhancement, and contingency management where available) for reducing cannabis use versus less active comparators.[14]
Practical package to name in viva draws on psychosocial intervention evidence for CUD integrated with psychosis relapse prevention.[14][8]
- Motivational interviewing / motivational enhancement [14]
- CBT for cannabis (urge surfing, high-risk situation planning, cognitive restructuring of "cannabis as medicine for my voices" beliefs when false) [14]
- Contingency management where commissioned [14]
- Family psychoeducation and reducing enabling cycles without expressed-emotion escalation [20]
- Sleep, routine, peer-network change, and vocational/education support [14]
- Integrated psychosis relapse plan linking cannabis lapses to early warning signs [8]
Cannabis withdrawal
Withdrawal is clinically real: irritability, anxiety, sleep disturbance, appetite change, restlessness, craving, depressed mood — typically peaking in the first week and lasting days to a few weeks depending on chronicity. Management is primarily supportive: sleep hygiene, short-term symptom-targeted care, psychoeducation that withdrawal is expected and not proof that "you need cannabis to be well," and close monitoring for psychosis rebound or suicide risk during the irritable phase. Review Connor and colleagues for clinical management framing.[15]
Pharmacotherapy for CUD (limited)
There is no universally licensed first-line anti-craving drug for CUD equivalent to opioid agonist therapy. N-acetylcysteine (NAC) showed benefit on cannabis use outcomes in a randomised trial of cannabis-dependent adolescents (Gray 2012); later replications and youth programmes have been mixed — present as adjunctive research-informed option under specialist protocols, not as a reflex prescription without context. Quote agent and trial context; do not invent a fixed universal dose regimen if your local protocol differs — state that dosing follows trial/local guidance and medical review.[16]
CBD in psychosis
McGuire RCT: CBD as adjunctive therapy in schizophrenia improved positive symptoms versus placebo in a multicentre trial. Exam framing: promising adjunctive research signal; not first-line monotherapy for acute psychosis; not a replacement for evidence-based antipsychotics; commercial CBD oil is not equivalent to trial product.[17]
Secondary prevention after psychosis onset
Continued cannabis use after onset associates with higher relapse risk in observational FEP cohorts; frequency and type of use matter. Cessation counselling is high-yield secondary prevention — motivational, not shaming.[8]
Specific subtypes and scenarios
Adolescent daily high-THC use with attenuated symptoms. Assess clinical high risk versus frank FEP; substance advice is mandatory; do not start antipsychotics for CHR alone without specialist rationale; protect education pathways.[3][11]
FEP with nightly skunk. Dual formulation; EIS multi-element care; low-dose antipsychotic; family work; CUD module from day one.[7][20]
Cannabis-induced psychotic disorder. Treat acute symptoms and safety; plan structured follow-up because conversion to schizophrenia or bipolar disorder after SIP is substantial in register studies — cannabis-associated SIP is not a benign one-off in population data.[9][10]
Starzer and colleagues reported high conversion rates from substance-induced psychosis to schizophrenia or bipolar disorder over follow-up, with substance type and other predictors mattering — cannabis-related SIP is among the clinically worrying groups for later primary illness.[9] Niemi-Pynttäri Finnish register data similarly showed meaningful conversion from substance-induced psychoses to schizophrenia across large inpatient cohorts.[10]
Established schizophrenia with ongoing CUD. Relapse risk, adherence collapse, metabolic double jeopardy (sedentary lifestyle + some antipsychotics). Integrated dual clinics beat revolving-door admissions without CUD plans.[8][20]
Medical cannabis / legalisation counselling. Legal status is not medical safety. High-THC products remain psychotogenic risk amplifiers; counsel frequency, potency, adolescent prohibition messaging, and personal risk (family history of psychosis).[13][7]
Dual formulation (examinable skill)
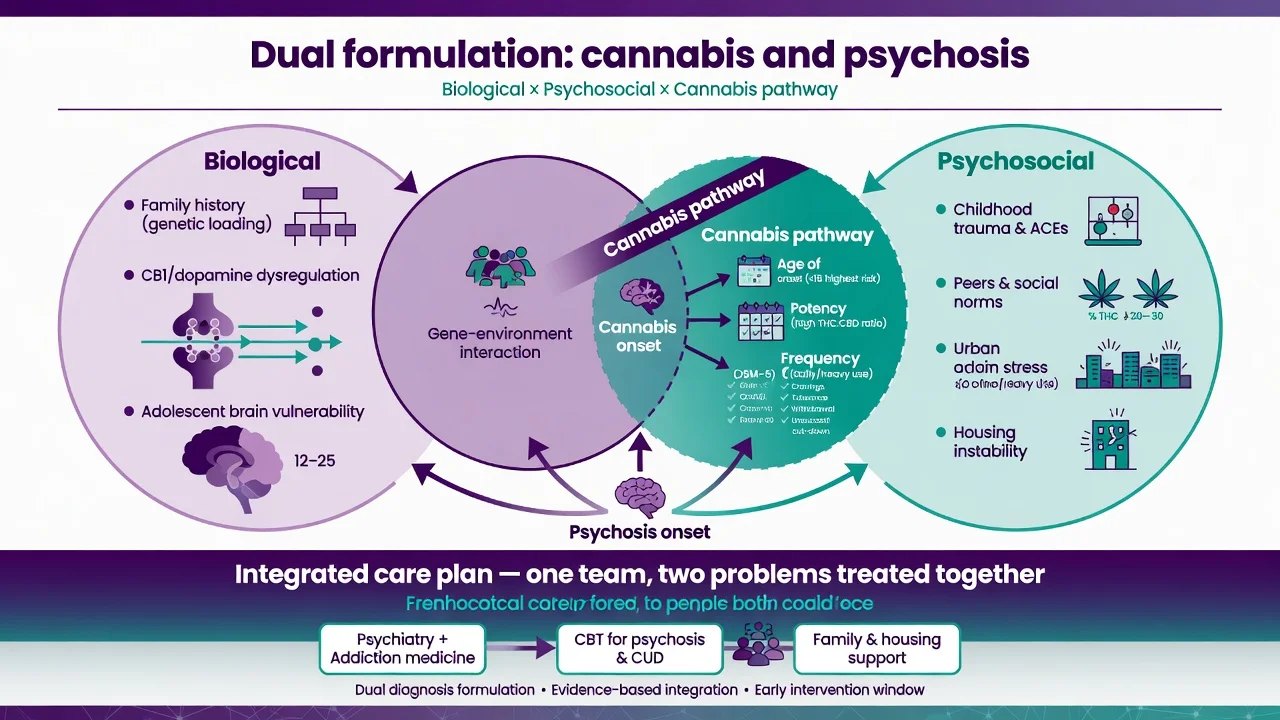
Write a dual formulation as you would for any complex case, covering biological, psychological, social, cannabis-axis and psychosis-axis factors in one integrated plan.[14][20]
- Biological: family history of psychosis, neurodevelopmental load, CB1/dopamine pathway, sleep loss, concurrent substances. [19]
- Psychological: trauma, anxiety self-medication beliefs, appraisal of voices, motivation stage. [14]
- Social: peers, housing, unemployment, cultural meanings of cannabis, legal pressures. [20]
- Cannabis axis: age of onset, potency, frequency, CUD criteria, withdrawal, prior quit attempts. [13][15]
- Psychosis axis: symptom content, duration, insight, risk, treatment response. [20]
The care plan must address both axes with named interventions and review dates.[14][20]
Complications and pitfalls
- Calling everything "drug-induced" and discharging without follow-up despite SIP conversion risk.[9][10]
- Calling everything "primary schizophrenia" and never offering CUD treatment.[14]
- Withholding antipsychotics until "clean UDS."[8]
- Ignoring adolescent potency trends and only asking "do you smoke weed?" without frequency/potency.[6][13]
- Missing organic disease under a cannabis story.[20]
- Moralising that destroys engagement; or colluding with minimisation that ignores relapse data.[8]
- Metabolic neglect while chasing cannabis lectures.[20]
- Marketing CBD oil as proven CUD cure.[17]
Prognosis and disposition
Better signals: early cessation, short DUP/short SIP duration, good premorbid function, family support, EIS engagement, absence of other substances. Worse signals: ongoing daily high-THC use, non-adherence, prior SIP conversions, poor premorbid function, polysubstance use.[8][9][11]
Disposition. Match setting to risk: community EIS dual-diagnosis pathways, addiction dual clinics, crisis teams, or inpatient when safety fails. Every discharge needs crisis contacts, early-warning signs that include cannabis lapse, medication plan, and a named review. SIP needs planned longitudinal follow-up even if the acute episode settles.[9][20]
Special populations
Adolescents and students. Highest teaching yield for age-of-onset and developmental risk; involve family carefully; protect education; peer-network interventions matter.[3][11]
Perinatal. Joint perinatal psychiatry; discuss fetal and maternal mental health risks of ongoing cannabis; treat psychosis with pregnancy-aware psychopharmacology; safeguarding assessment.[20]
Indigenous and culturally diverse communities. Cultural formulation of use meanings; avoid stereotypes; still apply potency/frequency risk science; use interpreters and family structures appropriately.[20]
Intellectual disability. Adapted communication; diagnostic overshadowing risk; capacity assessment for specific decisions.[20]
Older adults. New psychosis after cannabis still needs organic work-up; lower medication starting doses; falls and QTc risk.[20]
Forensic interface. Intoxication and violence risk, driving while impaired, fitness to plead interfaces — document carefully; statutes are jurisdiction-specific.[20]
Evidence, guidelines and regional differences
RANZCP schizophrenia and related disorders guidance emphasises comprehensive care, physical health monitoring, family involvement, and addressing substance comorbidity as part of recovery-oriented practice — cannabis is a first-line substance to ask about in every FEP and multi-episode review. Local EIS and dual-diagnosis service branding varies by state and district; integrated principles travel even when logos do not.[20]
Landmark list for viva: Andréasson; Moore; Arseneault; Marconi; Di Forti 2015 and EU-GEI 2019; Schoeler relapse; Large age of onset; Myles FEP prevalence; Starzer and Niemi-Pynttäri conversion; Petrilli potency review; Gates Cochrane CUD psychosocial; Connor withdrawal; Gray NAC; McGuire CBD; Vaucher Mendelian randomisation; Hasan review-of-reviews; RANZCP guidance.[1][2][5][7][9][19]
Exam pearls
[5] [9] [17]POTENCY
Self-test: 18-year-old daily skunk, 3 weeks of paranoia, last joint yesterday
Working dual formulation: cannabis-associated first presentation — SIP versus primary FEP not yet settled. Safety assessment, organic screen, baseline metabolic/ECG, collateral, risk. Offer low-dose antipsychotic if psychosis is clear and impairing (e.g. aripiprazole 10 mg daily with akathisia counselling), EIS referral, MI for cessation, family psychoeducation, written review within days. Do not discharge as 'just weed' without follow-up given conversion epidemiology. Plan CUD psychosocial package and psychosis relapse plan that names cannabis as a trigger.[7][9][14][20]
References
- [1]Andréasson S, Allebeck P, Engström A, et al. Cannabis and schizophrenia. A longitudinal study of Swedish conscripts Lancet, 1987.PMID 2892048
- [2]Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review Lancet, 2007.PMID 17662880
- [3]Arseneault L, Cannon M, Poulton R, et al. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study BMJ, 2002.PMID 12446537
- [4]Arseneault L, Cannon M, Witton J, et al. Causal association between cannabis and psychosis: examination of the evidence Br J Psychiatry, 2004.PMID 14754822
- [5]Marconi A, Di Forti M, Lewis CM, et al. Meta-analysis of the Association Between the Level of Cannabis Use and Risk of Psychosis Schizophr Bull, 2016.PMID 26884547
- [6]Di Forti M, Marconi A, Carra E, et al. Proportion of patients in south London with first-episode psychosis attributable to use of high potency cannabis: a case-control study Lancet Psychiatry, 2015.PMID 26359901
- [7]Di Forti M, Quattrone D, Freeman TP, et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study Lancet Psychiatry, 2019.PMID 30902669
- [8]Schoeler T, Petros N, Di Forti M, et al. Effects of continuation, frequency, and type of cannabis use on relapse in the first 2 years after onset of psychosis: an observational study Lancet Psychiatry, 2016.PMID 27567467
- [9]Starzer MSK, Nordentoft M, Hjorthøj C Rates and Predictors of Conversion to Schizophrenia or Bipolar Disorder Following Substance-Induced Psychosis Am J Psychiatry, 2018.PMID 29179576
- [10]Niemi-Pynttäri JA, Sund R, Putkonen H, et al. Substance-induced psychoses converting into schizophrenia: a register-based study of 18,478 Finnish inpatient cases J Clin Psychiatry, 2013.PMID 23419236
- [11]Large M, Sharma S, Compton MT, et al. Cannabis use and earlier onset of psychosis: a systematic meta-analysis Arch Gen Psychiatry, 2011.PMID 21300939
- [12]Myles H, Myles N, Large M Cannabis use in first episode psychosis: Meta-analysis of prevalence, and the time course of initiation and continued use Aust N Z J Psychiatry, 2016.PMID 26286531
- [13]Petrilli K, Ofori S, Hines L, et al. Association of cannabis potency with mental ill health and addiction: a systematic review Lancet Psychiatry, 2022.PMID 35901795
- [14]Gates PJ, Sabioni P, Copeland J, et al. Psychosocial interventions for cannabis use disorder Cochrane Database Syst Rev, 2016.PMID 27149547
- [15]Connor JP, Stjepanović D, Budney AJ, et al. Clinical management of cannabis withdrawal Addiction, 2022.PMID 34791767
- [16]Gray KM, Carpenter MJ, Baker NL, et al. A double-blind randomized controlled trial of N-acetylcysteine in cannabis-dependent adolescents Am J Psychiatry, 2012.PMID 22706327
- [17]McGuire P, Robson P, Cubala WJ, et al. Cannabidiol (CBD) as an Adjunctive Therapy in Schizophrenia: A Multicenter Randomized Controlled Trial Am J Psychiatry, 2018.PMID 29241357
- [18]Vaucher J, Keating BJ, Lasserre AM, et al. Cannabis use and risk of schizophrenia: a Mendelian randomization study Mol Psychiatry, 2018.PMID 28115737
- [19]Hasan A, von Keller R, Friemel CM, et al. Cannabis use and psychosis: a review of reviews Eur Arch Psychiatry Clin Neurosci, 2020.PMID 31563981
- [20]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681