Psych · Addiction psychiatry — dual diagnosis and integrated care
Dual diagnosis and integrated care
Also known as Dual diagnosis · Co-occurring disorders · Dual disorders · Comorbid mental illness and substance use · Integrated Dual Disorder Treatment · IDDT · Coexisting severe mental illness and substance misuse · NICE CG120 · NICE NG58 · Sequential parallel integrated care
Exam-exhaustive fellowship reference on dual diagnosis (co-occurring mental illness and substance use): etiological models, sequential/parallel/integrated care, stages of change, motivational interviewing, common comorbidity pairs, systems barriers, NICE/RANZCP-style principles, recovery. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Dual diagnosis (also co-occurring disorders, dual disorders) is the co-occurrence of a mental disorder and a substance use disorder (SUD) in the same person. In fellowship practice the high-stakes form is severe mental illness (SMI) plus SUD — schizophrenia-spectrum, bipolar, or severe depression with alcohol, cannabis, stimulants, opioids or other drugs — but the same integrated logic applies across severity. Examiners test whether you can name care models (sequential, parallel, integrated), stage-match intervention, keep both diagnoses on the problem list, and fix the systems failures that bounce people between mental health and alcohol and other drug (AOD) services.[1][4][6]
Overview and definition
Co-occurring disorders is preferred in many modern systems; dual diagnosis remains common in exams and Australasian clinical speech. Operationally: each disorder meets diagnostic threshold in its own right, or substance-induced mental disorder is on the differential until course after reduced use clarifies. Do not wait for a pure primary label before treating both active problems.[3][6]
No-wrong-door / no-exclusion. People present to either mental health or AOD services. Either door must engage both domains, or actively hand over with a named shared plan — not bounce the person as "too complex for us."[6][17]
[4] [5]Classification — models of care
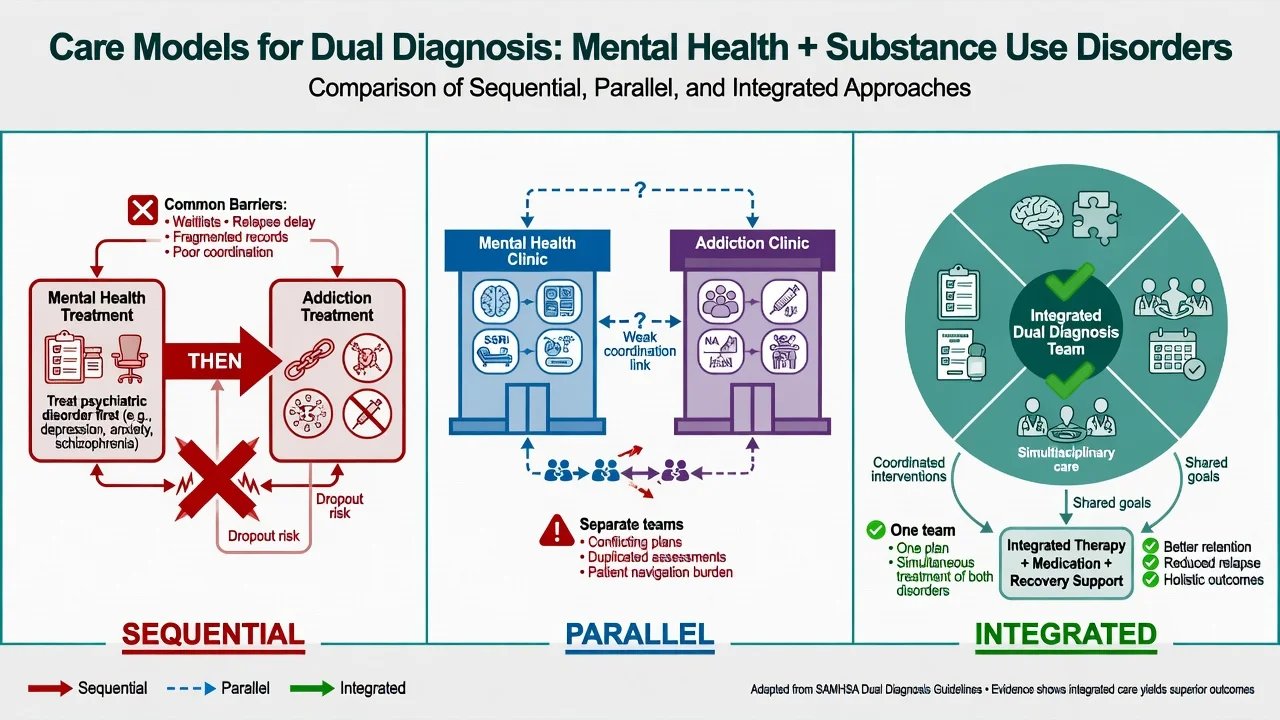
| Model | Structure | Typical failure mode | Fellowship stance |
|---|---|---|---|
| Sequential | One disorder treated to completion, then the other | Never "ready"; ping-pong; untreated psychosis or untreated alcohol | Historical; avoid as default |
| Parallel | Separate MH and AOD teams at the same time | No shared plan, conflicting advice, double booking burden | Acceptable only if tightly coordinated |
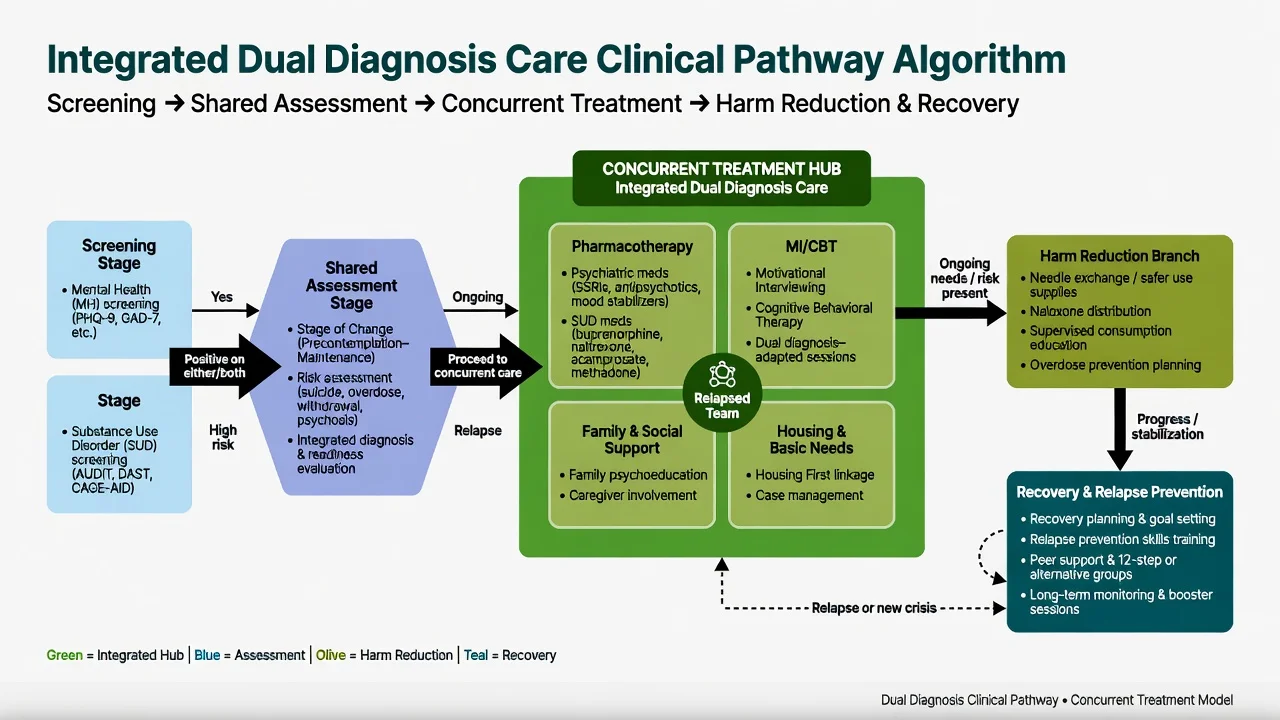
| Integrated | Same clinicians or team deliver both treatments in one cohesive package | Needs skill mix and fidelity | Preferred default for SMI + SUD |
| [4][6][7] |
Integrated Dual Disorder Treatment (IDDT) packages multi-element care: stage-wise substance work, psychiatric pharmacotherapy, motivational and cognitive-behavioural approaches, family, housing and vocational support within one program culture.[6][7][13]
Minkoff integrated model / CCISC. Conceptualises dual diagnosis as the expectation, not the exception, and designs systems so every program can meet co-occurring needs within a comprehensive continuous integrated system of care — not only a boutique dual clinic.[5][17]
NICE systems note (UK). NICE guidance on coexisting SMI and substance misuse emphasises that people should not be excluded; community guidance has stressed adapting services rather than inventing every specialist dual-diagnosis silo. Core principle for exams: coordinated concurrent care without exclusion, regardless of local branding.[6]
Epidemiology and risk
Dual diagnosis headlines
Population surveys established that mental disorders and alcohol/drug use disorders co-occur far above chance. The Epidemiologic Catchment Area study documented substantial comorbidity of mental disorders with alcohol and other drug abuse.[1] The National Comorbidity Survey Replication confirmed high 12-month comorbidity and severity clustering among anxiety, mood, impulse-control and substance disorders.[2]
In clinical SMI samples, hazardous substance use is frequent. Dual presentation associates with poorer adherence, more relapse and hospitalisation, homelessness, incarceration, blood-borne virus risk, and suicide — the exam reason integrated care is a systems priority, not a lifestyle add-on.[6][7]
Pathophysiology and etiological models
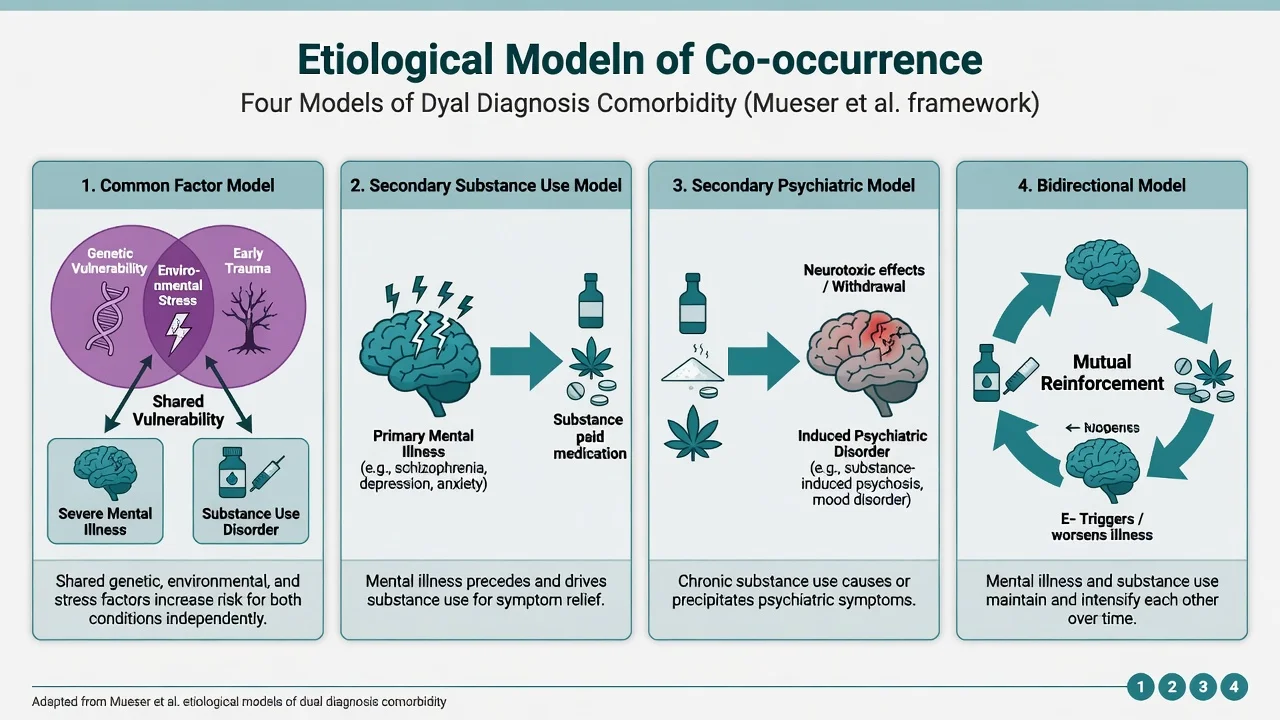
Mueser, Drake and Wallach organise increased comorbidity into four general models examiners expect by name.[3]
- Common factor — shared genetic, developmental or environmental vulnerability raises risk of both disorders.
- Secondary substance use disorder — mental illness increases vulnerability to SUD (including self-medication for dysphoria, negative symptoms, insomnia, or trauma-related arousal — a partial, not complete, explanation).
- Secondary psychiatric disorder — substance use precipitates or unmasks mental illness (classic: high-THC cannabis and psychosis incidence; stimulants and psychosis).
- Bidirectional — each disorder worsens the other in ongoing feedback.
Cannabis and psychosis. Daily and high-potency cannabis use associates with increased odds of psychotic disorder across European sites (EU-GEI).[14] After first-episode psychosis, continued high-frequency high-potency use associates with worse relapse-related outcomes.[15] Dual-diagnosis work here is secondary prevention with neurobiological grounding, not moral lecturing.
Clinical presentation and common pairs
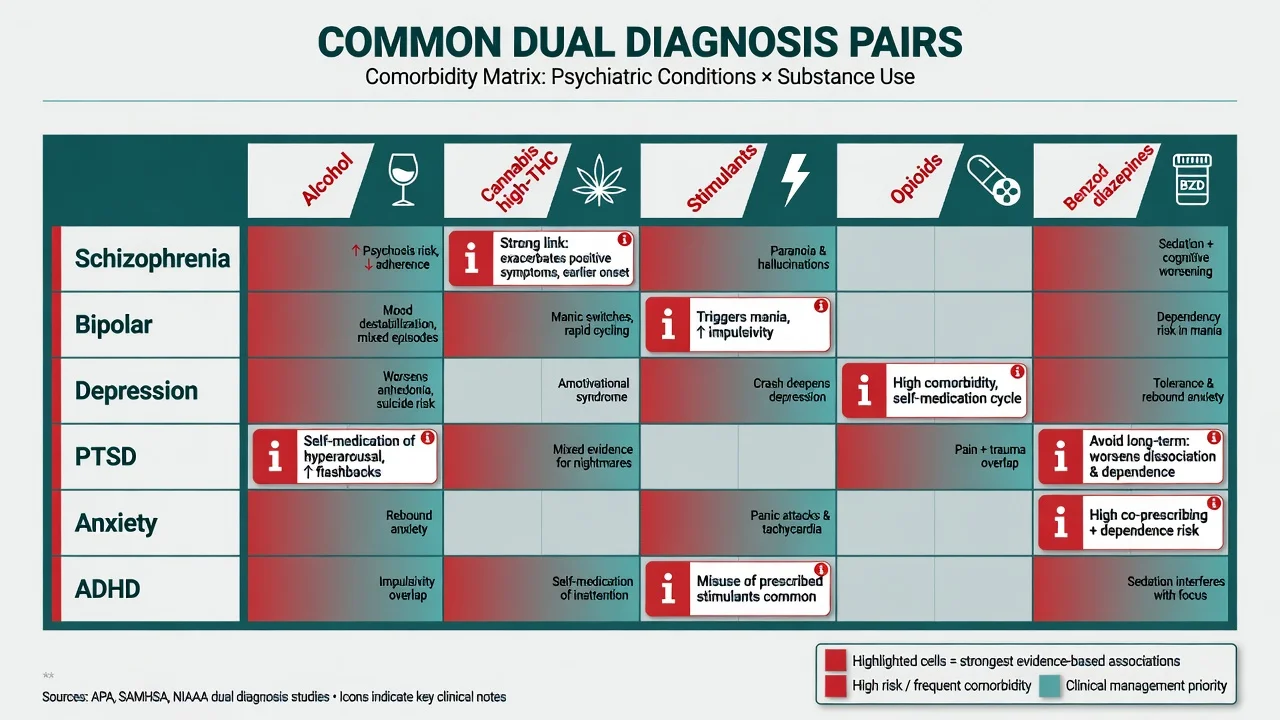
| Pair | Clinical pattern | Exam trap |
|---|---|---|
| Schizophrenia + cannabis/stimulants/alcohol | Earlier onset, more positive symptoms, poorer adherence | Labelling "just drugs" and stopping antipsychotic |
| Bipolar + alcohol/stimulants | Mania amplification; depressive drinking | Missing mood episode under intoxication |
| Depression + alcohol | Bidirectional worsening; suicide risk | SSRI alone without alcohol plan |
| PTSD + alcohol/opioids | Self-medication of hyperarousal/nightmares | Exposure work without substance safety |
| Anxiety + alcohol/benzodiazepines | Rebound anxiety; iatrogenic dependence | Long-term benzo as "treatment" |
| ADHD + stimulant misuse | Self-titration; diversion risk | Ignoring ADHD formulation when use is chaotic |
| Personality disorder + poly-substance | Interpersonal crisis + overdose risk | Diagnostic overshadowing of axis I treatable illness |
| [3][6][14] |
MSE under substance influence. Intoxication and withdrawal alter attention, affect, perception and insight. Record last use, objective signs of intoxication/withdrawal, and re-examine when safer. Collateral is essential when the history is minimised.[6]
Differential diagnosis
Win the differential on chronology, course after reduced use, and organic exclusion — not on a single urine screen.[3][6]
Primary mental illness + SUD
- Symptoms precede heavy use or persist weeks after abstinence
- Family history of primary disorder
- Classic syndrome structure
- Treat both concurrently
Substance-induced mental disorder
- Onset locked to intoxication or withdrawal
- Often remits with sustained abstinence
- May unmask primary illness over time
- Do not abandon care during the trial of reduced use
Organic / withdrawal emergency
- Delirium, Wernicke, seizure, fever
- Stimulant toxicity, opioid overdose
- Hepatic encephalopathy
- Medical first
Personality / trauma presentation
- Affective instability, abandonment themes
- Still screen for treatable mood/psychosis/SUD
- Risk of polypharmacy and benzo dependence
- Structured therapies when ready
Assessment
Structure every dual-diagnosis assessment as two complete assessments plus integration points.[6][13]
- Psychiatric history and MSE with quoted symptom examples.
- Substance timeline — substances, age of onset, quantity, frequency, route, last use, withdrawal history, prior AOD treatment, overdose history, injecting risks.
- Stage of change for each substance and for psychiatric adherence (precontemplation through maintenance).[10]
- Risk — suicide, self-harm, violence, vulnerability, child protection, driving, overdose (especially opioids + benzodiazepines + alcohol).
- Capacity for specific decisions; local Mental Health Act least-restrictive principles (do not invent foreign section numbers).
- Social recovery capital — housing, income, work/study, relationships, legal issues.
- Physical exam and targeted investigations.
- Motivation and goals in the person's words — the raw material for MI.[11]
Tools (conceptual). AUDIT, DUDIT, CAGE, ASSIST, and addiction severity inventories support quantification; they never replace clinical timeline and stage assessment. Brief intervention evidence is stronger for non-dependent unhealthy alcohol use than for severe dependence — dual SMI + dependence needs more than a single brief advice chat.[20]
[6]Investigations
Baseline directed by presentation: FBC, U&E, LFT, glucose/lipids when starting psychotropics, ECG if QTc-risk drugs or stimulant history, pregnancy test when relevant, infectious disease screen when risk (HIV, hepatitis B/C, syphilis). Urine drug screens support but never exclude primary illness or prove current clinical state. Image/EEG when organic red flags fire.[6][16]
Acute management
Stabilise life-threatening withdrawal (alcohol/benzodiazepine pathways with thiamine for alcohol risk), treat overdose, de-escalate agitation, exclude delirium and medical mimics, and start psychiatric treatment when indicated without demanding prior perfect abstinence.[6][16]
Least-restrictive setting that is still safe. Involve family or supports early under privacy law. If the person is precontemplative about substance use but accepting psychiatric care, engage the psychiatric door and keep the substance conversation open with MI — do not eject them for lack of readiness.[10][11]
Definitive management — integrated, stage-wise care
Principles of integrated care
Drake and colleagues summarise program implications: parallel separate systems do not deliver accessible, integrated, tailored interventions; integrated outpatient packages that combine mental health and substance treatment in one cohesive approach are the evidence-informed direction of travel, with multi-element components (stage-wise work, pharmacotherapy, psychosocial therapies, assertive outreach where needed).[4][6][7]
Fidelity matters. In the New Hampshire dual disorders study, higher fidelity assertive community treatment was associated with better client outcomes than low-fidelity delivery of the same nominal model.[18]
Stages of change
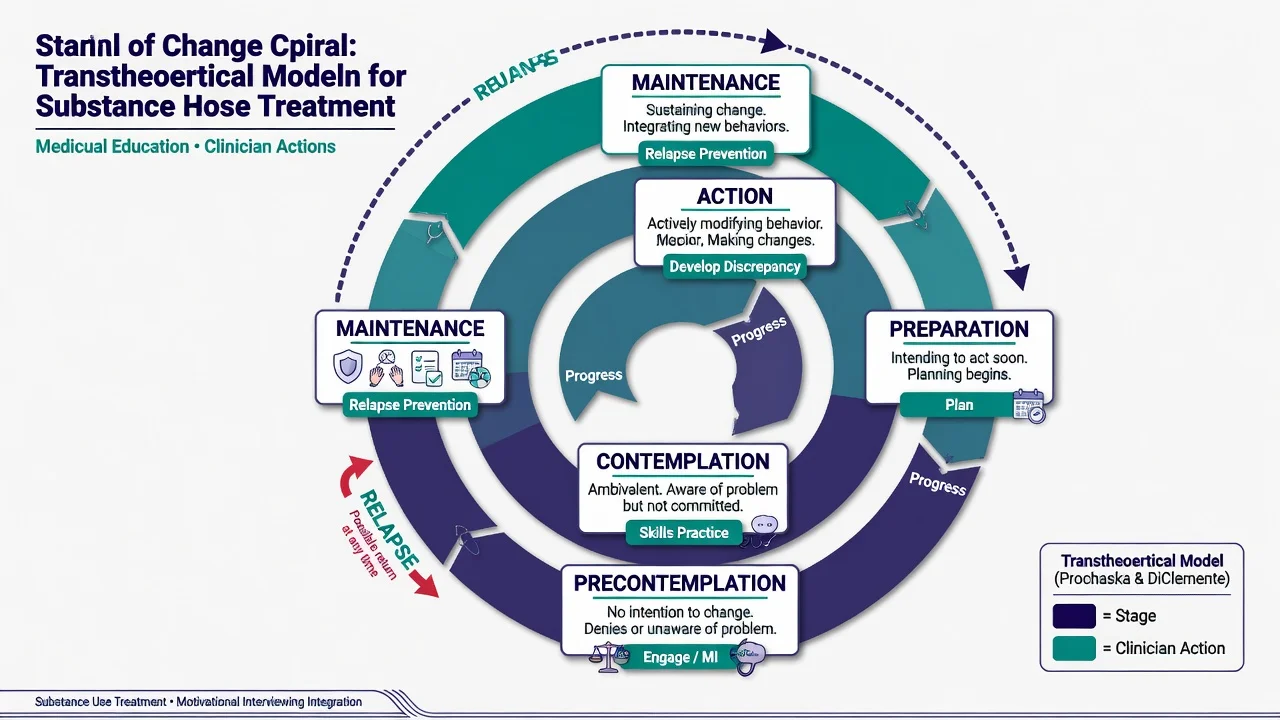
Prochaska and DiClemente's stages (precontemplation, contemplation, preparation, action, maintenance, with possible relapse) organise dual-diagnosis engagement.[10]
| Stage | Person's stance | Clinician move |
|---|---|---|
| Precontemplation | No intent to change substance use | Engage, build alliance, harm reduction, MI |
| Contemplation | Ambivalence | Develop discrepancy; explore pros/cons |
| Preparation | Planning change | Concrete plan, date, supports, meds if indicated |
| Action | Active change | Skills, CBT, contingency where available, pharmacotherapy |
| Maintenance | Sustaining | Relapse prevention, recovery capital |
| Relapse | Return to use | Non-punitive re-engagement; re-stage |
| [10][13] |
Motivational interviewing
MI is a collaborative, person-centred, directive style that helps resolve ambivalence and elicit the person's own reasons for change. Core spirit: partnership, acceptance, compassion, evocation. Classic principles include expressing empathy, developing discrepancy, rolling with resistance (sustain talk), and supporting self-efficacy.[11]
Meta-analytic evidence supports MI across target problems with variable effect sizes and larger short-term effects that often attenuate over time — use MI as engagement fuel, not as the only treatment for severe dependence or SMI.[11][12]
OARS skills (exam mnemonic): Open questions, Affirmations, Reflective listening, Summaries — plus recognising and reinforcing change talk.[11]
Psychosocial package
- Stage-wise dual-disorder counselling / CBT adaptations for dual diagnosis.[13]
- Family psychoeducation and communication work.[13]
- Contingency management where available and ethical for the substance target.[7]
- Assertive outreach / ACT platforms for high-need dual clients, with fidelity attention.[18]
- Peer recovery support services as adjunctive continuum elements.[19]
- Housing First / supported housing and vocational recovery (IPS principles) as clinical outcomes.[7][8]
Evidence honesty (Cochrane). Hunt and colleagues' Cochrane review of psychosocial interventions for people with both SMI and substance misuse finds limited high-quality evidence that specific psychosocial packages clearly outperform standard care on substance outcomes — methodological challenges and heterogeneity are large. Fellowship answer: integrate care because fragmentation fails clinically and ethically, while remaining honest that mega-RCTs have not produced a single silver-bullet dual therapy. Do not use Cochrane limits as a licence for therapeutic nihilism or sequential gatekeeping.[9][7]
Pharmacotherapy principles (dual setting)
Treat the psychiatric disorder with appropriate evidence-based agents and monitoring while addressing substance use pharmacologically when indicated. Examples of substance-targeted pharmacotherapy examiners expect you to name (exact regimens are jurisdiction- and product-information dependent).[6][16]
| Target | Agents / approaches (principles) | Dual-diagnosis notes |
|---|---|---|
| Alcohol use disorder | Naltrexone; acamprosate; disulfiram in selected adherent patients | Start after medical review; hepatic status for naltrexone/disulfiram |
| Opioid use disorder | Opioid agonist treatment (methadone or buprenorphine) as first-line for dependence | Integrate with mental health team; watch sedation with benzos |
| Nicotine | NRT, varenicline, bupropion as appropriate | High prevalence in SMI; treat actively |
| Psychosis | Antipsychotic at appropriate dose with metabolic/ECG baseline | Do not withhold for ongoing cannabis; counsel potency/frequency |
| Bipolar / depression | Mood stabilisers / antidepressants per primary diagnosis | Alcohol worsens course; plan both |
| [6][16] |
Harm reduction remains valid when abstinence is not the current stage: safer use advice, naloxone access for opioid risk, blood-borne virus prevention, thiamine for alcohol risk, and avoiding sudden unsupervised benzo/alcohol cessation that precipitates seizures.[6]
Systems barriers
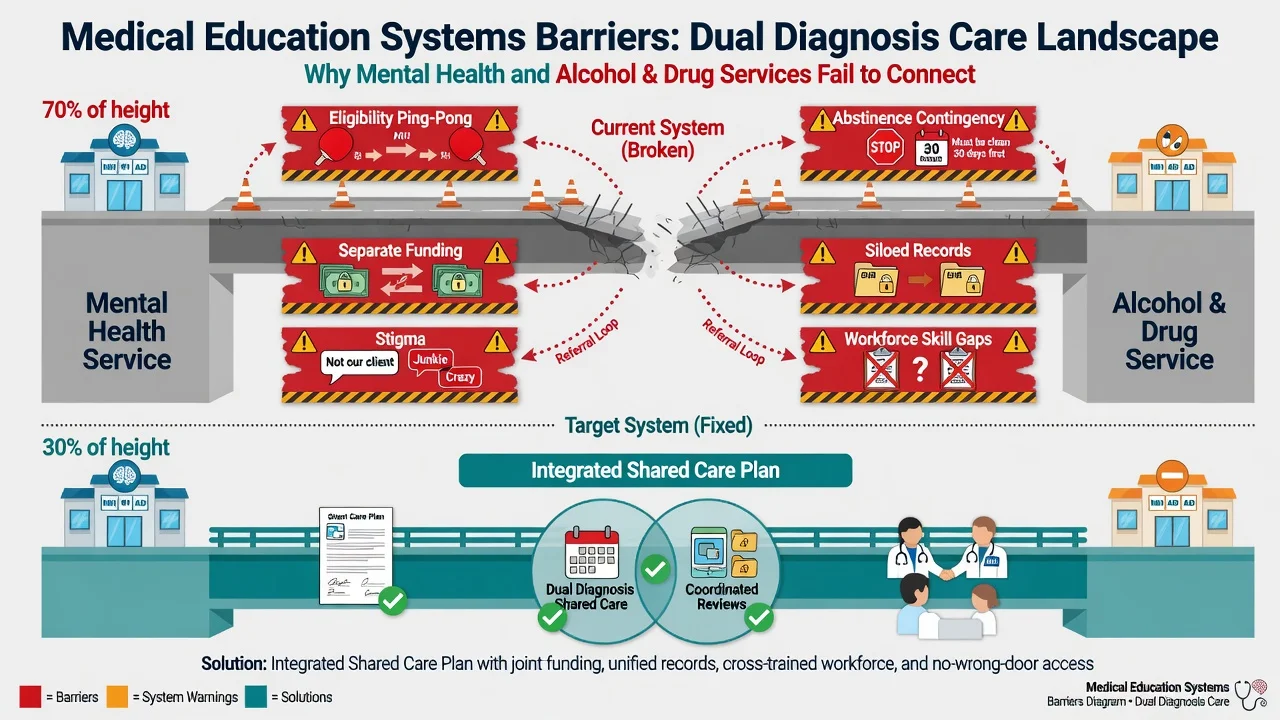
Classic failures: separate funding streams, separate records, workforce skill gaps, abstinence-contingent mental health admission criteria, mental-health-too-unstable exclusion from residential AOD, stigma, and clinician countertransference. Solutions: shared care plans, dual-trained staff, co-location or single team IDDT, joint governance, and CCISC-style expectation that co-occurrence is the norm.[6][17]
Subtypes and scenarios
Psychosis + cannabis/stimulants. Concurrent antipsychotic care, MI for substance reduction, family work; high-THC daily use is a relapse driver after FEP.[14][15][16]
Bipolar + alcohol. Mood stabilisation plus alcohol pharmacotherapy and MI; mania and intoxication amplify risk.[6]
Depression + alcohol. Treat depression and alcohol together; monitor suicide risk closely.[6]
PTSD + substance. Safety, substance stabilisation, then trauma-focused work when stage and support allow.[6][13]
Forensic dual diagnosis. Court liaison, diversion, integrated community orders with dual treatment conditions.[6]
Homelessness. Housing as treatment platform; integrated outreach.[7][8]
Youth / FEP. Early intervention multi-element care must include substance module from day one.[16]
Complications and pitfalls
- Sequential gatekeeping and service ping-pong.[4]
- Withholding antipsychotics or antidepressants until urine is clean.[6]
- Missing alcohol/benzo withdrawal risk.[6]
- Creating benzodiazepine dependence while "treating anxiety."[6]
- Opioid + sedative overdose clusters.[6]
- Over-reading a single UDS; under-taking collateral.[6]
- Using "self-medication" as the whole formulation.[3]
- Ignoring physical health (metabolic, hepatic, infectious).[16]
- Therapeutic nihilism after reading mixed RCT syntheses.[9]
Prognosis and recovery
Longitudinal New Hampshire dual diagnosis data show that substantial recovery across substance, psychiatric, and functional domains is possible over a decade of integrated community care for co-occurring schizophrenia and SUD.[8] Disposition matches intensity to need: integrated outpatient, high-fidelity ACT/IDDT, dual-capable residential programs, crisis plans, and peer supports.[18][19]
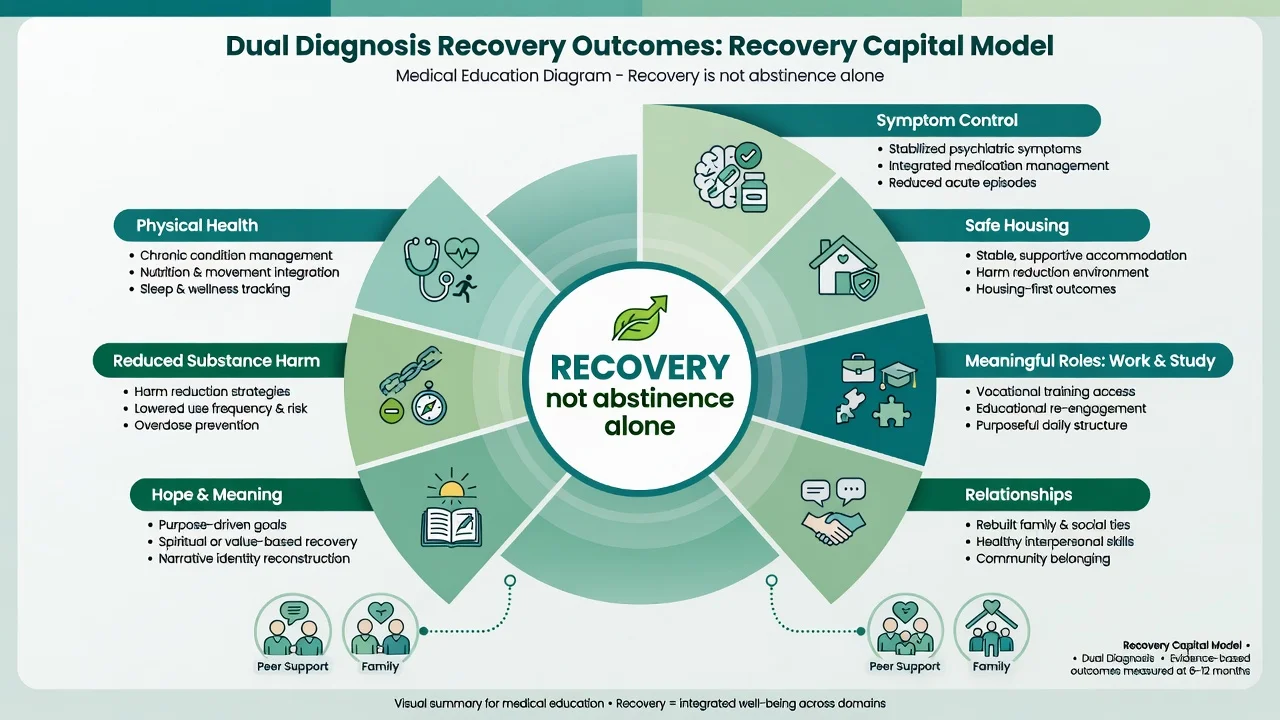
Recovery includes reduced substance harm or abstinence when chosen, psychiatric stability, housing, meaningful roles, relationships, and personal meaning — not a single biomarker.[8][19]
Special populations
Youth. Peers, potency culture, education preservation; parental involvement without infantilising.[16]
Perinatal. Joint perinatal psychiatry and AOD; safeguarding; breastfeeding and medication risk-benefit.[6]
Older adults. Alcohol + depression/cognitive; lower drug clearance; falls.[6]
Indigenous and culturally diverse. Cultural formulation, interpreter use, community supports; avoid pathologising culturally shaped content while treating form of illness and substance harm.[6]
Intellectual disability. Adapted communication; diagnostic overshadowing risk.[6]
Justice-involved. Integrated dual plans reduce revolving-door incarceration risk.[6]
Evidence, guidelines and regional differences
RANZCP schizophrenia guidance embeds substance use as a core treatment target within comprehensive care (not an afterthought). Local dual-diagnosis programs and AOD–MH partnerships vary by jurisdiction; the principles of concurrent integrated treatment, physical health monitoring, family work and recovery orientation travel even when logos differ.[16]
Landmark names for viva: Regier ECA; Kessler NCS-R; Mueser etiological models; Drake integrated treatment reviews; New Hampshire dual diagnosis outcomes; Minkoff/CCISC; Prochaska stages; MI (Miller lineage; Hettema/Lundahl syntheses); Hunt Cochrane 2019; Di Forti/Schoeler cannabis; RANZCP/NICE dual principles.[1][3][4][8][9]
Exam pearls
[4] [9] [14]INTEGRATE
Self-test: 24-year-old with schizophrenia and daily skunk cannabis, precontemplative
Do not discharge to 'come back when you stop smoking.' Start/continue antipsychotic with monitoring, engage with MI (OARS, discrepancy without confrontation), family psychoeducation, harm-reduction and potency/frequency counselling, housing/vocational support, shared dual care plan, and safety plan. Name stage: precontemplation for cannabis. Name model: integrated preferred over sequential.[11][15][16]
References
- [1]Regier DA, Farmer ME, Rae DS, et al. Comorbidity of mental disorders with alcohol and other drug abuse. Results from the Epidemiologic Catchment Area (ECA) Study JAMA, 1990.PMID 2232018
- [2]Kessler RC, Chiu WT, Demler O, et al. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication Arch Gen Psychiatry, 2005.PMID 15939839
- [3]Mueser KT, Drake RE, Wallach MA Dual diagnosis: a review of etiological theories Addict Behav, 1998.PMID 9801712
- [4]Drake RE, Mercer-McFadden C, Mueser KT, et al. Review of integrated mental health and substance abuse treatment for patients with dual disorders Schizophr Bull, 1998.PMID 9853791
- [5]Minkoff K An integrated treatment model for dual diagnosis of psychosis and addiction Hosp Community Psychiatry, 1989.PMID 2807203
- [6]Drake RE, Mueser KT, Brunette MF Management of persons with co-occurring severe mental illness and substance use disorder: program implications World Psychiatry, 2007.PMID 18188429
- [7]Drake RE, Mueser KT, Brunette MF, et al. A review of treatments for people with severe mental illnesses and co-occurring substance use disorders Psychiatr Rehabil J, 2004.PMID 15222148
- [8]Drake RE, McHugo GJ, Xie H, et al. Ten-year recovery outcomes for clients with co-occurring schizophrenia and substance use disorders Schizophr Bull, 2006.PMID 16525088
- [9]Hunt GE, Siegfried N, Morley K, et al. Psychosocial interventions for people with both severe mental illness and substance misuse Cochrane Database Syst Rev, 2019.PMID 31829430
- [10]Prochaska JO, DiClemente CC Stages and processes of self-change of smoking: toward an integrative model of change J Consult Clin Psychol, 1983.PMID 6863699
- [11]Hettema J, Steele J, Miller WR Motivational interviewing Annu Rev Clin Psychol, 2005.PMID 17716083
- [12]Lundahl B, Moleni T, Burke BL, et al. Motivational interviewing in medical care settings: a systematic review and meta-analysis of randomized controlled trials Patient Educ Couns, 2013.PMID 24001658
- [13]Brunette MF, Mueser KT Psychosocial interventions for the long-term management of patients with severe mental illness and co-occurring substance use disorder J Clin Psychiatry, 2006.PMID 16961419
- [14]Di Forti M, Quattrone D, Freeman TP, et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study Lancet Psychiatry, 2019.PMID 30902669
- [15]Schoeler T, Petros N, Di Forti M, et al. Effects of continuation, frequency, and type of cannabis use on relapse in the first 2 years after onset of psychosis: an observational study Lancet Psychiatry, 2016.PMID 27567467
- [16]Galletly C, Castle D, Dark F, et al. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the management of schizophrenia and related disorders Aust N Z J Psychiatry, 2016.PMID 27106681
- [17]Minkoff K, Cline CA Changing the world: the design and implementation of comprehensive continuous integrated systems of care for individuals with co-occurring disorders Psychiatr Clin North Am, 2004.PMID 15550290
- [18]McHugo GJ, Drake RE, Teague GB, et al. Fidelity to assertive community treatment and client outcomes in the New Hampshire dual disorders study Psychiatr Serv, 1999.PMID 10375153
- [19]Eddie D, Hoffman L, Vilsaint C, et al. Lived Experience in New Models of Care for Substance Use Disorder: A Systematic Review of Peer Recovery Support Services and Recovery Coaching Front Psychol, 2019.PMID 31263434
- [20]Saitz R Alcohol screening and brief intervention in primary care: Absence of evidence for efficacy in people with dependence or very heavy drinking Drug Alcohol Rev, 2010.PMID 20973848