Psych · Addiction psychiatry — behavioural addictions
Gambling disorder
Also known as Pathological gambling · Problem gambling · Compulsive gambling · Gambling addiction · Ludomania · Behavioural addiction gambling
Exam-exhaustive fellowship reference on gambling disorder — DSM-5-TR/ICD-11 criteria and reclassification; epidemiology, suicide and debt risk; reward-circuit and opioid-system mechanisms; CBT first-line care; off-label naltrexone and nalmefene evidence; comorbidity (SUD, mood, bipolar, personality); dopamine-agonist ICDs; screening and regional deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Gambling disorder (GD) is the only behavioural addiction formally co-located with substance-related disorders in DSM-5-TR. Examiners test criteria thresholds and reclassification history, suicide and financial risk assessment, CBT as first-line care, realistic appraisal of naltrexone/nalmefene evidence, dual diagnosis, and the classic dopamine-agonist trap in Parkinson disease and restless legs syndrome.[1][7][9]
Overview and definition
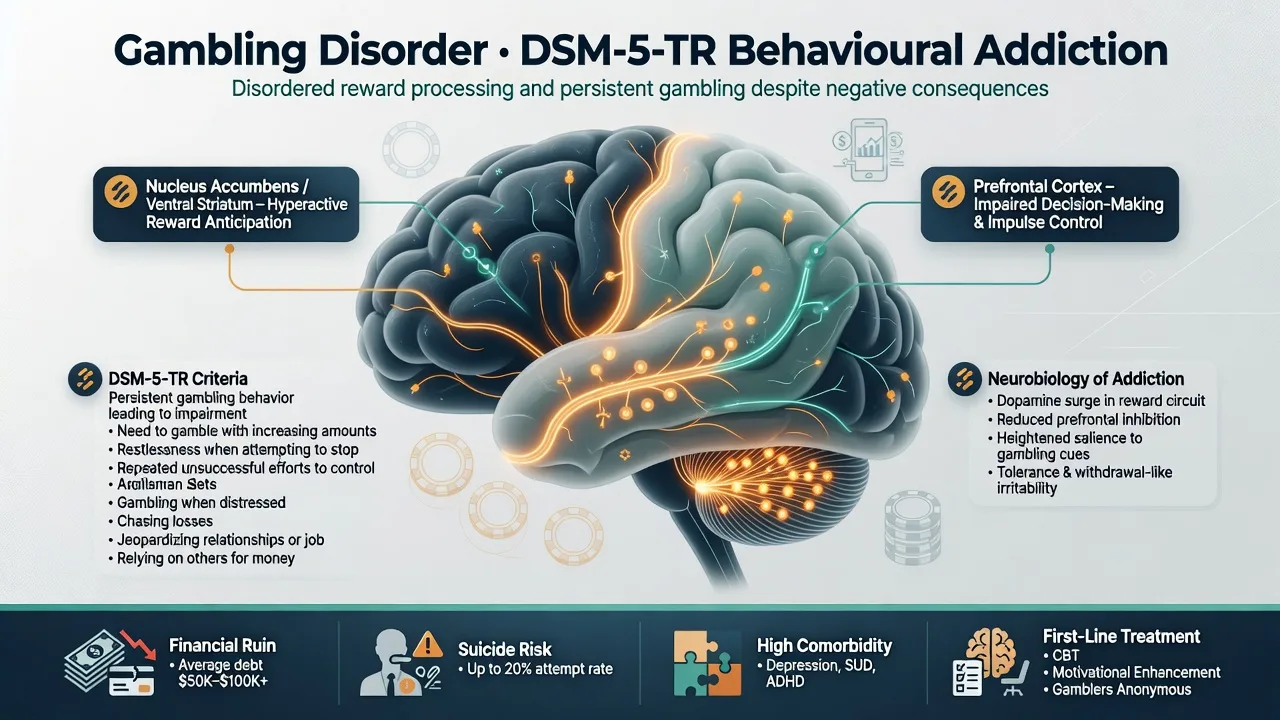
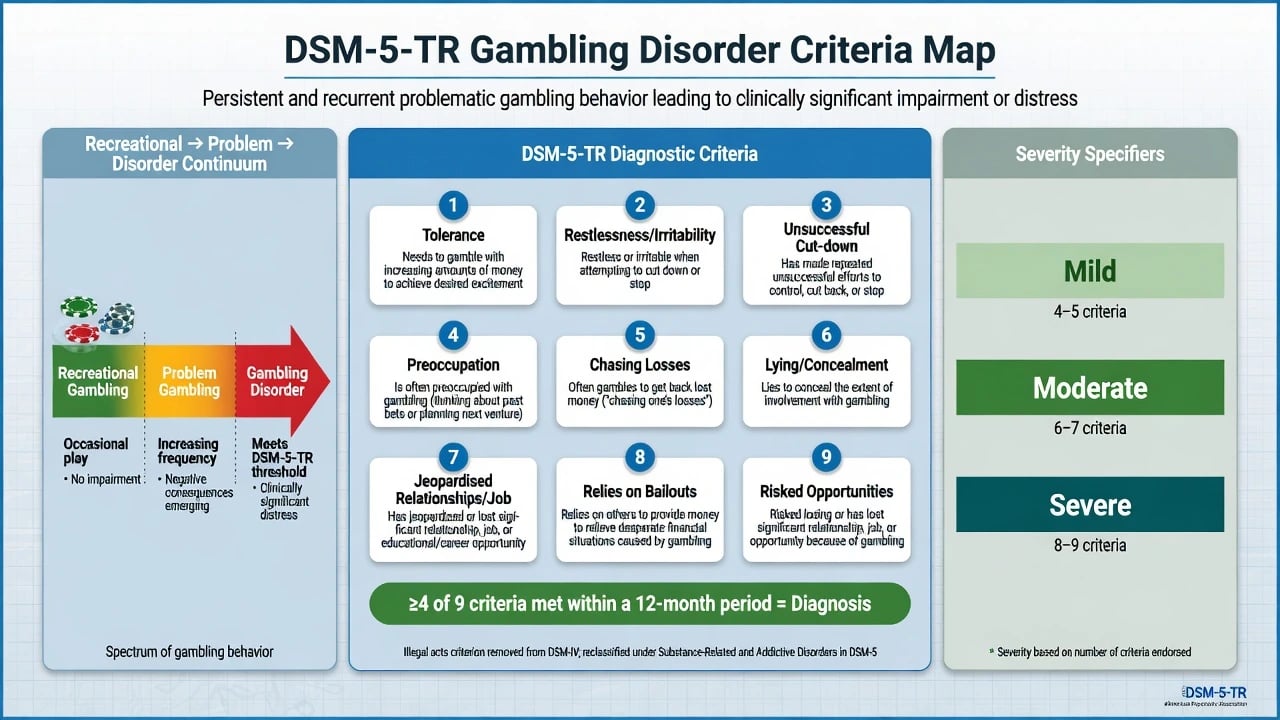
GD is a persistent, recurrent pattern of gambling leading to clinically significant impairment or distress. In DSM-5-TR, diagnosis requires at least 4 of 9 criteria within a 12-month period. Severity by criterion count: mild 4–5, moderate 6–7, severe 8–9.[1][15]
The nine criteria map to: (1) needing to gamble with increasing amounts for the desired excitement (tolerance); (2) restlessness or irritability when attempting to cut down or stop; (3) repeated unsuccessful efforts to control, cut back, or stop; (4) preoccupation with gambling; (5) often gambling when distressed; (6) after losing money, returning another day to get even (chasing losses); (7) lying to conceal the extent of involvement; (8) jeopardised or lost a significant relationship, job, or opportunity; (9) relying on others to provide money to relieve desperate financial situations (bailouts).[1]
DSM-5 changes vs DSM-IV pathological gambling (exam classics). The disorder moved from Impulse-Control Disorders Not Elsewhere Classified into Substance-Related and Addictive Disorders. The illegal acts criterion was removed. The diagnostic threshold fell from 5 of 10 to 4 of 9 criteria. Specifiers include episodic vs persistent course and early vs sustained remission after full criteria were previously met.[1][15]
ICD-11 recognises gambling disorder (with predominantly online vs offline patterns and episodic vs continuous course) and a broader harmful gambling construct. State which manual you are using when coding language is examined.[1]
Classification continuum
Recreational gambling
- Controlled spending and time
- No major role impairment
- Can stop without distress cascade
- Still may need public-health messaging
Problem gambling
- Harms present but may be subthreshold for GD
- PGSI-type screens capture this band
- Brief intervention and MI useful
- Monitor escalation of continuous-access products
Gambling disorder
- ≥4 DSM-5-TR criteria / 12 months
- Chasing, concealment, bailouts common
- High suicide and debt risk
- Needs structured CBT and dual-diagnosis care
Iatrogenic ICD
- Dopamine agonist–associated gambling
- Often with other ICDs (shopping, sex, eating)
- Primary intervention is drug review
- Not 'willpower failure'
Continuous forms (electronic gaming machines, online casino and in-play sports betting) produce rapid event frequency and are over-represented in clinical samples relative to lottery play.[1][12][13]
Epidemiology and risk
Headline epidemiology and harm facts
Large US surveys place lifetime pathological gambling near 0.4–0.6% of adults, with problem gambling several-fold higher; international problem-gambling prevalence varies with product mix, regulation, and measurement tool.[6][7][12] Meta-analytic work shows very high rates of comorbid nicotine dependence, other substance use disorders, mood and anxiety disorders, and personality pathology among problem and pathological gamblers.[8] Clinical series document substantial social, legal, and financial disability.[13]
Risk factors include male sex (historically), early onset, impulsivity, trauma, family history of substance use or gambling problems, psychiatric comorbidity, low socioeconomic status, and high environmental accessibility (liberalised markets, smartphones, 24/7 online products).[1][7][12] Women may show faster progression once problem gambling starts (telescoping) and higher internalising comorbidity.[1]
Pathophysiology
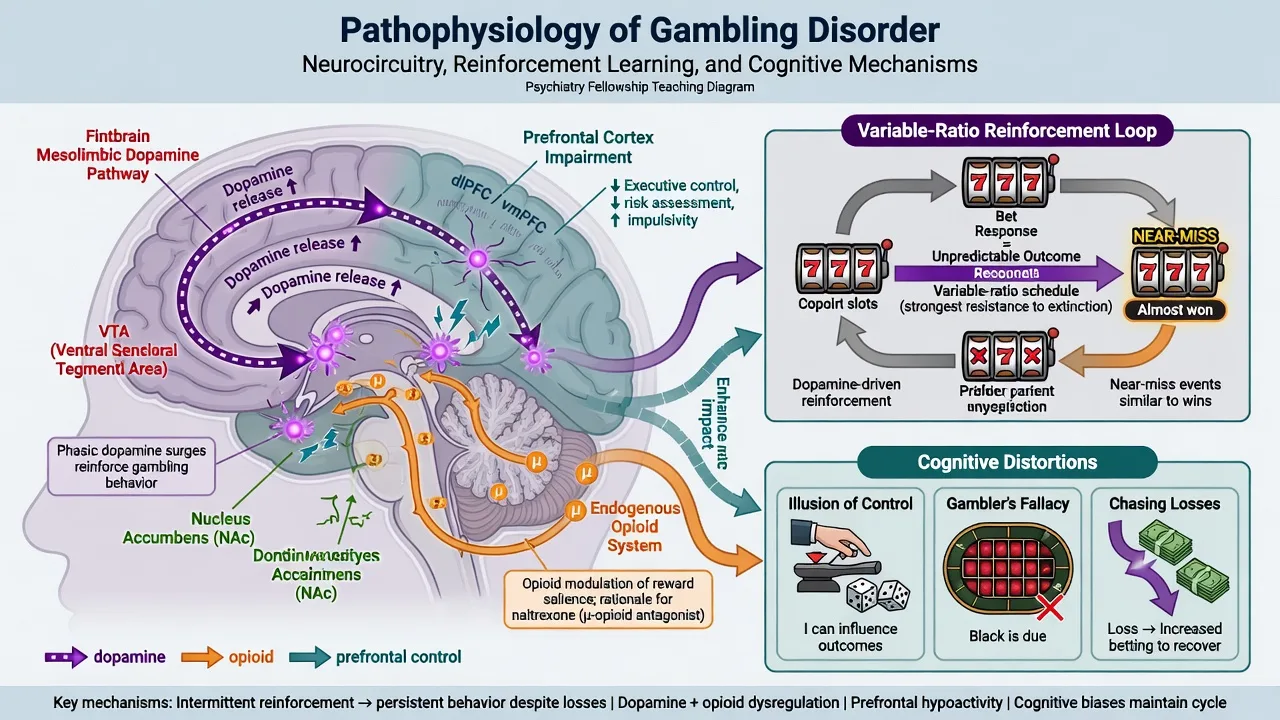
Neurobiological models implicate cortico-striato-limbic circuits for reward, salience attribution, craving, and habit — overlapping substance addictions more than classic OCD circuits.[1] Behavioural economics and learning theory emphasise variable-ratio reinforcement, near-miss effects, and conditioned cues (venues, apps, sports broadcasts). Cognitive distortions include illusion of control, gambler fallacy, superstitious rituals, and chasing-loss logic.[1][4]
Endogenous opioid systems modulate mesolimbic dopamine; this is the mechanistic rationale for studying opioid antagonists (naltrexone, nalmefene) against gambling urges.[1][2][3] Dopamine agonists (especially D2/D3-preferring agents used in Parkinson disease and restless legs syndrome) associate with impulse-control disorders including pathological gambling — a direct iatrogenic pathway examiners love.[9][14]
Clinical presentation
Typical phenomenology: escalating time and money; irritability when attempting abstinence; mental preoccupation with handicapping and fundraising; gambling to escape dysphoria; chasing losses; lying to partners; relationship breakdown; occupational failure; reliance on bailouts; and, in crises, suicidal ideation linked to debt and shame.[1][13]
MSE language. Describe affect (anxious, irritable, dysphoric after losses), thought content (gambling-focused plans, hopelessness about debt), insight (often partial — acknowledges harm yet minimises frequency), judgment, craving/urges, and risk (suicide, intimate-partner conflict, child neglect via depleted finances, forensic exposure).[1]
Forms. EGMs/pokies; casino tables; race and sports betting (including online in-play); online casino apps; speculative crypto-adjacent products in some cohorts. Continuous electronic forms carry high addictive liability.[12]
Differential diagnosis
Mania / hypomania
- Decreased need for sleep, grandiosity, pressured speech
- Spending and risk across domains, not only gambling
- Episodic with mood timeline
- Stabilise mood then reassess GD criteria
Substance-driven
- Intoxicated betting without independent pattern
- Still screen for independent GD when sober
- Alcohol common co-traveller
- Integrated dual-diagnosis care
Dopamine-agonist ICD
- Onset after agonist start or dose rise
- May include hypersexuality, shopping, binge eating
- Primary Rx: reduce/stop agonist with neurology
- Psychosocial support during taper
Recreational high stakes
- No loss of control or role collapse
- Can stop; finances remain planned
- Does not meet ≥4 criteria
- Still counsel on risk products
Do not confuse ego-syntonic reward-seeking gambling with classic OCD rituals performed to neutralise anxiety. Personality pathology (especially cluster B) may co-occur and complicate engagement without explaining away GD criteria.[1][6]
Clinical and bedside assessment
Structure history: preferred forms; session length and frequency; largest single loss; past-year net loss; loans, credit cards, payday lending, illegal acts; bailouts; self-exclusion attempts; prior GA/CBT; last gamble; alcohol and other drugs; mood and psychosis screens; ADHD traits; medication list (dopamine agonists); occupational and family impact; child-protection and domestic-violence risk.[1][13]
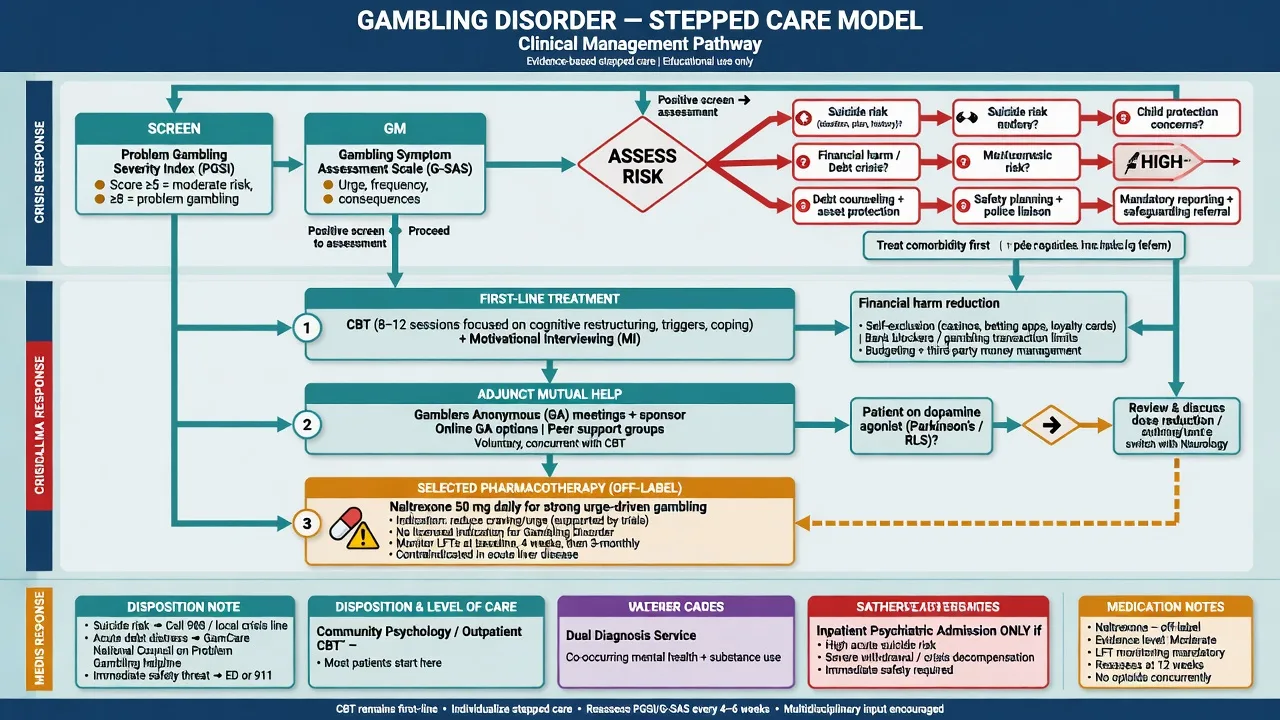
Scales (concepts you must own). Population and screening tools such as the Problem Gambling Severity Index (PGSI) stratify recreational / low-risk / moderate-risk / problem bands in public-health and primary-care contexts. The Gambling Symptom Assessment Scale (G-SAS) is a validated multi-item symptom scale used to track urge and gambling severity in treatment trials.[11] Brief screens (e.g. Lie/Bet-type two-item concepts) help case-finding in busy clinics — confirm with full criteria interview.[1]
Risk assessment is non-optional. Suicidal ideation and attempts are substantially elevated in clinical GD; debt crisis, relationship collapse, forensic threat, and comorbid depression/SUD amplify risk. Use a structured suicide assessment and safety plan.[1][7] Obtain collateral — partners often know true losses better than the patient reports.
Investigations
There is no diagnostic blood test for GD. Order urine drug screen when concurrent substance use is suspected. Before naltrexone, obtain baseline LFTs (and recheck during higher-dose or prolonged therapy); exclude acute hepatitis and counsel on alcohol co-use. Pregnancy test when relevant. Review Parkinson/RLS drug lists. Imaging is not routine for uncomplicated GD.[3][16]
Acute / crisis management
Stabilise medical issues if intoxicated or withdrawing from alcohol/sedatives. Create a collaborative safety plan, remove means, involve supports with consent when safe, and link to emergency financial counselling and gambling-help services. Inpatient admission is for risk or severe dual diagnosis, not for “detox from pokies” alone.[1]
Definitive management
Psychological therapies (first-line)
Cochrane synthesis supports cognitive-behavioural therapy for reducing gambling behaviour and related symptoms in the short term after therapy, while noting limitations in evidence quality and follow-up in older trials.[4] A key RCT found that individual CBT plus Gamblers Anonymous (GA) referral reduced gambling more during treatment than GA referral alone, with clinically meaningful improvements.[5]
CBT targets: cognitive distortions (control illusions, near-miss misinterpretation); urge monitoring and surfing; stimulus control (venue/app avoidance, device blockers); behavioural activation for dysphoria; problem-solving; and financial planning (budgeting, debt negotiation, third-party money management when agreed). Motivational interviewing and brief interventions help ambivalent or non-treatment-seeking patients. GA and other mutual-help groups are useful adjuncts, not a substitute for structured therapy in severe GD.[1][4][5]
Harm reduction and social interventions
Self-exclusion from venues and online operators; banking transaction blockers and spending limits; removal of betting apps; family agreements about cash access; occupational and legal support. Negotiate goals — some patients aim for total abstinence from all gambling; others initially target high-risk continuous forms.[1]
Pharmacotherapy
No medication has a formal regulatory indication specifically for GD in major jurisdictions; pharmacotherapy is always adjunctive to psychosocial care.[1]
Naltrexone (off-label). Oral opioid antagonist. Placebo-controlled trials (including Kim et al. 2001 and Grant et al. 2008) support reductions in gambling urges and behaviour in selected adults, particularly those with strong urges; dosing in trials has often been flexible and sometimes higher than the classic 50 mg alcohol-use dose, with careful monitoring.[2][3] Practical exam framing: discuss oral naltrexone, commonly starting around 50 mg daily after baseline LFTs, with specialist-supervised titration when used off-label for GD urges; avoid in acute hepatitis/liver failure; counsel on precipitated opioid withdrawal if the patient uses opioids; recheck LFTs on prolonged or higher-dose therapy. High-dose outpatient experience requires explicit safety monitoring.[3][16]
Nalmefene. Another opioid antagonist studied in multicentre double-blind work; selected doses reduced gambling symptoms versus placebo, with dosing sensitivity — know it as related evidence, not a first-line community default in all regions.[10]
Other agents. SSRIs may help comorbid anxiety/depression but are not first-line for pure GD. Mood stabilisers (e.g. lithium) are considered when bipolar comorbidity drives risk behaviour. Avoid dopamine agonists and review them if present.[1][9]
Treat comorbidity
NESARC and related work show dense comorbidity with alcohol and drug use disorders, mood and anxiety disorders, and personality disorders — treat concurrently, not sequentially forever.[6][8] Integrated dual-diagnosis care beats ping-pong between services.[1]
Australian and New Zealand practice emphasises state/territory gambling-help lines, self-exclusion schemes, venue harm-minimisation, and addiction psychology pathways. RANZCP-aligned care expects suicide risk competence, dual diagnosis, culturally safe assessment for Aboriginal and Torres Strait Islander and Māori peoples, and realistic off-label pharmacotherapy counselling. Electronic gaming machines remain a major local harm vector in many jurisdictions.[1][12]
Subtypes and scenarios
Online sports betting in young men — continuous in-play products, credit-card debt, peer normalisation. EGM-dependent middle age — long sessions, dissociation, community venue access. Escape gambling — more often internalising comorbidity and trauma. Bipolar interface — treat mania; do not label every manic spending spree as lifelong GD without longitudinal review. Forensic — fraud or theft to fund gambling; address GD in formulation and risk management without offering legal advice beyond clinical facts.[1][13]
Complications and pitfalls
Other pitfalls: moralising without offering CBT; naltrexone as solo “cure”; missing suicide; colluding with endless family bailouts that remove natural contingencies; missing alcohol dependence; diagnosing GD during untreated mania.[1][3]
Prognosis and disposition
Course is often chronic-relapsing, yet many community cases improve; clinical treatment-seekers are skewed toward higher severity and comorbidity.[1][7] Better outcomes associate with engagement in CBT, reduced access to high-risk products, debt stabilisation, treated dual diagnosis, and social support. Disposition ladder: GP shared care and gambling-help services → specialist addiction psychology/psychiatry → dual-diagnosis programmes → inpatient only for high suicide risk or severe concurrent illness.[1][4]
Special populations
Youth. High digital exposure; involve family systems; address school/financial proxy access. Older adults. Retirement fund depletion, cognitive vulnerability, loneliness-driven venue attendance. Women. Higher shame barriers and mood/anxiety comorbidity; screen actively. Parkinson disease / RLS. Systematic ICD enquiry when prescribing or reviewing dopamine agonists.[1][9] Cultural safety. Stigma, community shame, and access barriers require non-stereotyping, culturally informed formulation (FRANZCP expectation).[1]
Evidence and guidelines
Name at viva: Potenza Nature Reviews Disease Primers 2019 synthesis; Petry NESARC comorbidity 2005; Kessler NCS-R 2008; Lorains comorbidity meta-analysis 2011; Calado and Griffiths worldwide prevalence review 2016; Cowlishaw Cochrane psychological therapies 2012; Petry CBT RCT 2006; Kim 2001 and Grant 2008 naltrexone RCTs; Grant nalmefene 2010; G-SAS validation; Weintraub dopamine-agonist ICD studies.[1][2][3][4][5][6][7][8][9][10][11][12]
Exam pearls
GAMBLES
Self-test: criteria and naltrexone framing
List four DSM-5-TR criteria from memory including chasing losses and bailouts. State severity bands (mild 4–5, moderate 6–7, severe 8–9). Outline a CBT package. State that naltrexone is off-label, often discussed from ~50 mg oral daily with baseline LFTs and urge-focused selection, citing Kim/Grant trial evidence without claiming a formal GD indication.[1][2][3][5]
References
- [1]Potenza MN, Balodis IM, Derevensky J, Grant JE, Petry NM, Verdejo-Garcia A, et al. Gambling disorder Nat Rev Dis Primers, 2019.PMID 31346179
- [2]Kim SW, Grant JE, Adson DE, Shin YC Double-blind naltrexone and placebo comparison study in the treatment of pathological gambling Biol Psychiatry, 2001.PMID 11377409
- [3]Grant JE, Kim SW, Hartman BK A double-blind, placebo-controlled study of the opiate antagonist naltrexone in the treatment of pathological gambling urges J Clin Psychiatry, 2008.PMID 18384246
- [4]Cowlishaw S, Merkouris S, Dowling N, Anderson C, Jackson A, Thomas S Psychological therapies for pathological and problem gambling Cochrane Database Syst Rev, 2012.PMID 23152266
- [5]Petry NM, Ammerman Y, Bohl J, Doersch A, Gay H, Kadden R, et al. Cognitive-behavioral therapy for pathological gamblers J Consult Clin Psychol, 2006.PMID 16822112
- [6]Petry NM, Stinson FS, Grant BF Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions J Clin Psychiatry, 2005.PMID 15889941
- [7]Kessler RC, Hwang I, LaBrie R, Petukhova M, Sampson NA, Winters KC, et al. DSM-IV pathological gambling in the National Comorbidity Survey Replication Psychol Med, 2008.PMID 18257941
- [8]Lorains FK, Cowlishaw S, Thomas SA Prevalence of comorbid disorders in problem and pathological gambling: systematic review and meta-analysis of population surveys Addiction, 2011.PMID 21210880
- [9]Weintraub D, Koester J, Potenza MN, Siderowf AD, Stacy M, Voon V, et al. Impulse control disorders in Parkinson disease: a cross-sectional study of 3090 patients Arch Neurol, 2010.PMID 20457959
- [10]Grant JE, Odlaug BL, Potenza MN, Hollander E, Kim SW Nalmefene in the treatment of pathological gambling: multicentre, double-blind, placebo-controlled study Br J Psychiatry, 2010.PMID 20884959
- [11]Kim SW, Grant JE, Potenza MN, Blanco C, Hollander E The Gambling Symptom Assessment Scale (G-SAS): a reliability and validity study Psychiatry Res, 2009.PMID 19200607
- [12]Calado F, Griffiths MD Problem gambling worldwide: An update and systematic review of empirical research (2000-2015) J Behav Addict, 2016.PMID 27784180
- [13]Grant JE, Kim SW Demographic and clinical features of 131 adult pathological gamblers J Clin Psychiatry, 2001.PMID 11780876
- [14]Weintraub D, Siderowf AD, Potenza MN, Goveas J, Morales KH, Duda JE, et al. Association of dopamine agonist use with impulse control disorders in Parkinson disease Arch Neurol, 2006.PMID 16831966
- [15]Grant JE, Odlaug BL, Chamberlain SR Gambling disorder, DSM-5 criteria and symptom severity Compr Psychiatry, 2017.PMID 28260605
- [16]Kim SW, Grant JE, Yoon G, Williams KA, Remmel RP Safety of high-dose naltrexone treatment: hepatic transaminase profiles among outpatients Clin Neuropharmacol, 2006.PMID 16614539