Psych · Addiction psychiatry — behavioural addictions
Gaming and internet addiction
Also known as Internet gaming disorder · Gaming disorder · Pathological gaming · Video game addiction · Problematic internet use · Internet addiction · Online game addiction
Exam-exhaustive fellowship reference on gaming disorder and broader problematic internet use — ICD-11 clinical gaming disorder vs DSM-5-TR Section III IGD research criteria; epidemiology; I-PACE mechanisms; ADHD/ASD/depression differentials; CBT and STICA evidence; limited pharmacotherapy context; youth safeguarding and regional deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Gaming and broader problematic internet use sit at the contested edge of behavioural addiction nosology. Examiners test the ICD-11 vs DSM-5-TR status difference, functional-impairment thresholds, I-PACE mechanisms, youth and family assessment, CBT/STICA evidence quality, and realistic pharmacotherapy counselling without moral panic or hour-counting alone.[1][3][7]
Overview and definition
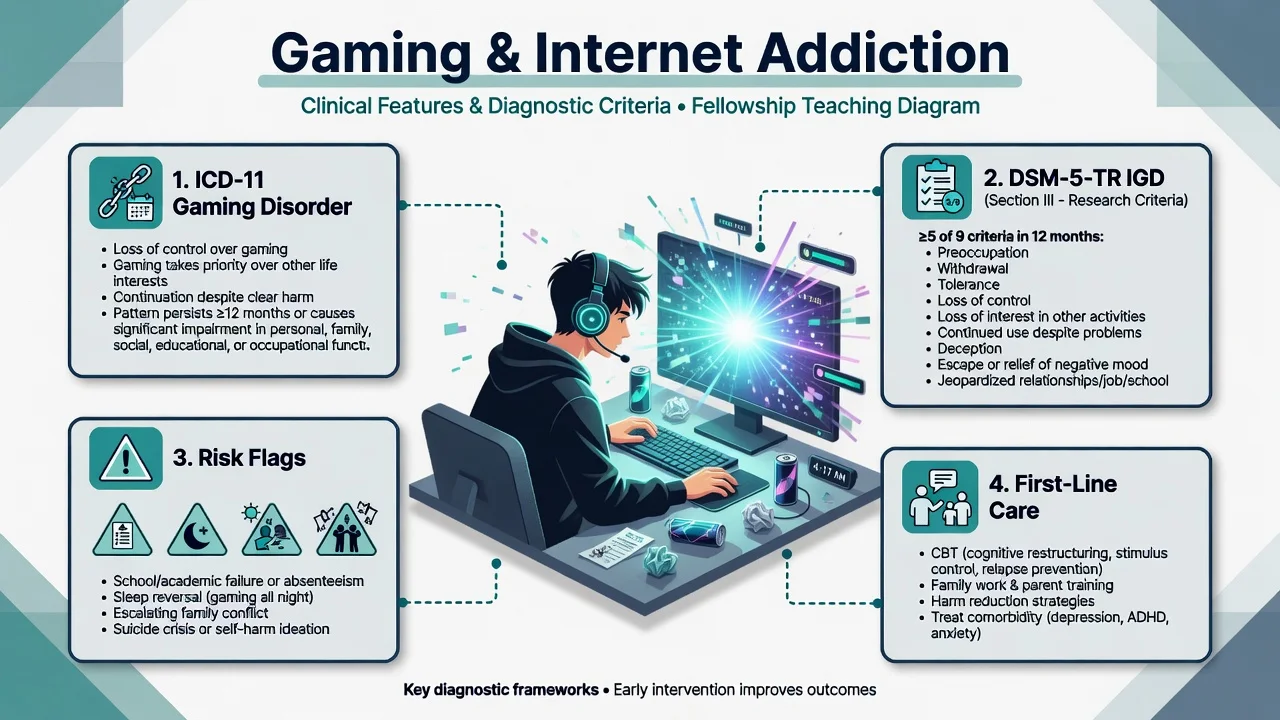
ICD-11 gaming disorder (GD) is included among disorders due to addictive behaviours. Core features are: (1) impaired control over gaming (onset, frequency, intensity, duration, termination, context); (2) increasing priority given to gaming such that it takes precedence over other life interests and daily activities; (3) continuation or escalation of gaming despite the occurrence of negative consequences. The pattern must be severe enough to result in significant impairment in personal, family, social, educational, occupational, or other important areas of functioning, and is usually evident over at least 12 months (a shorter duration may be justified if all diagnostic requirements are met and symptoms are severe).[1]
DSM-5-TR Internet gaming disorder (IGD) remains a condition for further study in Section III — not a fully official main-text diagnosis co-located with gambling disorder. Proposed criteria require persistent and recurrent use of the internet to engage in games, leading to clinically significant impairment or distress, with ≥5 of 9 symptoms over a 12-month period. The nine map to preoccupation, withdrawal symptoms when gaming is taken away (typically irritability/anxiety rather than autonomic SUD withdrawal), tolerance (need for increasing time), unsuccessful control attempts, loss of interest in other hobbies, continued excessive use despite psychosocial problems, deception regarding amount of gaming, use of games to escape or relieve negative mood, and jeopardised/lost relationship, job, or educational/career opportunity.[2]
Exam-critical contrast. Gambling disorder is fully listed in DSM-5-TR Substance-Related and Addictive Disorders. IGD is research-status only in DSM-5-TR, whereas ICD-11 treats gaming disorder as a clinical entity. Always state which manual you are using.[1][2]
Broader "internet addiction" is a contested umbrella covering social networking, streaming, shopping, and pornography use. Only gaming disorder has ICD-11 formal addictive-behaviour status; other domains require domain-specific formulation and should not be collapsed into one vague label without criteria.[1][3]
Classification continuum
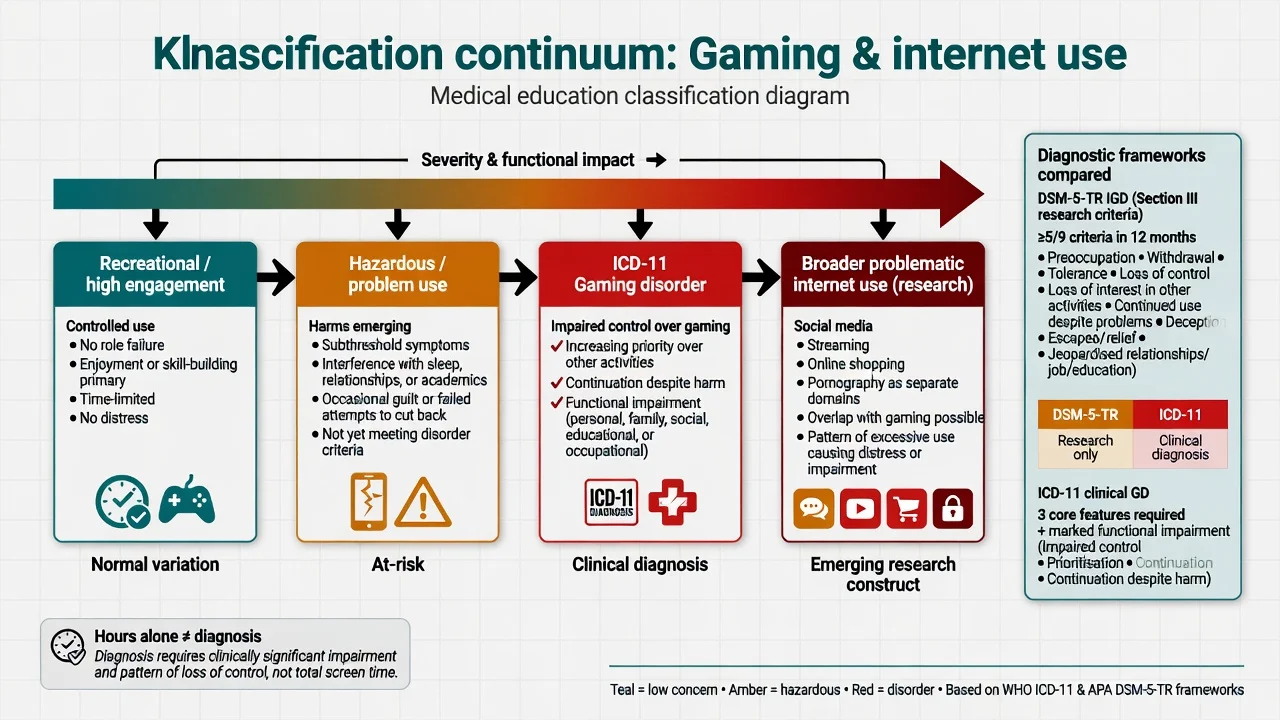
Recreational / high engagement
- High hours possible without role failure
- Can stop for school/work/sleep
- Skill or social goals primary
- Public-health messaging only
Hazardous / problem use
- Emerging sleep, grade, or relationship harm
- Subthreshold for full GD
- MI and brief family work useful
- Monitor high-risk game design
ICD-11 gaming disorder
- Impaired control + prioritisation + continuation despite harm
- Significant functional impairment
- Usually ≥12 months (shorter if severe)
- Needs structured CBT/family care
DSM-5-TR IGD (research)
- ≥5 of 9 criteria / 12 months
- Section III — not main-text disorder
- Useful research language
- State research status in exams
Predominantly online multiplayer and continuous-access products dominate clinical samples; loot-box and gacha mechanics create a bridge to gambling-like harm discussions.[1][11]
Epidemiology and risk
Headline epidemiology facts
Global systematic review and meta-analysis work places pooled gaming-disorder prevalence in a low single-digit percent band for many general-population estimates, with marked heterogeneity by instrument, threshold, region, and sample (higher in some male adolescent and East Asian clinical/community series).[7][8][12] Prevalence trend reviews show wide ranges historically because tools and cut-offs differed before ICD-11 and DSM-5 consensus language.[8][12]
Risk factors include male sex (historically), adolescence/young adulthood, ADHD and impulsivity, internalising disorders, social isolation, poor family functioning, and high-reinforcement game design (variable rewards, social obligation, ranking systems).[11][12] Longitudinal youth data associate pathological gaming patterns with worse grades and higher depression, anxiety, and social-phobia symptom trajectories over two years.[9]
Pathophysiology
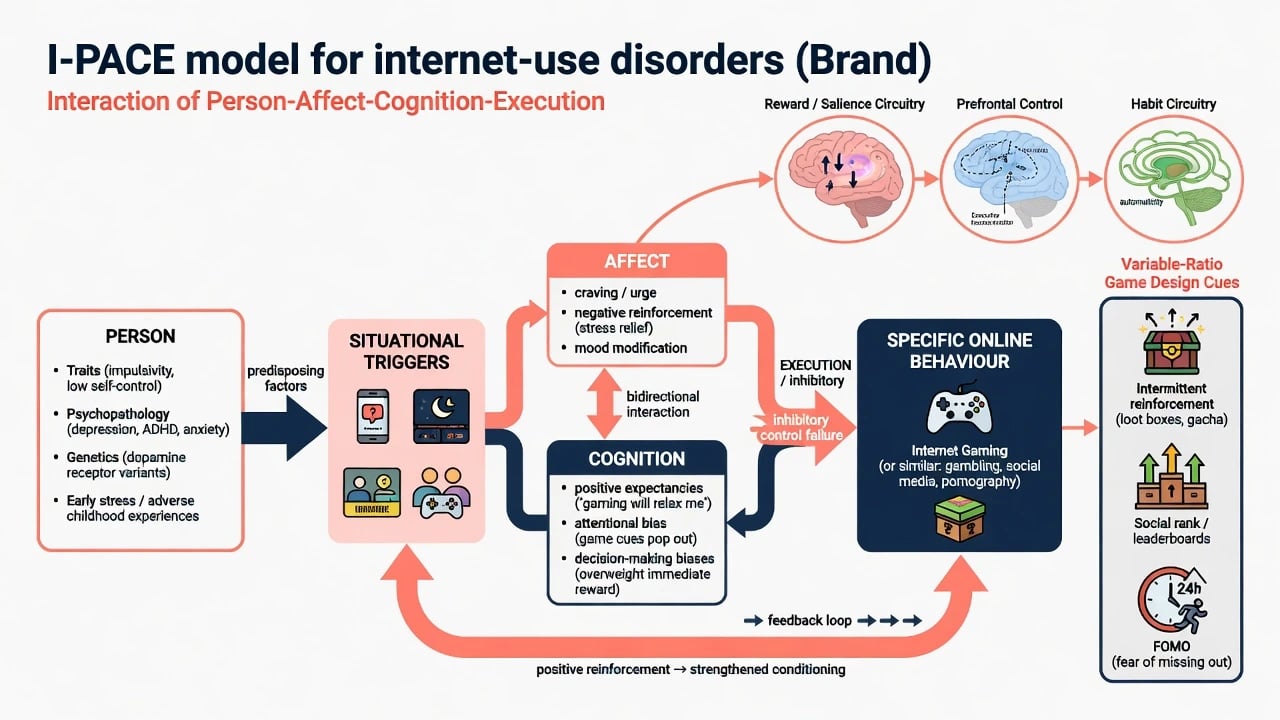
The I-PACE (Interaction of Person-Affect-Cognition-Execution) model is the viva-standard process model for specific internet-use disorders. Predisposing person factors (traits such as impulsivity, psychopathology, genetics, early stress) interact with situational triggers; affective responses (craving, stress relief, mood modification) and cognitive biases (positive expectancies, attentional bias to cues, decision-making biases favouring immediate reward) combine with reduced executive/inhibitory control to produce specific online behaviour. Conditioning strengthens the loop over time. The 2019 update generalises the process character across behavioural addictions beyond pure internet-use disorders.[3][4]
Neurobiologically, cortico-striatal reward and salience circuits, habit systems, and prefrontal control failure overlap other behavioural addictions. Game design exploits variable-ratio reinforcement, social rank, FOMO, and continuous multiplayer obligation — learning principles examiners expect named.[3][4]
Clinical presentation
Typical phenomenology: escalating session length and night play; irritability or restlessness when devices are limited; mental preoccupation with rank, raids, or patch cycles; neglect of hygiene, diet, and school; deception about hours; continued play after failed grades or relationship threats; use of games to escape dysphoria.[1][2][11]
MSE language. Describe appearance (sedentary, sleep-deprived), affect (irritable when limited, dysphoric offline), thought content (gaming-focused plans, hopelessness about school), insight (often partial — minimises hours), judgment, craving/urges, and risk (self-harm after conflict or failure, family violence, child safeguarding, financial microtransaction harm).[1][11]
Domain-specific internet patterns (social media, streaming, shopping, pornography) may co-occur or present alone — assess each domain rather than inventing a single non-specific "internet addiction" code without criteria.[3]
Differential diagnosis
High engagement hobby
- No loss of control or role collapse
- Maintains sleep/school/work
- Stops for obligations
- Hours may still be high
ADHD hyperfocus / ASD interest
- Neurodevelopmental history primary
- May co-occur with true GD
- Treat ADHD/ASD scaffolding
- Still apply impairment criteria
Depression escape
- Anhedonia across domains
- Gaming as avoidance
- Treat depression and reassess
- Safety risk elevated
Mania / substance
- Episodic sleep collapse, grandiosity
- Intoxicated multiplayer only
- Timeline discriminators
- Stabilise then reassess GD
Do not equate hours played with disorder. Do not moralise passionate gaming. Do not miss loot-box financial harm that belongs in a gambling-adjacent formulation.[1][2]
Clinical and bedside assessment
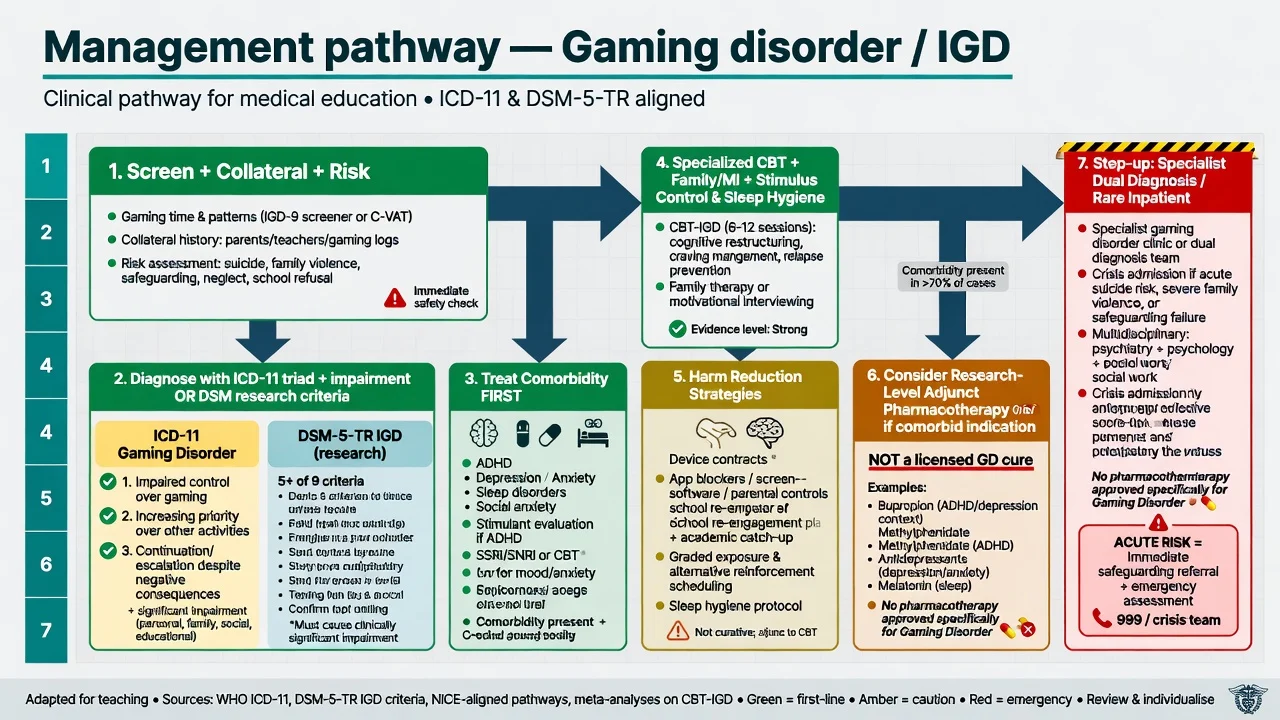
Structure history: preferred genres (MMORPG, FPS, battle royale, gacha); weekday vs weekend hours; night-time use; largest continuous session; school/work attendance and grades; family conflict and aggression when limited; microtransaction spend; other internet domains; mood, ADHD, ASD, psychosis screens; substances; sleep; online safety (grooming, bullying, illegal activity).[11][2]
Apply ICD-11 triad plus impairment and duration for clinical diagnosis. If using DSM-5 research language, require ≥5 of 9 with clinically significant impairment and state research status.[1][2] International consensus work supports structured assessment of the DSM-5 IGD approach for research and clinical communication.[2]
Scales (concepts). Short IGD scales (e.g. IGDS9-SF concepts) and broader internet-addiction inventories support case-finding and outcome tracking — they do not replace clinical criteria interviews. Collateral from parents/partners is essential in youth; gaming logs and router data are sometimes offered but are clinical aids, not covert policing.[2][11]
Risk assessment is mandatory after device confiscation crises, exam failures, and severe family conflict. Screen suicide, self-harm, domestic violence, and child protection issues.[11][1]
Investigations
There is no diagnostic blood test or routine imaging for GD/IGD. Consider basic bloods if severe self-neglect; urine drug screen when concurrent SUD is suspected; sleep evaluation when circadian collapse is extreme. Before any off-label or comorbidity-driven pharmacotherapy (e.g. bupropion), check blood pressure, seizure history, and mood polarity risks.[13][14]
Acute / crisis management
There is no autonomic detox protocol for pure gaming disorder. Stabilise suicide risk, family violence, and medical neglect first. Manage concurrent alcohol or sedative withdrawal if present. Involve child-protection and school pathways when minors are harmed or unsupervised online.[1][11]
Definitive management
Psychological therapies (first-line)
Meta-analytic synthesis finds cognitive-behavioural therapy reduces IGD symptoms and comorbid depression in the short term, with more uncertain effects on actual time spent gaming and limited long-term data — examiners should cite both benefit and evidence limits.[5] A multicentre randomised clinical trial of manualised STICA (short-term treatment for internet and computer game addiction) demonstrated efficacy versus wait-list control for internet and computer game addiction outcomes.[6] International CONSORT-focused reviews highlight variable trial quality and the need for rigorous protocols — know that the field is maturing, not that "nothing works."[10]
CBT package elements: gaming-related cognitive restructuring (beliefs about rank, obligation, escape); urge monitoring and surfing; stimulus control (device location, time windows, app blockers); behavioural activation offline; sleep scheduling; problem-solving; relapse planning around new releases. In adolescents, family therapy / parental contingency management and school liaison are core, not optional extras.[5][10][11]
Motivational interviewing suits ambivalent young people who reject the "addict" label. Prevention-oriented CBT cluster trials (e.g. PROTECT-style programmes) support school-based risk reduction for gaming and unspecified internet-use disorder trajectories.[15]
Harm reduction and social interventions
Negotiated device and time contracts; blue-light and sleep hygiene; removal of high-risk titles first if full abstinence is refused; banking/app controls for microtransactions; peer and offline activity substitution; educational catch-up plans. Policy and prevention reviews emphasise multi-level approaches (individual, family, school, industry design, regulation) rather than moral panic alone.[16]
Pharmacotherapy
No medication has a formal regulatory indication solely for gaming disorder. Psychosocial care remains primary.[10][1]
Bupropion (research/comorbidity context). Early work showed sustained-release bupropion reduced video-game craving and cue-related neural activity in internet video game addiction samples, and improved problematic online game play among patients with major depression treated with bupropion.[13][14] Exam framing: discuss as adjunctive, often when comorbid depression or smoking/ADHD-related indications exist; typical adult depression dosing frameworks (e.g. sustained-release bupropion titrated toward 150–300 mg daily oral under standard monitoring) apply to the depressive indication — not as a magic anti-gaming licence. Counsel seizure risk, avoid in eating-disorder/abrupt alcohol-benzo withdrawal contexts, monitor BP and mood switches. Do not present as first-line monotherapy for pure GD.[13][14]
Treat ADHD, anxiety, and depression with their own evidence-based agents and psychotherapies when comorbid; treating only "the games" while ignoring ADHD is a common failure mode.[11]
Treat comorbidity
ADHD, depression, anxiety, ASD traits, sleep disorders, and substance use are dense in clinical series — integrated care beats sequential ping-pong between CAMHS, addiction, and education services.[11][12]
Australian and New Zealand practice routes most cases through GP, headspace/youth mental health, school counselling, and addiction psychology rather than residential "game detox" industries. RANZCP-aligned care expects suicide risk competence, family-inclusive youth work, culturally safe assessment for Aboriginal and Torres Strait Islander and Māori young people, and honest counselling that ICD-11 GD is recognised while DSM-5-TR IGD remains research language in US-oriented texts.[1][7][16]
Subtypes and scenarios
Adolescent MMORPG school refusal — family conflict, night play, ADHD under-treatment. College dual cannabis + multiplayer — integrated dual formulation. Adult esports aspirant — occupational collapse despite "career" narrative. Loot-box spenders — gambling-adjacent harm. Non-gaming PIU — social media or streaming primacy with different reinforcers.[11][1]
Complications and pitfalls
Other pitfalls: moralising without CBT offer; confiscation-only plans; missing ADHD/depression; claiming a licensed anti-craving tablet for pure GD; conflating DSM research criteria with ICD-11 clinical diagnosis; ignoring loot boxes; pathologising girls' mobile gaming less than boys' PC gaming.[10][11][16]
Prognosis and disposition
Many community cases improve with maturation, structured limits, and treated comorbidity; clinical treatment-seekers are skewed toward higher severity and dual diagnosis.[9][12] Better outcomes associate with CBT engagement, family support, school reintegration, sleep restoration, and reduced access to highest-risk products. Disposition ladder: GP/youth primary mental health → specialist psychology → dual-diagnosis/addiction psychiatry → inpatient only for high suicide risk, severe self-neglect, or unmanageable dual diagnosis.[5][6][10] Relapse risk clusters around exams, holidays, and major game releases.
Special populations
Children and adolescents. Developmental framing; parental capacity; school; online safety; avoid pure punishment models; Paulus-level paediatric review evidence for high comorbidity and family context.[11] ADHD/ASD. Integrated neurodevelopmental care; special interest vs loss of control. Women and diverse gamers. Rising mobile/social patterns — do not use a male-PC stereotype. Cultural safety. East Asian clinical literature is historically denser; ANZ care must remain non-stereotyping and family-inclusive.[12][16]
Evidence and guidelines
Name at viva: Saunders 2017 delineation of gaming disorder; Petry 2014 international IGD assessment consensus; Brand I-PACE 2016 and 2019 update; Stevens 2021 global prevalence meta; Feng 2017 and Mihara/Higuchi 2017 epidemiology reviews; Gentile 2011 longitudinal youth study; Paulus 2018 child/adolescent review; Stevens 2019 CBT meta-analysis; Wölfling 2019 STICA RCT; King 2017 CONSORT treatment review; Lindenberg 2022 prevention RCT; Han 2010 and Kim 2012 bupropion studies; King 2018 policy and prevention review.[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16]
Exam pearls
GAMING
Self-test: ICD-11 triad and first-line care
References
- [1]Saunders JB, Hao W, Long J, King DL, Mann K, Fauth-Bühler M, et al. Gaming disorder: Its delineation as an important condition for diagnosis, management, and prevention J Behav Addict, 2017.PMID 28816494
- [2]Petry NM, Rehbein F, Gentile DA, Lemmens JS, Rumpf HJ, Mößle T, et al. An international consensus for assessing internet gaming disorder using the new DSM-5 approach Addiction, 2014.PMID 24456155
- [3]Brand M, Young KS, Laier C, Wölfling K, Potenza MN Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: An Interaction of Person-Affect-Cognition-Execution (I-PACE) model Neurosci Biobehav Rev, 2016.PMID 27590829
- [4]Brand M, Wegmann E, Stark R, Müller A, Wölfling K, Robbins TW, et al. The Interaction of Person-Affect-Cognition-Execution (I-PACE) model for addictive behaviors: Update, generalization to addictive behaviors beyond internet-use disorders, and specification of the process character of addictive behaviors Neurosci Biobehav Rev, 2019.PMID 31247240
- [5]Stevens MWR, King DL, Dorstyn D, Delfabbro PH Cognitive-behavioral therapy for Internet gaming disorder: A systematic review and meta-analysis Clin Psychol Psychother, 2019.PMID 30341981
- [6]Wölfling K, Müller KW, Dreier M, Ruckes C, Deuster O, Batra A, et al. Efficacy of Short-term Treatment of Internet and Computer Game Addiction: A Randomized Clinical Trial JAMA Psychiatry, 2019.PMID 31290948
- [7]Stevens MW, Dorstyn D, Delfabbro PH, King DL Global prevalence of gaming disorder: A systematic review and meta-analysis Aust N Z J Psychiatry, 2021.PMID 33028074
- [8]Feng W, Ramo DE, Chan SR, Bourgeois JA Internet gaming disorder: Trends in prevalence 1998-2016 Addict Behav, 2017.PMID 28662436
- [9]Gentile DA, Choo H, Liau A, Sim T, Li D, Fung D, Khoo A Pathological video game use among youths: a two-year longitudinal study Pediatrics, 2011.PMID 21242221
- [10]King DL, Delfabbro PH, Wu AMS, Doh YY, Kuss DJ, Pallesen S, et al. Treatment of Internet gaming disorder: An international systematic review and CONSORT evaluation Clin Psychol Rev, 2017.PMID 28458097
- [11]Paulus FW, Ohmann S, von Gontard A, Popow C Internet gaming disorder in children and adolescents: a systematic review Dev Med Child Neurol, 2018.PMID 29633243
- [12]Mihara S, Higuchi S Cross-sectional and longitudinal epidemiological studies of Internet gaming disorder: A systematic review of the literature Psychiatry Clin Neurosci, 2017.PMID 28436212
- [13]Han DH, Hwang JW, Renshaw PF Bupropion sustained release treatment decreases craving for video games and cue-induced brain activity in patients with Internet video game addiction Exp Clin Psychopharmacol, 2010.PMID 20695685
- [14]Kim SM, Han DH, Lee YS, Renshaw PF Bupropion in the treatment of problematic online game play in patients with major depressive disorder Exp Clin Psychopharmacol, 2012.PMID 21447539
- [15]Lindenberg K, Kindt S, Szász-Janocha C Effectiveness of Cognitive Behavioral Therapy-Based Intervention in Preventing Gaming Disorder and Unspecified Internet Use Disorder in Adolescents: A Cluster Randomized Clinical Trial JAMA Netw Open, 2022.PMID 35179587
- [16]King DL, Delfabbro PH, Doh YY, Wu AMS, Kuss DJ, Pallesen S, et al. Policy and Prevention Approaches for Disordered and Hazardous Gaming and Internet Use: an International Perspective Curr Addict Rep, 2018.PMID 28677089