Psych · Addiction psychiatry — hallucinogen-related disorders
Hallucinogen-related disorders
Also known as Hallucinogen use disorder · Psychedelic intoxication · LSD intoxication · Psilocybin adverse effects · Bad trip · Hallucinogen persisting perception disorder · HPPD · Classic psychedelics · Serotonergic hallucinogens
Fellowship-depth atlas on hallucinogen-related disorders — classic serotonergic psychedelics (LSD, psilocybin, mescaline, DMT), intoxication and bad-trip care, low dependence liability versus use disorder, HPPD, substance-induced psychosis, set/setting risk, and the clinical interface with psychedelic-assisted therapy research. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Hallucinogen-related disorders cover intoxication, use disorder, persisting perception phenomena, and substance-induced mental disorders linked to classic serotonergic psychedelics (LSD, psilocybin, mescaline, DMT/ayahuasca) and the clinical interface with related street agents. Fellowship work is to separate class pharmacology, acute safety, HPPD, dual formulation of psychosis, and the careful reading of psychedelic-assisted therapy trials without equating festival use to protocolised research care.[1][2]
In DSM-5-TR, relevant constructs include other hallucinogen intoxication, other hallucinogen use disorder, hallucinogen persisting perception disorder (HPPD), and other hallucinogen-induced disorders (psychotic, bipolar, depressive, anxiety, and related). Phencyclidine (PCP) and related arylcyclohexylamines are coded separately; MDMA is an entactogen with overlapping party contexts but a different primary toxidrome. ICD-11 frames acute intoxication and harmful pattern/dependence for hallucinogens where applicable. A positive urine screen neither times the intoxication nor diagnoses a use disorder.[2]
Classic psychedelics produce rapid tolerance with frequent dosing and cross-tolerance within the class, and they do not typically generate a life-threatening autonomic withdrawal syndrome analogous to alcohol or benzodiazepines. The high-yield clinical traps are bad trips, dangerous behaviour while impaired, HPPD, and mislabelled psychosis — not "detox seizures."[2][3]
Classification
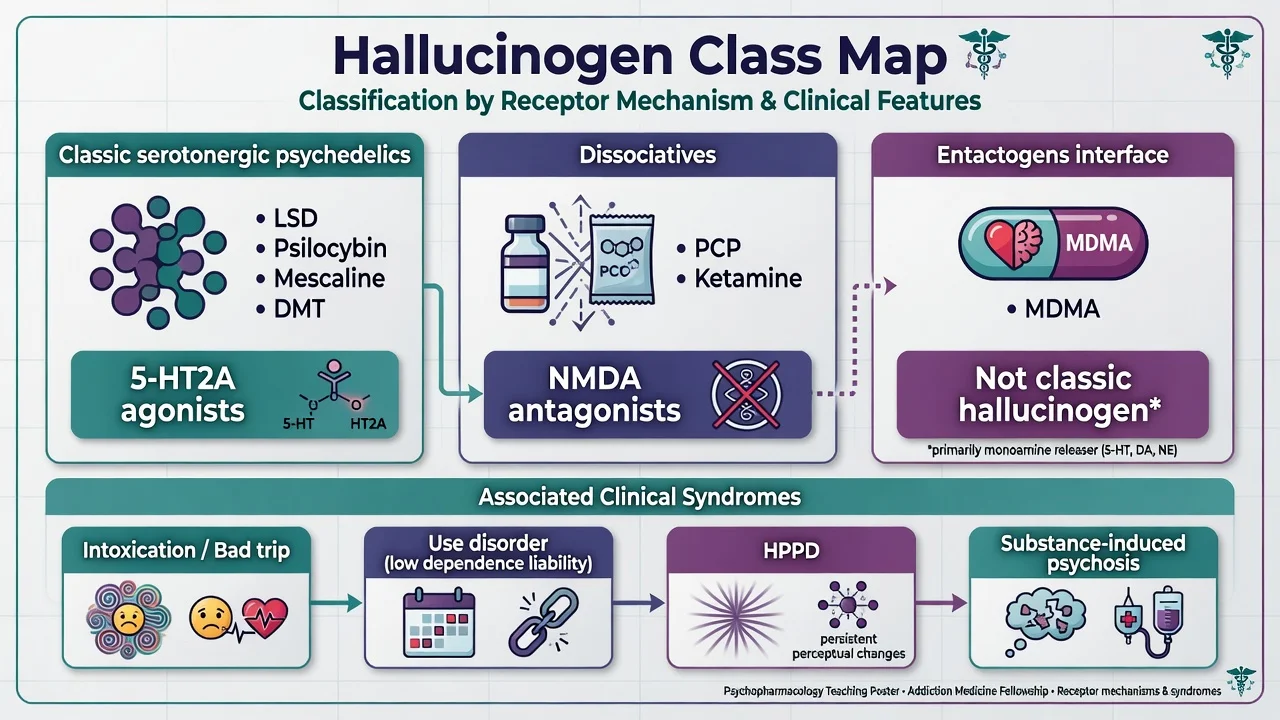
| Class | Examples | Primary mechanism (exam level) | Acute discriminators |
|---|---|---|---|
| Classic serotonergic psychedelics | LSD, psilocybin, mescaline, DMT/ayahuasca | 5-HT2A agonism | Perceptual distortion, ego dissolution, often partial insight; mild–moderate sympathetic activation |
| Dissociatives | PCP, ketamine, analogues | NMDA antagonism | Dissociation, nystagmus, analgesia, more medical risk at high dose |
| Entactogen interface | MDMA | Monoamine release/reuptake effects | Empathogenic affect; hyperthermia and hyponatraemia risk at festivals |
Use disorder for classic hallucinogens is less common than for opioids, stimulants or alcohol, reflecting intermittent use patterns and lower compulsive re-dosing for many users — but DSM-5-TR criteria still apply when control is lost, obligations are neglected, or use continues despite harm.[2][8]
Epidemiology and risk factors
Lifetime psychedelic use is not rare in population surveys, but daily compulsive use is uncommon relative to other drug classes. Multicriteria expert rankings place LSD and mushrooms among lower overall-harm substances compared with alcohol and heroin — a relative statement that must never be misread as zero risk.[8] Large US population analyses have not found lifetime psychedelic use to be independently associated with increased mental health problems at the population level; this does not exclude individual catastrophic reactions, HPPD, or substance-induced psychosis.[7]
Risk modifiers for adverse acute reactions include high dose, unknown purity/adulterants, anxious or unstable mindset, unsupervised or chaotic setting, youth, personal or family psychosis liability, and polysubstance use (alcohol, cannabis, stimulants).[1][5] Survey data show challenging ("bad trip") experiences are not rare in uncontrolled use; a minority report enduring psychological symptoms or seeking help, and emergency medical treatment after magic mushrooms in Global Drug Survey data is uncommon, with psychological symptoms (anxiety/panic, paranoia) dominating when it occurs.[5][12]
Pathophysiology
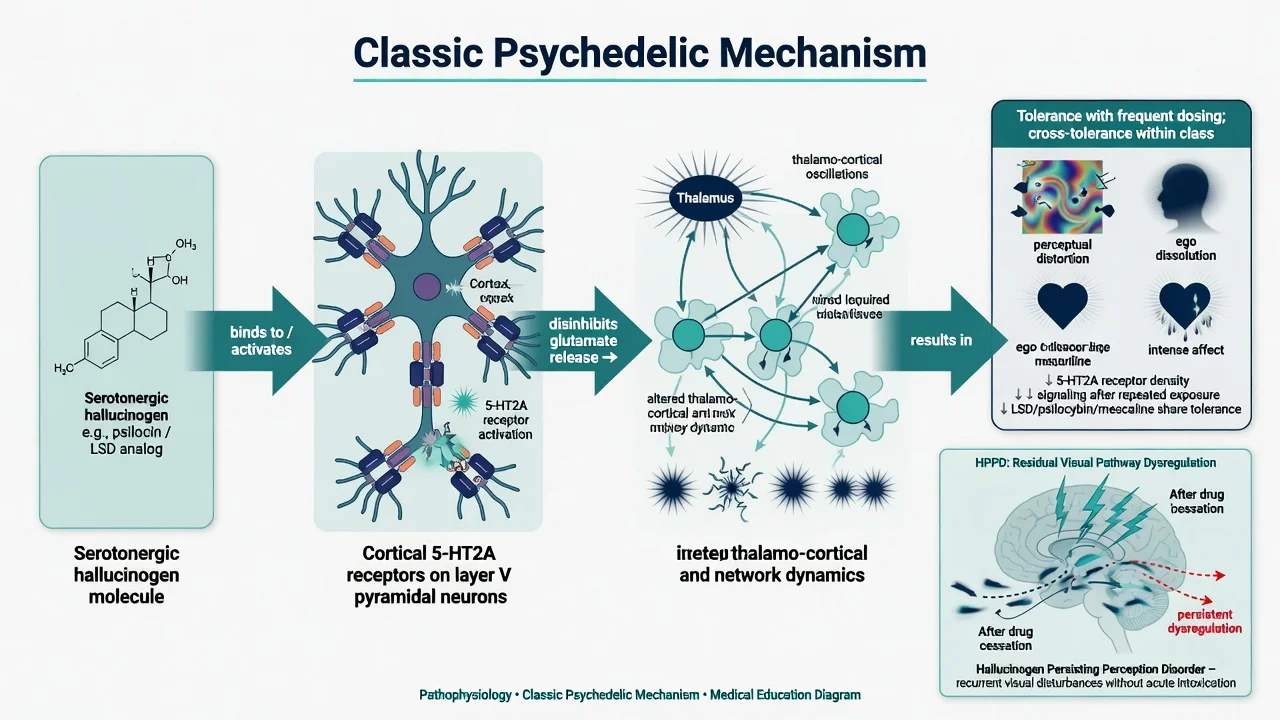
There is broad consensus that classic psychedelics act as agonists or partial agonists at 5-HT2A receptors, with particular importance for receptors on apical dendrites of neocortical layer V pyramidal cells. Downstream effects reorganise thalamo-cortical and large-scale network dynamics underlying perception, cognition, mood and self-boundaries.[2]
Tolerance to classic psychedelics develops quickly with frequent dosing; cross-tolerance occurs within the class and reverses after a period of abstinence. Dependence liability is relatively low compared with opioids or stimulants, consistent with intermittent rather than continuous reinforcement patterns for many users.[2]
HPPD hypotheses include residual disinhibition or dysregulation of visual pathways after serotonergic hallucinogen exposure; the mechanism is not fully settled. Clinically, distinguish transient benign flashbacks from the DSM construct of re-experienced perceptual symptoms with clinically significant distress or impairment after cessation.[3][4]
Dissociatives (PCP/ketamine) act primarily via NMDA receptor antagonism and produce a different toxidrome — do not conflate street "hallucinogen" labels with mechanism.[2]
Clinical presentation
Intoxication and the bad trip
Typical classic psychedelic intoxication: intensified colours and patterns, geometric visual phenomena, time distortion, synaesthesia-like experiences, labile or intense affect (from bliss to terror), mystical-type or ego-dissolution experiences, mydriasis, and mild-to-moderate tachycardia or hypertension. Insight is often partially retained — a useful discriminator from frank delirium.[2][6]
A "bad trip" is acute dysphoric intoxication: panic, paranoia, catastrophic interpretations of perceptual change, agitation, and risk of dangerous behaviour (running into traffic, heights, self-harm). Duration roughly tracks the agent (LSD longer than typical oral psilocybin; smoked/vapourised DMT brief; ayahuasca prolonged with prominent GI phase).[1][5]
Pooled experimental data in screened, prepared volunteers show dose-related profound subjective effects with low rates of severe long-term harm under research conditions — the contrast with unsupervised high-dose use is itself an examinable point.[6]
Hallucinogen use disorder
Look for impaired control, social impairment, risky use, and pharmacological criteria applied to hallucinogens. Physiological withdrawal is usually not the clinical centrepiece; craving, continued use despite harm, and escalating dose after tolerance are more relevant when present.[2]
HPPD
HPPD features re-experiencing of perceptual phenomena (visual snow, trailing, afterimages, geometric patterns, halos) after the acute drug effect has ended, with distress or functional impairment. It appears uncommon but genuine and can persist for months or years in some cases.[3][4]
Substance-induced psychotic disorder
Psychotic symptoms temporally linked to intoxication or shortly thereafter require dual formulation with primary psychotic disorder if they persist after a reasonable washout and collateral review. Youth and family history raise the stakes for longitudinal follow-up.[5][7]
Differential diagnosis
| Presentation | Favours classic psychedelic state | Favours alternative | Discriminators |
|---|---|---|---|
| Perceptual change + panic | Known recent use; partial insight; expected duration | Primary panic disorder alone | Timeline, mydriasis, companions' history |
| Psychosis after party drug | Clear temporal link; may settle | First-episode schizophrenia/bipolar | Family history, washout course, collateral |
| Persistent visual phenomena | After cessation; HPPD criteria | Migraine aura, epilepsy, Charles Bonnet, primary psychosis | Duration, insight, visual-only vs multimodal, eye/neuro work-up thresholds |
| Severe dissociation + nystagmus | PCP/ketamine class | Classic 5-HT2A psychedelic | Toxidrome features, not street name |
| Hyperthermia / hyponatraemia | MDMA or adulterant | Pure LSD/psilocybin less typical | Festival context, sodium, temperature |
| Agitation + clonus + hyperreflexia | Serotonin toxicity (esp. MAOI + tryptamine) | Simple bad trip | Drug list, neuromuscular findings |
Can't-miss organics: hypoglycaemia, head injury, encephalitis, seizure, hyponatraemia (especially MDMA co-use), serotonin toxicity, and high-toxicity adulterants (e.g. NBOMe sold as LSD).[1][12]
Clinical and bedside assessment
- ABC and vitals first — temperature, HR, BP, SpO2, glucose; medical bay if toxicity or collapse.
- Substance timeline — claimed agent vs likely substance, dose if known, last use, expected remaining duration, polysubstance, prior bad trips/HPPD/psychosis.
- MSE with examples — not "hallucinating"; e.g. "sees trailing geometric lattices on walls; believes companions can read his thoughts; oriented; partially reassured by staff presence."
- Risk — accidental injury, suicide/self-harm under terror, absconding, sexual vulnerability, driving, child protection.
- Capacity and legal status — jurisdiction-specific least-restrictive principles; do not invent foreign section numbers.
- Collateral — festival friends, ambulance, family, prior MH and AOD history.
- Dual diagnosis screen — emerging psychosis, bipolar, PTSD, anxiety, depression, other SUD.
Investigations
| Domain | Tests / actions | Why |
|---|---|---|
| Bedside | Vitals, glucose, ECG if chest pain/severe tachycardia or before antipsychotics when used | Exclude medical toxicity; baseline if sedating |
| Bloods | U&E (especially if MDMA/collapse), CK if prolonged agitation/restraint, pregnancy test when relevant | Hyponatraemia, rhabdomyolysis, disposition |
| Toxicology | Urine/serum screen | Supportive only — many novel agents missed |
| Imaging / special | CT/MRI, EEG, ophthalmology if red flags | Focal neurology, atypical persistent visual phenomena |
| Infectious | As indicated by risk history | Not routine for pure short-lived intoxication |
Management — resuscitation and acute care
Acute priorities:
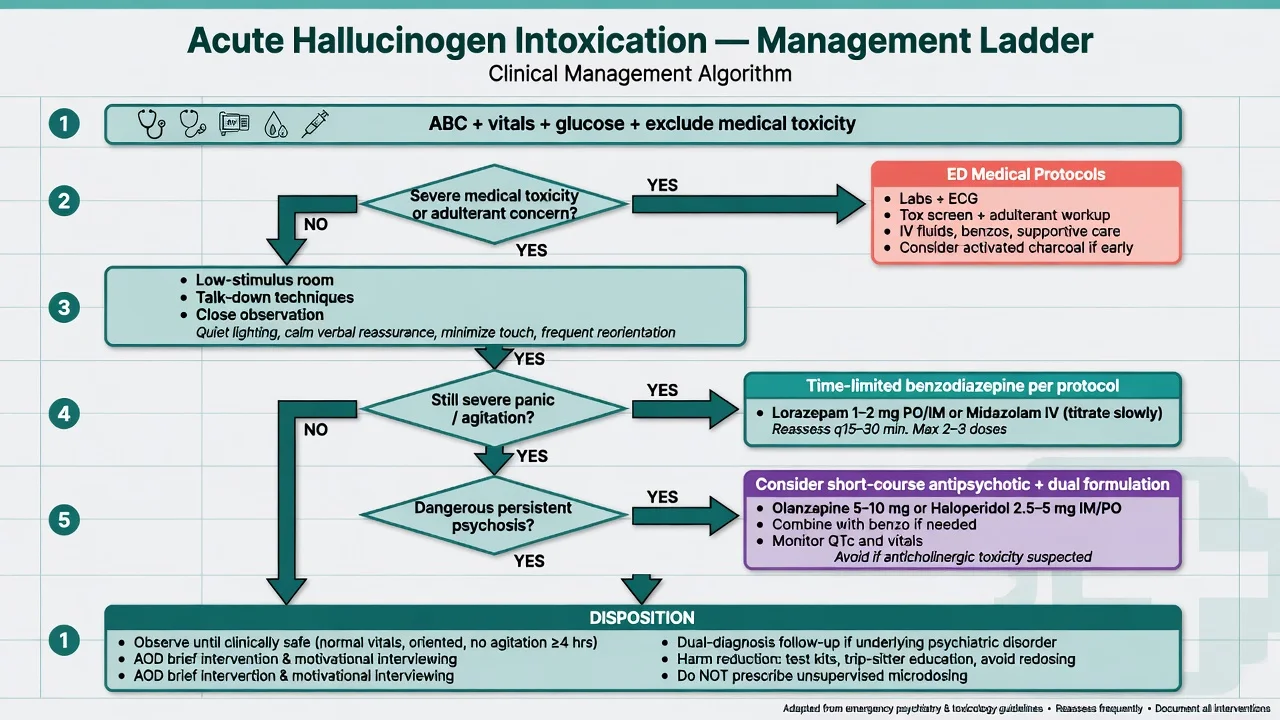
- Low-stimulus environment and talk-down — calm voice, simple orientation cues, reduced sensory load, continuous observation until effects decline. Research safety literature codifies preparation, support and interpersonal presence as core risk reducers; adapt the spirit to ED/acute psychiatry without claiming research conditions.[1][6]
- Hydration and basic comfort — avoid overhydration if MDMA/hyponatraemia is possible; follow ED fluid protocols.
- Benzodiazepines for severe anxiety/agitation when non-pharmacological measures fail — time-limited, local protocol (example teaching range: oral diazepam 5–10 mg or lorazepam 1–2 mg orally when safe to take, with lower starting doses in frailty/respiratory risk; parenteral only per local RT pathway with airway monitoring). Do not stack sedatives blindly with alcohol co-intoxication.[1]
- Antipsychotics — reserved for dangerous or persistent psychosis/severe agitation not settling with support and benzodiazepines; time-limit and reassess after the intoxication window (example teaching: olanzapine 5–10 mg orally if appropriate and protocol-compatible). Not every visual distortion needs an antipsychotic.[1][5]
- Minimise restraint — physical restraint escalates injury and distress; use least restrictive means.
- Serotonin toxicity pathway if MAOI-containing brew plus serotonergic co-ingestants — medical toxicology management, not talk-down alone.[2]
Management — definitive care, HPPD and the research interface
Hallucinogen use disorder
No approved substitution or anti-craving standard analogous to opioid agonist treatment exists for classic hallucinogens. Care is psychosocial: motivational interviewing, CBT-informed skills, contingency approaches where feasible, dual-diagnosis treatment of co-occurring disorders, and harm-reduction advice (dose uncertainty, adulterants, set/setting, avoiding driving, avoiding use with psychosis risk).[2][8]
HPPD
Psychoeducation, cessation of further hallucinogens and often cannabis, treatment of comorbid anxiety/depression, and ophthalmology/neurology review when the differential is open. Specific pharmacotherapy evidence is limited and largely case-based; do not invent a mandatory first-line drug algorithm beyond treating comorbidities and avoiding re-exposure.[3][4]
Psychedelic-assisted therapy — exam-level precision
Controlled trials report signals for psilocybin with psychological support in treatment-resistant depression (e.g. single 25 mg oral psilocybin dose superior to 1 mg control at 3 weeks on primary depression outcome in COMPASS Phase 2b), comparative work versus escitalopram, and reductions in heavy drinking days with psilocybin-assisted psychotherapy in alcohol use disorder.[9][10][11]
Exam traps:
- Trial participants are screened, prepared, supported and integrated — not equivalent to unsupervised microdosing or festival use.[1][6]
- Efficacy signals do not create a routine prescribing right for recreational products in ANZ standard care.
- Primary outcome nuances matter (e.g. Carhart-Harris 2021 did not show a significant difference on the primary QIDS endpoint versus escitalopram in the selected sample — secondary outcomes and context still discussed).[11]
- Never advise patients to self-treat depression or AUD with illicit psychedelics based on headlines.
| Approach | Role | Exam precision |
|---|---|---|
| Talk-down / observation | First-line acute intoxication | Core of Johnson-style safety ethos in clinical form[1] |
| Benzodiazepines | Severe panic/agitation | Time-limited; local RT protocol overrides examples |
| Antipsychotics | Dangerous persistent psychosis | Not routine for all perceptual change |
| MI / CBT / dual care | Use disorder and comorbidity | No OAT-equivalent standard |
| HPPD care | Education, cessation, comorbidity Rx | Limited drug-specific RCT base[3][4] |
| PAT research | Protocolised experimental care | Cite Goodwin/Bogenschutz/Carhart-Harris accurately; not DIY scripts[9][10][11] |
Specific subtypes and scenarios
Festival bad trip with partial insight. Quiet space, talk-down, observe through peak; benzo if severe panic; discharge only when MSE safe and supports available.[1][5]
Youth first-episode psychosis after LSD/psilocybin. Dual formulation; early intervention pathway; family work; organic thresholds if atypical.[5][7]
HPPD months after last use. Validate; exclude alternative visual diagnoses; stop further psychedelics/cannabis; treat anxiety; specialist follow-up.[3][4]
Ayahuasca + SSRI/MAOI concern. Serotonin toxicity vigilance; medical management if present.[2]
"Microdosing script" request after TRD headlines. Explain trial context, risks, legal status, and evidence-based depression care; do not collude with unregulated supply.[9][11]
Severe nystagmus and dissociation sold as "acid." Treat as dissociative toxidrome until proven otherwise.[2]
Complications and pitfalls
- Medical: injury while impaired, adulterant toxicity (NBOMe), serotonin toxicity, MDMA co-use hyperthermia/hyponatraemia, rare prolonged psychiatric sequelae.
- Psychiatric: bad trip trauma, HPPD, substance-induced psychosis, exacerbation of underlying mood/anxiety disorders, iatrogenic over-sedation.
- Pitfalls: assuming alcohol-like withdrawal seizures; lifelong schizophrenia label after a single linked episode; equating population non-association with zero individual risk; equating PAT trial efficacy with recreational prescribing; treating every visual change with depot antipsychotics; missing adulterants by trusting the street name.
Prognosis and disposition
Most pure classic intoxications resolve within hours with supportive care if medical complications are absent. Many people later reappraise challenging experiences as meaningful — that retrospective narrative does not reduce acute duty of care for safety.[5][6] HPPD may persist and impair function in a minority.[3] Disposition ladder: medical clearance and safe MSE → brief AOD intervention → dual-diagnosis follow-up if psychosis/mood risk → crisis plan and written advice against driving and further use while residual effects remain.
Special populations
Youth. Higher vulnerability to adverse psychological reactions and diagnostic ambiguity with emerging psychosis; family engagement is essential.[5][7]
Personal or family history of psychosis or bipolar disorder. Relative contraindication to unsupervised use and to research enrolment; counsel high individual risk even if population averages look reassuring.[1][7]
Pregnancy. Avoid; no established fetal safety for recreational psychedelics; obstetric liaison if exposure already occurred.[1][2]
Indigenous and ceremonial contexts. Cultural competence without romanticising risk or pathologising all traditional use; still assess capacity, consent and medical risk.[1][2]
Forensic / custody. Document intoxication stage, capacity, injury risk and observation needs during residual perceptual disturbance.[1]
Evidence, guidelines and regional differences
| Source | High-yield takeaway |
|---|---|
| Nichols 2016 | 5-HT2A mechanism and class pharmacology reference[2] |
| Johnson/Richards/Griffiths 2008 | Human research safety: preparation, set, setting, support[1] |
| Halpern and Pope 2003; Martinotti 2018 | HPPD clinical reality and limited evidence base for treatment[3][4] |
| Carbonaro 2016; Kopra 2022 | Challenging experiences in uncontrolled use; rare EMT after mushrooms with psych symptoms dominant[5][12] |
| Studerus 2011 | Acceptable risk profile in screened experimental volunteers under monitoring[6] |
| Krebs 2013; Nutt 2010 | Population mental-health non-association; relative harm ranking context[7][8] |
| Goodwin 2022; Bogenschutz 2022; Carhart-Harris 2021 | PAT research interface — TRD, AUD, vs escitalopram nuances[9][10][11] |
ANZ: Recreational psychedelic presentations appear in ED and acute psychiatry, often festival- or party-linked; there is no routine licensed pathway for recreational psilocybin prescribing as standard depression care. RANZCP dual-diagnosis and addiction competence frames apply. UK: NICE dual-diagnosis principles and evolving research landscape; BAP-style psychopharmacology literacy expected for trial claims. US: Active clinical trial ecosystem and FDA research interest; still distinguish protocolised PAT from illicit use. Quote the jurisdiction you are working in.[1][9]
Exam pearls
- 5-HT2A for classic psychedelics; NMDA for dissociatives — do not conflate classes.[2]
- No classic life-threatening withdrawal for LSD/psilocybin — bad trip, injury risk and HPPD dominate.[2][3]
- Talk-down first; benzodiazepines for severe agitation; antipsychotics not automatic.[1]
- HPPD = post-cessation perceptual re-experiencing with distress/impairment — not every afterimage.[3][4]
- Population data can look reassuring and individuals can still develop psychosis or HPPD — hold both truths.[7]
- Trial ≠ DIY: Goodwin 25 mg psilocybin signal and Bogenschutz AUD results do not authorise unsupervised microdosing scripts.[9][10]
- Carhart-Harris vs escitalopram: know the primary endpoint nuance, not just media summary.[11]
- Adulterated "LSD" can be high-toxicity — treat toxidrome, not brand.[1][12]
- Dual formulation for post-use psychosis; timeline beats day-one lifelong label.[5]
- Relative harm ranking low does not equal zero individual risk.[8]
References
- [1]Johnson MW, Richards WA, Griffiths RR Human hallucinogen research: guidelines for safety J Psychopharmacol, 2008.PMID 18593734
- [2]Nichols DE Psychedelics Pharmacol Rev, 2016.PMID 26841800
- [3]Halpern JH, Pope HG Jr Hallucinogen persisting perception disorder: what do we know after 50 years? Drug Alcohol Depend, 2003.PMID 12609692
- [4]Martinotti G, Santacroce R, Pettorruso M, et al. Hallucinogen Persisting Perception Disorder: Etiology, Clinical Features, and Therapeutic Perspectives Brain Sci, 2018.PMID 29547576
- [5]Carbonaro TM, Bradstreet MP, Barrett FS, et al. Survey study of challenging experiences after ingesting psilocybin mushrooms: Acute and enduring positive and negative consequences J Psychopharmacol, 2016.PMID 27578767
- [6]Studerus E, Kometer M, Hasler F, Vollenweider FX Acute, subacute and long-term subjective effects of psilocybin in healthy humans: a pooled analysis of experimental studies J Psychopharmacol, 2011.PMID 20855349
- [7]Krebs TS, Johansen PØ Psychedelics and mental health: a population study PLoS One, 2013.PMID 23976938
- [8]Nutt DJ, King LA, Phillips LD Drug harms in the UK: a multicriteria decision analysis Lancet, 2010.PMID 21036393
- [9]Goodwin GM, Aaronson ST, Alvarez O, et al. Single-Dose Psilocybin for a Treatment-Resistant Episode of Major Depression N Engl J Med, 2022.PMID 36322843
- [10]Bogenschutz MP, Ross S, Bhatt S, et al. Percentage of Heavy Drinking Days Following Psilocybin-Assisted Psychotherapy vs Placebo in the Treatment of Adult Patients With Alcohol Use Disorder: A Randomized Clinical Trial JAMA Psychiatry, 2022.PMID 36001306
- [11]Carhart-Harris R, Giribaldi B, Watts R, et al. Trial of Psilocybin versus Escitalopram for Depression N Engl J Med, 2021.PMID 33852780
- [12]Kopra EI, Ferris JA, Winstock AR, et al. Adverse experiences resulting in emergency medical treatment seeking following the use of magic mushrooms J Psychopharmacol, 2022.PMID 35388724