Psych · Addiction psychiatry — public health and systems
Harm reduction and public health approaches
Also known as Harm minimisation · Needle and syringe programmes · Needle exchange · Opioid substitution treatment public health · Supervised consumption sites · Supervised injecting facilities · Drug consumption rooms · Take-home naloxone · Overdose prevention · Addiction stigma
Exam-exhaustive fellowship reference on harm reduction and public-health approaches to drug use — principles and ethics; needle-syringe programmes; opioid agonist treatment as population intervention; supervised consumption; take-home naloxone; stigma; combined coverage; regional policy deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Harm reduction sits at the centre of modern addiction psychiatry viva and MEQ answers. Examiners test whether you can (1) define the approach without moral theatre, (2) name the four pillar interventions with landmark evidence, and (3) design a systems plan for a patient who is still using. Abstinence may be a legitimate personal goal; it is never a legitimate gate for sterile equipment, naloxone, or emergency care.[1][17][18]
Overview and definition
Harm reduction (also called harm minimisation in some ANZ policy language) is a set of pragmatic strategies and ideas aimed at reducing the adverse health, social, and economic consequences of psychoactive drug use for individuals, families, and communities — without requiring cessation as a precondition of receiving help.[1][2] It is one arm of a classic comprehensive drug strategy triad: supply reduction, demand reduction, and harm reduction.
Hawk and colleagues articulate healthcare-applicable principles that map cleanly onto CASC and viva ethics questions: humanism, pragmatism, individualism, autonomy, incrementalism, and accountability without termination (do not eject people from care for continued use).[1] Marlatt and Witkiewitz locate harm reduction as both a public-health policy frame and a clinical intervention research tradition spanning alcohol, injecting drug use, and other risk behaviours.[2]
Related but distinct concepts. Decriminalisation and legalisation are criminal-law reforms. “Safer supply” and prescribed diacetylmorphine are pharmaceutical risk-management strategies for selected populations. Harm reduction is the broader clinical and public-health posture that can exist under many legal regimes.[2][18]
Classification and intervention map
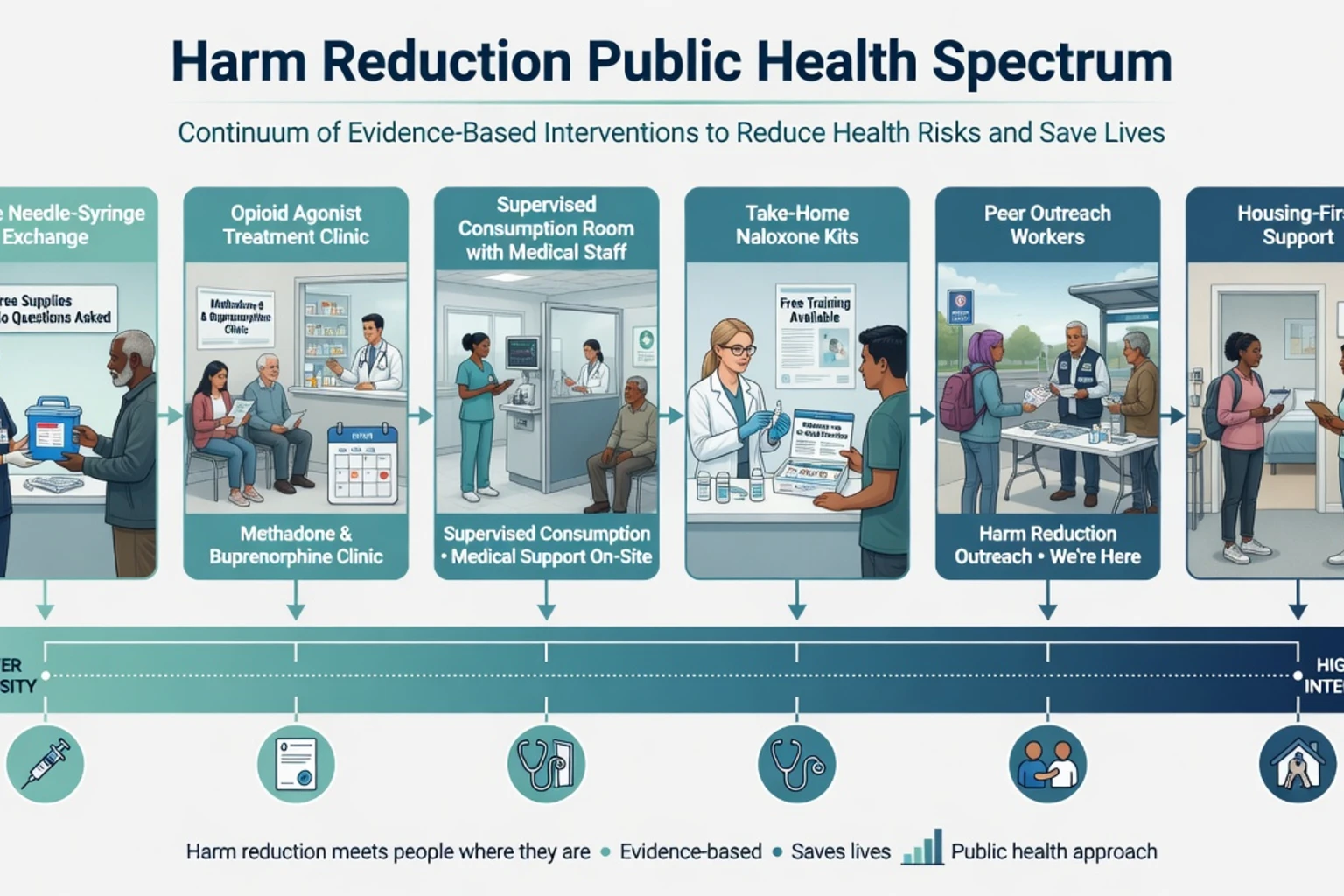
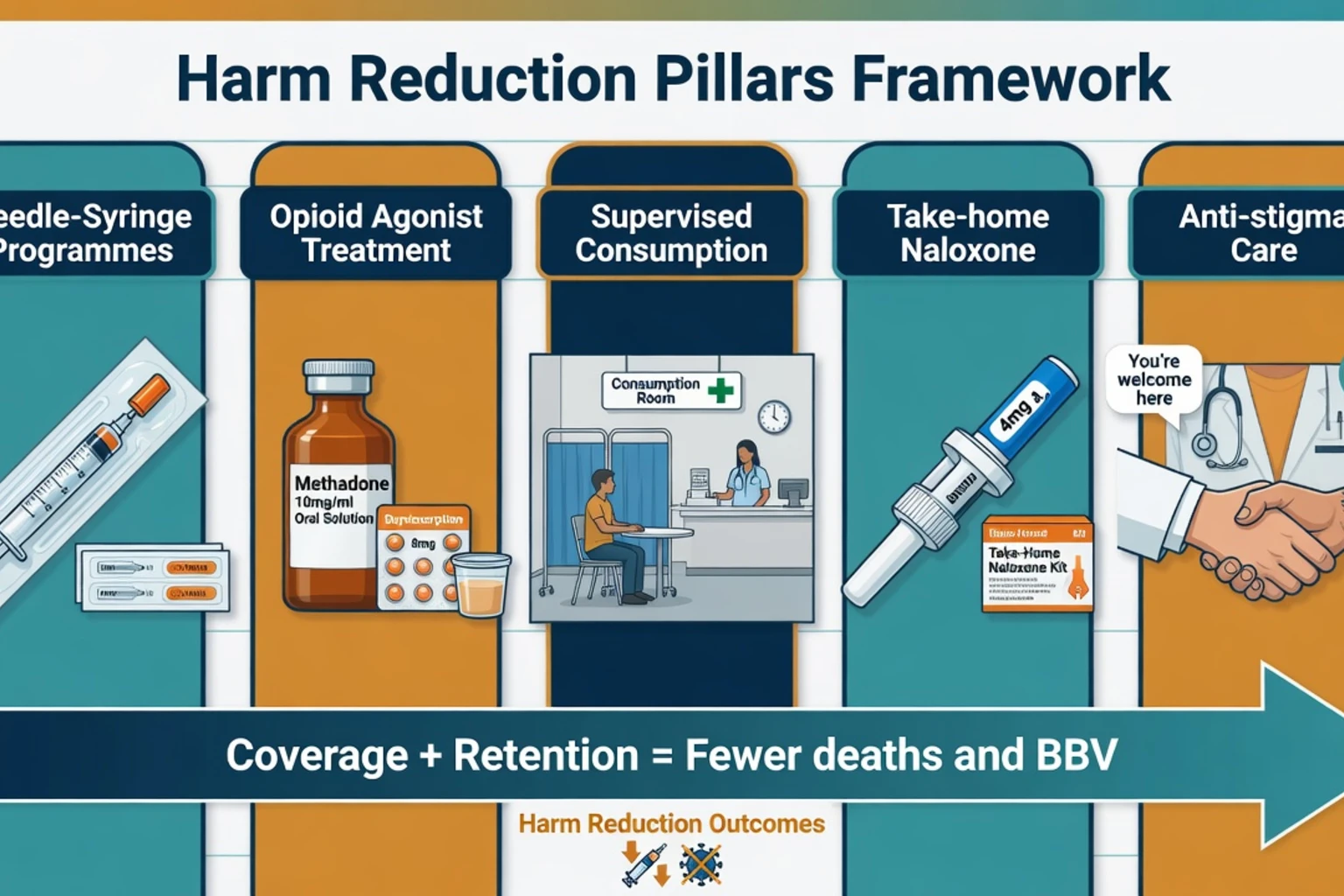
Needle-syringe programmes (NSP)
- Sterile needles, syringes, and ancillary equipment
- Safe disposal and return
- Low-threshold, often anonymous access
- Education, BBV testing, referral bridges
Opioid agonist treatment (OAT/OST)
- Methadone or buprenorphine maintenance
- Reduces illicit use, injecting, mortality
- Public-health and individual clinical dual role
- Retention is the key process outcome
Supervised consumption (SCS/SIF/DCR)
- On-site supervised use with overdose response
- Reduces public injecting and discarded equipment
- Linkage to treatment and social care
- Jurisdiction-specific legality
Naloxone and overdose response
- Take-home naloxone (THN) kits
- Peer/family training
- ED and post-release distribution
- Complements, does not replace, MOUD
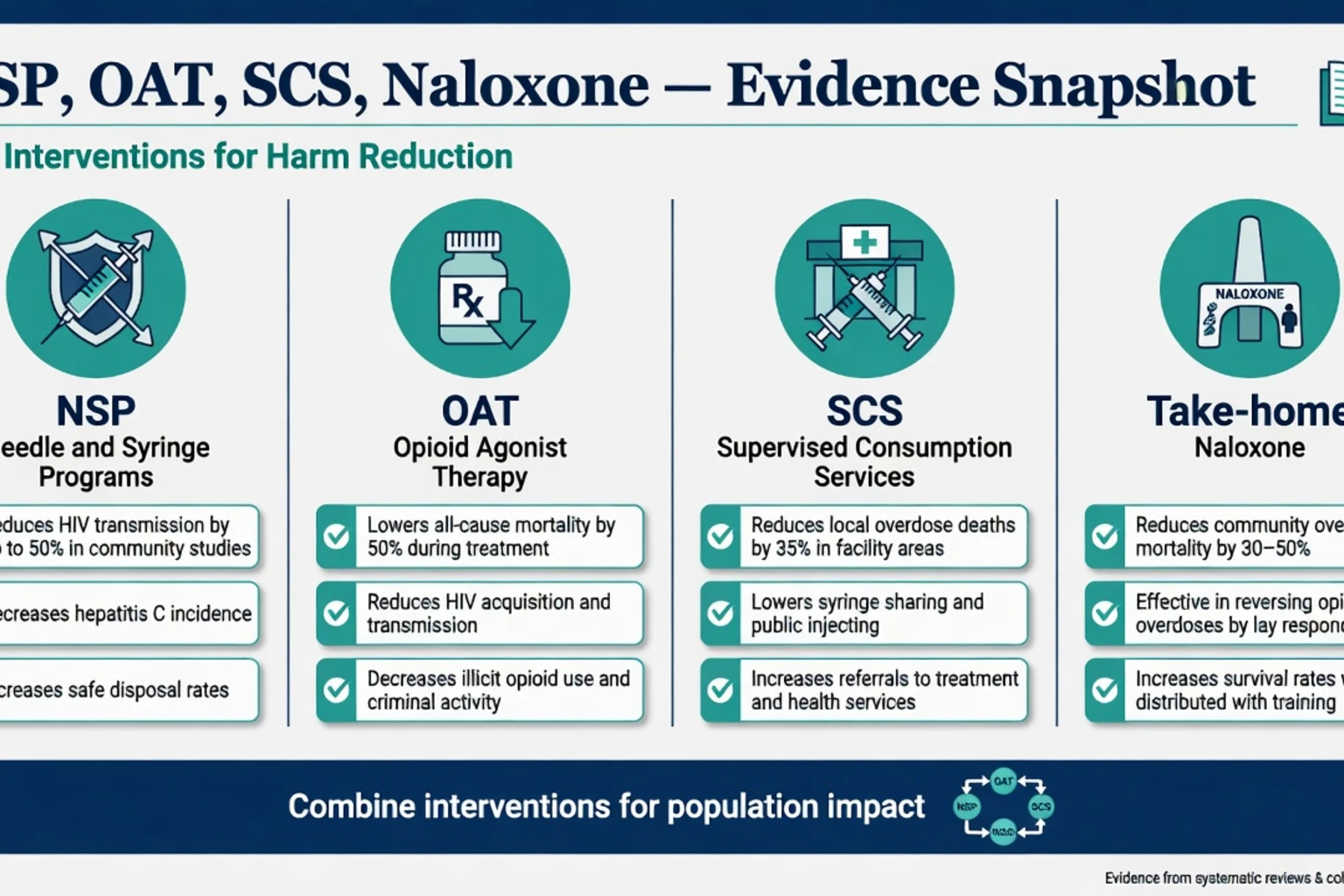
These pillars are complementary. High-coverage NSP plus OAT is more powerful for blood-borne virus control than either alone; naloxone and supervised consumption target acute overdose mortality; stigma reduction determines whether people will actually use any of them.[3][10][11][15][17]
Epidemiology and risk
Population framing facts for viva
Global patterns of opioid use and dependence produce substantial disability, overdose death, and infection risk; illicit fentanyl contamination amplifies overdose lethality in affected regions.[18] All-cause mortality falls during opioid substitution/agonist treatment and rises after cessation — the single most important systems message when a patient or family demands “detox only.”[9] High-risk windows include the days and weeks after prison release, after detoxification without maintenance, after hospital discharge without OAT restart, and during periods of solitary use with poly-sedative co-use.[15][18]
Mechanisms — how interventions interrupt harm
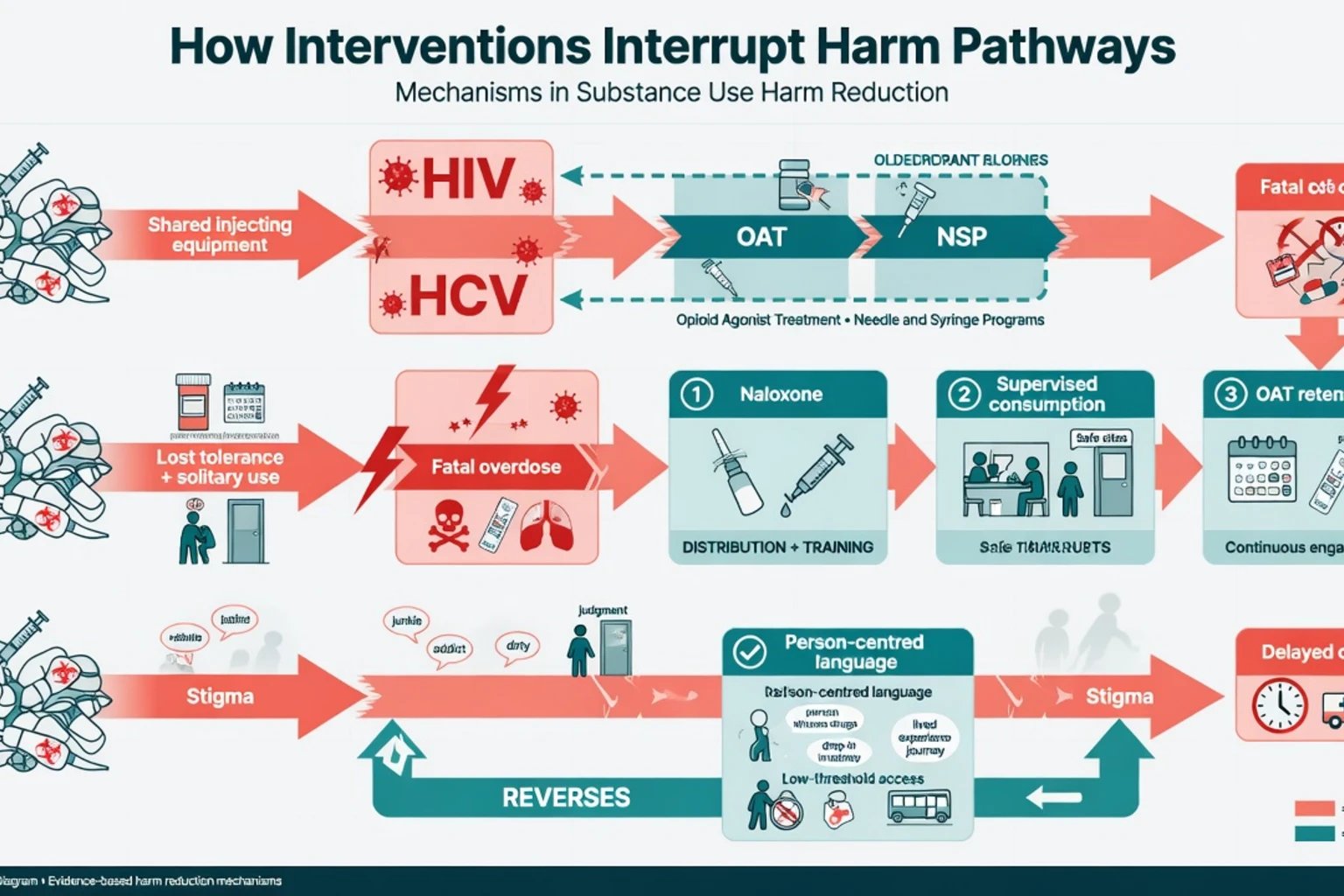
Blood-borne viruses. HIV and HCV transmit efficiently through shared injecting equipment. Providing sterile equipment reduces receptive syringe sharing; early programme evaluations in New York City syringe-exchange sites documented lower HIV incidence among participants compared with non-participants, and subsequent international reviews and meta-analyses support NSP as an HIV prevention intervention among people who inject drugs.[3][4][5][6]
Overdose. µ-Opioid agonists suppress brainstem respiratory drive. Naloxone competitively antagonises µ-receptors and restores ventilation when given in time. Take-home naloxone programmes extend this reverse pharmacology into the community, where most overdoses occur.[15] OAT reduces illicit opioid use and overdose risk through pharmacological stabilisation; supervised consumption places medical response at the point of use.[9][13][14]
Risk environment. Individual behaviour is shaped by housing, policing, drug market toxicity, and service accessibility. Low-threshold services change the environment, not only the person.[2][18]
Stigma. Labeling, status loss, and discrimination delay care, worsen pain management, and increase mortality risk. Stigma is a modifiable clinical and systems target, not a soft “culture” side note.[17]
Clinical presentation and bedside assessment
Patients who need harm reduction rarely present saying “I want a public-health intervention.” They present with abscesses, overdose, housing crisis, psychosis, pregnancy, child-protection contact, or criminal-justice involvement. The fellowship skill is to offer concurrent risk reduction and treatment rather than sequential “stop using first.”[1][18]
History structure (non-stigmatising). Substances, routes, sharing practices, last overdose, prior OAT/NSP contact, solitary vs peer use, sedative co-use, housing, legal status, pregnancy potential, children at home, and goals (safer use, reduced use, abstinence, housing first).[1][18]
MSE and risk. Consciousness, craving, insight, suicide and overdose risk, capacity for specific decisions, safeguarding. Capacity is decision-specific; continued use does not automatically equal incapacity.[1]
Motivational stance. Affirm any incremental reduction (e.g. always using with a peer, never sharing, carrying naloxone). Do not collapse “not ready for abstinence” into “not ready for care.”[1][2]
Differential framing traps
Harm reduction
- Evidence-based mortality and BBV reduction
- Compatible with recovery goals
- Does not require legalisation
- Keeps people alive for later change
False 'enabling' frame
- Assumes help increases use harm
- Ignores Sordo/Aspinall/Marshall data
- Often driven by stigma not evidence
- Leads to gatekeeping and early discharge
Abstinence-only gatekeeping
- Withholds NSP/naloxone until 'ready'
- Raises fatal overdose risk after detox alone
- Violates incrementalism principle
- Exam fail when presented as gold standard
OAT as 'another addiction'
- Common family/patient myth
- Counter with retention-mortality evidence
- Distinguish therapeutic dependence from OUD
- Language: medication for OUD, not 'replacement high'
Reject the false dichotomy: you can support a patient’s long-term abstinence goal and prescribe buprenorphine, hand over naloxone, and give sterile equipment today.[1][9][17]
Investigations and surveillance
Individual. Offer HIV, HBV, HCV testing with pre/post counselling and treatment linkage; pregnancy test when relevant; wound cultures or blood cultures when infection is suspected; ECG and metabolic baseline when OAT is planned. Interpret urine drug screens as engagement tools — not as moral tests that terminate care.[11][18]
Population. Track NSP coverage (syringes per person who injects per year), OAT coverage of the dependent population, naloxone kit distribution, and overdose deaths. Coverage intensity, not programme existence alone, drives population impact.[3][10][18]
Acute management — overdose and the post-revival window
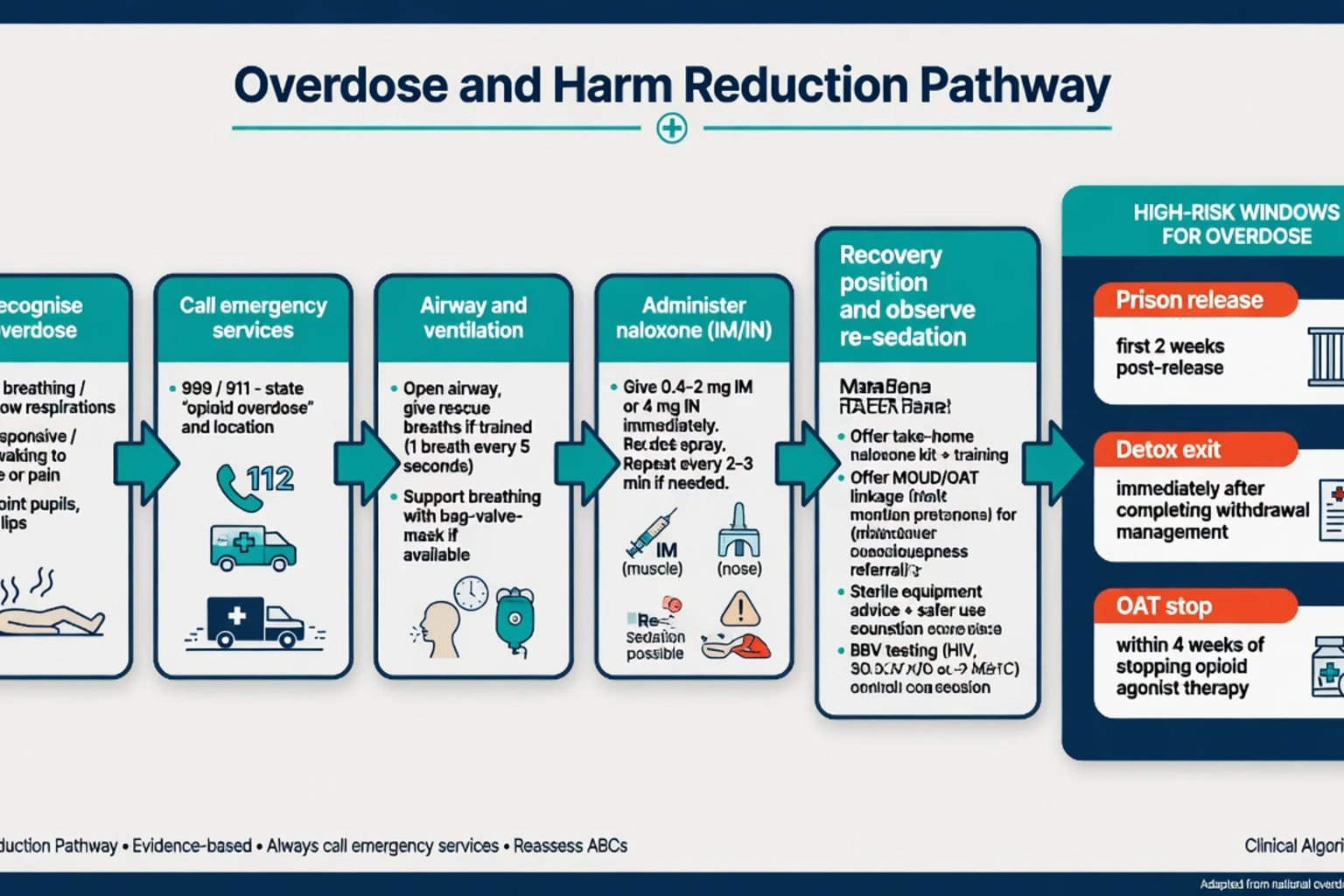
Community take-home naloxone education (exam script). Recognise slow or absent breathing and unresponsiveness; call emergency services; give intranasal or intramuscular naloxone as supplied in the kit (product-specific dosing — commonly 2–4 mg per intranasal device, or 0.4–2 mg IM depending on formulation); recovery position; stay until help arrives; be prepared to repeat doses. McDonald and Strang’s systematic review applying Bradford Hill criteria supports effectiveness of take-home naloxone programmes for reducing overdose mortality with a favourable safety profile.[15]
Parenteral emergency care. Typical teaching range 0.4–2 mg naloxone IV/IM/SC, repeated to restore adequate ventilation — not necessarily full alertness, because abrupt full reversal can precipitate severe withdrawal and agitation.[15]
Definitive public-health and clinical interventions
Needle and syringe programmes (NSP / needle exchange)
NSPs provide sterile injecting equipment, safe disposal, brief education, and bridges to testing and treatment. Aspinall and colleagues’ systematic review and meta-analysis associated NSP exposure with reduced HIV transmission among people who inject drugs (with stronger effects in higher-quality analyses).[3] Des Jarlais and colleagues documented lower HIV incidence among New York City syringe-exchange participants in a foundational evaluation era.[4] Wodak and Cooney’s comprehensive international review and Fernandes and colleagues’ overview of systematic reviews support NSP as a core HIV-prevention intervention, while noting heterogeneity and the need for adequate coverage and multi-component packages.[5][6]
Exam-safe practice points. Low-threshold access (including secondary distribution where legal); never require “clean time”; combine with OAT and antiviral treatment for HCV; address local disposal and community concerns with data, not denial.[3][5][6][11]
Opioid agonist / substitution treatment as public health
Methadone maintenance reduces illicit opioid use and improves retention versus non-replacement approaches; buprenorphine maintenance is effective versus placebo and informative against methadone in Cochrane synthesis.[7][8] Sordo and colleagues’ meta-analysis of cohort studies is the mortality pearl: risk is lower during treatment and rises after leaving treatment.[9] MacArthur and colleagues showed opiate substitution treatment associates with reduced HIV transmission among people who inject drugs.[10] Platt and colleagues’ Cochrane review synthesises needle-syringe programmes and opioid substitution therapy for preventing hepatitis C transmission — combination coverage is the practical takeaway for systems answers.[11]
Clinical doses (link to OUD topic for full induction detail). Methadone maintenance often 60–120 mg orally daily after careful low-and-slow induction. Buprenorphine maintenance commonly 8–24 mg sublingual daily after withdrawal-guided induction. These are disease-modifying medications, not last-resort “rewards.”[7][8]
Supervised consumption / safer injecting facilities
Supervised consumption services provide a hygienic space, sterile equipment, and staff ready to reverse overdose. Kerr and colleagues found that use of Vancouver’s safer injection facility was associated with reduced syringe sharing.[12] Marshall and colleagues reported a 35% reduction in fatal overdose rates within 500 m of Insite after opening, compared with the rest of the city — the population-level overdose paper most examiners expect by name.[13] Potier and colleagues’ systematic literature review concludes that supervised injection services are associated with safer injecting conditions, improved access to care, and reductions in overdose and public nuisance indicators, without increasing drug use or crime in the evaluated literature.[14]
Take-home naloxone and prison-release focus
Scale THN through pharmacies, ED, prisons, peer programmes, and OAT clinics. Post-release from custody is a classic high-fatality window — naloxone plus OAT continuity is the dual answer.[15][18]
Heroin-assisted treatment (selected jurisdictions)
For chronic refractory heroin dependence despite optimised oral methadone, the UK RIOTT trial found supervised injectable heroin (and, in some arms, injectable methadone) reduced street heroin use more than optimised oral methadone alone in highly selected patients under supervised conditions.[16] This is a specialist, highly regulated option — not first-line, but essential viva knowledge for “treatment-refractory” stems.
Psychosocial, housing, and peer components
Housing-first, peer outreach, contingency management, and integrated dual-diagnosis care amplify medical interventions. They do not replace OAT for severe opioid dependence.[2][18]
Stigma as a clinical and public-health intervention target
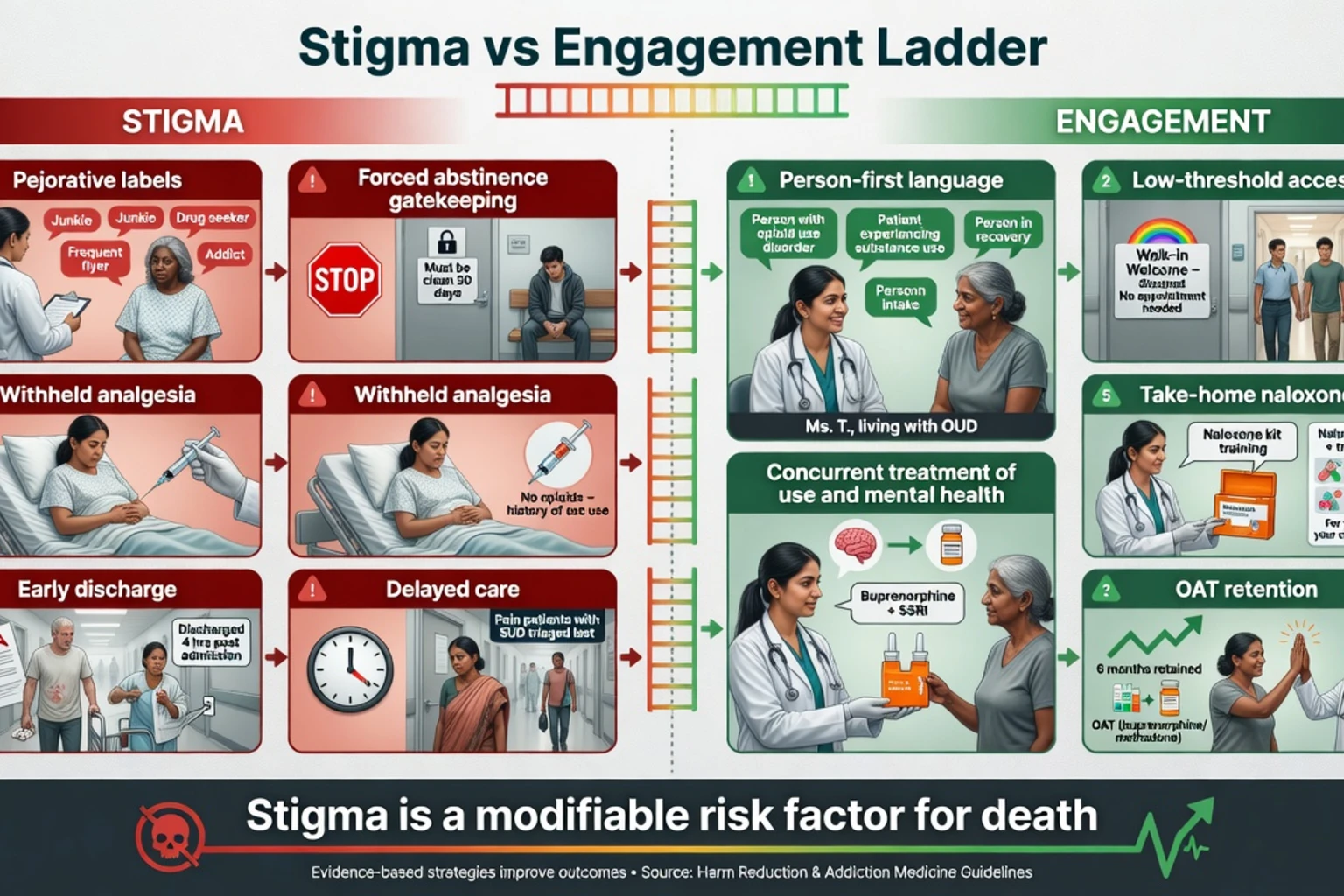
Volkow frames stigma as a driver of the toll of addiction: it shapes policy, clinician behaviour, and patient self-concept, and it reduces uptake of effective treatments.[17] Practical anti-stigma actions examiners want named: person-first language (“person with opioid use disorder,” not “junkie”); avoid “dirty/clean” urine language; do not withhold indicated analgesia; do not condition emergency care on abstinence; include people with lived experience in service design; train staff on MOUD as evidence-based medicine.[1][17]
Subtypes and scenarios
Open urban drug scene. Package NSP + OAT access expansion + supervised consumption advocacy/operation + THN saturation + street outreach.[13][14]
Rural and remote. Telehealth OAT, long-acting injectable buprenorphine where available, community pharmacy dosing, mail-order or pharmacy naloxone, mobile NSP.[18]
Prison continuum. Start or continue OAT in custody; discharge with THN and same-week community dosing appointment.[15][18]
Stimulant injecting. No population-scale agonist equivalent to OAT for methamphetamine; NSP, wound care, psychosis pathways, and contingency frameworks still apply.[2][18]
Pregnancy. Prefer OAT over forced withdrawal; non-stigmatising antenatal partnership; NSP still relevant if injecting continues.[18]
Complications and pitfalls
Other pitfalls: moral panic closures of supervised sites; fear that naloxone increases risk-taking (not supported as a reason to withhold by the THN evidence base); methadone induction toxicity when public-health scale-up outruns clinical training; ignoring fentanyl-era naloxone re-dosing; diagnostic overshadowing of medical illness in people who inject drugs.[14][15][18]
Prognosis and disposition
Individual survival tracks engagement with OAT and low-threshold services; population overdose and BBV rates track combined intervention coverage.[9][10][18] Disposition is a ladder: peer contact → NSP → primary care or pharmacy OAT → specialist addiction → hospital or supervised consumption → residential options when desired and available. Recovery endpoints are negotiated: safer use, reduced use, abstinence, employment, family reconnection — not a single moral metric.[1][2]
Special populations
Indigenous and culturally diverse communities. Culturally safe, community-controlled harm-reduction services; avoid stereotype and forced-intervention defaults. Youth. Consent, family engagement, age-appropriate low-threshold access. Older adults. Pharmaceutical opioid dependence, falls, polypharmacy. Custody. Highest-risk transitions. Co-occurring severe mental illness. Integrated dual care plus harm reduction — sequential “abstinence first” is obsolete.[1][17][18]
Regional deltas
Australia has a long history of national NSP policy under a harm-minimisation drug strategy; OAT is delivered through regulated opioid treatment programmes with jurisdiction-specific takeaway rules; take-home naloxone access has expanded via pharmacy and prescription pathways. Supervised injecting facilities operate in limited locations (e.g. Sydney Medically Supervised Injecting Centre; Melbourne services) with local evaluation politics. RANZCP training expects competence in OAT, dual diagnosis, and non-stigmatising care.[5][18]
Evidence, guidelines, and controversies
Name at viva: Aspinall (NSP–HIV); Des Jarlais (NYC); Wodak/Cooney and Fernandes (NSP reviews); Mattick Cochrane methadone and buprenorphine; Sordo (OST mortality); MacArthur (OST–HIV); Platt (NSP+OST–HCV); Kerr and Marshall (Insite); Potier (SIS review); McDonald and Strang (THN); Strang RIOTT; Volkow stigma; Degenhardt global opioids; Hawk principles.[1][3][4][5][6][7][8][9][10][11][12][13][14][15][16][17][18]
Controversies for balanced answers: supervised consumption legality and local opposition; safer-supply politics; coerced treatment ethics; measuring “success” as abstinence only versus survival and quality of life.[2][14][18]
Exam pearls
NEEDLE
Self-test: five viva openers
(1) Define harm reduction in one sentence without saying “encouraging drug use.” (2) Quote one NSP–HIV paper and one OST–mortality paper. (3) Explain supervised consumption outcomes without claiming it is legal everywhere. (4) Teach a family how to use take-home naloxone. (5) Rewrite a stigmatising discharge plan into a harm-reduction plan.[1][3][9][13][15]
References
- [1]Hawk M, Coulter RWS, Egan JE, Fisk S, Reuel Friedman M, Tula M, et al. Harm reduction principles for healthcare settings Harm Reduct J, 2017.PMID 29065896
- [2]Marlatt GA, Witkiewitz K Update on harm-reduction policy and intervention research Annu Rev Clin Psychol, 2010.PMID 20192791
- [3]Aspinall EJ, Nambiar D, Goldberg DJ, Hickman M, Weir A, Van Velzen E, et al. Are needle and syringe programmes associated with a reduction in HIV transmission among people who inject drugs: a systematic review and meta-analysis Int J Epidemiol, 2014.PMID 24374889
- [4]Des Jarlais DC, Marmor M, Paone D, Titus S, Shi Q, Perlis T, et al. HIV incidence among injecting drug users in New York City syringe-exchange programmes Lancet, 1996.PMID 8855855
- [5]Wodak A, Cooney A Do needle syringe programs reduce HIV infection among injecting drug users: a comprehensive review of the international evidence Subst Use Misuse, 2006.PMID 16809167
- [6]Fernandes RM, Cary M, Duarte G, Jesus G, Alarcão J, Torre C, et al. Effectiveness of needle and syringe Programmes in people who inject drugs - An overview of systematic reviews BMC Public Health, 2017.PMID 28399843
- [7]Mattick RP, Breen C, Kimber J, Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev, 2009.PMID 19588333
- [8]Mattick RP, Breen C, Kimber J, Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev, 2014.PMID 24500948
- [9]Sordo L, Barrio G, Bravo MJ, Indave BI, Degenhardt L, Wiessing L, et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies BMJ, 2017.PMID 28446428
- [10]MacArthur GJ, Minozzi S, Martin N, Vickerman P, Deren S, Bruneau J, et al. Opiate substitution treatment and HIV transmission in people who inject drugs: systematic review and meta-analysis BMJ, 2012.PMID 23038795
- [11]Platt L, Minozzi S, Reed J, Vickerman P, Hagan H, French C, et al. Needle syringe programmes and opioid substitution therapy for preventing hepatitis C transmission in people who inject drugs Cochrane Database Syst Rev, 2017.PMID 28922449
- [12]Kerr T, Tyndall M, Li K, Montaner J, Wood E Safer injection facility use and syringe sharing in injection drug users Lancet, 2005.PMID 16039335
- [13]Marshall BDL, Milloy MJ, Wood E, Montaner JSG, Kerr T Reduction in overdose mortality after the opening of North America's first medically supervised safer injecting facility: a retrospective population-based study Lancet, 2011.PMID 21497898
- [14]Potier C, Laprévote V, Dubois-Arber F, Cottencin O, Rolland B Supervised injection services: what has been demonstrated? A systematic literature review Drug Alcohol Depend, 2014.PMID 25456324
- [15]McDonald R, Strang J Are take-home naloxone programmes effective? Systematic review utilizing application of the Bradford Hill criteria Addiction, 2016.PMID 27028542
- [16]Strang J, Metrebian N, Lintzeris N, Potts L, Carnwath T, Mayet S, et al. Supervised injectable heroin or injectable methadone versus optimised oral methadone as treatment for chronic heroin addiction (RIOTT): a randomised trial Lancet, 2010.PMID 20511018
- [17]Volkow ND Stigma and the Toll of Addiction N Engl J Med, 2020.PMID 32242351
- [18]Degenhardt L, Grebely J, Stone J, Hickman M, Vickerman P, Marshall BDL, et al. Global patterns of opioid use and dependence: harms to populations, interventions, and future action Lancet, 2019.PMID 31657732