Psych · Addiction psychiatry — inhalant-related disorders
Inhalant-related disorders
Also known as Volatile substance misuse · VSM · Chroming · Solvent abuse · Petrol sniffing · Glue sniffing · Huffing · Sudden sniffing death · Nitrous oxide misuse · Whippets · Inhalant use disorder
Fellowship-depth atlas on inhalant-related disorders — volatile solvent, aerosol and hydrocarbon gas misuse (including petrol sniffing and chroming), sudden sniffing death, chronic toluene neurotoxicity, recreational nitrous oxide myeloneuropathy, adolescent epidemiology, psychosocial care, and the absence of licensed anti-craving pharmacotherapy. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Inhalants are volatile substances inhaled for intoxication, not therapeutic gases under supervised medical use. Fellowship work is to recognise the product classes and methods (sniffing, huffing, bagging/chroming), treat acute medical toxicity (arrhythmia, asphyxia, aspiration, burns), manage adolescent dual-diagnosis complexity, and avoid inventing an opioid-style substitution pathway that does not exist.[1][14]
In DSM-5-TR, inhalant intoxication and inhalant use disorder capture solvents, aerosols and related volatiles; nitrites are often handled separately; recreational nitrous oxide is frequently discussed clinically with inhalants even when coding systems place it under other dissociative or inhalant-adjacent categories. ICD-11 frames disorders due to use of volatile inhalants. A single negative standard urine drug screen neither excludes recent volatile use nor proves a use disorder.[1]
This leaf topic covers acute toxidromes, sudden sniffing death, chronic solvent neurotoxicity, N2O myeloneuropathy, epidemiology and the psychosocial/public-health treatment frame.[3][5][8]
Classification
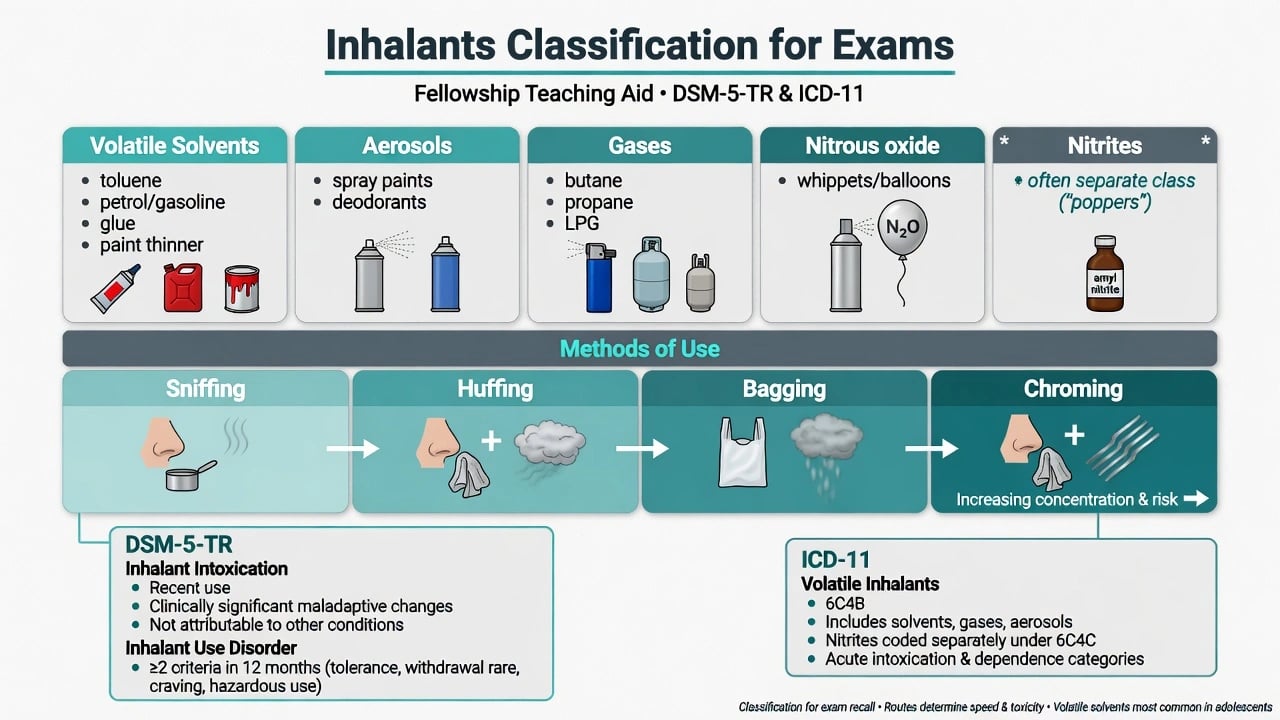
| Class | Examples | Exam discriminators |
|---|---|---|
| Volatile solvents | Toluene, petrol/gasoline, glue, paint thinner | Adolescent chroming; chronic white-matter injury; paint stains/odour |
| Aerosols | Spray paints, deodorants, hair sprays | Propellant + solvent mix; bagging risk |
| Hydrocarbon gases | Butane, propane, LPG, lighter fluid | High sudden sniffing death association; cooler burns |
| Nitrous oxide | Whippets, balloons, diverted medical cylinders | Myeloneuropathy; functional B12 deficiency |
| Nitrites ("poppers") | Amyl/butyl nitrite | Often separate class; sexual-context use; hypotension/metHb risk |
Methods matter for dose and hypoxia risk: open sniffing is lower intensity than huffing (cloth) or bagging/chroming (plastic bag), which concentrate vapour and increase asphyxia and cardiac risk.[1][14]
Epidemiology and risk factors
Inhalants are among the earliest substances tried in adolescence. US survey work shows meaningful rates of adolescent abuse/dependence among those who use, with high multi-problem profiles rather than isolated "experimentation only" narratives when a disorder is present.[9][11] Adult lifetime inhalant use is lower than adolescent experimentation peaks, and patterns of adult disorder differ from youth-onset trajectories.[1]
Risk markers for heavier use and disorder include early onset, conduct problems, trauma exposure, school disengagement, homelessness or street involvement, remoteness and poverty, and concurrent other substance use. Adolescent clinical samples with inhalant use disorders show high rates of comorbid psychiatric and behavioural problems, including mood, conduct and other SUD comorbidity.[10][11][14]
ANZ framing: petrol sniffing and chroming have had high public-health visibility in some remote communities; urban recreational nitrous oxide presentations (myeloneuropathy, falls, psychiatric contact) have risen in many high-income settings. Pair clinical care with community-controlled and supply-reduction strategies where relevant.[14]
Pathophysiology
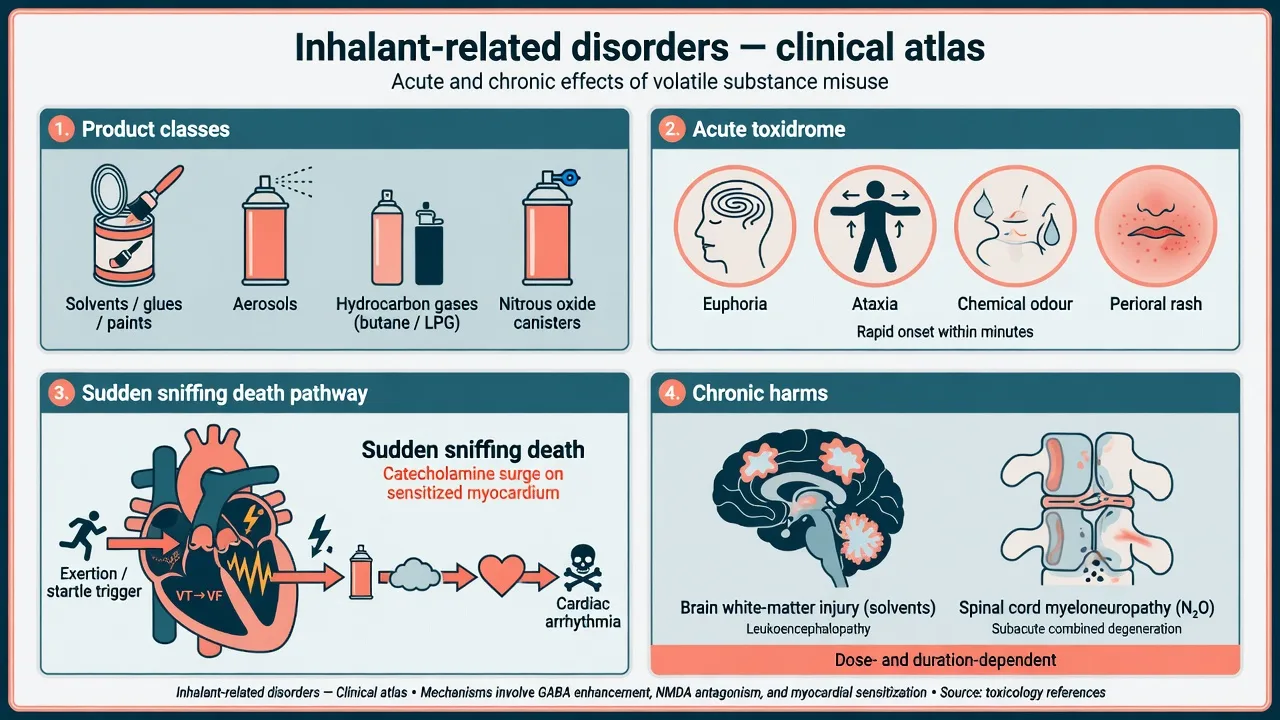
Volatiles are highly lipid-soluble and absorbed rapidly across the pulmonary interface, producing onset within minutes and relatively brief intoxication that drives re-dosing. Acute CNS effects resemble other CNS depressants: euphoria, disinhibition, ataxia, then drowsiness.[1][6]
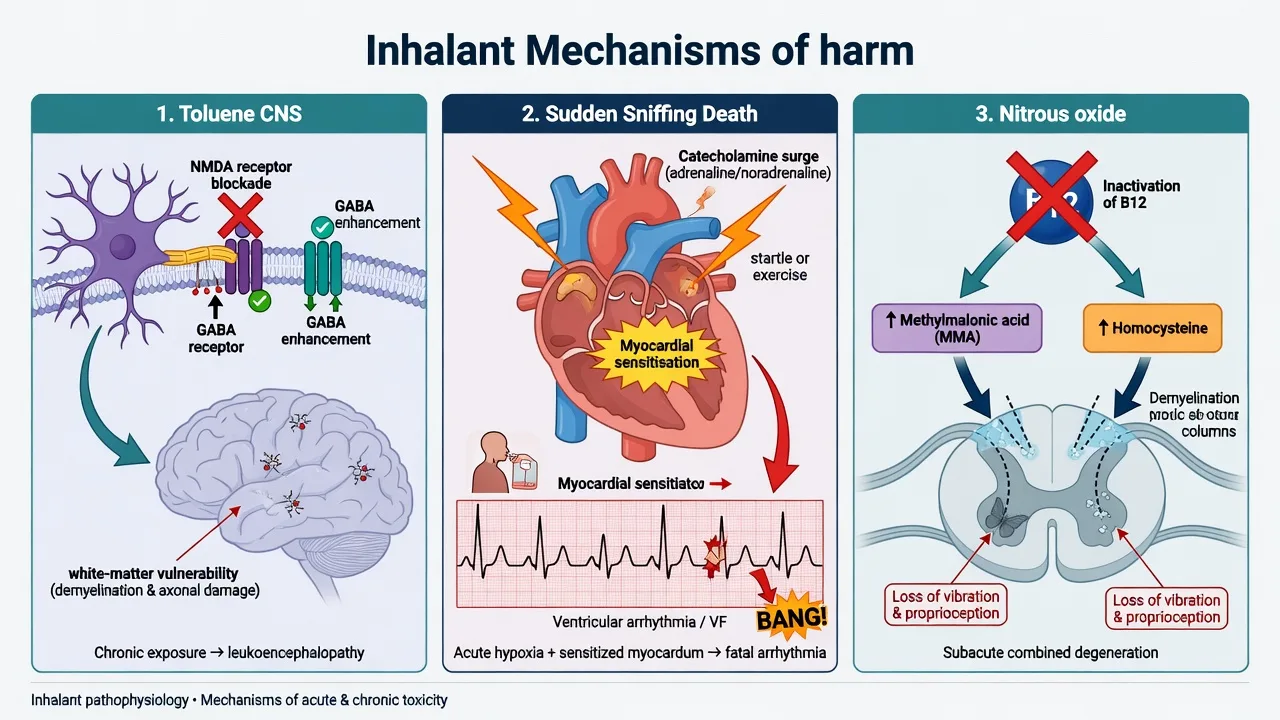
Toluene acts on multiple molecular targets including NMDA receptor antagonism and enhancement of inhibitory (GABA/glycine) signalling. Chronic high-level misuse is associated with white-matter injury, neuropsychological deficits and a leukoencephalopathy phenotype on imaging research series — not a trivial "high only" story.[5][6][7]
Sudden sniffing death (also discussed as inhaled hydrocarbon-associated sudden collapse) classically links hydrocarbon exposure to myocardial sensitisation, with fatal ventricular arrhythmia often precipitated by exertion, fright or catecholamine surge during or immediately after use — including in first-time users. Hypoxia and other mechanisms can co-exist, but the arrhythmia teaching point is high-yield.[2][3][4]
Nitrous oxide oxidises the active cobalt in cobalamin, producing functional vitamin B12 deficiency. Serum B12 may be normal while methylmalonic acid (MMA) and homocysteine rise; the clinical syndrome is a subacute myeloneuropathy resembling subacute combined degeneration, potentially reversible if use stops and B12 is replaced early.[8]
Clinical presentation
Acute intoxication
Typical features: rapid euphoria or light-headedness, disinhibition, diplopia, slurred speech, ataxia, impaired judgement, hallucinations at higher doses, then sedation. Clues include chemical odour on breath or clothing, paint stains, perioral rash ("huffer's rash"), empty bags or canisters, and cooler/frostbite burns from gas canisters.[1][14]
Medical toxicity and sudden death
Severe presentations: syncope, seizure, coma, aspiration, chemical pneumonitis, trauma from falls, burns, and sudden collapse with cardiac arrest during or just after use. Treat collapse after hydrocarbon inhalation as a cardiac emergency until proven otherwise.[2][4]
Chronic solvent neurotoxicity
Long-term toluene misuse associates with cognitive slowing, executive dysfunction, apathy, affective blunting, tremor, cerebellar signs and white-matter injury patterns in the neuroimaging literature. Residual deficits may persist after abstinence.[5][7]
Nitrous oxide myeloneuropathy
Subacute bilateral paraesthesia, gait ataxia, Rombergism, impaired vibration and joint-position sense, Lhermitte-like symptoms, and sometimes bladder or motor involvement. Psychiatric services may see the patient for depression, anxiety or falls first — always ask about balloons/whippets.[8]
Psychiatric comorbidity
Depression, anxiety, trauma-related symptoms, self-harm, psychosis-like experiences and other substance use are common in clinical inhalant samples. Dual formulation is mandatory when psychosis or major mood syndromes appear with heavy use.[10][11]
Differential diagnosis
| Presentation | Favours inhalant-related state | Favours alternative | Discriminators |
|---|---|---|---|
| Ataxic intoxicated youth | Chemical odour, paint stains, empty bags/canisters | Alcohol, GHB, benzo, hypoglycaemia | Collateral, scene, glucose, short time course |
| Sudden collapse | Recent hydrocarbon use + exertion/startle | Primary arrhythmia, PE, seizure, overdose opioid | History of chroming/butane; ECG; ACLS first |
| Subacute sensory ataxia | Heavy N2O use; raised MMA/homocysteine | GBS, copper deficiency, MS, compressive myelopathy | N2O history; B12 functional markers; MRI cord |
| Chronic apathy + cognitive decline | Years of toluene; white-matter pattern | Schizophrenia residual, TBI, primary dementia | Timeline of solvent exposure; neuropsych |
| Hallucinations | Intoxication window, clear odour | Primary psychosis, stimulant MAP, encephalitis | Course with abstinence; organic work-up thresholds |
| Hypotension in sexual context | Nitrite ("poppers") use | Sepsis, cardiogenic shock | Sexual history; metHb if severe cyanosis |
Can't-miss organics: arrhythmia/ACS pathway, head injury, aspiration pneumonia, carbon monoxide or other toxic gases, hypoglycaemia, and in N2O cases progressive myeloneuropathy with permanent disability if missed.[4][8]
Clinical and bedside assessment
- ABC and vitals first — airway risk if sedated, SpO2, glucose, temperature, ECG after recent hydrocarbon use or any syncope.
- Exposure inventory — products, method (sniff, huff, bag/chrome), frequency, last use, solitary vs group, access points (home shed, retail, peers).
- MSE with examples — e.g. "disinhibited, smelling of paint, ataxic gait, believes friends are laughing at him; oriented to place."
- Risk — suicide, accidental death (SSD, asphyxia, fire), exploitation, driving, child protection, school harm.
- Capacity and legal status — jurisdiction-specific least-restrictive principles; do not invent section numbers.
- Collateral — family, school, community AOD, ambulance/police scene description.
- Comorbidity screen — trauma, ADHD/conduct, depression, psychosis, other SUD, neurodevelopmental vulnerability.
Investigations
| Domain | Tests / actions | Why |
|---|---|---|
| Bedside | ECG, continuous monitoring if recent use/syncope, glucose, SpO2 | Arrhythmia and hypoxia risk |
| Bloods | U&E, LFT, FBC, CK if prolonged immobility | Medical complications; baseline |
| N2O work-up | Serum B12, folate, MMA, homocysteine | Functional B12 deficiency may have normal B12 |
| Imaging | MRI brain if chronic cognitive change; MRI cord if myelopathy | White-matter / dorsal-column patterns — specialist reporting |
| Toxicology | Standard UDS | Often misses volatiles — clinical diagnosis dominates |
| Pregnancy | Test when relevant | Fetal solvent syndrome counselling pathway |
Management — resuscitation and acute care
Acute priorities:
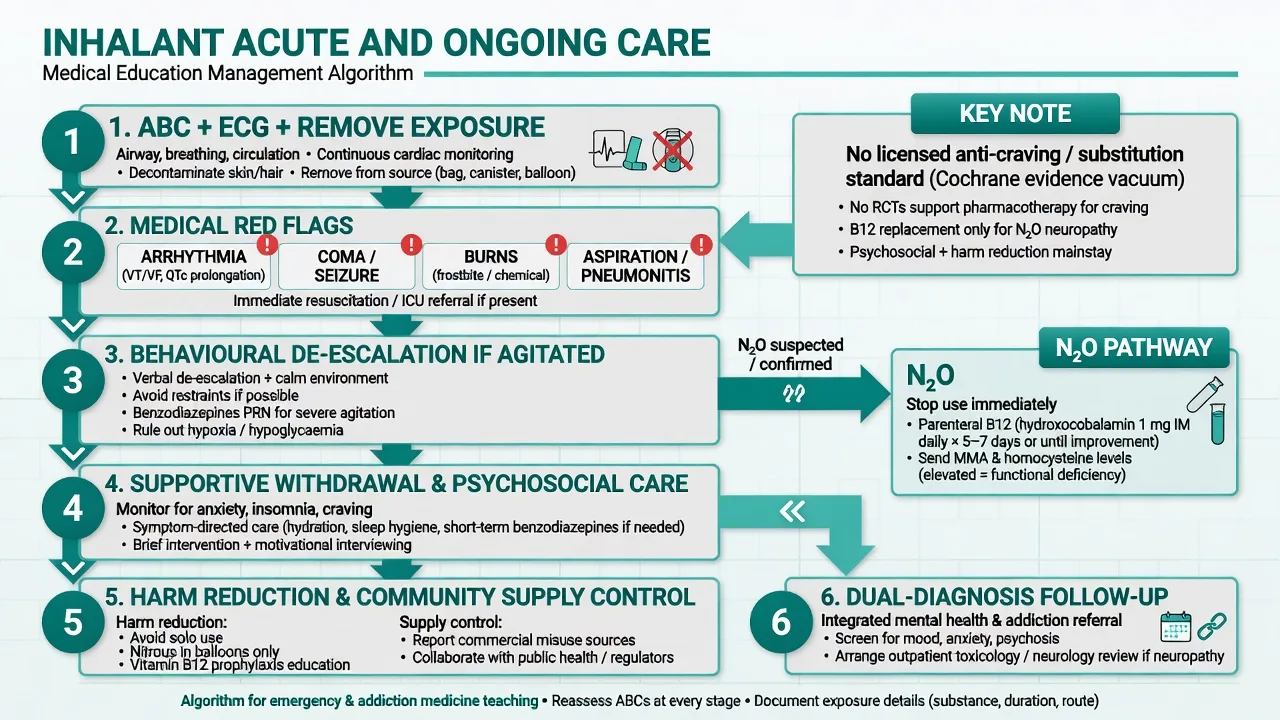
- Remove ongoing exposure — bag, cloth, canister, confined space; oxygen as indicated; protect airway.
- Cardiac and ACLS readiness — ECG, monitoring; treat arrhythmias per emergency protocols; minimise unnecessary rough stimulation when safe, recognising real-world resus needs dominate theory.
- Concurrent injuries — burns (including cooler burns), aspiration, trauma from falls.
- Behavioural ladder — low-stimulus environment, de-escalation; short-term sedation only if essential under local rapid-tranquillisation guidance with airway and ECG awareness (example: oral lorazepam 1–2 mg if safe to take orally and no oversedation risk from residual volatiles — local protocol overrides).
- N2O myeloneuropathy pathway — immediate cessation; check B12, MMA, homocysteine; start high-dose parenteral B12 without waiting for every result if clinical suspicion is high. A common teaching regimen is hydroxocobalamin 1 mg IM daily for several days (often cited as about 5–7 days in acute neurology pathways) then spaced dosing per local protocol, plus folate support and rehab referral; confirm exact regimen with neurology/local guideline.[8]
- Do not start "inhalant OAT" — there is no licensed substitution analogue of methadone for volatiles.[12]
Management — definitive care and evidence vacuum
What is standard
Supportive care for intoxication and mild withdrawal-like symptoms (irritability, sleep disturbance, craving) is the medical baseline. The treatment backbone is psychosocial: engagement, motivational work, family and school involvement, structured youth AOD care, case management, recreational/engagement programmes, and residential options in selected severe cases. Systematic review evidence is limited in quality but points to multi-component psychosocial approaches rather than a single magic drug.[13][14]
No licensed anti-craving / substitution standard
Be precise in exams: a Cochrane review found no randomised trials meeting inclusion criteria for pharmacotherapy of inhalant dependence/abuse. Do not invent approved anti-craving agents or "replacement solvents." Treat comorbid depression, psychosis or ADHD with standard indicated agents when the risk-benefit is clear, but that is comorbidity care — not inhalant substitution.[12]
| Approach | Role | Exam-level precision |
|---|---|---|
| Psychosocial packages | Core ongoing care | Case management, counselling, recreation/engagement, residential — MacLean synthesis[13] |
| Youth-integrated assessment | Prevention + treatment pathway | Nguyen synthesis: family, school, community, dual diagnosis[14] |
| Harm reduction / supply control | Public health lever | Retail controls on N2O where legislated; low-aromatic fuel and community programmes for petrol sniffing; family product lock-up education |
| Parenteral B12 (N2O only) | Disease-modifying for myeloneuropathy | Stop N2O + B12 replacement; not a craving drug for solvents[8] |
| Pharmacotherapy for IUD itself | No licensed standard | Cochrane evidence vacuum — do not invent OAT-equivalent[12] |
Dual diagnosis and discharge
Treat dangerous mood, psychotic or trauma syndromes actively. Before discharge: medical clearance (including ECG if indicated), documented suicide/accidental-death plan, youth AOD and mental-health follow-up, family education about product access, and written advice on when to return (syncope, chest pain, progressive numbness, severe mood change).[10][14]
Specific subtypes and scenarios
Adolescent chroming with school failure. Confidential youth interview plus family work; screen trauma and conduct; engage school; restrict product access at home without pure punishment framing.[9][14]
Petrol sniffing in remote community. Pair individual care with community-controlled responses and supply reduction (e.g. low-aromatic fuel programmes historically used in Australia) — clinical care alone is incomplete.[14]
Butane collapse after exercise. SSD pathway teaching case — resus, family counselling about first-use death risk.[2][4]
Urban N2O myeloneuropathy. Stop balloons/whippets; parenteral B12; neurology/rehab; address group use and retail access.[8]
Chronic toluene cognitive syndrome. Neuropsych assessment, abstinence support, disability and occupational planning; dual formulate vs primary SMI.[5]
Polysubstance street-involved youth. Integrated dual-diagnosis care; housing and peer support; watch for mixed toxidromes.[10][11]
Complications and pitfalls
- Medical: sudden sniffing death, asphyxia, aspiration, burns, trauma, chemical pneumonitis, chronic organ toxicity, fetal solvent syndrome risk in pregnancy.
- Neurological: toluene white-matter injury, cerebellar and cognitive syndromes, N2O myeloneuropathy with lasting disability if delayed.
- Psychiatric: depression, suicide, dual-diagnosis mislabeling, missed trauma.
- Pitfalls: assuming UDS rules out inhalants; missing SSD arrhythmia teaching; treating only with "willpower lectures"; inventing anti-craving standards; assuming normal serum B12 excludes N2O toxicity; forcing lifelong schizophrenia labels without solvent neurotoxicity differential; ignoring family/community supply pathways.
Prognosis and disposition
Many young people who experiment do not develop severe chronic disorder; early onset, high comorbidity and ongoing access worsen course. Chronic toluene injury may partially improve with sustained abstinence, but residual cognitive deficits are common in heavy long-term users. N2O myeloneuropathy often improves with early cessation and B12, with delayed treatment predicting worse outcome.[5][8][11]
Disposition ladder: medical clearance (and cardiac observation after concerning hydrocarbon exposure) → short admission if suicide, severe intoxication sequelae or progressive myelopathy → community youth AOD + mental health shared care with early review and family engagement.[14]
Special populations
Children and early adolescents. Developmental assessment, school liaison, child-protection thresholds when caregivers supply or fail to protect access.[9][14]
Remote and Aboriginal and Torres Strait Islander communities. Culturally safe, community-controlled partnerships; address social determinants and supply; avoid deficit-only framing while still naming medical risk honestly.[14]
Pregnancy. Counsel fetal solvent syndrome and pregnancy risks of volatile misuse; obstetric and addiction liaison; no unproven mandatory "inhalant OAT."[3]
Intellectual disability / neurodevelopmental vulnerability. Higher exploitation and access risk; simplified safety plans; carer education.[11]
Forensic / custody. Document residual intoxication, ECG/observation needs, empty canisters found, and cognitive capacity for interview.[1]
Evidence, guidelines and regional differences
| Source | High-yield takeaway |
|---|---|
| Howard 2011 | Clinical epidemiology and disorder framing for inhalants in the US — still a core teaching review[1] |
| Bass 1970; Bowen 2011; Berling 2025 | Sudden sniffing death / hydrocarbon-associated sudden collapse — arrhythmia teaching lineage to contemporary toxicology framing[2][3][4] |
| Yücel 2008; Cruz 2014; Shaw 2025 | Toluene long-term harm and molecular mechanisms[5][6][7] |
| Wu 2004; Sakai 2004; Perron 2009 | Adolescent epidemiology and comorbidity density[9][10][11] |
| Konghom Cochrane 2010 | No eligible RCTs for pharmacotherapy of inhalant dependence — evidence vacuum[12] |
| MacLean 2012; Nguyen 2016 | Psychosocial interventions and youth prevention/assessment/treatment synthesis[13][14] |
| Swart 2021 | N2O myeloneuropathy clinical series teaching functional B12 markers[8] |
ANZ: Petrol sniffing and chroming have shaped public-health responses (including low-aromatic fuel and community programmes); urban N2O presentations increasingly hit ED and neurology. UK: Strong contemporary focus on recreational N2O legislation and myeloneuropathy pathways alongside classic solvent misuse in some youth groups. US: Howard/Wu epidemiology base; volatile misuse remains under-recognised in adult services. Quote the jurisdiction you are working in for supply-control laws.[1][8][14]
Exam pearls
- Sudden sniffing death = arrhythmia after hydrocarbons, often with exertion or startle — not only progressive sedation.[2][4]
- Standard UDS often misses volatiles — clinical diagnosis.[1]
- No licensed anti-craving/substitution standard — Cochrane vacuum; psychosocial + public health are core.[12][13]
- N2O: functional B12 deficiency; MMA/homocysteine; stop use; parenteral B12 early.[8]
- Peak age is often younger than classic alcohol/opioid stems — ask about chroming and balloons explicitly.[9]
- Chronic toluene → white-matter cognitive syndrome; dual formulate with primary psychosis.[5]
- Adolescent IUD samples are high-comorbidity, not "mild curiosity only."[10][11]
- Petrol sniffing responses need clinical care plus supply/community strategies.[14]
- Pregnancy: name fetal solvent syndrome risk counselling.[3]
- Legal frameworks for N2O and solvent sales are jurisdiction-specific — principles yes, invented statute numbers no.[14]
References
- [1]Howard MO, Bowen SE, Garland EL, et al. Inhalant use and inhalant use disorders in the United States Addict Sci Clin Pract, 2011.PMID 22003419
- [2]Bass M Sudden sniffing death JAMA, 1970.PMID 5467774
- [3]Bowen SE Two serious and challenging medical complications associated with volatile substance misuse: sudden sniffing death and fetal solvent syndrome Subst Use Misuse, 2011.PMID 21609149
- [4]Berling I, Buckley NA, Isoardi KZ Rare but relevant: Hydrocarbons and sudden sniffing syndrome Addiction, 2025.PMID 40275758
- [5]Yücel M, Takagi M, Walterfang M, Lubman DI Toluene misuse and long-term harms: a systematic review of the neuropsychological and neuroimaging literature Neurosci Biobehav Rev, 2008.PMID 18456329
- [6]Cruz SL, Rivera-García MT, Woodward JJ Review of toluene action: clinical evidence, animal studies and molecular targets J Drug Alcohol Res, 2014.PMID 25360325
- [7]Shaw AA, Woodward JJ Toluene Toxicity in the Brain: From Cellular Targets to Molecular Mechanisms Annu Rev Pharmacol Toxicol, 2025.PMID 39847463
- [8]Swart G, Blair C, Lu Z, et al. Nitrous oxide-induced myeloneuropathy Eur J Neurol, 2021.PMID 34427020
- [9]Wu LT, Pilowsky DJ, Schlenger WE Inhalant abuse and dependence among adolescents in the United States J Am Acad Child Adolesc Psychiatry, 2004.PMID 15381887
- [10]Sakai JT, Hall SK, Mikulich-Gilbertson SK, Crowley TJ Inhalant use, abuse, and dependence among adolescent patients: commonly comorbid problems J Am Acad Child Adolesc Psychiatry, 2004.PMID 15322411
- [11]Perron BE, Howard MO Adolescent inhalant use, abuse and dependence Addiction, 2009.PMID 19426292
- [12]Konghom S, Verachai V, Srisurapanont M, et al. Treatment for inhalant dependence and abuse Cochrane Database Syst Rev, 2010.PMID 21154379
- [13]MacLean S, Cameron J, Harney A, Lee NK Psychosocial therapeutic interventions for volatile substance use: a systematic review Addiction, 2012.PMID 22248138
- [14]Nguyen J, O'Brien C, Schapp S Adolescent inhalant use prevention, assessment, and treatment: A literature synthesis Int J Drug Policy, 2016.PMID 26969125