Psych · Addiction psychiatry — psychosocial interventions
Mutual help programmes and contingency management
Also known as Alcoholics Anonymous · Narcotics Anonymous · Twelve-step facilitation · 12-step programmes · SMART Recovery · Contingency management · Voucher reinforcement · Prize-based contingency management · Peer support recovery · Mutual aid addiction
Exam-exhaustive fellowship reference on mutual-help programmes (AA, NA, SMART Recovery, TSF) and contingency management (voucher and prize-based reinforcement) — definitions, mechanisms, landmark evidence, protocol parameters, dual-diagnosis integration, ethics, and regional deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Mutual-help and contingency management (CM) are high-yield psychosocial tools that examiners use to test whether you can separate peer fellowship from professional therapy, name landmark evidence without ideology, and design a protocol rather than wave at “support groups.” McLellan’s chronic-illness framing reminds you that addiction care needs long-term support structures, not one-off detox theatre.[11][12]
Overview and definition
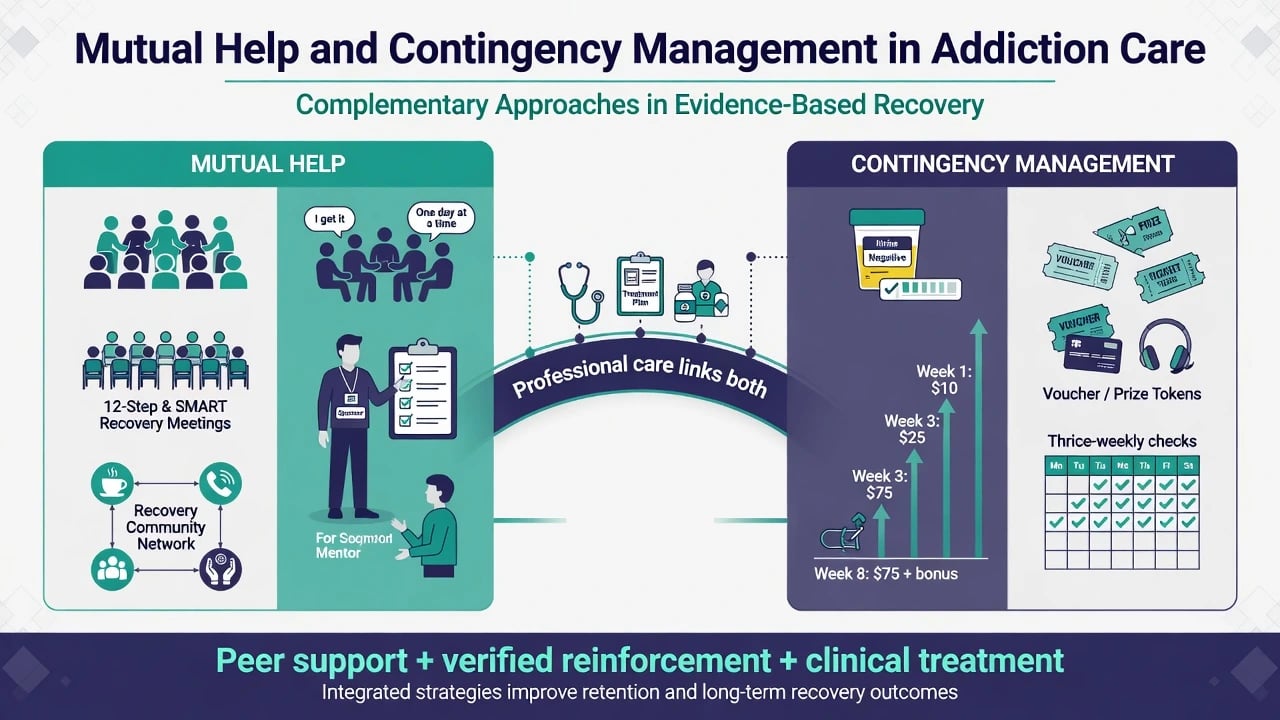
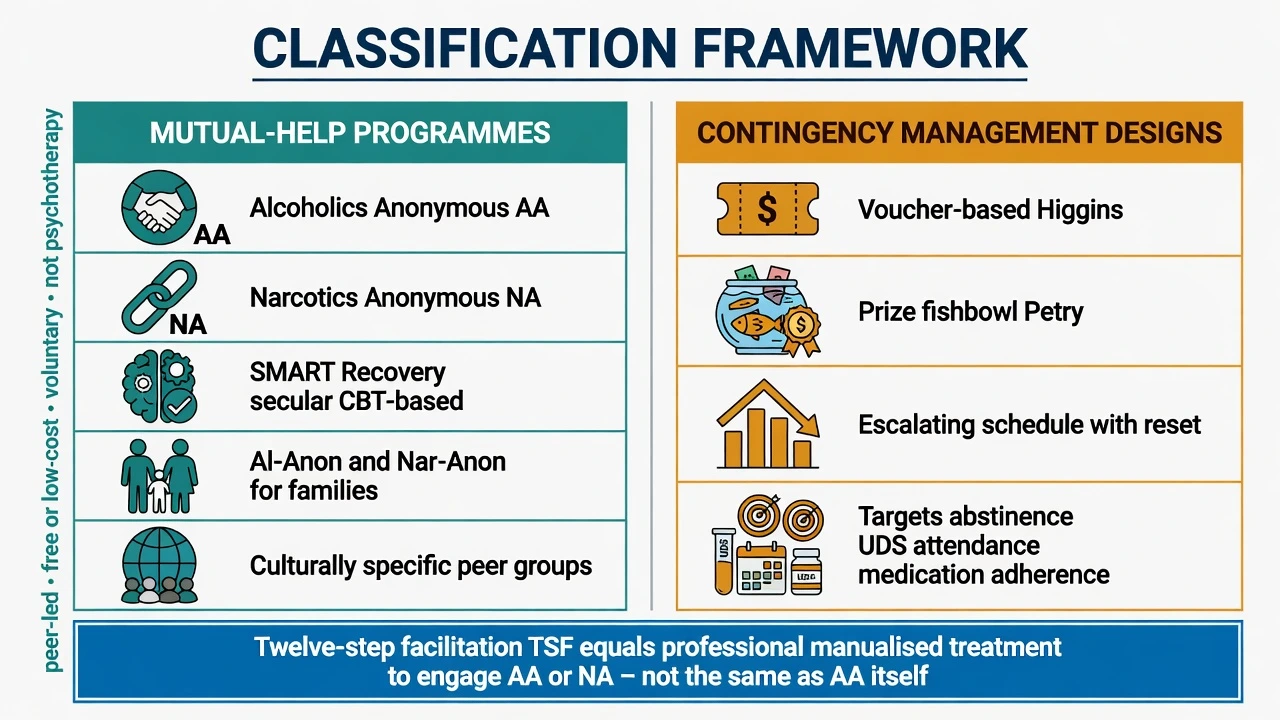
Mutual-help (mutual aid, peer recovery support) programmes are voluntary, usually free or low-cost, peer-led groups that offer recovery identity, social network change, and ongoing support outside the professional clinical record. Alcoholics Anonymous (AA) and Narcotics Anonymous (NA) are the best-known 12-step fellowships; SMART Recovery, LifeRing, Women for Sobriety, and culturally specific groups offer alternatives, including secular cognitive-behavioural peer formats.[12][14][15]
Twelve-step facilitation (TSF) is a professional, manualised treatment whose goal is to engage patients in AA/NA participation (meetings, steps, sponsorship). TSF is not AA. Project MATCH included TSF as one of three professionally delivered outpatient therapies alongside CBT and motivational enhancement therapy (MET).[3][12]
Contingency management is the systematic application of operant reinforcement: a tangible reinforcer (voucher, prize draw, privilege) is delivered immediately when an objectively verified target behaviour occurs — most often a substance-negative urine/oral fluid test, sometimes session attendance or medication adherence.[4][5][6]
Classification and programme map
Mutual-help fellowships
- Peer-led, voluntary, free/low-cost
- AA, NA, SMART, family groups
- No clinical case notes as therapy
- Ongoing recovery capital after formal treatment
Twelve-step facilitation
- Professional, manualised therapy
- Goal: engage AA/NA involvement
- Billable clinical episode
- Used in Project MATCH
Voucher CM (Higgins)
- Monetary voucher for verified abstinence
- Escalating magnitude + reset
- Classic cocaine behavioural trials
- Higher average cost per patient
Prize CM (Petry)
- Draws from fishbowl for prizes
- Low average cost, variable reward
- Meta-analytic support
- Caution if active gambling disorder
Epidemiology and service context
Mutual-help is among the most widely accessed free recovery resources for alcohol problems worldwide; professional systems under-use assertive linkage despite the public-health economics of free ongoing support.[1][2][12] Stimulant use disorders still lack a population-scale agonist equivalent to methadone/buprenorphine; psychosocial intensity — especially CM — is therefore examiner-critical when pharmacotherapy options are limited.[8][10] Early dropout and weak retention are core process risks across SUD care; both mutual-help density and CM target retention and continuous abstinence windows.[4][11]
Viva number-and-name anchors
Mechanisms
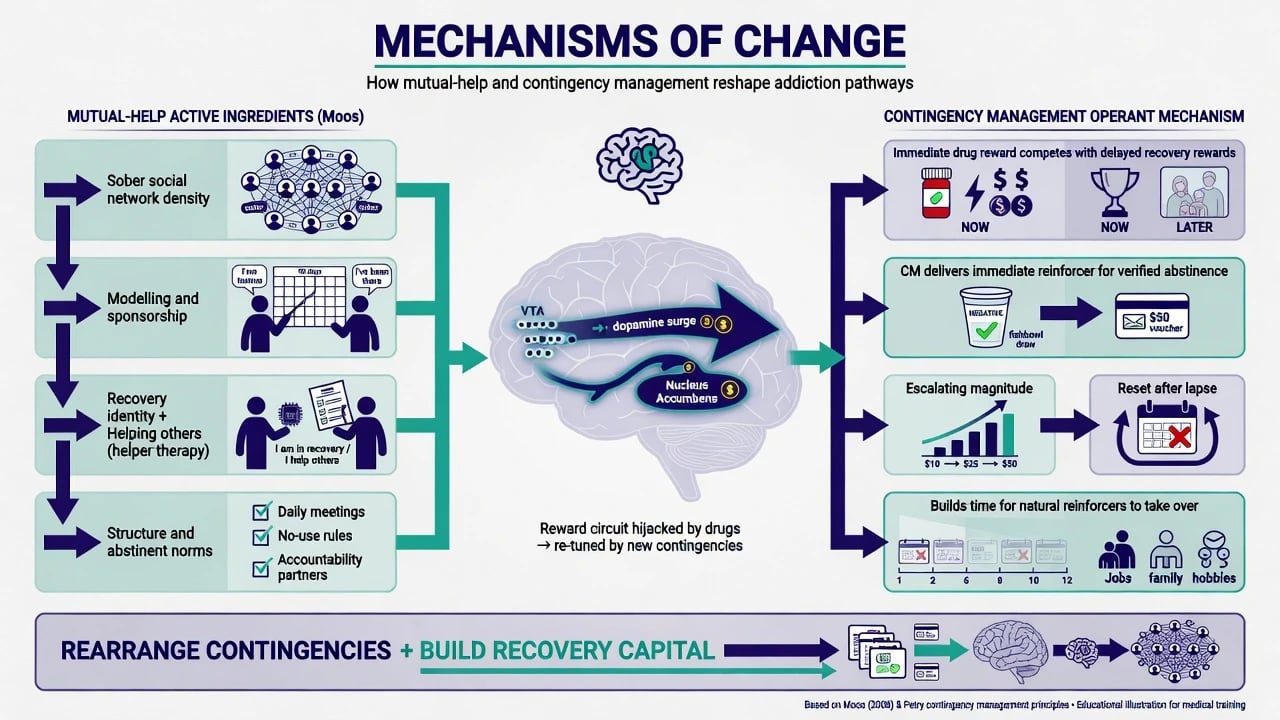
Mutual-help active ingredients. Moos describes substance-focused self-help effects through bonding and support, goal direction and structure, abstinent norms, modelling, and helping others (helper-therapy principle). Network density of non-using peers and recovery identity shift are the sociological engines examiners expect.[13][14]
CM operant logic. Psychoactive drugs deliver immediate reinforcement; natural recovery rewards (health, relationships, employment) are delayed. CM inserts an immediate, certain, contingent reward for verified abstinence or attendance, often with escalating magnitude after consecutive successes and a reset after a miss — buying time for natural reinforcers and skills to take hold.[4][5][7]
Not spirituality-only. Kaskutas’ “faith meets science” framing and the 2020 Cochrane synthesis treat AA as an intervention with measurable outcomes, not a theological debate. Secular mutual-help options exist when spiritual language is a barrier.[1][14][15]
Clinical presentation and assessment
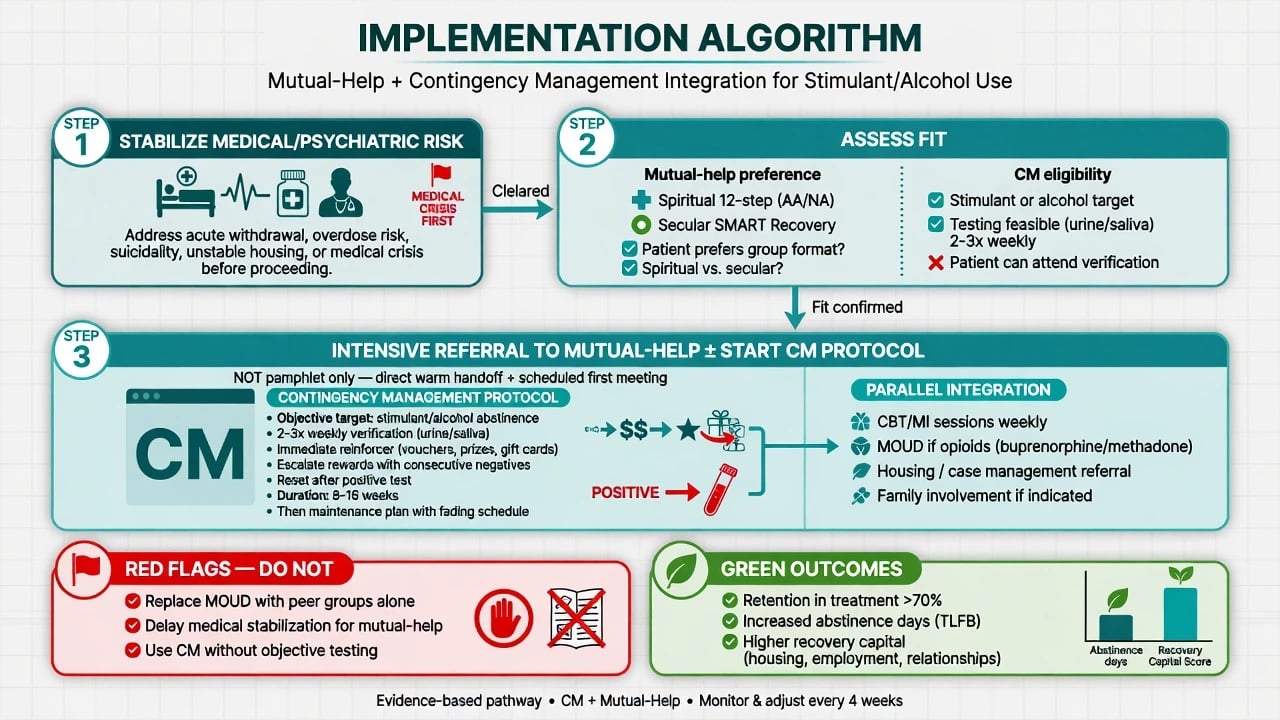
Patients rarely say “I need contingency management.” They present with stimulant relapse, alcohol dependence after detox, dual diagnosis, criminal-justice testing, or family crisis. Fellowship tasks: (1) map prior mutual-help fit and barriers; (2) decide whether intensive TSF-style linkage is indicated; (3) decide whether an objective, fundable CM target exists.[12][3]
History structure. Substances and routes; prior detox/residential; meetings tried (which fellowship, frequency, sponsorship); reasons for dropout (religion, stigma, transport, gender safety); willingness for urine/oral fluid testing; gambling history (prize CM caution); family mutual-help interest (Al-Anon/Nar-Anon); goals (abstinence vs reduction).[12][15]
MSE and risk. Craving, insight, suicidality, capacity, safeguarding. Acute medical or psychiatric instability overrides meeting-first plans.[11]
Differential framing
Mutual-help
- Peer-led recovery community
- No formal psychotherapy contract
- Lifelong optional attendance
- Complementary to clinical care
Group psychotherapy
- Professionally led
- Clinical records and goals
- Selected membership
- Time-limited episode
CM
- Verified contingent reinforcement
- Protocolised schedule
- Time-limited intensive phase
- Not unstructured cash gifts
Exam traps
- AA = TSF (false)
- CM = bribery (false framing)
- Peer groups replace MOUD (dangerous)
- Pamphlet = intensive referral (false)
Investigations and verification
Abstinence-targeted CM depends on objective verification — typically urine drug screening or oral fluid two to three times weekly during the active protocol for stimulant targets; breath alcohol or EtG where alcohol is the target. Attendance-only CM is weaker for use outcomes but can support engagement when toxicology is impractical; state the limitation.[4][5][8] Mutual-help itself needs no laboratory work; process metrics include self-reported meeting frequency, sponsorship, and retention weeks.[12]
Acute management
Post-detox or post-overdose windows are high-yield for warm handoff: schedule a specific meeting, problem-solve transport, introduce a peer recovery worker if available, and consider starting CM when a verifiable target exists. Passive “here is a list” referral underperforms intensive facilitation approaches emphasised in the mutual-help policy literature.[12][1]
If a CM urine is positive: withhold that session’s reinforcer per protocol, apply schedule reset if designed that way, maintain alliance, and escalate clinical review — do not convert CM into a shaming tribunal.[4][6]
Definitive management
Mutual-help and twelve-step facilitation
The 2020 Cochrane review by Kelly, Humphreys, and Ferri concluded that AA and other 12-step programmes, and TSF treatments designed to increase AA participation, produce rates of continuous abstinence that are at least as high as other established treatments and higher in some comparisons, with AA free of charge at the point of use — a public-health advantage when retention in recovery support is the goal.[1][2] Project MATCH found broadly comparable posttreatment drinking outcomes across TSF, CBT, and MET, with limited support for the a priori matching hypotheses that dominated the design era.[3]
Clinical practice. Offer TSF-style or intensive referral for AUD when abstinence-oriented peer support fits; always offer secular alternatives (e.g. SMART Recovery) when spiritual language is unacceptable. Family members may benefit from Al-Anon/Nar-Anon. Dual-diagnosis patients need explicit affirmation that psychotropic medications are compatible with recovery for most people — challenge anti-medication myths without attacking the fellowship wholesale.[12][14][15]
Contingency management protocols
Examiners want named protocol elements, not the word “incentives.” Core features synthesised across CM meta-analyses and classic behavioural trials include an objective target (e.g. stimulant-negative urine), frequent monitoring (often 2–3 times weekly), an immediate reinforcer when the target is met, escalating magnitude for consecutive successes, reset after a failed test in many designs, and a time-limited intensive phase (commonly about 8–16 weeks) followed by maintenance planning.[4][5][7][8]
Evidence spine. Prendergast and colleagues’ meta-analysis supports CM across substance use disorders.[4] Lussier and colleagues quantify voucher-based reinforcement therapy benefits and moderators (immediacy, magnitude).[5] Benishek and colleagues support prize-based CM as an efficacious lower-cost variant.[6] Higgins’ early behavioural cocaine work established the abstinence-verification plus escalating voucher tradition.[7] Roll and colleagues demonstrated multi-site CM efficacy for methamphetamine use disorders.[8] Dutra’s psychosocial meta-analysis is often quoted for the comparatively large effect-size signal of CM among psychosocial packages, especially for abstinence during treatment.[10]
CM with opioid agonist treatment. Bolívar and colleagues’ systematic review and meta-analysis found CM improves end-of-treatment outcomes among patients receiving medication for opioid use disorder — critical for stimulant co-use and retention adjuncts. CM supplements MOUD; it does not replace methadone or buprenorphine.[9]
Integration. Pair CM and mutual-help with MI/CBT, anti-craving medication where indicated (see anti-craving topic), housing, and family work. COMBINE reminds alcohol services that structured behavioural platforms and medications are complementary, not rival silos.[16][10]
Subtypes and scenarios
Alcohol. AA/TSF high-yield; quote Cochrane 2020 and MATCH main-effects literacy; SMART if secular preference.[1][3][15]
Stimulants/methamphetamine. CM is among the strongest behavioural options; multi-site methamphetamine CM evidence (Roll) and psychosocial syntheses (Dutra) are viva currency.[8][10]
Opioids. Prioritise agonist/partial-agonist treatment; add CM for co-stimulant use or attendance; NA/mutual-help as recovery capital, not MOUD substitute.[9][11]
Youth, perinatal, custody. Adapt mutual-help access and incentive programmes with safeguarding, consent, and continuity at prison release.[12]
Complications and pitfalls
Other traps: delaying rewards until end of month (kills contingency); using CM as punishment theatre; prize CM without gambling assessment; ending CM with no mutual-help or CBT aftercare so effects decay; cultural mismatch when only classic AA is offered; ignoring women’s safety and childcare barriers to evening meetings.[4][5][15]
Prognosis and disposition
Greater mutual-help involvement associates with better long-term abstinence outcomes in the synthesised AA/TSF literature and observational recovery research; CM effects are typically strongest while reinforcement is active, so plan maintenance (natural reinforcers, continued meetings, skills practice).[1][2][4][14] Disposition ladder: brief advice and directory (weak) → intensive mutual-help linkage ± CM in outpatient care → intensive outpatient/residential when environment overwhelms → always protect MOUD continuity for OUD.[9][11]
Special populations
Dual diagnosis. Affirm medications; dual-recovery groups where available; do not force pure 12-step language if it threatens engagement.[12] Indigenous and culturally diverse communities. Prefer culturally safe peer pathways alongside or instead of default fellowships.[15] Women and LGBTQ+ people. Women-only or affirming meetings; trauma-informed peer spaces. Older adults. Transport and sensory access. Family. Al-Anon/Nar-Anon as adjunct for concerned others.[12][14]
Regional deltas
Australian alcohol and other drug services historically under-deliver formal CM at scale despite stimulant burden; mutual-help (AA/NA/SMART) is widely available in metropolitan areas with patchier rural access. RANZCP addiction competence expects psychosocial literacy including peer support and behavioural reinforcement principles. Local prize or voucher programmes may be constrained by funding rules — name the evidence even when implementation is incomplete.[8][10][12]
Evidence, guidelines, and controversies
Name at viva: Kelly/Humphreys/Ferri Cochrane 2020 and distillation paper; Project MATCH; Prendergast CM meta-analysis; Lussier voucher meta-analysis; Benishek prize CM; Higgins cocaine behavioural trials; Roll methamphetamine CM; Bolívar CM+MOUD; Dutra psychosocial synthesis; Humphreys self-help policy; Moos active ingredients; Kaskutas AA science; Zemore non-12-step mutual help; McLellan chronic illness; COMBINE behavioural platform context.[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16]
Controversies for balanced answers. Spirituality vs secular recovery; whether CM “pays people not to use”; durability after reinforcement ends; underfunding of CM despite effect sizes; quality variation across mutual-help meetings; anti-medication subcultures in some peer spaces (address without dismissing free recovery capital).[1][4][14][15]
Exam pearls
REWARD
Self-test: five viva openers
References
- [1]Kelly JF, Humphreys K, Ferri M Alcoholics Anonymous and other 12-step programs for alcohol use disorder Cochrane Database Syst Rev, 2020.PMID 32159228
- [2]Kelly JF, Abry A, Ferri M, Humphreys K Alcoholics Anonymous and 12-Step Facilitation Treatments for Alcohol Use Disorder: A Distillation of a 2020 Cochrane Review Alcohol Alcohol, 2020.PMID 32628263
- [3]Project MATCH Research Group Matching Alcoholism Treatments to Client Heterogeneity: Project MATCH posttreatment drinking outcomes J Stud Alcohol, 1997.PMID 8979210
- [4]Prendergast M, Podus D, Finney J, Greenwell L, Roll J Contingency management for treatment of substance use disorders: a meta-analysis Addiction, 2006.PMID 17034434
- [5]Lussier JP, Heil SH, Mongeon JA, Badger GJ, Higgins ST A meta-analysis of voucher-based reinforcement therapy for substance use disorders Addiction, 2006.PMID 16445548
- [6]Benishek LA, Dugosh KL, Kirby KC, Matejkowski J, Clements NT, Seymour BL, et al. Prize-based contingency management for the treatment of substance abusers: a meta-analysis Addiction, 2014.PMID 24750232
- [7]Higgins ST, Budney AJ, Bickel WK, Hughes JR, Foerg F, Badger G Achieving cocaine abstinence with a behavioral approach Am J Psychiatry, 1993.PMID 8480823
- [8]Roll JM, Petry NM, Stitzer ML, Brecht ML, Peirce JM, McCann MJ, et al. Contingency management for the treatment of methamphetamine use disorders Am J Psychiatry, 2006.PMID 17074952
- [9]Bolívar HA, Klemperer EM, Coleman SRM, DeSarno M, Skelly JM, Higgins ST Contingency Management for Patients Receiving Medication for Opioid Use Disorder: A Systematic Review and Meta-analysis JAMA Psychiatry, 2021.PMID 34347030
- [10]Dutra L, Stathopoulou G, Basden SL, Leyro TM, Powers MB, Otto MW A meta-analytic review of psychosocial interventions for substance use disorders Am J Psychiatry, 2008.PMID 18198270
- [11]McLellan AT, Lewis DC, O'Brien CP, Kleber HD Drug dependence, a chronic medical illness: implications for treatment, insurance, and outcomes evaluation JAMA, 2000.PMID 11015800
- [12]Humphreys K, Wing S, McCarty D, Chappel J, Gallant L, Haberle B, et al. Self-help organizations for alcohol and drug problems: toward evidence-based practice and policy J Subst Abuse Treat, 2004.PMID 15063905
- [13]Moos RH Active ingredients of substance use-focused self-help groups Addiction, 2008.PMID 18269361
- [14]Kaskutas LA Alcoholics anonymous effectiveness: faith meets science J Addict Dis, 2009.PMID 19340677
- [15]Zemore SE, Lui C, Mericle A, Hemberg J, Kaskutas LA A longitudinal study of the comparative efficacy of Women for Sobriety, LifeRing, SMART Recovery, and 12-step groups for those with AUD J Subst Abuse Treat, 2018.PMID 29606223
- [16]Anton RF, O'Malley SS, Ciraulo DA, Cisler RA, Couper D, Donovan DM, et al. Combined pharmacotherapies and behavioral interventions for alcohol dependence: the COMBINE study: a randomized controlled trial JAMA, 2006.PMID 16670409