Psych · Addiction psychiatry — neonatal abstinence
Neonatal abstinence syndrome
Also known as NAS · NOWS · Neonatal opioid withdrawal syndrome · Neonatal drug withdrawal · Finnegan scoring · Eat Sleep Console · MOTHER trial neonatal outcomes
Exam-exhaustive fellowship reference on neonatal abstinence syndrome and neonatal opioid withdrawal syndrome — definition, epidemiology, mechanisms, Finnegan vs Eat-Sleep-Console assessment, non-pharmacologic care, opioid pharmacotherapy, maternal OAT implications (MOTHER/Suarez), differential diagnosis, breastfeeding, and non-punitive dyad care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
6 MCQs with explanations
Target exams
Red flags
Neonatal abstinence is a high-yield addiction–perinatal interface for FRANZCP MEQs and CASCs, MRCPsych papers, ABPN items, and MD/DNB vivas. Examiners test whether you can separate expected treatable withdrawal after OAT from moralised child-protection theatre, apply supportive care first, and name landmark evidence (MOTHER, Suarez, ESC, Kraft) under pressure.[1][10][12][13]
Overview and definition
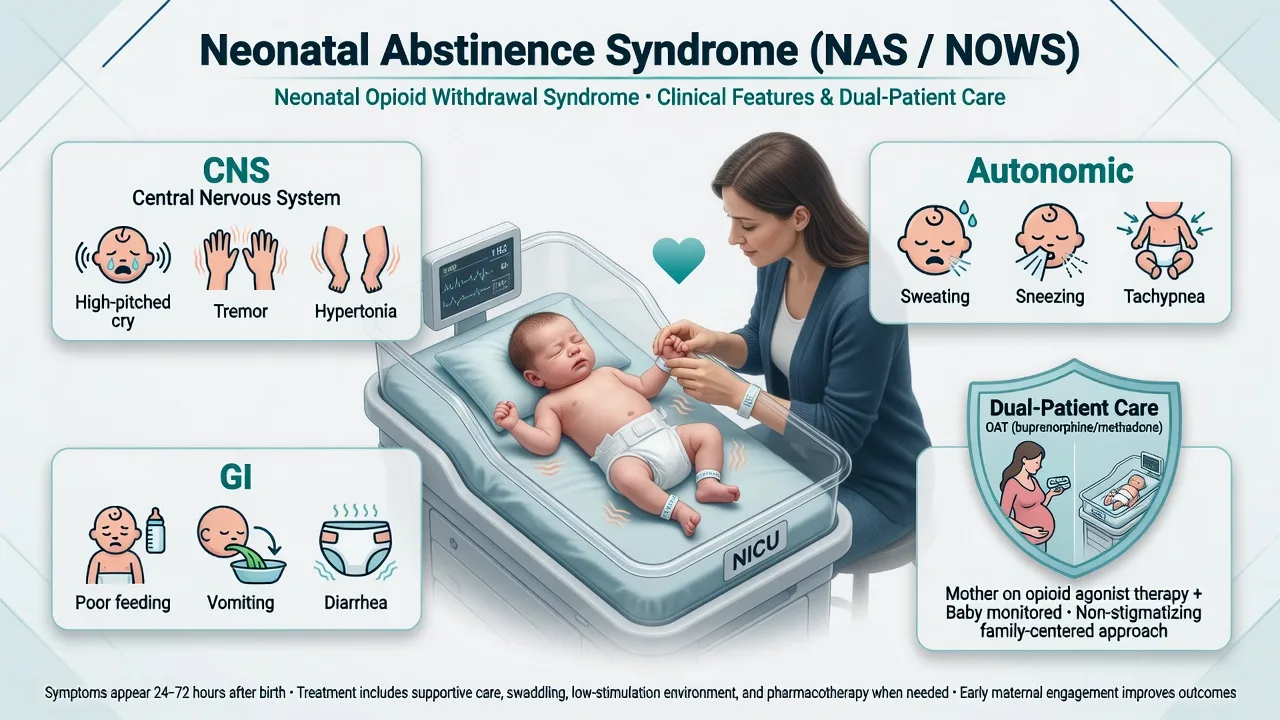
Neonatal abstinence syndrome (NAS) is a constellation of CNS, autonomic, and gastrointestinal signs after birth when fetal exposure to dependence-forming substances ends abruptly. Neonatal opioid withdrawal syndrome (NOWS) is the preferred contemporary term when the syndrome is primarily opioid-driven; AAP clinical guidance centres NOWS within the broader neonatal drug-withdrawal landscape.[2][3][10]
NAS is not the same construct as fetal alcohol spectrum disorder (FASD). FASD is a lifelong teratogenic neurodevelopmental spectrum; NAS/NOWS is an acute postnatal withdrawal state that is usually time-limited with supportive ± pharmacologic care.[3][9]
Critical exam frame: NAS after therapeutic maternal methadone or buprenorphine is expected and treatable. It is not, by itself, evidence that OAT was the wrong choice, nor automatic proof of child neglect. Maternal OAT remains first-line for opioid use disorder in pregnancy because forced detox risks maternal relapse, overdose, and obstetric harm.[1][14]
Classification and exposure map
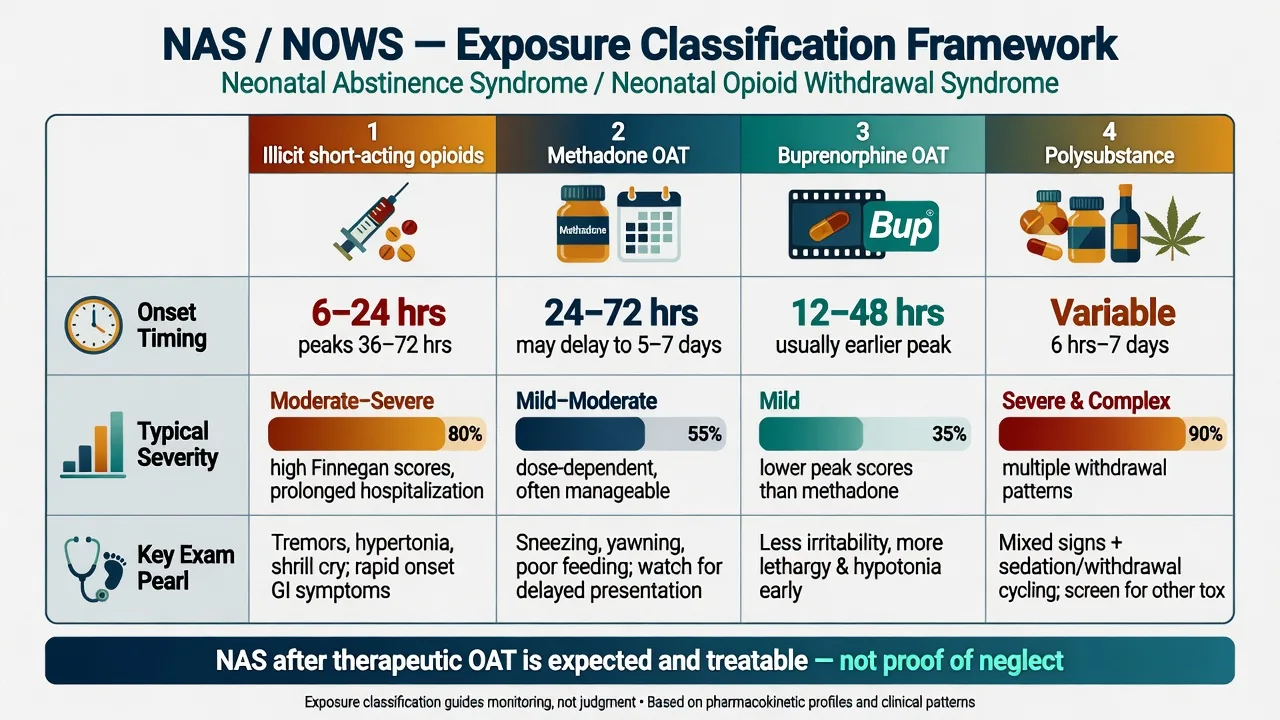
Short-acting opioids
- Heroin/fentanyl-type exposures
- Earlier onset often within 24–48 h
- Unregulated dosing and polysubstance common
- Maternal overdose/relapse risk high postpartum
Methadone OAT
- Long half-life; delayed peak often day 2–4+
- NAS more frequently treated than buprenorphine in MOTHER
- Do not force detox in pregnancy
- Observation window must match delayed risk
Buprenorphine OAT
- MOTHER: less neonatal morphine, shorter stay vs methadone
- Suarez cohort: favourable neonatal outcomes at scale
- Maternal retention/choice still decisive
- Partial agonist pharmacology for the dyad
Polysubstance modifiers
- Benzodiazepines prolong/complexify withdrawal
- SSRIs: poor neonatal adaptation overlap
- Nicotine increases autonomic irritability
- Alcohol → FASD pathway is separate
Epidemiology and risk
Headline NAS facts
Surveillance systems in high-income countries documented substantial increases in NAS diagnoses and NICU resource use over the 2000s–2010s, tracking the maternal opioid epidemic and expanded recognition/coding.[4][5][11] Hirai and colleagues linked NAS with maternal opioid-related diagnoses across US hospital data from 2010–2017, underscoring a dual maternal–neonatal public-health burden.[11]
Severity is imperfectly predicted by maternal OAT dose alone. Modifiers include polysubstance use, tobacco, gestational age, delayed prenatal care, and the care model (rooming-in and parental presence reduce escalation needs in QI and trial settings).[3][6][9] Equity requires culturally safe, non-punitive pathways — especially for Indigenous, rural, and justice-involved families — without stereotyping communities as the causal problem.[10][14]
Pathophysiology
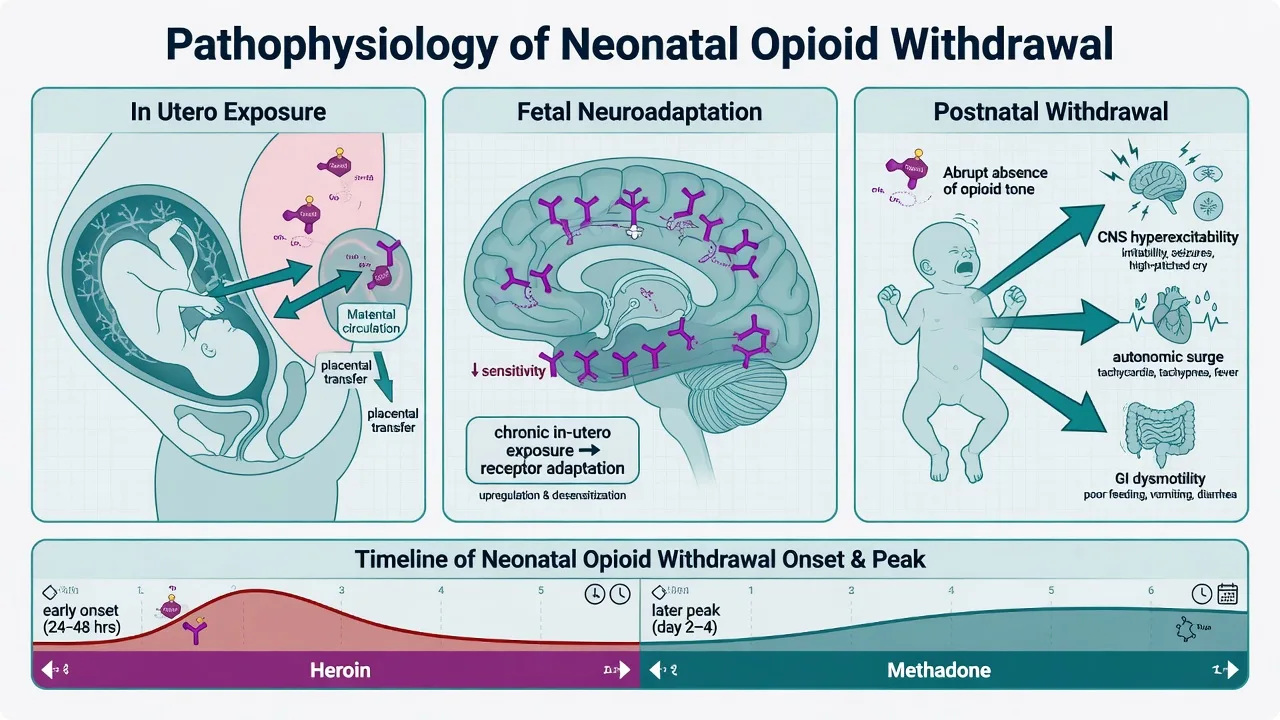
Opioids cross the placenta. Sustained fetal exposure produces neuroadaptation in endogenous opioid and linked monoamine systems. At birth, opioid input ceases while receptors remain adapted, yielding CNS hyperexcitability, autonomic dysregulation, and gastrointestinal hypermotility — the three classic clinical domains.[2][3][9]
Onset timing tracks pharmacokinetics. Short-acting illicit opioids often declare within the first 1–2 days. Methadone-exposed infants may peak later (commonly into day 2–4 or beyond), which is why premature “social discharge” without observation planning is an examiner trap. Buprenorphine-exposed infants still need structured observation, though MOTHER neonatal burden was lower than with methadone.[1][2][3]
Non-opioid exposures modify phenotype: SSRI/SNRI poor neonatal adaptation, benzodiazepine sedative withdrawal, and nicotine-related irritability can coexist with true opioid withdrawal and must not be collapsed into a single moral narrative.[2][9][10]
Clinical presentation
CNS. High-pitched or excessive cry, irritability, tremors, hypertonia, exaggerated Moro, sleep fragmentation; seizures are uncommon but critical when present.[2][3]
Autonomic. Sweating, sneezing, yawning, mottling, temperature instability, tachypnoea, nasal stuffiness.[2][3]
Gastrointestinal. Poor coordination of suck–swallow, frantic non-nutritive sucking, vomiting, diarrhoea, poor weight gain, and diaper-area skin injury from loose stools.[2][3][9]
Dyad context. Maternal sleep deprivation, stigma, fear of child-protection involvement, and postpartum relapse risk run in parallel with neonatal care. Psychiatry’s job is often liaison: keep the mother on OAT, support bonding, and translate NAS as a medical problem to obstetric, paediatric, and statutory partners.[10][14]
Differential diagnosis
Sepsis / CNS infection
- Fever, lethargy, poor perfusion
- Never skip parallel work-up when atypical
- Antibiotics per protocol if indicated
- NAS does not exclude infection
Metabolic / endocrine
- Hypoglycaemia, hypocalcaemia
- Electrolyte crises from diarrhoea
- Thyrotoxicosis rare but considered
- Check glucose early
SSRI adaptation
- Timing often early
- Respiratory and tone changes
- History of antenatal SSRI key
- May coexist with opioid withdrawal
Iatrogenic NICU opioids
- Post-sedation taper in non-SUD exposures
- Different social narrative
- Same supportive ± taper skills
- Avoid stigma transfer
Assessment
History: substances (type, route, last use), OAT agent and verified dose, benzodiazepines, alcohol, tobacco, SSRIs, BBV status, antenatal care engagement, prior NAS-affected infants, housing, IPV, and child-protection context — framed non-punitively.[9][10][14]
Finnegan-type scoring (including MOTHER modifications) tallies CNS, metabolic/vasomotor/respiratory, and GI signs on a repeated schedule. Strengths: structured shared language. Limits: inter-rater variability and threshold-driven pharmacotherapy that can prolong hospitalisation when non-pharmacologic care is underused.[2][3][9]
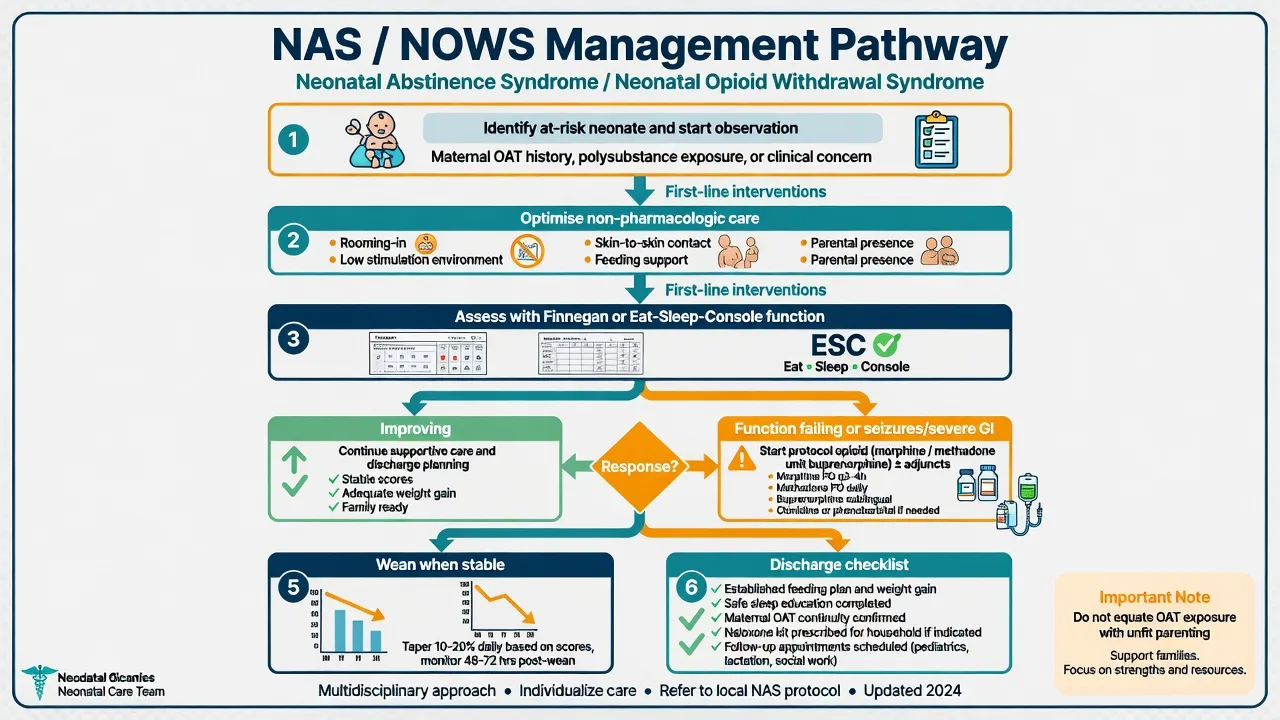
Eat, Sleep, Console (ESC) shifts the question from “how many signs?” to “can the infant eat effectively, sleep approximately one hour undisturbed, and be consoled within a short time?” Grossman and colleagues developed and disseminated this function-focused approach; the multicentre Young NEJM 2023 RCT found ESC shortened time until infants were medically ready for discharge compared with usual care, without a significant increase in specified adverse outcomes in the trial setting.[6][8][13]
Escalate urgently for seizures, severe dehydration, respiratory compromise, or failure of optimised supportive care.[2][10]
Investigations
Check glucose early in irritable or poorly feeding neonates. Add electrolytes, calcium, and septic evaluation when the course is atypical or systemic signs appear. Toxicology (urine, meconium, cord) can clarify exposures but has false positives/negatives and requires informed consent and a clinical purpose — not surveillance theatre that drives future care avoidance.[2][9][10]
EEG/imaging is for seizures, focal neurology, or atypical encephalopathy — not routine classic NAS. Confirm maternal OAT dose with the prescribing clinic rather than relying on self-report alone when planning observation length.[3][10]
Acute / emergency management
Severe GI losses need fluid and electrolyte resuscitation. Avoid oversedation from stacked sedatives while treating withdrawal. On the postnatal ward, maternal overdose is a separate emergency — protect the infant’s environment and continue non-punitive maternal overdose care with naloxone and OAT linkage as indicated.[9][14]
Definitive management
Non-pharmacologic care (default first-line)
Low sensory environment, swaddling, skin-to-skin, clustered cares, on-demand feeding (including breastfeeding when appropriate), and rooming-in with parental presence are the foundation. QI work by Grossman and colleagues showed that reorganising care around supportive measures and function can dramatically reduce morphine exposure and length of stay compared with historic Finnegan-threshold cultures.[6][8][9]
ESC operationalises this: maximise parental consoling and feeding support before concluding that medication is required.[8][13]
Pharmacotherapy
Start protocol opioids when optimised non-pharmacologic care fails or when severe features (e.g. seizures, intractable vomiting/diarrhoea with clinical compromise) demand it.[2][9][10]
Morphine (oral) remains a common first pharmacologic agent in many units. Teaching-range starting regimens are protocol-local (often on the order of approximately 0.03–0.1 mg/kg/dose orally every 3–4 hours, titrated to scores/function, then weaned). Exact unit protocols supersede any memorised single number — examiners want the principle of weight-based opioid replacement with structured weaning plus citation-aware safety.[2][3][9]
Methadone is an alternative opioid in some comparative neonatal protocols; selection is unit- and specialist-dependent.[9][10]
Buprenorphine (sublingual) for the neonate was studied by Kraft and colleagues (NEJM 2017): among term infants with NAS, sublingual buprenorphine reduced duration of treatment and length of hospital stay versus oral morphine in that trial setting — specialised pharmacy and monitoring required.[7]
Adjuncts (clonidine, phenobarbital) are used for refractory symptoms or polysubstance phenotypes under specialist protocols; they are not casual first-line add-ons.[2][3][9]
Maternal OAT choice and neonatal burden
The MOTHER randomised trial found that neonates exposed to buprenorphine required less morphine and had shorter hospital stays than methadone-exposed neonates, though maternal discontinuation was higher in the buprenorphine arm — individualise using retention, preference, and prior response.[1] Large observational data (Suarez NEJM 2022) also favour buprenorphine on several neonatal outcomes versus methadone at population scale, without overturning methadone as a valid, often necessary choice.[12] ACOG framing: treat maternal OUD with OAT; plan for neonatal monitoring rather than forced detox “to prevent NAS.”[14]
Breastfeeding and bonding
When the mother is stable on methadone or buprenorphine, not using illicit drugs, and HIV pathways allow, breastfeeding is generally encouraged and may reduce NAS severity and support bonding. Active illicit stimulant use, heavy alcohol intoxication, or other specific contraindications change the advice — specialist individualisation is required.[3][9][10]
Subtypes and high-yield scenarios
Methadone- vs buprenorphine-exposed. Use MOTHER/Suarez frames; still observe both; do not weaponise neonatal differences against a stable methadone patient.[1][12]
Polysubstance. Expect longer or more complex courses; watch benzodiazepine contribution; keep ESC/supportive care intensive.[2][9]
Preterm infants. Scoring tools are less validated; clinical judgment and neonatology leadership dominate.[10]
Iatrogenic NICU opioid taper. Same pharmacology of withdrawal without the maternal SUD stigma narrative — apply the same medical compassion.[2]
Child-protection interface. Report when statutory thresholds for harm/neglect are met; OAT exposure alone is not automatic removal. Collaborative safety planning beats covert urine “gotchas.”[10][14]
Complications and pitfalls
Prognosis and disposition
Most pharmacologically treated NAS resolves over days to a few weeks depending on protocol and severity; many infants never need opioids if supportive care is excellent.[6][9][13] Long-term neurodevelopment is confounded by polysubstance exposure, tobacco, poverty, and caregiving adversity — counsel honestly without deterministic doom narratives.[3][10]
Discharge checklist. Stable feeding and weight trajectory; parental competence with consoling; safe sleep; community maternal OAT appointment booked; take-home naloxone for households with overdose risk; contraception and maternal mental-health follow-up; early developmental surveillance plan.[9][10][14]
Special populations and regional deltas
Neonatal units use local NAS/NOWS protocols aligned with paediatric societies and hospital QI; psychiatry contributes perinatal addiction liaison, OAT continuity, culturally safe care for Aboriginal and Torres Strait Islander and Māori families, and non-punitive child-protection collaboration. Mother–baby units may support complex dual-diagnosis mothers when available.[10][14]
Evidence and guidelines
Name under pressure: Jones MOTHER 2010; Suarez 2022; Hudak AAP 2012; Patrick AAP NOWS 2020; Kocherlakota 2014; Wachman JAMA 2018; Tolia/Patrick/Hirai epidemiology; Grossman QI 2017 and ESC assessment 2018; Young ESC RCT 2023; Kraft neonatal buprenorphine 2017; ACOG CO 711.[1][2][3][4][5][6][7][8][9][10][11][12][13][14]
Exam pearls
NAS-CARE
Self-test: name the trials
MOTHER (Jones 2010): buprenorphine vs methadone in pregnancy — neonatal treatment burden lower with buprenorphine. Suarez 2022: large cohort reinforcing favourable neonatal outcomes with buprenorphine vs methadone. Kraft 2017: neonatal sublingual buprenorphine vs morphine for NAS treatment duration. Young 2023: ESC vs usual care — shorter time to medical readiness for discharge. Grossman QI: supportive-care redesign cuts morphine use and LOS.[1][6][7][12][13]
References
- [1]Jones HE, Kaltenbach K, Heil SH, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure N Engl J Med, 2010.PMID 21142534
- [2]Hudak ML, Tan RC; Committee on Drugs; Committee on Fetus and Newborn Neonatal drug withdrawal Pediatrics, 2012.PMID 22291123
- [3]Kocherlakota P Neonatal abstinence syndrome Pediatrics, 2014.PMID 25070299
- [4]Tolia VN, Patrick SW, Bennett MM, et al. Increasing incidence of the neonatal abstinence syndrome in U.S. neonatal ICUs N Engl J Med, 2015.PMID 25913111
- [5]Patrick SW, Davis MM, Lehmann CU, Cooper WO Increasing incidence and geographic distribution of neonatal abstinence syndrome: United States 2009 to 2012 J Perinatol, 2015.PMID 25927272
- [6]Grossman MR, Berkwitt AK, Osborn RR, et al. An Initiative to Improve the Quality of Care of Infants With Neonatal Abstinence Syndrome Pediatrics, 2017.PMID 28562267
- [7]Kraft WK, Adeniyi-Jones SC, Chervoneva I, et al. Buprenorphine for the Treatment of the Neonatal Abstinence Syndrome N Engl J Med, 2017.PMID 28468518
- [8]Grossman MR, Lipshaw MJ, Osborn RR, Berkwitt AK A Novel Approach to Assessing Infants With Neonatal Abstinence Syndrome Hosp Pediatr, 2018.PMID 29263121
- [9]Wachman EM, Schiff DM, Silverstein M Neonatal Abstinence Syndrome: Advances in Diagnosis and Treatment JAMA, 2018.PMID 29614184
- [10]Patrick SW, Barfield WD, Poindexter BB; Committee on Fetus and Newborn; Committee on Substance Use and Prevention Neonatal Opioid Withdrawal Syndrome Pediatrics, 2020.PMID 33106341
- [11]Hirai AH, Ko JY, Owens PL, Stocks C, Patrick SW Neonatal Abstinence Syndrome and Maternal Opioid-Related Diagnoses in the US, 2010-2017 JAMA, 2021.PMID 33433576
- [12]Suarez EA, Huybrechts KF, Straub L, et al. Buprenorphine versus Methadone for Opioid Use Disorder in Pregnancy N Engl J Med, 2022.PMID 36449419
- [13]Young LW, Ounpraseuth ST, Merhar SL, et al. Eat, Sleep, Console Approach or Usual Care for Neonatal Opioid Withdrawal N Engl J Med, 2023.PMID 37125831
- [14]American College of Obstetricians and Gynecologists Committee Opinion No. 711 Summary: Opioid Use and Opioid Use Disorder in Pregnancy Obstet Gynecol, 2017.PMID 28742670