Psych · Addiction psychiatry — nicotine and behavioural addictions
Nicotine and behavioural addictions
Also known as Tobacco use disorder · Nicotine dependence · Smoking cessation · Varenicline · NRT · Gambling disorder · Pathological gambling · Gaming disorder · Internet gaming disorder · Behavioural addiction
Exam-exhaustive fellowship reference on nicotine/tobacco use disorder (FTND, combination NRT, varenicline, bupropion, e-cigarettes, EAGLES, dual diagnosis with SMI), gambling disorder, and gaming/internet-use disorders (ICD-11 vs DSM-5-TR). FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Overview and definition
Nicotine dependence and behavioural (process) addictions sit on a shared conceptual axis of impaired control, craving, continued use despite harm, and functional decline, but they differ in legal product environments, mortality pathways, and the strength of the pharmacological evidence base.[18] Tobacco remains the highest-mortality addiction routinely encountered in general adult and dual-diagnosis psychiatry; gambling and gaming are the behavioural phenotypes most examinable at fellowship level.[11][21]
This topic covers three exam pillars in one place: (1) tobacco/nicotine use disorder — assessment, FTND, NRT, varenicline, bupropion, e-cigarettes; (2) gambling disorder; (3) gaming and related internet-use problems, framed carefully so candidates neither over-pathologise hobbies nor miss genuine disorder.[16][17]
Classification
Tobacco use disorder (DSM-5-TR) and nicotine in ICD-11
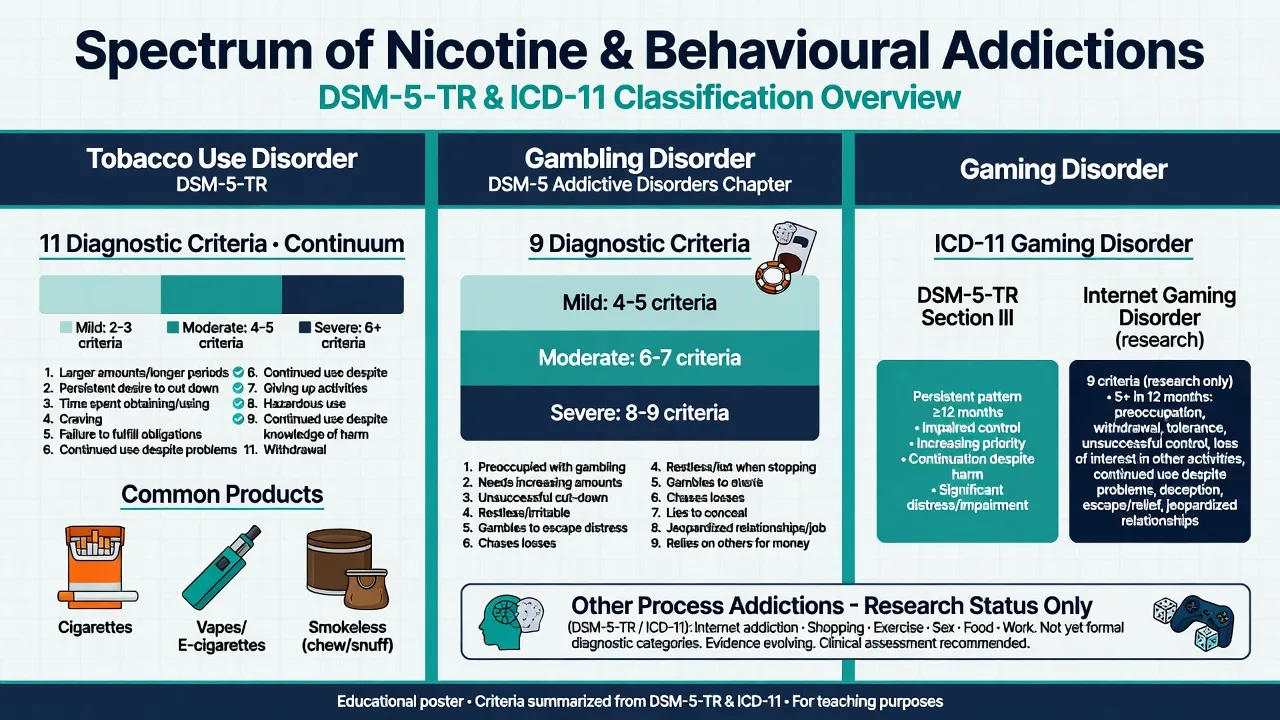
DSM-5-TR tobacco use disorder uses the standard 11 substance-use criteria over 12 months (or shorter if use is continuous), with severity mild 2–3, moderate 4–5, severe ≥6. Tolerance and withdrawal count when present; physiological dependence alone in someone only using NRT under medical direction is interpreted in clinical context. ICD-11 uses harmful pattern of use and dependence language for nicotine-containing products.[22]
Product class is not the disorder: cigarettes, roll-your-own, cigars, heated tobacco, nicotine vapes, and smokeless tobacco can all sustain dependence. Dual use (smoke + vape) is common during transitions.[20]
Gambling disorder
DSM-5 moved gambling disorder into Substance-Related and Addictive Disorders — a classic nosology pearl. Diagnosis requires ≥4 of 9 criteria in 12 months (preoccupation; escalating bets; unsuccessful cut-downs; restlessness/irritability when stopping; gambling to escape; chasing losses; lying; relationship/job/education jeopardy; reliance on others for money). Severity bands: mild 4–5, moderate 6–7, severe 8–9. ICD-11 also recognises gambling disorder with impaired control, increasing priority, and continuation despite consequences plus functional impairment.[11]
Gaming disorder and related constructs
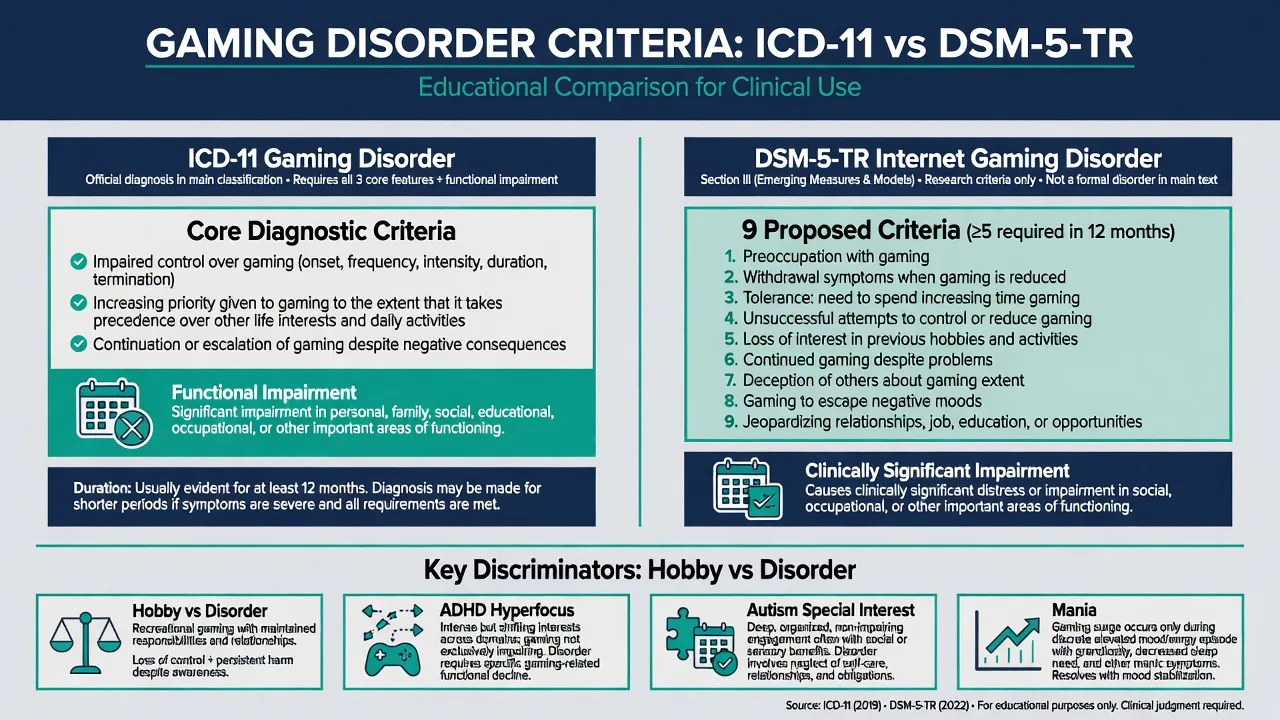
ICD-11 gaming disorder requires a persistent pattern of gaming behaviour characterised by impaired control, increasing priority given to gaming, and continuation despite negative consequences, with significant impairment, usually over ≥12 months (shorter if severe). DSM-5-TR Internet gaming disorder remains in Section III as a condition for further study (research criteria; often taught as ≥5 of 9 proposed items with impairment) — not equivalent to a fully settled main-text diagnosis in the same way as gambling.[16]
Other proposed process addictions (shopping, pornography, social media, “internet addiction” as a unitary diagnosis) remain research-contested; assess harm and comorbidity without forcing unvalidated labels.[17][18]
Epidemiology and risk factors
Tobacco kills on a population scale; among people with severe mental illness (SMI), smoking prevalence is several-fold higher than the general population and contributes substantially to the 10–25 year mortality gap via cardiovascular and cancer pathways.[21] Risk factors for nicotine dependence include early initiation, parental modelling, lower socioeconomic status, concurrent substance use, and untreated mental illness.[21]
Gambling disorder lifetime prevalence is lower than nicotine dependence but concentrates severe financial, forensic, and suicide harm; men historically show higher rates for many traditional gambling forms, while online products are reshaping sex and age patterns.[11] Gaming problems concentrate in adolescents and young adults, with elevated comorbidity of ADHD, autism spectrum traits, depression, and anxiety; East Asian clinical recognition preceded wider ICD-11 adoption debates.[16]
Pathophysiology
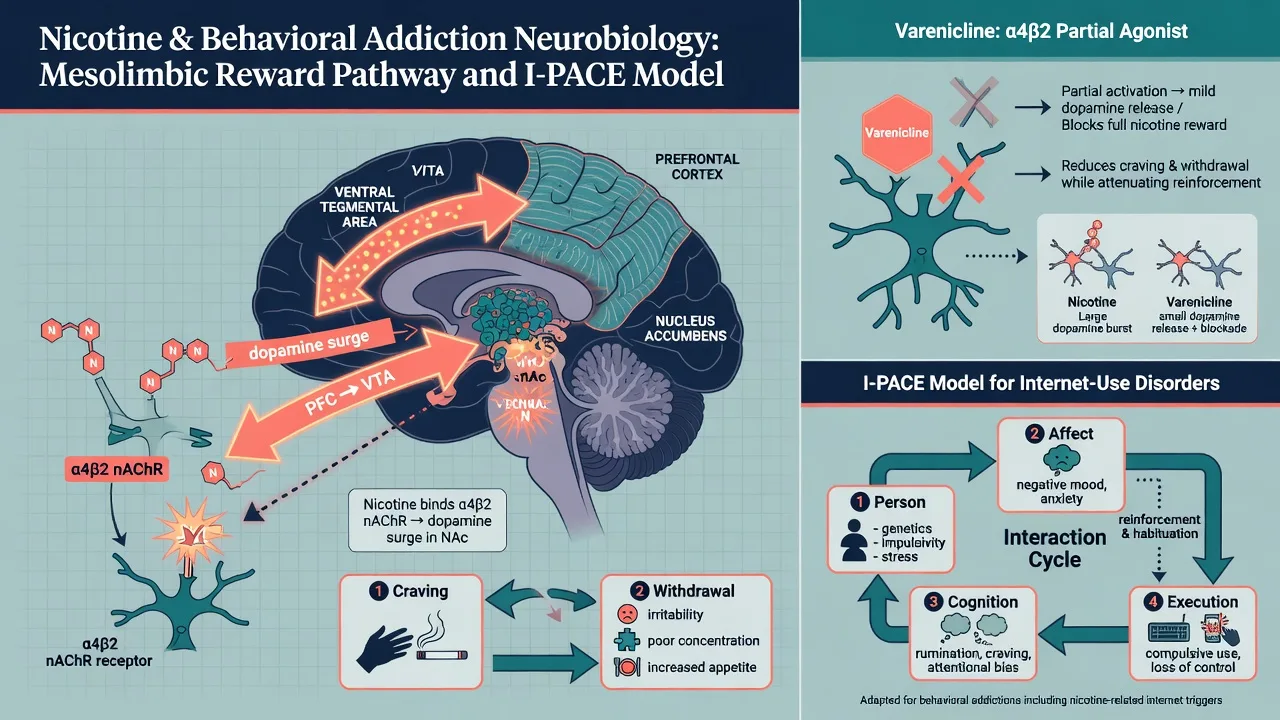
Nicotine binds α4β2 nicotinic acetylcholine receptors, driving mesolimbic dopamine release (ventral tegmental area → nucleus accumbens) that encodes reinforcement and cue learning. Chronic exposure produces tolerance and a withdrawal syndrome of irritability, anxiety, poor concentration, increased appetite, and intense craving — often misread on wards as “personality” or primary anxiety.[5][22]
Varenicline is an α4β2 partial agonist: partial receptor activation reduces withdrawal while concurrent occupancy blocks full nicotine reward if the person smokes.[2][5] Bupropion aids cessation via noradrenergic/dopaminergic effects and nicotinic antagonist properties; its antidepressant profile is secondary for the cessation indication but clinically useful when depression coexists.[8]
Behavioural addictions engage overlapping reward, salience, habit, and prefrontal control networks without an exogenous drug. The I-PACE model (Interaction of Person–Affect–Cognition–Execution) organises how predisposing traits, affective triggers, cognitive biases, and executive failure maintain specific internet-use disorders.[17] Gambling urge circuitry also implicates endogenous opioid signalling — the rationale for naltrexone trials, not proof that every patient needs an opioid antagonist.[10][13]
Clinical presentation
Nicotine
Daily smoking with early morning use, failed quit attempts, and cue-triggered craving is typical. Withdrawal peaks in the first few days of abstinence and drives early relapse; alcohol, stress, and other smokers are classic precipitants.[22] Vaping-predominant patterns may show lower carbon monoxide but still high nicotine delivery and dependence.
Gambling
Core phenomenology: chasing losses, escalating bets, concealment from family, borrowing or theft, relationship collapse, and occupational failure. Suicidal ideation often clusters with catastrophic debt disclosure.[11] Electronic gaming machines and continuous online sports betting provide high-frequency reinforcement schedules.
Gaming
Loss of control over onset/frequency/intensity/duration, prioritisation of gaming over school/work/sleep/hygiene, continuation despite failing grades or family conflict, and irritability when access is limited. Night-time play with circadian collapse is common in severe presentations.[16]
Dual diagnosis patterns
Smoking with schizophrenia or bipolar disorder is the rule more than the exception in many clinics; self-medication hypotheses do not justify withholding treatment.[14][15][21] Gambling may surge in mania or with stimulant use; gaming harm often co-travels with ADHD or social anxiety.
Differential diagnosis
| Presentation | More like disorder when… | Discriminator / alternative |
|---|---|---|
| Heavy smoking | Loss of control, withdrawal, failed cut-downs, role harm | Occasional social smoking without criteria |
| Recreational gambling | Chasing, bailouts, concealment, impairment | Entertainment spending within means |
| Heavy gaming | Impaired control + priority + continuation despite harm | Healthy hobby; ADHD hyperfocus; autism interest; mania episode only |
| Irritability on ward | Temporal link to nicotine deprivation | Akathisia, delirium, primary mood/psychosis relapse |
| New gambling in older adult | Temporal link to dopamine agonist start/increase | Primary late-onset gambling disorder still possible but screen meds |
Clinical and bedside assessment
Tobacco
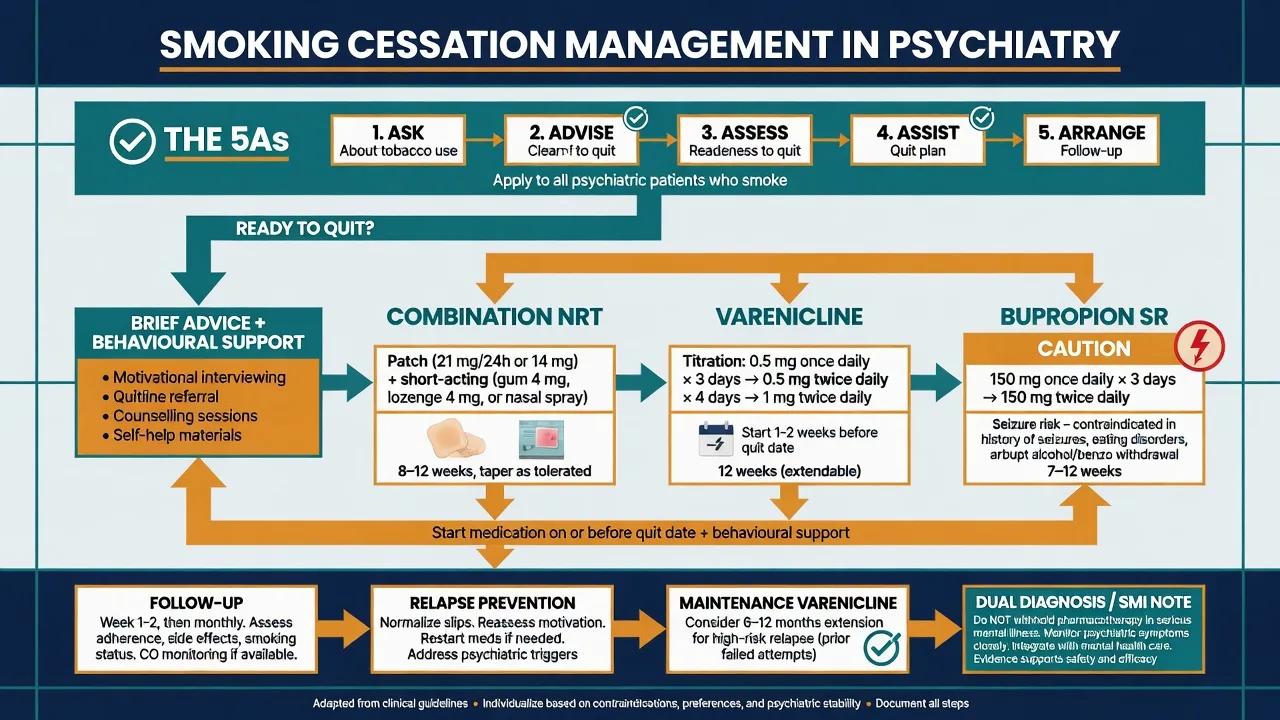
Use the 5As: Ask, Advise (clear personalised message), Assess readiness, Assist (plan + pharmacotherapy), Arrange follow-up. Brief physician advice increases quit rates even without intensive programmes.[19]
Fagerström Test for Nicotine Dependence (FTND) items include cigarettes per day and time to first cigarette (≤5 minutes = high dependence marker), among others; the Heaviness of Smoking Index uses the two strongest items when time is short.[9] Record prior pharmacotherapy, psychiatric stability, seizure history, pregnancy, and concurrent substances. Exhaled CO or cotinine can verify abstinence when needed.
Gambling
Map forms (EGMs, sports, casino, online, lottery), frequency, net losses, debt structure, illegal acts, and family impact. Screen suicide risk at first contact when debt crisis is present. Collateral from partners often reveals concealment. Outcome measures such as urge scales (e.g. G-SAS concept) support monitoring more than one-off diagnosis.[11]
Gaming and internet use
Hours alone are insufficient — require functional impairment. Assess school/work, sleep, nutrition, aggression when limited, offline friendships, and other online behaviours. In youth, include parents and school; assess capacity and safeguarding when neglect or violence risk appears.[16]
Investigations
Laboratory work is sparse compared with alcohol or opioids. Consider exhaled CO / cotinine for verification when results change management; before bupropion, document seizure history, eating disorder, abrupt sedative/alcohol withdrawal risk, and interacting drugs that lower seizure threshold; and use a metabolic and cardiovascular risk panel in SMI smokers (BP, glucose, lipids) as physical health parity — not as a barrier to cessation meds. Neuroimaging is reserved for organic differential (e.g. frontotemporal change, new late behavioural disinhibition).[8][21]
Management — resuscitation and acute care
Pure nicotine withdrawal is uncomfortable, not a classic ABC emergency. Priorities shift when suicide or violence risk accompanies gambling debt crisis or SMI decompensation (standard psychiatric emergency pathways and safety planning); when inpatient smoke-free settings require NRT on arrival rather than after conflict escalates; when rare nicotine liquid ingestion (children) presents as medical toxicology; and when acute mania or psychosis drives reckless gambling/gaming — treat the primary syndrome while containing access and finances.[11][21][22]
Management — definitive and stepwise
Behavioural support for smoking
Combine advice + structured behavioural support (counselling, quitline, practical coping plans) with pharmacotherapy whenever possible. Practical strategies for the struggling smoker include addressing high-risk situations, arranging early follow-up, and treating under-dosed NRT as a fixable error rather than “patient failure”.[19][22]
Nicotine replacement therapy (NRT)
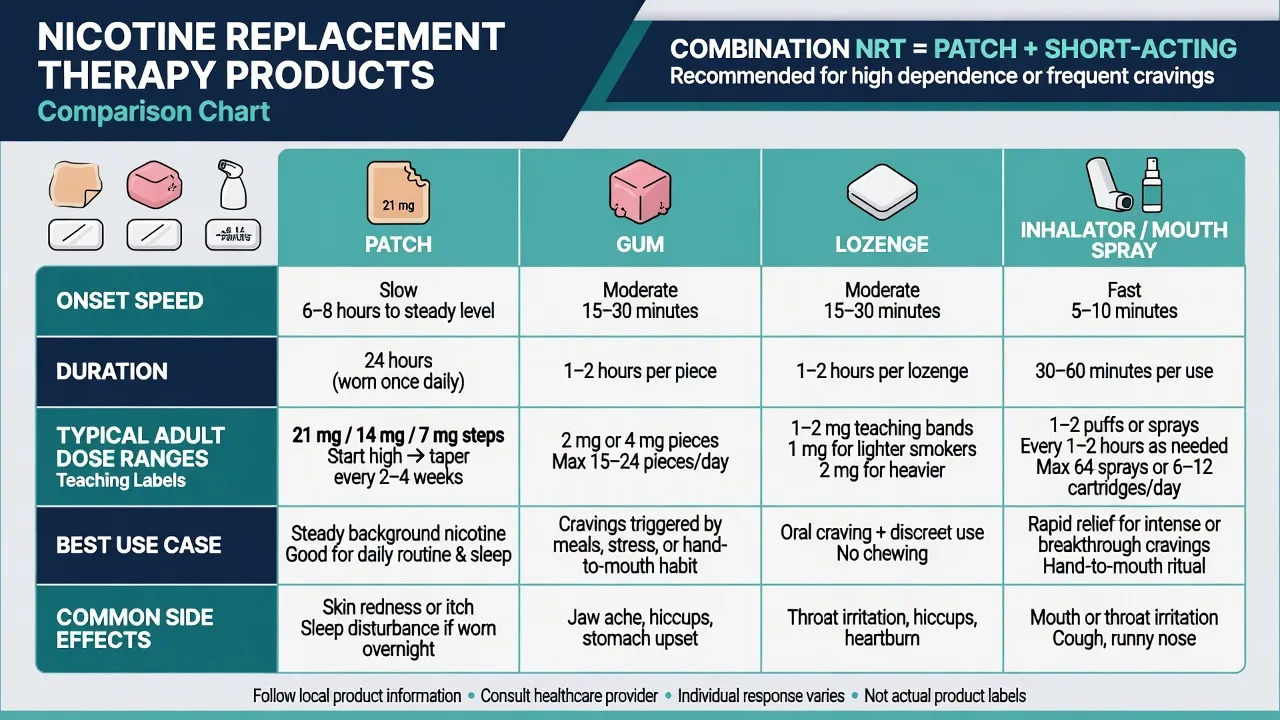
Combination NRT (long-acting patch plus short-acting gum/lozenge/inhalator/spray for breakthrough craving) outperforms single-form NRT for many dependent smokers; higher-dose and longer-duration strategies are supported in systematic review for selected patients.[6][7]
Teaching-level adult patterns (always confirm local product information): Patch commonly 21 mg/24 h (or 14 mg if lighter smoker) for several weeks, then step down to 14 mg then 7 mg, with a typical course often 8–12 weeks, individualised; gum 2 mg or 4 mg (higher for more dependent smokers), chewed with “park” technique, with usual maxima in product labels (often taught around 15–24 pieces/day — follow label); lozenge 1–2 mg bands by dependence (allow to dissolve, do not chew); mouth spray / inhalator for rapid breakthrough craving relief within labelled maximum daily uses. Under-dosing and stopping at the first slip are common pitfalls.[7][22]
Varenicline
Landmark RCTs showed superior continuous abstinence versus placebo and advantages versus bupropion SR in phase 3 programmes.[2][3] Standard adult titration (confirm label): 0.5 mg once daily for 3 days → 0.5 mg twice daily for 4 days → 1 mg twice daily; start 1–2 weeks before the quit date when feasible; usual initial course 12 weeks. Maintenance varenicline for an additional period can reduce relapse among abstainers.[4][5]
EAGLES (Anthenelli et al., Lancet 2016) found that in smokers with and without psychiatric disorders, varenicline and bupropion did not show significantly increased moderate-to-severe neuropsychiatric adverse events versus nicotine patch or placebo on the primary composite endpoint, while confirming varenicline’s efficacy advantage — the key modern answer to post-marketing scare-era exam stems.[1] Nausea, sleep disturbance, and vivid dreams are common; monitor mood and suicidality as good psychiatric practice for any cessation attempt, not as a unique absolute contraindication narrative divorced from EAGLES.
Bupropion SR
Bupropion is an evidence-based cessation aid (Cochrane antidepressants review).[8] Teaching schedule often: 150 mg once daily for 3 days, then 150 mg twice daily (at least 8 hours apart), start 1–2 weeks before quit date, continue 7–12 weeks. Contraindications/cautions: seizure history, current or prior diagnosis of bulimia/anorexia nervosa, abrupt withdrawal from alcohol or benzodiazepines, monoamine oxidase inhibitor interactions, and other seizure-threshold risks. Combination with NRT is used in some pathways; blood pressure monitoring is prudent.
Electronic cigarettes
Cochrane evidence supports that nicotine e-cigarettes can help more people quit smoking than NRT in randomised comparisons, with ongoing monitoring of adverse events.[20] Fellowship viva stance: discuss as a cessation tool with regulatory and youth-uptake caveats, dual-use risks, and region-specific policy (ANZ vs UK vs US differ). Do not market recreational youth vaping as harm reduction.
Regional deltas — tobacco treatment. ANZ: strong smoke-free culture; subsidised NRT/varenicline access varies by jurisdiction and PBS/Pharmac listing era — check current formulary; vaping regulation has been restrictive relative to some UK harm-reduction framing. UK: NICE and stop-smoking services often integrate e-cigarettes as a quit aid option alongside licensed medicines. US: FDA-approved meds (NRT, varenicline, bupropion); e-cigarette regulatory landscape fluid; youth prevention emphasis high. Always name the jurisdiction when quoting subsidy or legality.[20][22]
Gambling disorder treatment
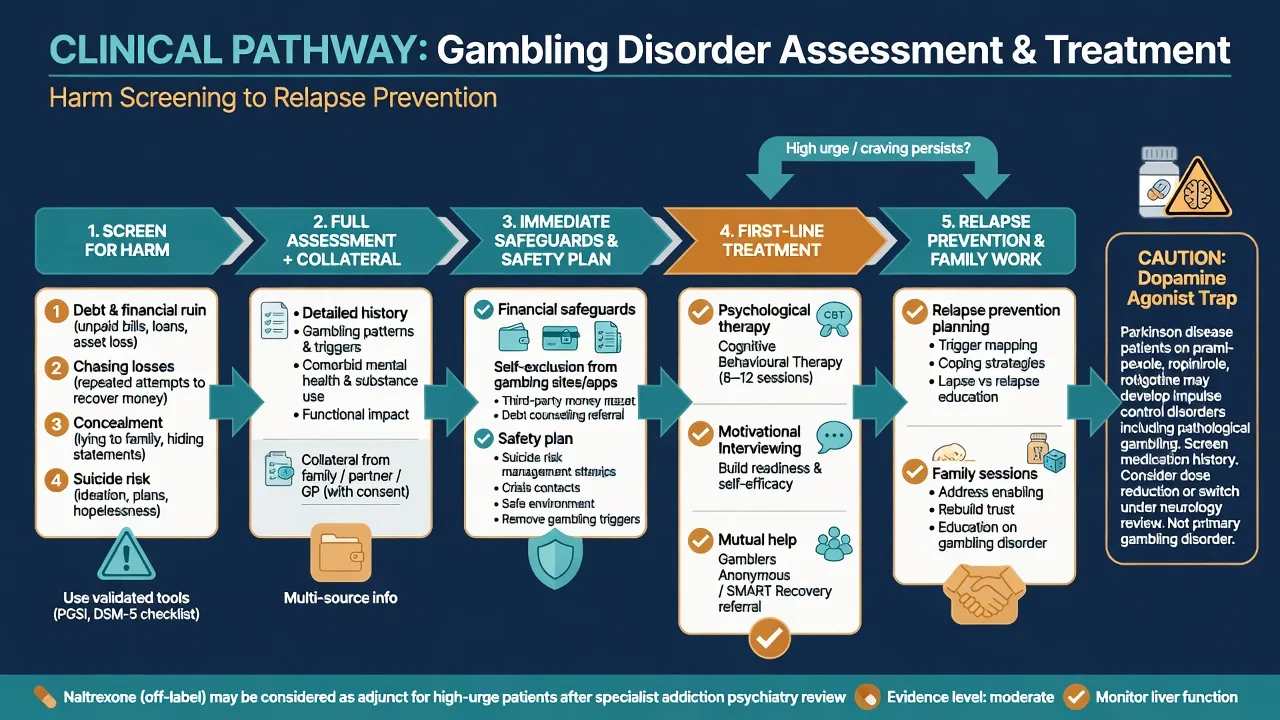
First-line care is psychological: CBT, motivational interviewing, and mutual-help (e.g. Gamblers Anonymous) with evidence summarised in Cochrane review of psychological therapies.[12] Immediate financial safeguards (self-exclusion, third-party money management, app blockers) and suicide safety planning are clinical interventions, not optional social work afterthoughts.[11]
Pharmacotherapy is second-line/adjunctive. A double-blind trial of naltrexone reduced gambling urges versus placebo in selected patients; Cochrane review of pharmacological interventions for disordered gambling finds overall evidence limited and heterogeneous — do not present naltrexone as mandatory first-line monotherapy.[10][13] Typical off-label teaching discussion: oral naltrexone after excluding contraindications (acute hepatitis, current opioid use), specialist supervision, and integrated psychosocial care. SSRIs may treat comorbid depression/anxiety without being proven anti-gambling specifics.
Gaming and internet-use problems
Treat functional collapse with CBT-informed approaches, family interventions, school re-engagement, sleep restoration, and treat comorbidity (ADHD, depression, anxiety, autism support needs).[16][17] Digital curfews and device limits work better inside a collaborative plan than as pure punishment. There is no high-quality “varenicline equivalent” for gaming; avoid inventing medication algorithms.
Specific subtypes and scenarios
Inpatient psychiatry and smoke-free wards
Implement smoke-free policy with same-day NRT offering, behavioural support, and discharge cessation planning. Withholding nicotine treatment is a quality failure and equity issue for SMI populations.[21]
Schizophrenia and bipolar smokers
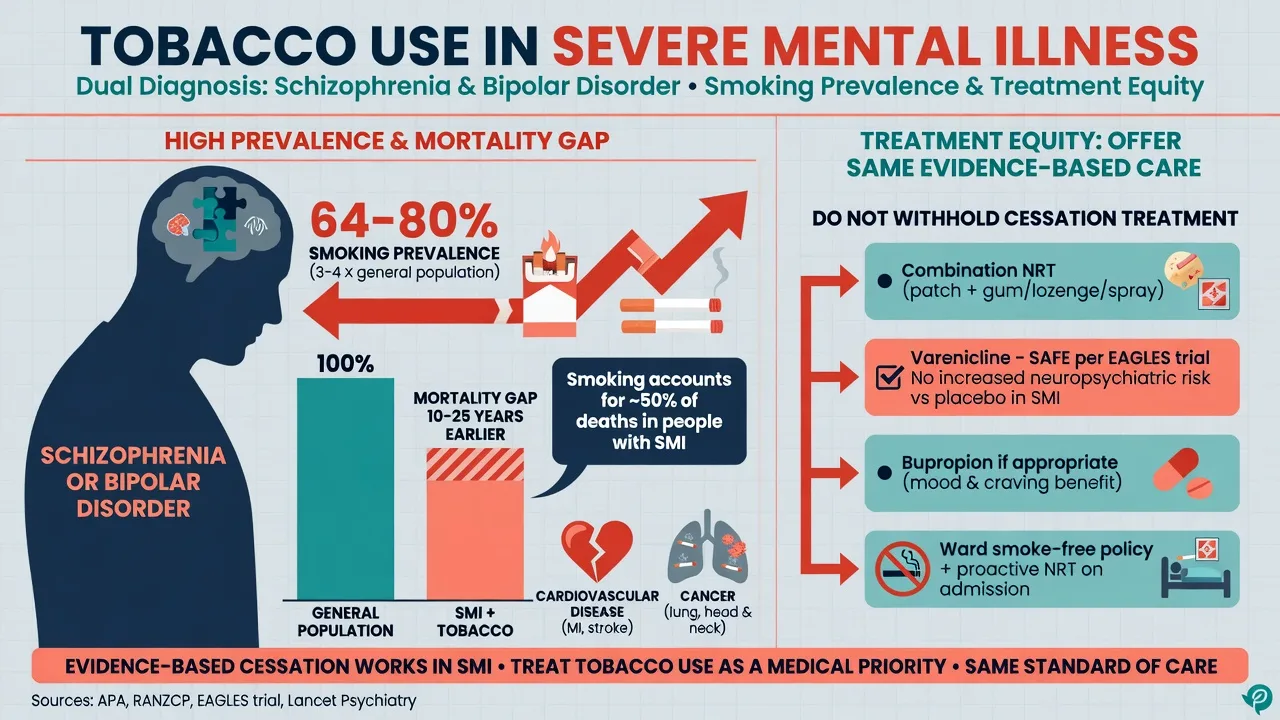
Do not refuse varenicline solely because of diagnosis. Cochrane review supports that cessation interventions can work in schizophrenia; specialist reviews outline multi-component strategies including high-intensity behavioural support and pharmacotherapy.[14][15] EAGLES included psychiatric cohorts and undercuts blanket neuropsychiatric prohibition narratives.[1] Watch clozapine levels if smoking status changes substantially (induction via polycyclic aromatic hydrocarbons in smoke, not nicotine per se — exam pearl).
Pregnancy
Highest-intensity behavioural support; NRT if a woman cannot stop unassisted, under specialist advice and informed consent; avoid casual use of varenicline/bupropion without contemporary guideline review. Fetal and maternal benefit of cessation is substantial.[19][22]
Online sports betting and youth gaming
Rapid continuous reinforcement, credit products, and 24/7 access escalate harm. Assess debt instruments and family financial abuse risk. For adolescents, involve carers and education systems early.[11][16]
Complications and pitfalls
- Varenicline fear without EAGLES literacy — outdated absolute avoidance stems.[1]
- Bupropion in seizure-risk contexts.[8]
- Patch-only under-dosing in heavy smokers who need combination NRT.[7]
- Bailout collusion in gambling without structure, or ignoring suicidality.[11]
- Missing dopamine agonist-induced ICD (pramipexole, etc.).
- Moral panic gaming without impairment, or missing mania/ADHD. [11][16][18]
Prognosis and disposition
Most smokers cycle through multiple quit attempts; each assisted attempt can succeed. Maintenance pharmacotherapy and early follow-up reduce relapse.[4][22] Gambling is often chronic-relapsing; early help-seeking and debt restructuring improve trajectory.[11] Disposition ladder: GP shared care and quitline → addiction psychology/psychiatry → dual-diagnosis services → inpatient only for psychiatric risk or inability to keep safe. Harm-reduction interim goals (cut-down, temporary NRT, smoke-free home, gambling blockers) are valid when full abstinence is not yet achievable.[11][22]
Special populations
Youth need attention to vaping dependence, school policies, parental consent frameworks, and developmental gaming assessment; older adults still gain cardiovascular benefit from quitting and need polypharmacy/dopamine-agonist review; Indigenous and culturally diverse communities require distinction between ceremonial tobacco practices and commercial dependence with culturally safe cessation programmes; intellectual disability / forensic settings need accessible NRT and simplified behavioural support within environmental smoking cultures; pregnancy/lactation prioritises highest-intensity behavioural care first with specialist product advice.[11][16][19][21]
Evidence, guidelines, and controversies
Stronger evidence base
- Varenicline RCTs (Gonzales, Jorenby) and maintenance (Tonstad)
- EAGLES neuropsychiatric safety and efficacy
- Cahill network meta and partial-agonist Cochrane
- NRT form/dose Cochrane; brief advice; bupropion Cochrane
Weaker / evolving evidence
- Naltrexone and other drugs for gambling (selected trials; Cochrane limited)
- Gaming pharmacotherapy algorithms
- Unitary internet addiction as a formal diagnosis
- Long-term population effects of e-cigarettes vs youth uptake trade-offs
Guideline posture (principles; verify local documents): RANZCP / NICE / APA all support active tobacco treatment in psychiatric populations; NICE and some UK services are more explicit on e-cigarettes as quit aids than some ANZ policy eras; gambling care emphasises psychosocial first-line with specialist addiction input for complex dual diagnosis.[12][20][21]
Exam pearls
5As of smoking care
5As
Identify tobacco use every clinical encounter
Clear, personalised advice to quit
Readiness, dependence (FTND), prior attempts
Behavioural support + NRT/varenicline/bupropion plan
Follow-up, relapse support, community quitline
- Time to first cigarette ≤5 minutes ≈ high dependence (FTND).[9]
- Combination NRT for heavy smokers; do not under-dose.[7]
- Varenicline titration to 1 mg BD; start before quit date; maintenance option.[2][4]
- EAGLES is the neuropsychiatric safety talking point.[1]
- Do not withhold cessation meds in schizophrenia by diagnosis alone.[1][14]
- Smoking cessation can raise clozapine levels (smoke hydrocarbons, not nicotine patch).
- DSM-5 put gambling in addictive disorders; IGD is Section III research criteria; ICD-11 has gaming disorder.[11][16]
- Gambling first-line = psychosocial + money/safety, not naltrexone-first.[12][13]
- Screen dopamine agonists for new impulse-control behaviours.
- Ward ban without NRT is poor practice.[21]
References
- [1]Anthenelli RM, Benowitz NL, West R, St Aubin L, McRae T, Lawrence D, et al. Neuropsychiatric safety and efficacy of varenicline, bupropion, and nicotine patch in smokers with and without psychiatric disorders (EAGLES): a double-blind, randomised, placebo-controlled clinical trial Lancet, 2016.PMID 27116918
- [2]Gonzales D, Rennard SI, Nides M, Oncken C, Azoulay S, Billing CB, et al. Varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs sustained-release bupropion and placebo for smoking cessation: a randomized controlled trial JAMA, 2006.PMID 16820546
- [3]Jorenby DE, Hays JT, Rigotti NA, Azoulay S, Watsky EJ, Williams KE, et al. Efficacy of varenicline, an alpha4beta2 nicotinic acetylcholine receptor partial agonist, vs placebo or sustained-release bupropion for smoking cessation: a randomized controlled trial JAMA, 2006.PMID 16820547
- [4]Tonstad S, Tønnesen P, Hajek P, Williams KE, Billing CB, Reeves KR, et al. Effect of maintenance therapy with varenicline on smoking cessation: a randomized controlled trial JAMA, 2006.PMID 16820548
- [5]Cahill K, Lindson-Hawley N, Thomas KH, Fanshawe TR, Lancaster T Nicotine receptor partial agonists for smoking cessation Cochrane Database Syst Rev, 2016.PMID 27158893
- [6]Cahill K, Stevens S, Perera R, Lancaster T Pharmacological interventions for smoking cessation: an overview and network meta-analysis Cochrane Database Syst Rev, 2013.PMID 23728690
- [7]Theodoulou A, Chepkin SC, Ye W, Fanshawe TR, Bullen C, Hartmann-Boyce J, et al. Different doses, durations and modes of delivery of nicotine replacement therapy for smoking cessation Cochrane Database Syst Rev, 2023.PMID 37335995
- [8]Hughes JR, Stead LF, Hartmann-Boyce J, Cahill K, Lancaster T Antidepressants for smoking cessation Cochrane Database Syst Rev, 2014.PMID 24402784
- [9]Heatherton TF, Kozlowski LT, Frecker RC, Fagerström KO The Fagerström Test for Nicotine Dependence: a revision of the Fagerström Tolerance Questionnaire Br J Addict, 1991.PMID 1932883
- [10]Grant JE, Kim SW, Hartman BK A double-blind, placebo-controlled study of the opiate antagonist naltrexone in the treatment of pathological gambling urges J Clin Psychiatry, 2008.PMID 18384246
- [11]Hodgins DC, Stea JN, Grant JE Gambling disorders Lancet, 2011.PMID 21600645
- [12]Cowlishaw S, Merkouris S, Dowling N, Anderson C, Jackson A, Thomas S Psychological therapies for pathological and problem gambling Cochrane Database Syst Rev, 2012.PMID 23152266
- [13]Dowling N, Merkouris S, Lubman D, Thomas S, Bowden-Jones H, Cowlishaw S Pharmacological interventions for the treatment of disordered and problem gambling Cochrane Database Syst Rev, 2022.PMID 36130734
- [14]Tsoi DT, Porwal M, Webster AC Interventions for smoking cessation and reduction in individuals with schizophrenia Cochrane Database Syst Rev, 2013.PMID 23450574
- [15]Evins AE, Cather C Effective Cessation Strategies for Smokers with Schizophrenia Int Rev Neurobiol, 2015.PMID 26472528
- [16]Petry NM, Rehbein F, Gentile DA, Lemmens JS, Rumpf HJ, Mößle T, et al. An international consensus for assessing internet gaming disorder using the new DSM-5 approach Addiction, 2014.PMID 24456155
- [17]Brand M, Young KS, Laier C, Wölfling K, Potenza MN Integrating psychological and neurobiological considerations regarding the development and maintenance of specific Internet-use disorders: An Interaction of Person-Affect-Cognition-Execution (I-PACE) model Neurosci Biobehav Rev, 2016.PMID 27590829
- [18]Grant JE, Potenza MN, Weinstein A, Gorelick DA Introduction to behavioral addictions Am J Drug Alcohol Abuse, 2010.PMID 20560821
- [19]Stead LF, Buitrago D, Preciado N, Sanchez G, Hartmann-Boyce J, Lancaster T Physician advice for smoking cessation Cochrane Database Syst Rev, 2013.PMID 23728631
- [20]Lindson N, Butler AR, McRobbie H, Bullen C, Hajek P, Begh R, et al. Electronic cigarettes for smoking cessation Cochrane Database Syst Rev, 2024.PMID 38189560
- [21]Williams JM, Ziedonis D Addressing tobacco among individuals with a mental illness or an addiction Addict Behav, 2004.PMID 15236808
- [22]Rigotti NA Strategies to help a smoker who is struggling to quit JAMA, 2012.PMID 23073954