Psych · Addiction psychiatry — substance use disorders
Opioid substitution therapy and withdrawal
Also known as Opioid agonist treatment · OAT · OST · MOUD · Methadone maintenance · Buprenorphine induction · Opioid withdrawal · COWS · Medication for opioid use disorder
Fellowship-depth leaf on opioid withdrawal and substitution: COWS staging, symptomatic care, methadone and buprenorphine induction/titration/monitoring, naloxone rescue, naltrexone timing, pregnancy OAT, and retention-mortality evidence. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
This leaf focuses on what examiners grill hardest after the OUD definition: withdrawal phenomenology and COWS, safe methadone and buprenorphine induction, naloxone rescue technique, antagonist timing, and pregnancy. Detoxification without a retention plan is not a moral victory if it returns the patient to use at lost tolerance.[4][10][13]
Overview and definition
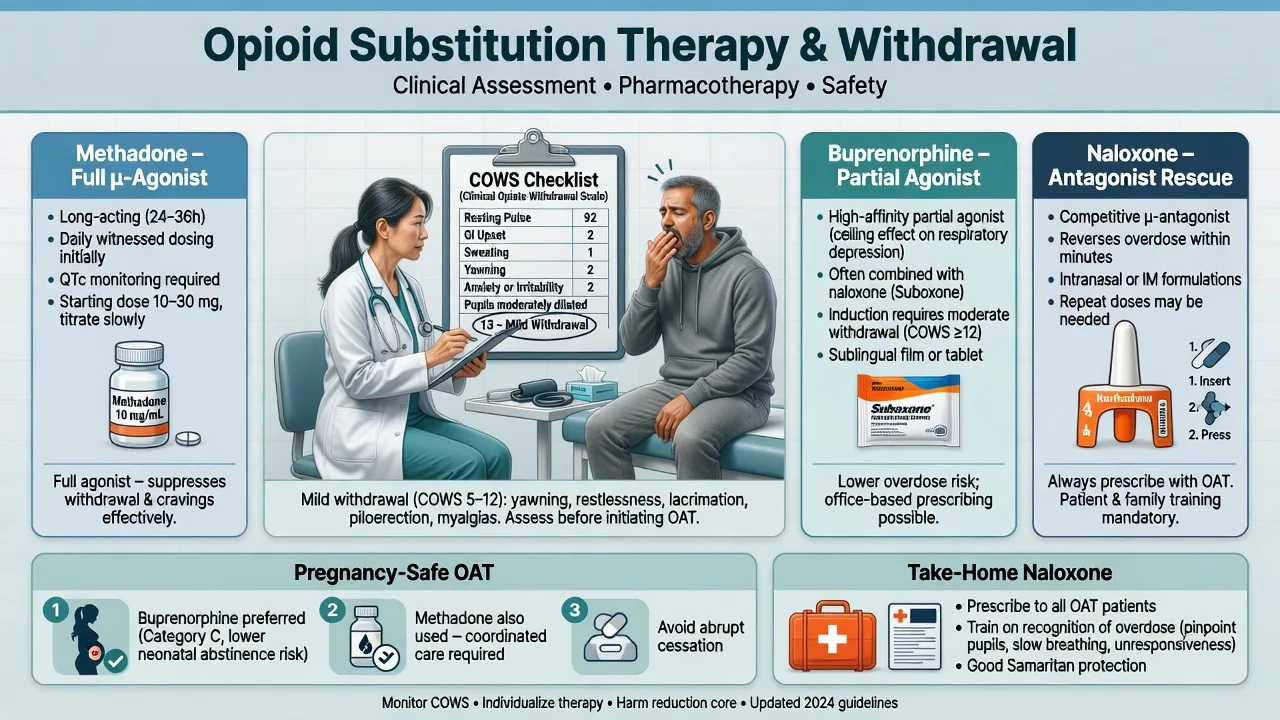
Opioid withdrawal is a time-limited neuroadaptive state after dose reduction, cessation, or receptor displacement. Opioid substitution therapy (OST) — also called opioid agonist treatment (OAT) or medication for opioid use disorder (MOUD) — means supervised full or partial µ-agonist medication (methadone; buprenorphine ± naloxone) that stabilises receptors, suppresses craving and illicit use, and reduces mortality when patients remain in treatment.[1][2][4][10]
Withdrawal management is not synonymous with cure. Physiological dependence (tolerance + withdrawal) can exist without the full compulsive syndrome of OUD; conversely, most moderate–severe OUD needs long-term OAT rather than a short “clean” detox alone.[10][15]
Classification and pharmacology map
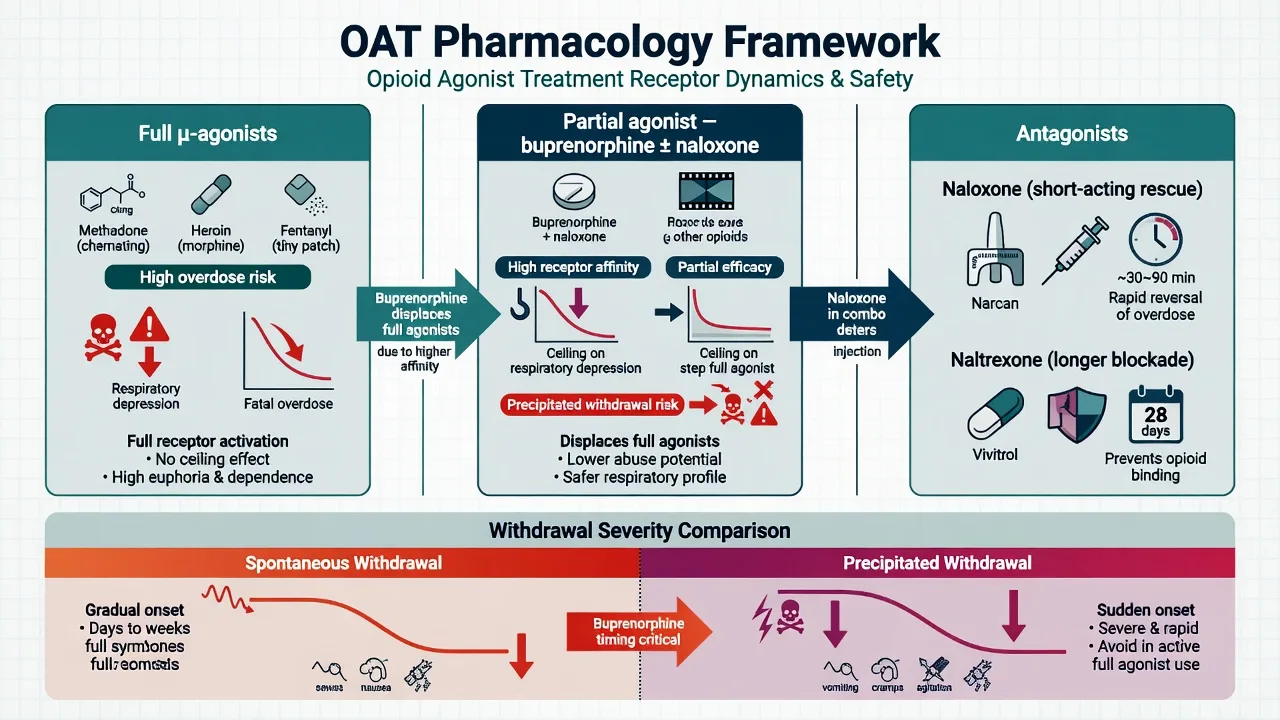
Full µ-agonists
- Heroin, morphine, oxycodone, fentanyl, methadone
- Methadone: long half-life OAT full agonist
- High overdose risk if uncontrolled
- Delayed toxicity risk during methadone induction
Partial agonist
- Buprenorphine ± naloxone
- High affinity, lower intrinsic efficacy
- Relative respiratory ceiling vs full agonists
- Precipitated withdrawal if full agonist still present
Antagonists
- Naloxone: short-acting overdose rescue
- Naltrexone oral or XR-IM after detox
- No agonist reinforcement
- Precipitate withdrawal if opioids on board
Clinical states
- Spontaneous withdrawal
- Precipitated withdrawal
- Intoxication / overdose
- Stable OAT maintenance
Pharmacologic class drives both emergency risk and which induction algorithm you open first.[8][10]
Epidemiology and mortality framing
Mortality and retention anchors
Retention in opioid substitution treatment is associated with lower mortality than periods off treatment; risk rises after cessation.[4][14] After non-fatal opioid overdose, receipt of medication for OUD associates with reduced mortality — discharge without an OAT offer is a systems failure.[13] High-risk windows examiners love: first week of methadone if over-rapid titration; post-detox; post-release from custody; missed doses with loss of tolerance.[4][10]
Pathophysiology
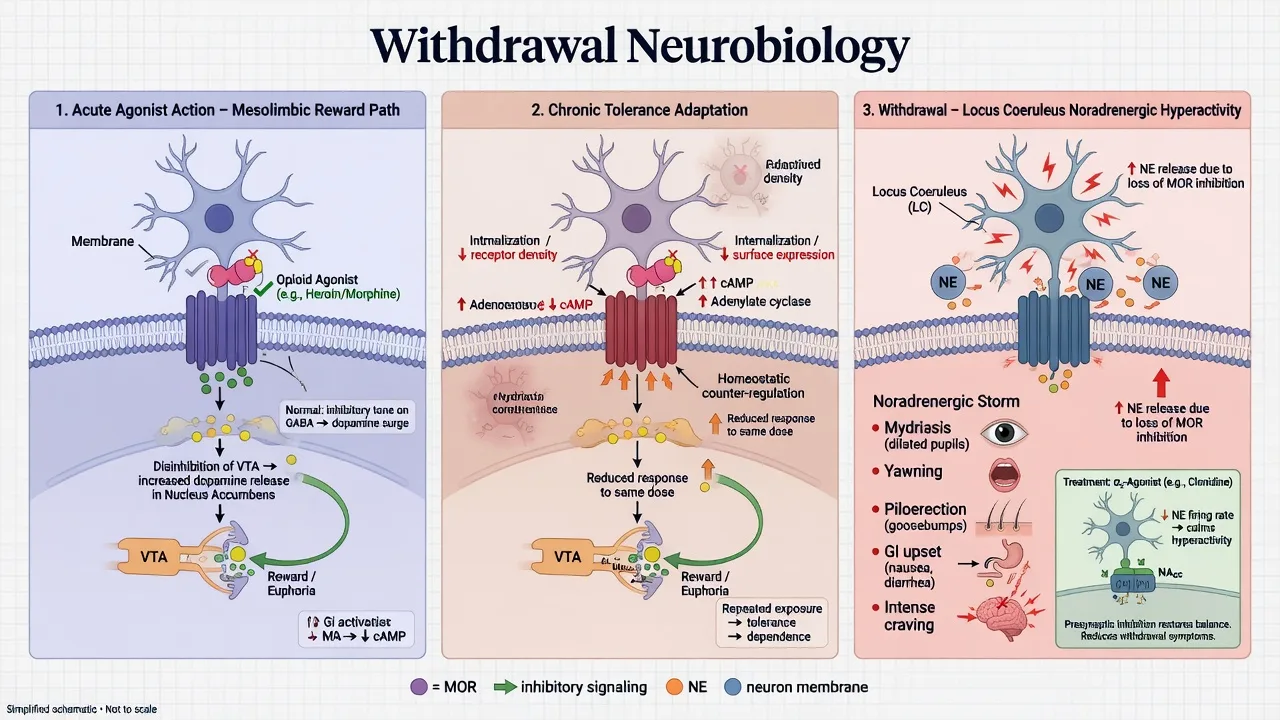
µ-Opioid receptor agonism produces analgesia and reward; chronic exposure yields tolerance and a withdrawal syndrome on cessation. Locus coeruleus noradrenergic hyperactivity contributes to yawning, lacrimation, mydriasis, piloerection, sweating, and GI hypermotility — hence α2-adrenergic agonists (clonidine, lofexidine) as adjunctive withdrawal agents.[9]
Buprenorphine combines high receptor affinity with partial efficacy: relative ceiling on respiratory depression versus full agonists, but capacity to displace residual full agonists and precipitate withdrawal. Methadone is a full agonist with a long half-life and tissue accumulation — therapeutic for once-daily OAT, lethal if induction is aggressive. Naloxone competitively antagonises µ-receptors with a shorter clinical duration than many agonists, so re-sedation is expected after fentanyl or methadone exposure.[8][10]
Clinical presentation
Spontaneous withdrawal. Flu-like autonomic picture: lacrimation, rhinorrhoea, yawning, mydriasis, piloerection, sweating, myalgia, abdominal cramps, diarrhoea, nausea, restlessness, anxiety, insomnia, craving. Short-acting opioids (heroin, many IR pharmaceuticals): onset often 6–12 h, peak 1–3 days. Methadone withdrawal starts later and lasts longer. Adult pure opioid withdrawal is rarely directly fatal; the fatal pathway is relapse at lost tolerance.[3][10]
Precipitated withdrawal. Abrupt, severe syndrome minutes after buprenorphine, naloxone, or naltrexone when full agonists remain. Management is supportive; do not “chase” with more antagonist. Rebuild trust and reschedule induction when objective withdrawal is adequate.[10]
Overdose context. Coma/reduced consciousness, respiratory depression, miosis (not always classic with co-ingestants). Always treat ABCs first.[8]
Differential diagnosis
Viral / GI illness
- No tight link to last opioid time
- Fever source may be real infection
- Still examine for injecting complications
Anxiety / panic
- Less autonomic GI and piloerection package
- COWS helps objectify
- Can co-exist with craving
Sedative withdrawal
- Alcohol/benzo — seizure and delirium risk
- Opioid withdrawal alone rarely seizes adults
- Polysubstance is the trap
Stimulant crash
- Dysphoria, hypersomnia, less classic opiate signs
- UDS and history discriminate
Never miss medical co-travelers: sepsis, head injury, hypoxia, hypoglycaemia, aspiration after overdose.[8]
Bedside assessment and COWS
Structure history: opioid type, route, approximate daily amount, exact last use time, prior OAT drug and dose, overdoses and naloxone response, benzodiazepines/alcohol, injecting and BBV, mental health and suicide risk, housing, forensic/child protection, and pregnancy possibility.[10]
COWS — own the bands
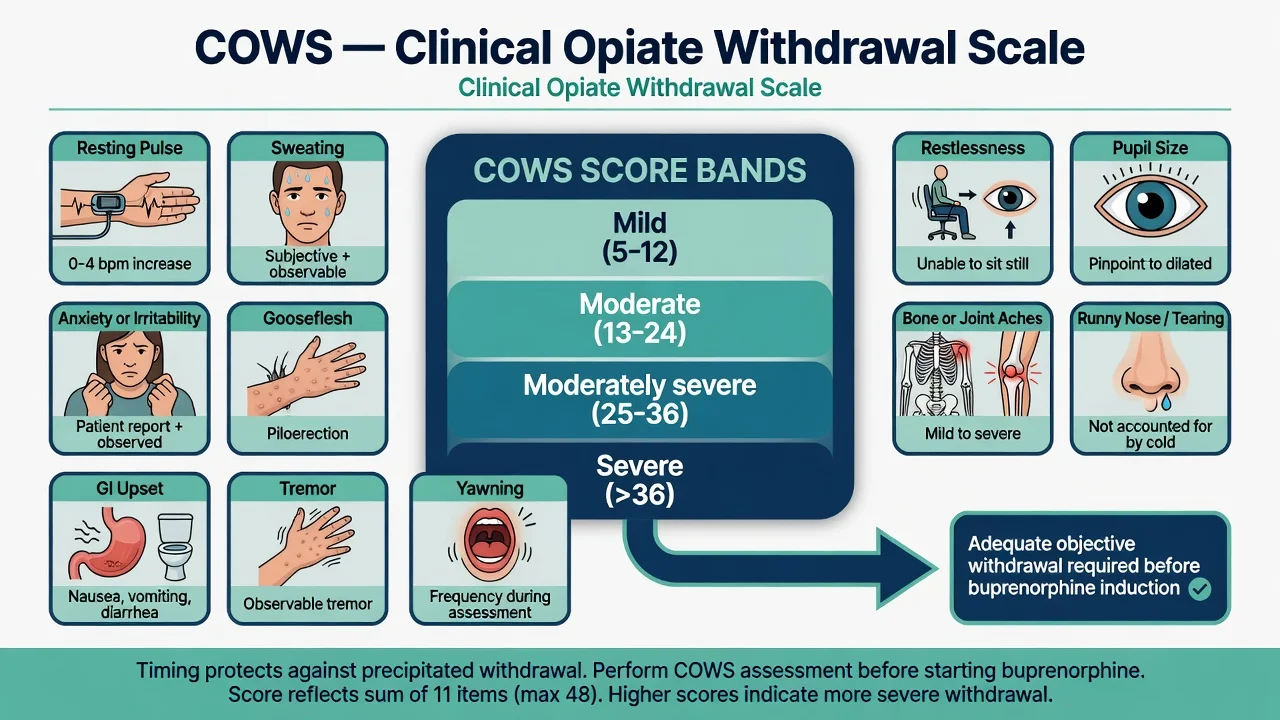
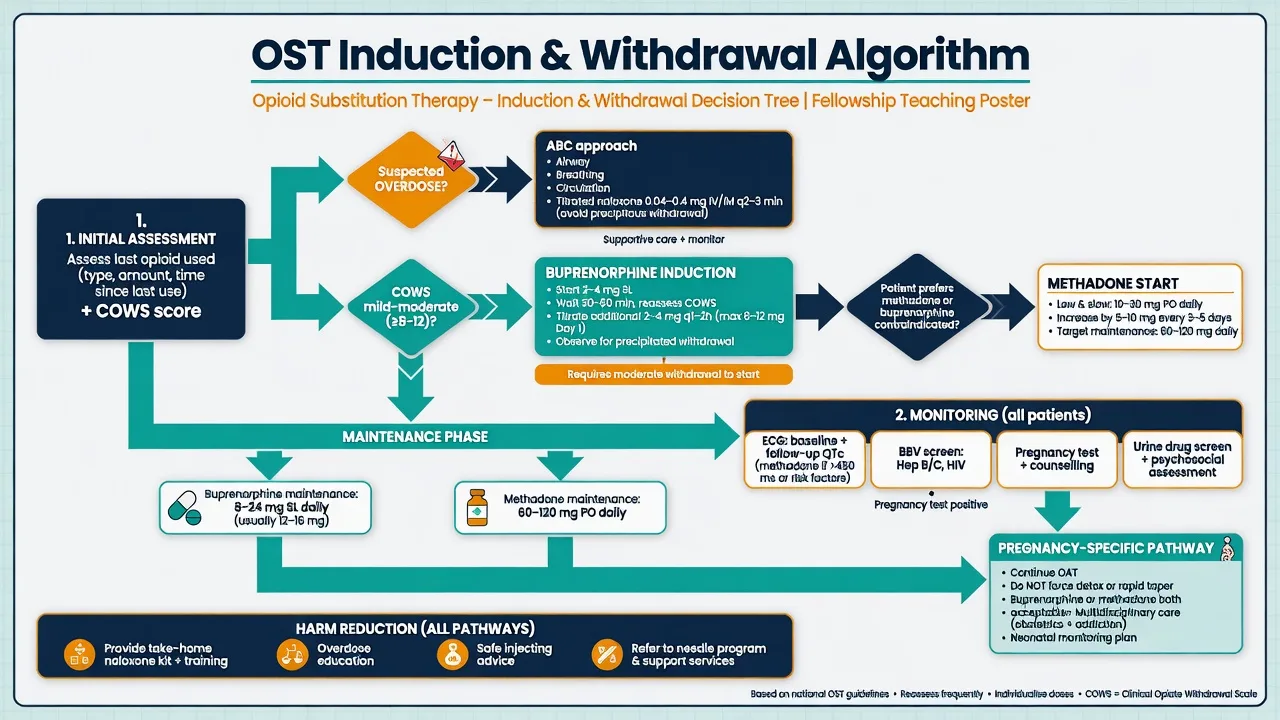
The Clinical Opiate Withdrawal Scale rates 11 domains (resting pulse; sweating; restlessness; pupil size; bone/joint aches; runny nose or tearing; GI upset; tremor; yawning; anxiety or irritability; gooseflesh). Common total-score bands: mild 5–12, moderate 13–24, moderately severe 25–36, severe greater than 36. Serial scores guide symptomatic care and buprenorphine readiness. Many protocols wait for at least mild–moderate objective withdrawal (often COWS around 8–12 or higher, protocol- and fentanyl-dependent) before the first buprenorphine dose.[3][10]
MSE covers consciousness, affect, craving, insight, motivation, and risk (overdose, suicide, vulnerability). Capacity is decision-specific; least-restrictive legal options are jurisdiction-local — do not invent foreign statute numbers.[10]
Investigations
Bedside: respiratory rate, SpO2, glucose, pregnancy test, ECG when methadone planned or arrhythmia risk. Labs: FBC, U&E, LFT; HIV, HBV, HCV serology. UDS: interpret with humility (false positives/negatives; fentanyl-specific assays; separate methadone and buprenorphine tests). Use UDS for safety and engagement, not moral theatre.[10]
QTc. Methadone can prolong QTc; screen at baseline and when doses are high, symptoms appear, or QT-prolonging/CYP-interacting drugs are added. Correct potassium and magnesium.[11]
Acute management — overdose and symptomatic withdrawal
Naloxone. Competitive µ-antagonist. Typical adult parenteral teaching range: 0.4–2 mg IV/IM/SC, repeated every few minutes to restore adequate ventilation (not necessarily full alertness — abrupt full reversal can precipitate severe withdrawal and agitation). Intranasal kits commonly deliver about 2–4 mg per device depending on product. Infusion may be needed for methadone or massive fentanyl exposure because naloxone can wear off first.[8][10]
After survival: take-home naloxone, overdose education, and same-episode buprenorphine initiation when COWS allows, with assertive clinic linkage. ED-initiated buprenorphine/naloxone improved engagement versus brief intervention alone in a landmark RCT.[6][13]
Symptomatic withdrawal (non-OAT adjuncts). α2-Agonists reduce autonomic symptoms: clonidine often 0.1–0.2 mg oral every 6–8 hours with blood-pressure monitoring (hold if hypotensive/bradycardic); lofexidine where licensed. Add antiemetics, antidiarrhoeals, non-opioid analgesia, and sleep support. Buprenorphine itself is also an evidence-based withdrawal agent when induction rules are met. Planned detox alone has high relapse — always couple with overdose prevention and a maintenance offer.[9][10]
Definitive management — methadone, buprenorphine, naltrexone
Methadone and buprenorphine maintenance reduce illicit opioid use and improve retention versus non-replacement approaches; office-based buprenorphine–naloxone expands access where regulation allows.[1][2][16]
Methadone (full agonist OAT)
Induction. Start low and go slow because accumulation over the first days can kill. Day-1 oral doses in many specialist protocols are often 10–30 mg for patients with clear opioid tolerance (lower if low/uncertain tolerance, older age, heavy alcohol/benzo use, or respiratory disease), with careful review before same-day small increments. Avoid aggressive titration in week 1; peak induction toxicity often appears around days 3–7. Maintenance for most patients settles around 60–120 mg orally daily, sometimes higher under specialist review. Supervise dosing early; takeaways follow local stability criteria.[1][10]
Monitoring. Sedation and respiratory rate early; CYP3A4 and sedative interactions; ECG/QTc as above; LFT and clinical review; pregnancy status. After missed doses, do not blindly reissue the full prior dose if tolerance may have fallen — re-titrate per local OST guidelines.[10][11]
Buprenorphine (± naloxone)
Induction: wait until adequate objective withdrawal (COWS-guided) to avoid precipitated withdrawal. Typical teaching start: 2–4 mg sublingual, reassess in about 1–2 hours, day-1 total often toward 8 mg if tolerated (local protocols and fentanyl-era high-dose or micro-induction pathways exist in specialist hands). Maintenance commonly 8–24 mg sublingual daily (some jurisdictions allow up to 32 mg). Film/tablet must dissolve fully; advise against injecting diverted product. Long-acting injectable buprenorphine exists in many ANZ services via specialist pathways.[2][10][16]
Transfers. Methadone-to-buprenorphine transfer usually needs methadone reduction and adequate withdrawal before first buprenorphine dose — precipitated withdrawal mid-transfer is a classic viva failure mode.[10]
Naltrexone pathway
Oral naltrexone 50 mg daily (or thrice-weekly regimens in some protocols) and extended-release intramuscular naltrexone (commonly 380 mg every 4 weeks where available) require a completed opioid-free period (often about 7–10 days after short-acting opioids; longer after methadone) with negative UDS / supervised withdrawal before first dose. In X:BOT, once induction succeeded, XR-naltrexone and buprenorphine–naloxone had similar effectiveness, but XR-naltrexone was harder to initiate — counsel pathway choice honestly.[5][10]
Psychosocial care and duration
Counselling, contingency management, and keyworking support OAT but do not replace it for most severe dependence. In prescription opioid dependence, POATS showed high relapse after tapering off buprenorphine — favour longer treatment rather than arbitrary short courses.[15] Duration is often years, individualised; premature taper for administrative optics is harmful.[4][10]
Australian and New Zealand opioid treatment programs regulate methadone and buprenorphine with supervised dosing, jurisdiction-specific takeaway policies, and expanding long-acting injectable buprenorphine. RANZCP addiction competence expects safe induction, risk management, dual diagnosis, and culturally safe care. Needle-syringe programs and take-home naloxone are standard harm-reduction pillars.[14][10]
Subtypes and high-yield scenarios
Fentanyl-era induction. High-potency illicit fentanyl can prolong the wait for “safe” COWS thresholds and increase precipitated-withdrawal risk; specialist micro-induction or higher-dose protocols may be used — know that ordinary textbook waits may need adaptation, not abandonment of OAT.[10]
Hospital admission. Continue verified community OAT after clinic liaison; cover withdrawal if dose unconfirmed; do not leave patients in untreated withdrawal or uncontrolled pain.[10]
Custody / post-release. Continuity of OAT plus take-home naloxone targets a known mortality spike.[4][14]
Polysubstance use. Benzodiazepines and alcohol multiply overdose risk on methadone and illicit opioids — manage sedatives actively.[8][10]
Complications and pitfalls
Other pitfalls: diverted OAT; injecting crushed tablets; ignoring QTc-interacting drugs; forced taper; withholding acute analgesia without a plan; framing OAT as “replacing one addiction with another” against mortality evidence.[4][11]
Prognosis and disposition
Retention is the dominant modifiable survival factor.[4][14] Disposition spans specialist clinics, GP shared care, residential rehab after or alongside stabilisation, hospital, and custody. After any non-fatal overdose, disposition is incomplete without a MOUD offer and naloxone supply.[13]
Special populations — pregnancy first
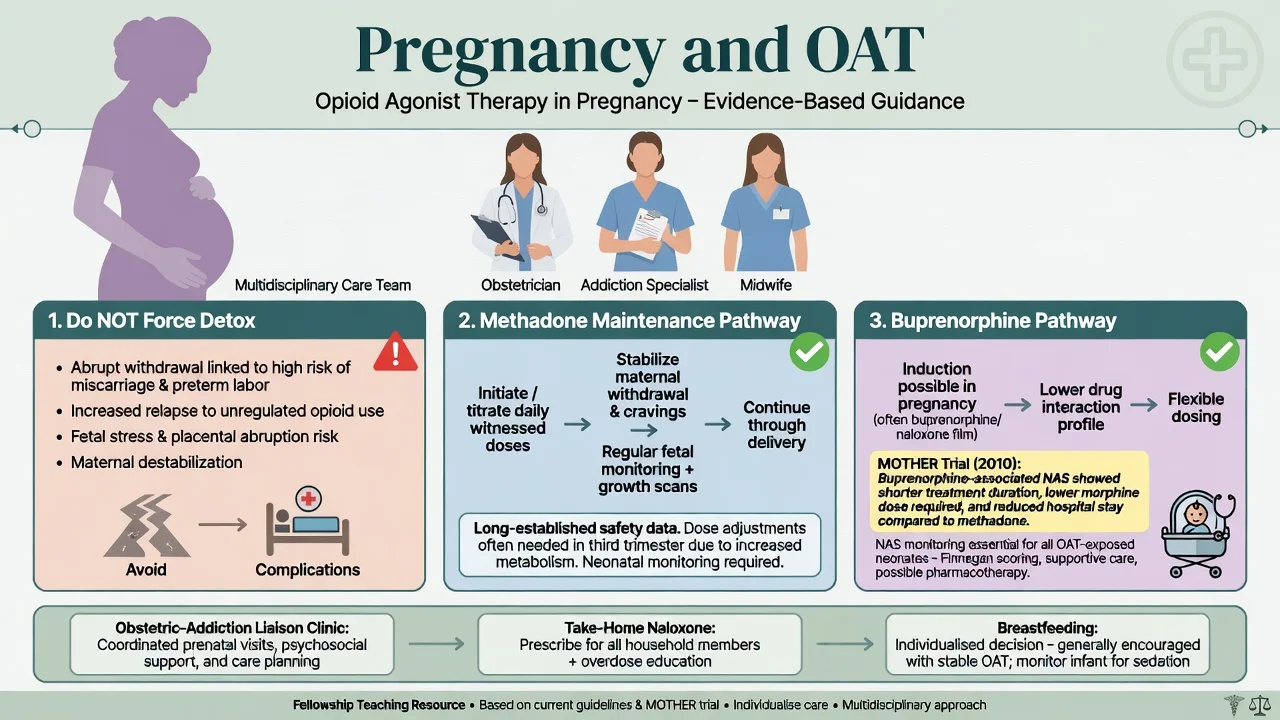
Pregnancy. Opioid withdrawal risks miscarriage, preterm labour, and return to unregulated use. Maintenance agonist treatment is preferred over detoxification for dependent pregnant patients. Both methadone and buprenorphine are used. The MOTHER trial found buprenorphine-exposed neonates required less treatment for neonatal abstinence syndrome and had shorter hospital stays than methadone-exposed neonates, with retention nuances — choice is individualised. Cochrane synthesis supports maintenance agonist treatments in pregnancy. Breastfeeding decisions are individualised with specialist advice when the mother is stable on OAT and not using illicit drugs.[7][12]
Youth / older adults. Consent and family engagement in adolescents; lower starting doses, falls, and polypharmacy later in life.[10]
Chronic pain dual pathway. If OUD is present, treat with OAT while delivering multimodal analgesia — abandoning both pain and addiction care is the failure mode.[10][15]
Evidence and guidelines
Name at viva: Mattick Cochrane methadone and buprenorphine; Sordo mortality meta-analysis; NSW pharmacotherapy cohort; Wesson and Ling COWS; Boyer overdose; Gowing α2-agonists; D’Onofrio ED initiation; Lee X:BOT; Jones MOTHER; Minozzi pregnancy Cochrane; Larochelle post-overdose MOUD; Fudala office-based buprenorphine–naloxone; Weiss POATS; Krantz QTc; ASAM 2020.[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15][16]
Exam pearls
COWS-OAT
Self-test: name doses under pressure
Methadone day-1 often 10–30 mg oral with slow titration; maintenance commonly 60–120 mg daily. Buprenorphine induction 2–4 mg SL steps after withdrawal; maintenance often 8–24 mg daily. Naloxone 0.4–2 mg parenteral repeated to ventilation; IN kits commonly 2–4 mg/device. Naltrexone oral 50 mg daily or XR-IM ~380 mg/4 weeks after detox. Clonidine ~0.1–0.2 mg every 6–8 h with BP checks for autonomic withdrawal.[8][9][10]
References
- [1]Mattick RP, Breen C, Kimber J, Davoli M Methadone maintenance therapy versus no opioid replacement therapy for opioid dependence Cochrane Database Syst Rev, 2009.PMID 19588333
- [2]Mattick RP, Breen C, Kimber J, Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioid dependence Cochrane Database Syst Rev, 2014.PMID 24500948
- [3]Wesson DR, Ling W The Clinical Opiate Withdrawal Scale (COWS) J Psychoactive Drugs, 2003.PMID 12924748
- [4]Sordo L, Barrio G, Bravo MJ, Indave BI, Degenhardt L, Wiessing L, et al. Mortality risk during and after opioid substitution treatment: systematic review and meta-analysis of cohort studies BMJ, 2017.PMID 28446428
- [5]Lee JD, Nunes EV, Novo P, Bachrach K, Bailey GL, Bhatt S, et al. Comparative effectiveness of extended-release naltrexone versus buprenorphine-naloxone for opioid relapse prevention (X:BOT): a multicentre, open-label, randomised controlled trial Lancet, 2018.PMID 29150198
- [6]D'Onofrio G, O'Connor PG, Pantalon MV, Chawarski MC, Busch SH, Owens PH, et al. Emergency department-initiated buprenorphine/naloxone treatment for opioid dependence: a randomized clinical trial JAMA, 2015.PMID 25919527
- [7]Jones HE, Kaltenbach K, Heil SH, Stine SM, Coyle MG, Arria AM, et al. Neonatal abstinence syndrome after methadone or buprenorphine exposure N Engl J Med, 2010.PMID 21142534
- [8]Boyer EW Management of opioid analgesic overdose N Engl J Med, 2012.PMID 22784117
- [9]Gowing L, Farrell M, Ali R, White JM Alpha₂-adrenergic agonists for the management of opioid withdrawal Cochrane Database Syst Rev, 2016.PMID 27140827
- [10]American Society of Addiction Medicine The ASAM National Practice Guideline for the Treatment of Opioid Use Disorder: 2020 Focused Update J Addict Med, 2020.PMID 32511106
- [11]Krantz MJ, Martin J, Stimmel B, Mehta D, Haigney MC QTc interval screening in methadone treatment Ann Intern Med, 2009.PMID 19153406
- [12]Minozzi S, Amato L, Jahanfar S, Bellisario C, Ferri M, Davoli M Maintenance agonist treatments for opiate-dependent pregnant women Cochrane Database Syst Rev, 2020.PMID 33165953
- [13]Larochelle MR, Bernson D, Land T, Stopka TJ, Wang N, Xuan Z, et al. Medication for Opioid Use Disorder After Nonfatal Opioid Overdose and Association With Mortality: A Cohort Study Ann Intern Med, 2018.PMID 29913516
- [14]Degenhardt L, Randall D, Hall W, Law M, Butler T, Burns L Mortality among clients of a state-wide opioid pharmacotherapy program over 20 years: risk factors and lives saved Drug Alcohol Depend, 2009.PMID 19608355
- [15]Weiss RD, Potter JS, Fiellin DA, Byrne M, Connery HS, Dickinson W, et al. Adjunctive counseling during brief and extended buprenorphine-naloxone treatment for prescription opioid dependence: a 2-phase randomized controlled trial Arch Gen Psychiatry, 2011.PMID 22065255
- [16]Fudala PJ, Bridge TP, Herbert S, Williford WO, Chiang CN, Jones K, et al. Office-based treatment of opiate addiction with a sublingual-tablet formulation of buprenorphine and naloxone N Engl J Med, 2003.PMID 12954743