Psych · Addiction psychiatry — pharmaceutical and OTC misuse
Pharmaceutical and over-the-counter drug misuse
Also known as OTC drug abuse · Non-prescription medicine misuse · Codeine dependence · Gabapentinoid misuse · Loperamide abuse · Dextromethorphan abuse · Purple drank · Pharmacy medicine dependence · Prescription drug diversion · Pharmaceutical opioid dependence
Exam-exhaustive fellowship reference on pharmaceutical and over-the-counter drug misuse — codeine and Australian rescheduling, gabapentinoids, loperamide cardiotoxicity, DXM, antihistamines, purple drank, diverted psychotropics and stimulants, pseudoephedrine precursor control, assessment, OAT for pharmaceutical opioids, and regional policy deltas. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Fellowship candidates must dismantle the myth that “pharmacy medicines cannot create real addiction.” Qualitative work shows people often reject an “addict” identity precisely because the product is legal and pharmacy-sourced, which delays help-seeking and invites clinician minimisation.[1] Population surveys confirm non-prescription medicine misuse and dependence are not rare curiosities.[2] In Australia, the February 2018 move of codeine to prescription-only status is a board-favourite policy natural experiment with measurable reductions in codeine-related harm signals and shifts in analgesic markets.[6][7][8]
Overview and definition
Misuse covers use outside approved indication, dose, duration, or person (including intentional intoxication). Non-medical use emphasises psychoactive intent. Dependence / use disorder follows DSM-5-TR or ICD-11 substance-class criteria (impaired control, social impairment, risky use, tolerance, withdrawal) — there is no single “OTC use disorder” code; you classify by pharmacology (opioid, sedative, stimulant, other).[2][3][5]
Diversion is transfer from a legitimate supply chain to non-prescribed users (friends, street markets, online). Iatrogenic dependence after long-term prescribed use still warrants treatment; moral purity tests fail exams and patients.[1][5][15]
Sources include single GP scripts, multiple pharmacies (“pharmacy hopping”), residual stockpiles from pre-rescheduling eras, friends/family cabinets, and unregulated online sellers. Stigma and identity conflict are part of the clinical presentation, not soft background colour.[1][3]
Classification
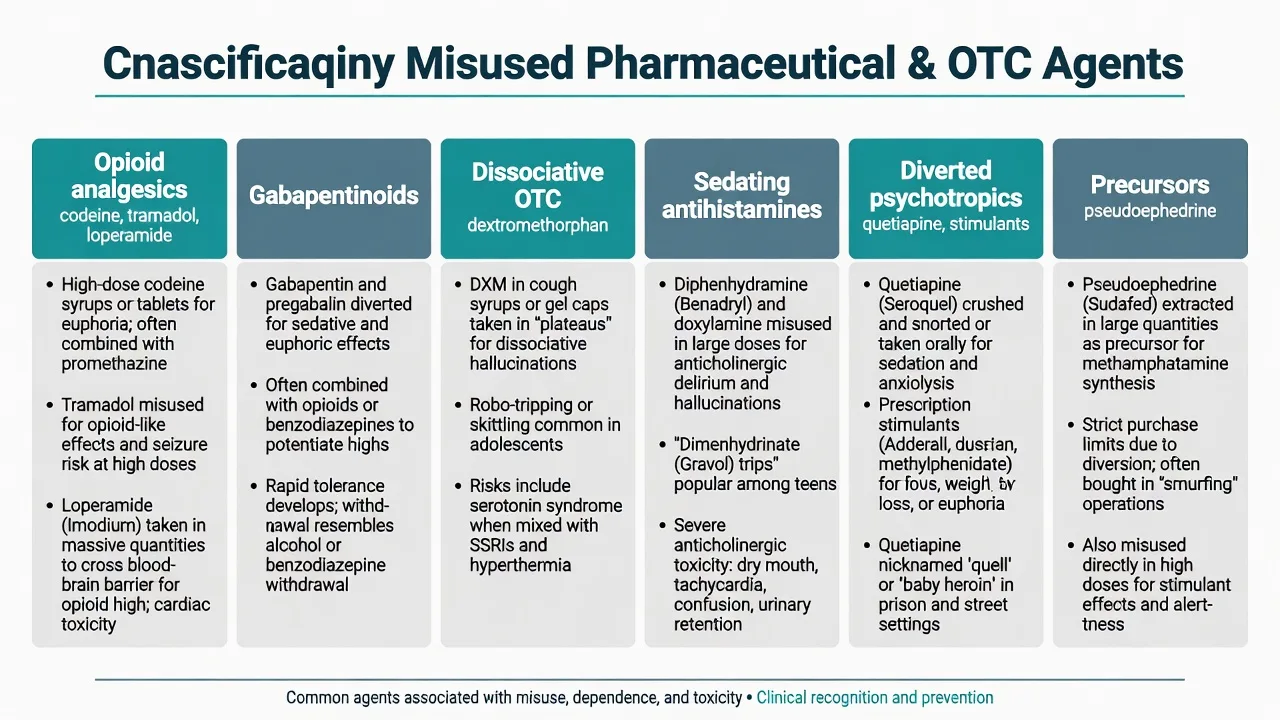
| Class | High-yield agents | Exam phenotype |
|---|---|---|
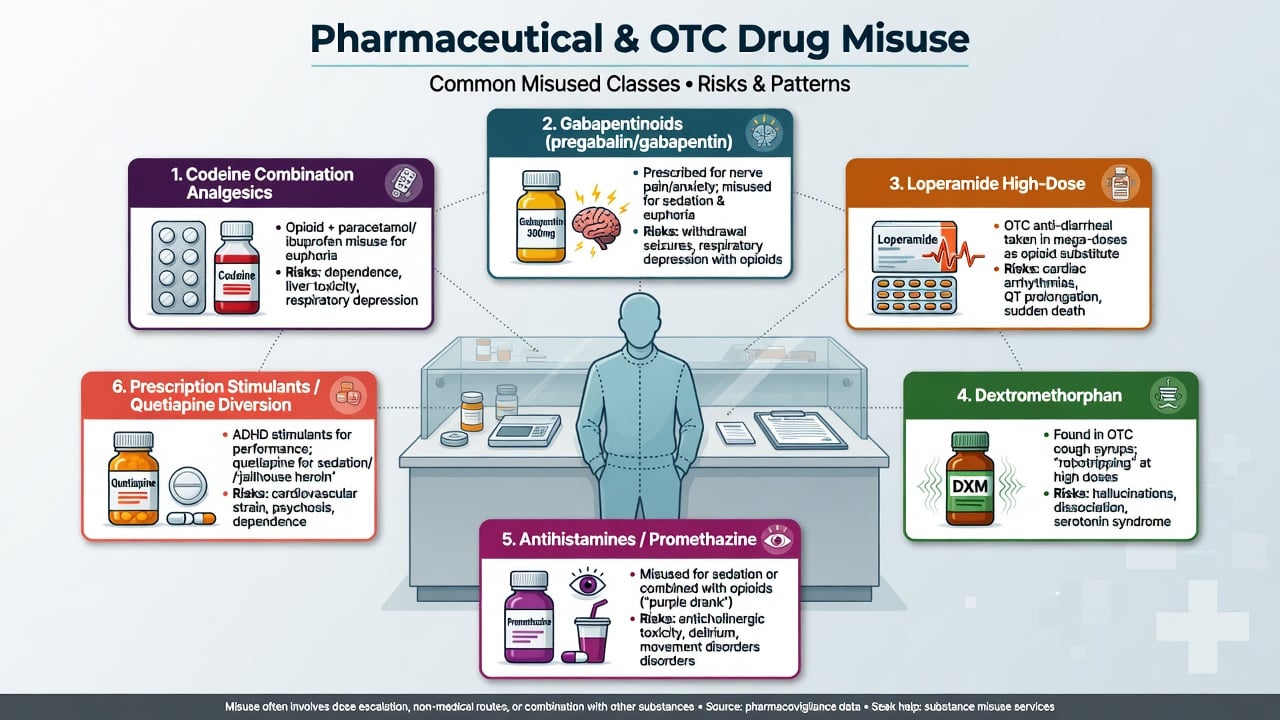
| Opioid analgesics | Codeine combinations, tramadol, diverted strong opioids | Escalating packs, withdrawal, combination-product organ injury |
| Peripheral opioid / anti-diarrhoeal | Loperamide mega-dose | “Poor man’s methadone” + arrhythmia/arrest |
| Gabapentinoids | Pregabalin, gabapentin | Euphoria/sedation, opioid co-use, prison diversion |
| Dissociative OTC | Dextromethorphan (DXM) | Dose-related dissociation, youth “robotripping” |
| Sedating antihistamines | Promethazine, diphenhydramine, doxylamine | Anticholinergic toxicity; purple drank partner |
| Diverted psychotropics | Quetiapine, prescription stimulants | Sleep/come-down use; study-drug diversion |
| Precursors | Pseudoephedrine | Methamphetamine manufacture control, not a SUD diagnosis alone |
Purple drank (also called lean, sizzurp in some cultures) is codeine plus promethazine cough syrup, often mixed with soft drink — a social-recreational pattern with medical toxicity from both opioid and antihistamine components.[14]
Epidemiology and risk
Non-prescription medicine misuse appears in general-population surveys and community-pharmacy research internationally.[2][3] Risk clusters: chronic pain and headache self-medication, anxiety/insomnia, prior substance use disorder, youth experimentation, and limited access or willingness to attend addiction services.[1][2][5]
Codeine and Australian rescheduling. OTC combination codeine historically produced dependence and serious morbidity (notably codeine-ibuprofen gastroenterological and haematological harm).[4][5] From 1 February 2018, Australia rescheduled codeine-containing medicines to prescription-only. Evaluations showed reductions in codeine use and related harm signals (including poisons-centre type endpoints in Cairns and colleagues) and market substitution toward non-opioid OTC analgesics.[6][7] Subsequent work found declines in hospital admissions for paracetamol poisoning after rescheduling — a reminder that combination products couple opioid dependence risk to paracetamol dose.[8]
Gabapentinoids. Once marketed as low-abuse anticonvulsants/analgesics, gabapentin and pregabalin show clear misuse, abuse, and diversion signals, enriched among people who use opioids and in forensic/prison settings.[9][10][11]
Loperamide. High-dose misuse for opioid effects or withdrawal self-treatment is linked in post-marketing and case series data to life-threatening cardiac dysrhythmia and death.[12][13]
Policy and clinical anchors
Pathophysiology
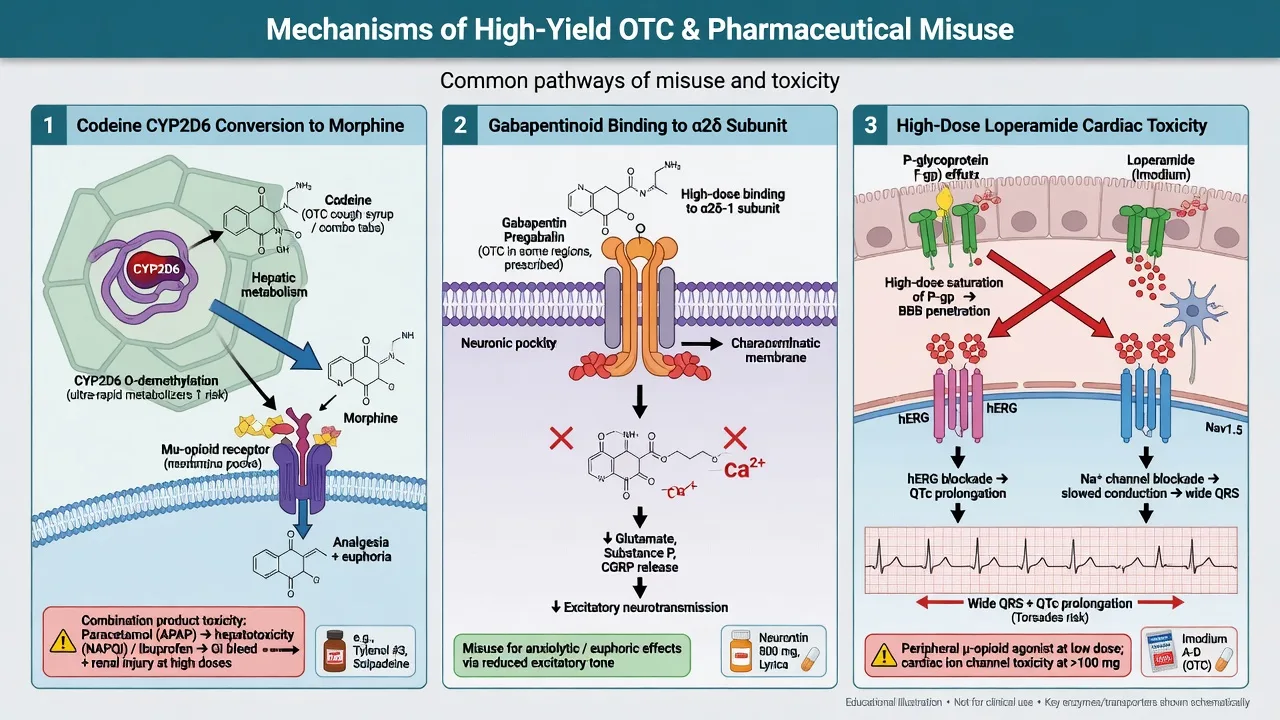
Codeine is a prodrug: O-demethylation via CYP2D6 yields morphine. Ultra-rapid metabolisers can experience exaggerated opioid effects at standard doses; poor metabolisers get little analgesia and may escalate tablet counts. Combination products smuggle paracetamol hepatotoxicity or ibuprofen GI bleed, renal injury, and anaemia into the dependence story — Frei’s MJA series is the classic ANZ teaching set.[4][5]
Gabapentinoids bind the α2δ subunit of voltage-gated calcium channels, reducing excitatory neurotransmitter release. At supra-therapeutic doses they produce sedation, euphoria, dissociation, and — critically — additive respiratory depression with opioids.[9][10][11]
Loperamide is a μ-opioid agonist designed for peripheral antidiarrhoeal action. At massive doses, and especially with P-glycoprotein or CYP3A4 inhibitors, central opioid effects emerge. Cardiac toxicity reflects sodium-channel and hERG potassium-channel effects → QRS widening, QTc prolongation, ventricular arrhythmias, and sudden death.[12][13]
Dextromethorphan is an NMDA-receptor antagonist (with sigma-1 activity) producing dose-related dissociative states. Combinations with serotonergic agents raise serotonin-toxicity concern in acute care stems.[2]
Promethazine and first-generation antihistamines add anticholinergic delirium risk and deepen opioid sedation in purple-drank patterns.[14]
Clinical presentation
Codeine / pharmaceutical opioid pathway. Escalating daily tablet counts, multiple pharmacy narratives, rebound headaches, morning withdrawal (rhinorrhoea, myalgias, dysphoria, craving), constipation alternating with use, and sometimes occult melaena, iron-deficiency anaemia, or abnormal LFTs from the non-opioid partner drug.[3][4][5]
Gabapentinoid pathway. Sedation, ataxia, euphoria, dose escalation beyond neuropathic-pain scripts, withdrawal anxiety and insomnia on missed doses, frequent co-use with opioids or benzodiazepines.[9][10]
Loperamide mega-dose. Opioid-like relief of withdrawal or intentional intoxication plus syncope, palpitations, seizures, or out-of-hospital cardiac arrest — the history may be hidden until family finds blister packs.[12][13]
DXM. Mild stimulation at low recreational ranges progressing to dissociation, nystagmus, agitation, or stupor; youth party or solitary use common in stems.[2]
MSE language that scores marks: craving; unsuccessful cut-downs; time spent obtaining (pharmacy circuits); continued use despite ulcer, arrest, or relationship harm; secrecy; and the rationalisation “it is only chemist medicine.”[1][5]
Differential diagnosis
| Mimic | Favours pharmaceutical/OTC misuse dependence | Favours alternative |
|---|---|---|
| Primary chronic pain / migraine | Dose escalation, withdrawal relief dosing, pharmacy hopping | Stable multimodal plan, no control loss |
| Primary anxiety / insomnia | Rebound tightly linked to gabapentinoid/sedative cuts | Anxiety independent of dose for months |
| Cardiogenic syncope / channelopathy | Loperamide mega-dose history, wide QRS/QTc | Structural heart disease without tox history |
| Primary psychosis | Anticholinergic delirium (antihistamines) or DXM intoxication tempo | Schizophrenia course without tox triggers |
| Illicit heroin OUD | Pharmaceutical supply, combination-product labs | Injecting marks, heroin-specific market history |
| Intentional paracetamol overdose alone | Opioid dependence narrative + chronic combination use | Single self-harm act without dependence pattern |
Clinical and bedside assessment
- Agent inventory — name, strength, tablets per day (prescribed vs actual), duration, routes, all sources (GP, ED, dentist, multiple pharmacies, online, peers).[3][5]
- Co-use — alcohol, illicit opioids, benzodiazepines, gabapentinoids, stimulants, cannabis.[9][10]
- Harm screen — overdoses, seizures, syncope, GI bleed, jaundice, driving, childcare, work safety-critical roles, suicidality.[4][12]
- Collateral — pharmacy dispense history, real-time prescription monitoring where available, GP shared record, family.[3][5]
- Identity and motivation — expect resistance to “addiction” language; use motivational interviewing and concrete medical harms rather than moral confrontation alone.[1]
Physical exam: vitals, pupils, hydration, abdominal tenderness/melaena signs, neurological exam, injection sites if dual pathway, cognitive screen when sedating polypharmacy is chronic.[4][5]
Investigations
- ECG whenever loperamide mega-dose, syncope, polypharmacy QT risk, or unexplained arrhythmia is possible — do not wait for a perfect history.[12][13]
- LFTs, INR, paracetamol concentration when combination products or hepatotoxicity suspected.[8][4]
- FBC, iron studies, U&E, creatinine for chronic NSAID-codeine use (anaemia, renal injury).[4]
- Urine drug screen is adjunctive only — many agents are missed or nonspecific; never use a negative screen to refute a clear history.[5]
- Pregnancy test when relevant; telemetry/troponin if arrhythmic presentation.[12]
Management — resuscitation and emergencies
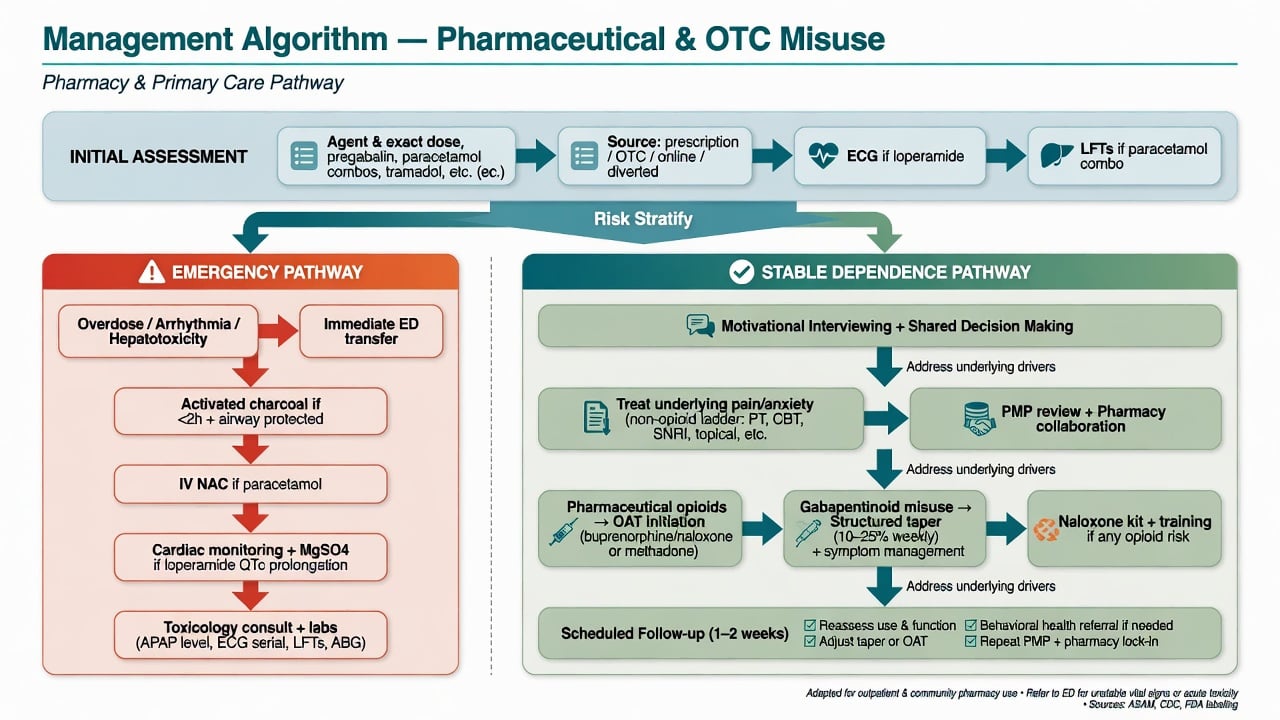
- Opioid toxicity (codeine, other pharmaceutical opioids, loperamide): airway, ventilation, oxygen, naloxone titrated to respiration (not necessarily full arousal). Loperamide may require repeated or higher cumulative naloxone and prolonged observation because of kinetics; unstable rhythm management takes priority over pure “naloxone-and-discharge” thinking.[12][13][15]
- Loperamide cardiac toxicity: ACLS protocols, correct electrolytes, involve toxicology/cardiology early; sodium bicarbonate is often considered for wide-complex sodium-channel toxicity patterns per toxicology guidance; avoid stacking pro-arrhythmic antiarrhythmics without specialist advice.[12][13]
- Paracetamol mass exposure: standard acetylcysteine pathways; do not let the opioid story distract from timed paracetamol risk.[8]
- GI haemorrhage from ibuprofen combinations: resuscitate, reverse coagulopathy as indicated, urgent gastroenterology.[4]
- DXM / anticholinergic crisis: supportive care, benzodiazepines for severe agitation when appropriate, serotonin-toxicity recognition if serotonergic co-ingestants.[2][14]
Management — definitive and stepwise
Step 1 — Name the problem without moral theatre
Validate that dependence on pharmacy medicines is real, common enough to study, and treatable. Link help to medical outcomes (liver, gut, heart, overdose) rather than identity attack.[1][5]
Step 2 — Pharmaceutical opioid / codeine dependence
Systematic review supports structured identification and treatment of codeine dependence; do not offer only “stop buying Nurofen Plus” without a withdrawal and craving plan.[5] Cochrane-level synthesis supports opioid agonist treatment for people dependent on pharmaceutical opioids — methadone or buprenorphine pathways are disease-modifying options analogous to heroin OUD care, individualised to setting and preference.[15]
Teaching induction principles (always check local protocols; do not invent fixed universal milligram laws in exams without context):
- Buprenorphine (including long-acting formulations where available): induct when adequate opioid withdrawal is present (or use local low-dose/micro-induction protocols) to reduce precipitated-withdrawal risk; typical early transmucosal ranges are often discussed in the order of 2–8 mg on day one with titration under supervision — confirm current local product guidance and monitoring.[15]
- Methadone: start low (commonly discussed community teaching bands around 10–30 mg orally on day one in stable outpatients, lower if high overdose risk), titrate slowly with observed dosing early, watch accumulation over several days.[15]
- Supply take-home naloxone education for patient and contacts when opioid dependence is present.[15]
Taper-only strategies may suit highly motivated, lower-dose, well-supported patients but are not the sole ethical option when criteria for OUD are met.[5][15]
Step 3 — Stop the silent partner toxins
Replace combination products with a deliberate plan: non-opioid analgesia ladder, physiotherapy, headache services, CBT-informed pain approaches, and explicit paracetamol daily maximum counselling when any paracetamol remains. Investigate and treat established GI or hepatic injury.[4][7][8]
Step 4 — Gabapentinoids
Review indication; deprescribe when benefit is unclear or misuse is evident; taper rather than abrupt stop after high-dose continuous use; avoid casual co-prescribing with opioids; use prescription monitoring and single-prescriber agreements when diversion is suspected.[9][10][11]
Step 5 — Other agents
- DXM / antihistamines: cessation support, treat underlying anxiety/insomnia, youth-informed brief intervention, emergency pathways for acute toxicity.[2][14]
- Quetiapine diversion: stop unmonitored sedative use; offer evidence-based insomnia care; address methamphetamine come-down context if present without replacing one unmonitored sedative with another indefinitely.
- Stimulant diversion: prescribe ADHD treatment with diversion-risk mitigation (limited quantities, long-acting formulations when appropriate, collateral); treat non-medical use as a substance problem when criteria met.
- Pseudoephedrine: clinical addiction care is rarely the main story — precursor regulation (including Australian pharmacy real-time systems such as Project STOP-type programmes) is a public-health control; candidates should know the policy frame from McKetin’s precursor review logic without inventing statute numbers.[16]
Step 6 — Psychosocial and systems
Motivational interviewing, CBT elements, contingency management where available, family education, and pharmacy partnership (alerts, staged supply, refusal scripts that still offer referral). Real-time prescription monitoring jurisdictions differ — describe the function (detect multi-prescriber opioid/gabapentinoid patterns) rather than fabricate local Act names.[1][3][5]
Specific subtypes and scenarios
Post-2018 Australian codeine legacy. Some patients transitioned to prescribed codeine, other opioids, or non-opioid OTC escalation; others entered treatment. Rescheduling reduced population harm signals but did not abolish individual dependence needing care.[6][7][8]
Frei-type codeine-ibuprofen catastrophe. Young or middle-aged adult with unexplained anaemia, gastric ulcer, or renal impairment and a quiet history of dozens of combination tablets daily — treat both the surgical/medical crisis and the opioid dependence.[4]
OAT client on high-dose pregabalin. Review pain indication, overdose synergy, supervised supply, and collaborative deprescribing — not automatic punitive discharge for a positive screen without a plan.[9][10]
Loperamide withdrawal self-treatment. Offer legitimate withdrawal management or OAT; ban the cardiotoxic workaround with education and ECG if exposure was high.[12][15]
Youth DXM and purple drank. Medical clearance for toxidrome, brief MI, parental/safeguarding as indicated, school/college harm education without sensationalism.[14][2]
Complications and pitfalls
- Missing paracetamol or ibuprofen toxicity while debating “whether codeine addiction is real”[4][8]
- No ECG in loperamide mega-dose[12]
- Abrupt gabapentinoid stop after high-dose use[10]
- Assuming rescheduling means no residual codeine patients need OAT access[6][15]
- Identity confrontation without medical framing → disengagement[1]
- Substituting unmonitored online benzodiazepines or gabapentinoids after losing OTC codeine access
Prognosis and disposition
Many patients stabilise with OAT or structured taper plus treatment of pain, headache, anxiety, and social stressors.[5][15] Relapse risk rises if only the medicine is removed and the original problem is ignored. Higher acuity (inpatient/ED observe/HDU): arrhythmia, severe withdrawal, high suicide risk, unsafe supply at home, complex medical comorbidity.[12][4] Disposition should name follow-up owner: addiction service, GP shared care, pharmacy, pain clinic, and crisis contacts.
Special populations
Youth. DXM, purple drank, stimulant diversion for exams; assess neurodevelopmental and peer context.[14]
Older adults. Sedating antihistamines and gabapentinoids → falls, confusion; deprescribe aggressively when risk exceeds benefit.[10]
Pregnancy. Pharmaceutical opioid dependence needs specialist obstetric-addiction pathways and OAT consideration; punitive discharge increases harm.[15]
Chronic pain and dual diagnosis. Integrated care beats sequential ping-pong between pain and addiction services.[5][9]
Rural / Indigenous contexts. Pharmacy access patterns, stigma, and limited specialist coverage require pragmatic telehealth and primary-care shared models without lowering medical standards.[1][3]
Evidence and guidelines
- Frei 2010 MJA — case series defining severe OTC codeine-ibuprofen morbidity for ANZ teaching.[4]
- Nielsen 2018 MJA — systematic review on identifying and treating codeine dependence.[5]
- Cairns 2020 Addiction; Schaffer 2020 MJA; Noghrehchi 2023 — Australian codeine rescheduling outcomes and related poisoning trends.[6][7][8]
- Smith 2016; Evoy 2021; Schifano 2014 — gabapentinoid misuse evidence arc.[9][10][11]
- Eggleston 2017; Swank 2017 FAERS — loperamide cardiotoxicity.[12][13]
- Nielsen 2022 Cochrane — OAT for pharmaceutical opioid dependence.[15]
- Cooper 2013; Fingleton 2017; Miuli 2020; McKetin 2011 — identity, population rates, purple drank, precursor policy.[1][2][14][16]
Exam pearls
- Feb 2018 Australia codeine Rx-only — quote the policy and cite harm-reduction evaluation literature.[6][7]
- Combination products = two toxidromes.[4][8]
- Loperamide mega-dose → ECG.[12]
- Gabapentinoids are misusable and opioid-synergistic.[9][10]
- Pharmaceutical opioid dependence → consider OAT.[15]
- Purple drank = codeine + promethazine.[14]
- Patients may say “I can’t be an addict” — believe the pharmacology, not the label on the box.[1]
Codeine combinations
- Opioid dependence + partner-drug organ injury
- ANZ rescheduling natural experiment
- OAT or structured taper
Gabapentinoids
- α2δ calcium-channel ligands
- Misuse enriched with opioids
- Deprescribe/taper; watch respiratory synergy
Loperamide mega-dose
- Central opioid effects at extreme dose
- QRS/QTc/VT/VF risk
- ECG + tox/cardiology, not reassurance
References
- [1]Cooper RJ. 'I can't be an addict. I am.' Over-the-counter medicine abuse: a qualitative study BMJ Open, 2013.PMID 23794565
- [2]Fingleton NA, Watson MC, Duncan EM, Matheson C. Non-prescription medicine misuse, abuse and dependence: a cross-sectional survey of the UK general population J Public Health (Oxf), 2017.PMID 28985351
- [3]Van Hout MC, Norman I. Misuse of non-prescription codeine containing products: Recommendations for detection and reduction of risk in community pharmacy Int J Drug Policy, 2016.PMID 26454626
- [4]Frei MY, Nielsen S, Dobbin MD, Tobin CL. Serious morbidity associated with misuse of over-the-counter codeine-ibuprofen analgesics: a series of 27 cases Med J Aust, 2010.PMID 20819050
- [5]Nielsen S, MacDonald T, Johnson JL. Identifying and treating codeine dependence: a systematic review Med J Aust, 2018.PMID 29848240
- [6]Cairns R, Schaffer AL, Brown JA, Pearson SA, Buckley NA. Codeine use and harms in Australia: evaluating the effects of re-scheduling Addiction, 2020.PMID 31577369
- [7]Schaffer AL, Cairns R, Brown JA, Gisev N, Buckley NA, Pearson SA. Changes in sales of analgesics to pharmacies after codeine was rescheduled as a prescription only medicine Med J Aust, 2020.PMID 32200566
- [8]Noghrehchi F, Cairns R, Buckley NA. Hospital admissions for paracetamol poisoning declined following codeine re-scheduling in Australia Int J Drug Policy, 2023.PMID 37116402
- [9]Smith RV, Havens JR, Walsh SL. Gabapentin misuse, abuse and diversion: a systematic review Addiction, 2016.PMID 27265421
- [10]Evoy KE, Sadrameli S, Contreras J, Covvey JR, Peckham AM, Morrison MD. Abuse and Misuse of Pregabalin and Gabapentin: A Systematic Review Update Drugs, 2021.PMID 33215352
- [11]Schifano F. Misuse and abuse of pregabalin and gabapentin: cause for concern? CNS Drugs, 2014.PMID 24760436
- [12]Eggleston W, Clark KH, Marraffa JM. Loperamide Abuse Associated With Cardiac Dysrhythmia and Death Ann Emerg Med, 2017.PMID 27140747
- [13]Swank KA, Wu E, Kortepeter C, McAninch J, Levin RL. Adverse event detection using the FDA post-marketing drug safety surveillance system: Cardiotoxicity associated with loperamide abuse and misuse J Am Pharm Assoc (2003), 2017.PMID 28073687
- [14]Miuli A, Stigliano G, Lalli A, Coladonato M, D'Angelo L, Esposito F, et al. "Purple Drank" (Codeine and Promethazine Cough Syrup): A Systematic Review of a Social Phenomenon with Medical Implications J Psychoactive Drugs, 2020.PMID 32748711
- [15]Nielsen S, Tse WC, Larance B. Opioid agonist treatment for people who are dependent on pharmaceutical opioids Cochrane Database Syst Rev, 2022.PMID 36063082
- [16]McKetin R, Sutherland R, Bright DA, Norberg MM, Shand FL. A systematic review of methamphetamine precursor regulations Addiction, 2011.PMID 21895829