Psych · Addiction psychiatry — stimulant and methamphetamine use
Stimulant and methamphetamine use
Also known as Methamphetamine use disorder · Crystal meth · Ice · Amphetamine-type stimulants · Stimulant use disorder · Methamphetamine-associated psychosis · MAP · ATS · Speed · Cocaine use disorder interface
Exam-exhaustive fellowship reference on stimulant and methamphetamine use — intoxication and withdrawal, methamphetamine-associated psychosis, cardiovascular risk, behavioural disturbance, psychosocial treatment (contingency management, CBT, Matrix), limited pharmacotherapy evidence, dual diagnosis and harm reduction. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Stimulant and methamphetamine use sits at the centre of addiction psychiatry, emergency psychiatry and dual-diagnosis work. The clinical job is not merely to name "ice use," but to define the disorder severity, map intoxication versus withdrawal versus substance-induced mental disorder, exclude life-threatening medical complications, manage behavioural disturbance safely, and deliver evidence-based psychosocial care while being honest about the thin pharmacotherapy evidence base.[1][2]
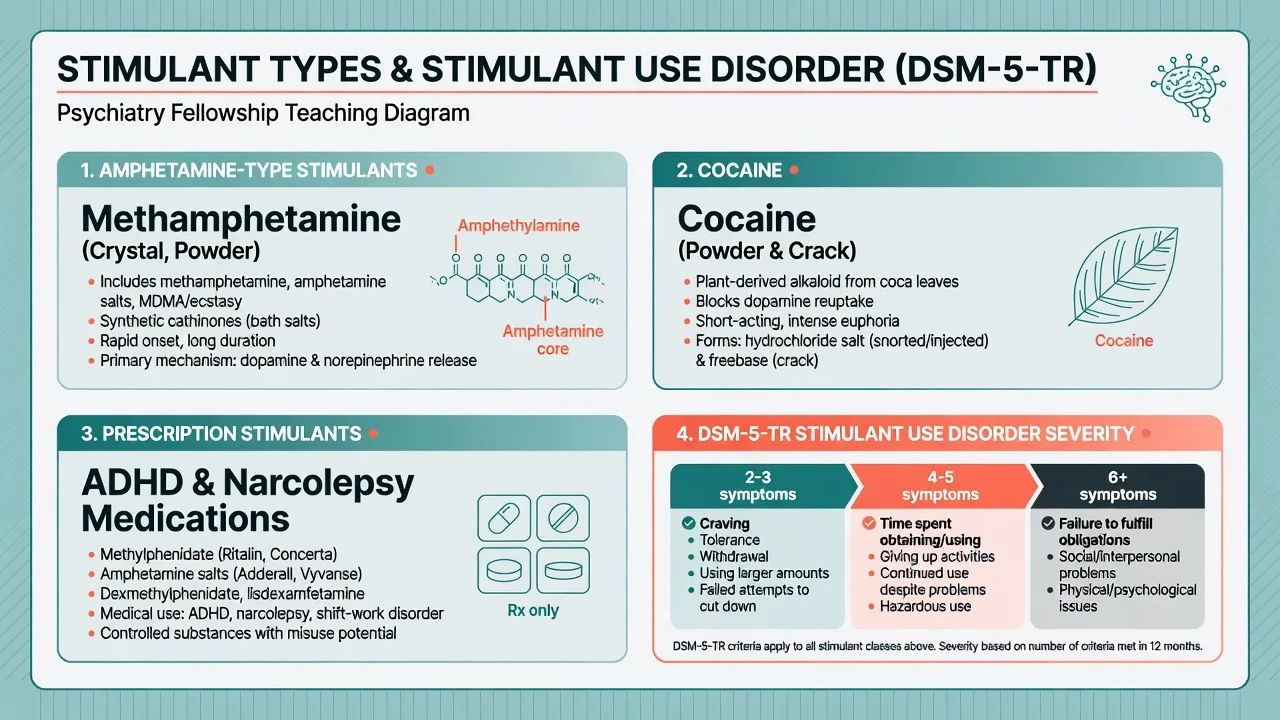
In DSM-5-TR, stimulant use disorder is diagnosed when a problematic pattern of amphetamine-type stimulant, cocaine or other stimulant use leads to clinically significant impairment or distress, with severity graded by criterion count (mild 2–3, moderate 4–5, severe 6 or more) over a 12-month period. ICD-11 frames a spectrum from hazardous use through harmful pattern of use to dependence, plus separate codes for substance-induced mental and behavioural disorders. Fellowship candidates must speak both languages and avoid equating any single positive urine drug screen with a use-disorder diagnosis.[1]
Classification
Clinically useful categories for viva and service design:
| Class | Examples | Exam discriminators |
|---|---|---|
| Amphetamine-type stimulants (ATS) | Methamphetamine (crystal/"ice", base, powder), amphetamine, MDMA, synthetic cathinones | Longer duration of action for meth; MAP risk; ANZ public-health focus |
| Cocaine | Powder cocaine, crack | Shorter half-life; intense binge; local anaesthetic CV effects |
| Prescription stimulants | Methylphenidate, dexamfetamine, lisdexamfetamine | Diversion, ADHD comorbidity, supervised medical use vs misuse |
| Other | Some novel psychoactive stimulants | Unpredictable potency; toxicology may miss agents |
Methamphetamine-associated psychosis (MAP) is a clinical syndrome of delusions and/or hallucinations temporally linked to methamphetamine use. It may remit with abstinence or persist and force a dual formulation with primary psychotic disorder. DSM-5-TR substance-induced psychotic disorder requires that symptoms are not better explained by a primary psychotic disorder and that they develop during or soon after intoxication or withdrawal; examiners test the timeline and the evolution after confirmed abstinence.[7]
Epidemiology and risk factors
Methamphetamine remains a high-burden drug class in Australia and New Zealand, with crystal methamphetamine smoking and injecting patterns driving acute behavioural and medical presentations. Risk clusters include younger adults, male sex (with important exceptions such as chemsex networks), trauma histories, ADHD and externalising disorders, homelessness, criminal justice contact, and polysubstance use (alcohol, cannabis, GHB, opioids).[1]
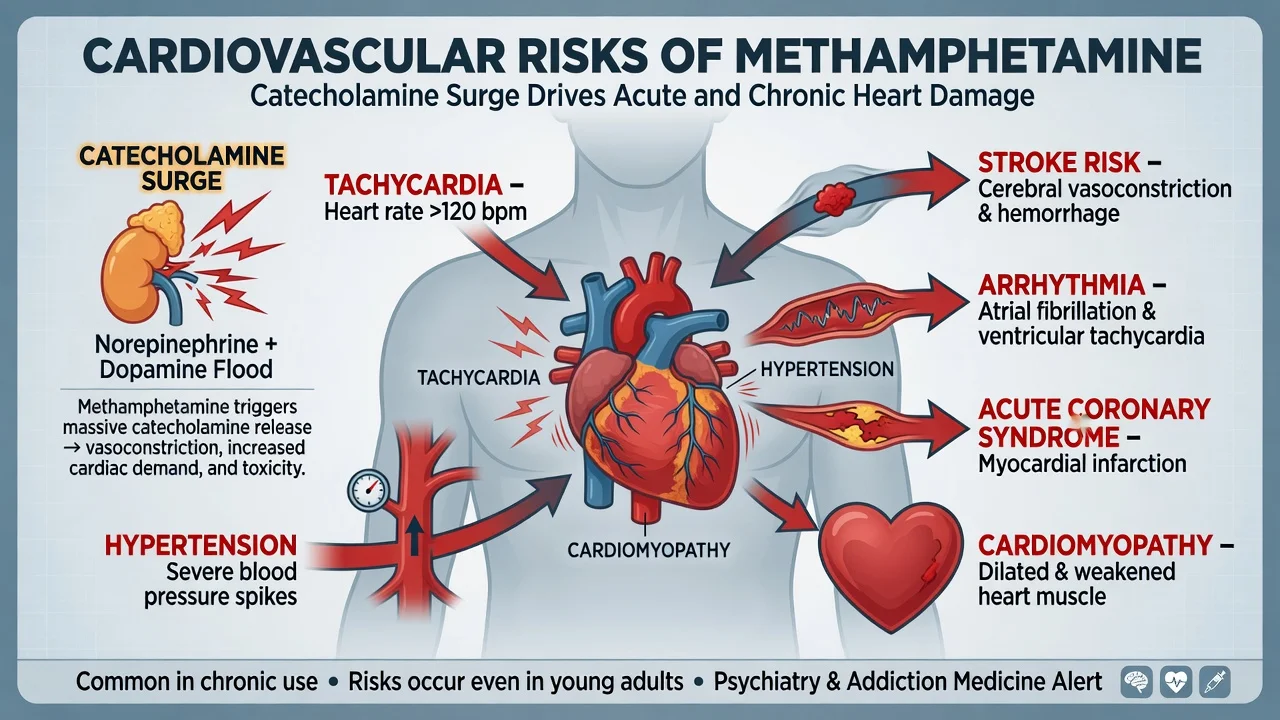
Prospective longitudinal work shows dose-related psychotic symptoms in chronic methamphetamine users: periods of heavier use carry higher odds of psychotic experiences even after accounting for other factors.[7] The same research programme links methamphetamine use periods with elevated violent behaviour risk, reinforcing dynamic risk formulation rather than trait labelling.[8] Cardiovascular disease — acute coronary syndromes, cardiomyopathy, arrhythmias, stroke — is a major non-psychiatric mortality and morbidity pathway.[6]
Pathophysiology
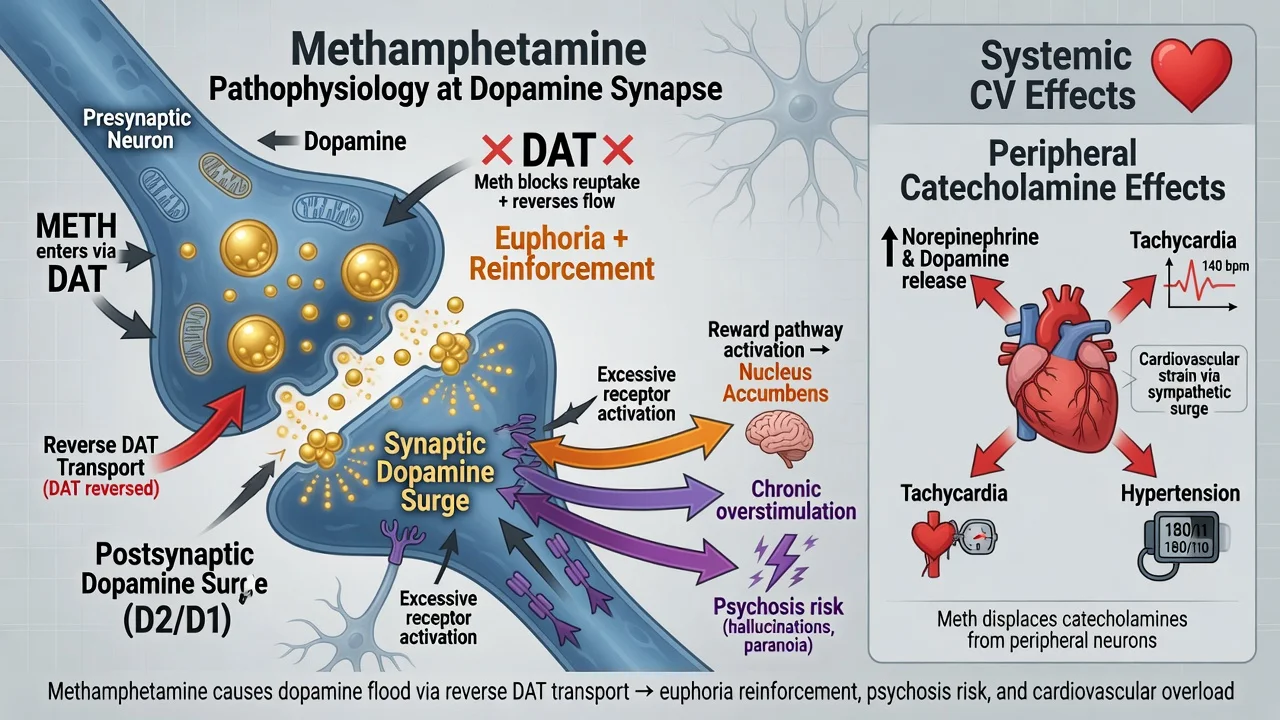
Methamphetamine is a potent releaser and reuptake inhibitor of dopamine, noradrenaline and serotonin. It enters terminals via monoamine transporters and promotes reverse transport, dumping monoamines into the synapse. The resulting striatal dopamine surge underpins intense reinforcement, binge patterning and compulsive re-dosing. Relative to cocaine, methamphetamine has a longer half-life and greater potential for sustained monoaminergic stress and neurotoxicity signals.[6]
Psychosis risk is conceptualised as state-related dopaminergic and broader monoaminergic dysregulation, modulated by dose, frequency, sleep deprivation, concurrent cannabis, and vulnerability (including familial psychosis liability). Peripheral catecholamine excess explains acute tachycardia, hypertension, vasoconstriction and the pathway to myocardial ischaemia, arrhythmia and dilated cardiomyopathy with heavy use.[6][7]
Clinical presentation
Intoxication
Typical intoxication features: euphoria or irritability, increased energy, decreased need for sleep, hypervigilance, pressured speech, mydriasis, tachycardia, hypertension, bruxism, reduced appetite, and at higher doses agitation, paranoia and hallucinations. Severe toxicity includes hyperthermia, seizures, stroke, acute coronary syndrome and excited delirium-type presentations — medical stabilisation first.[17]
Withdrawal and crash
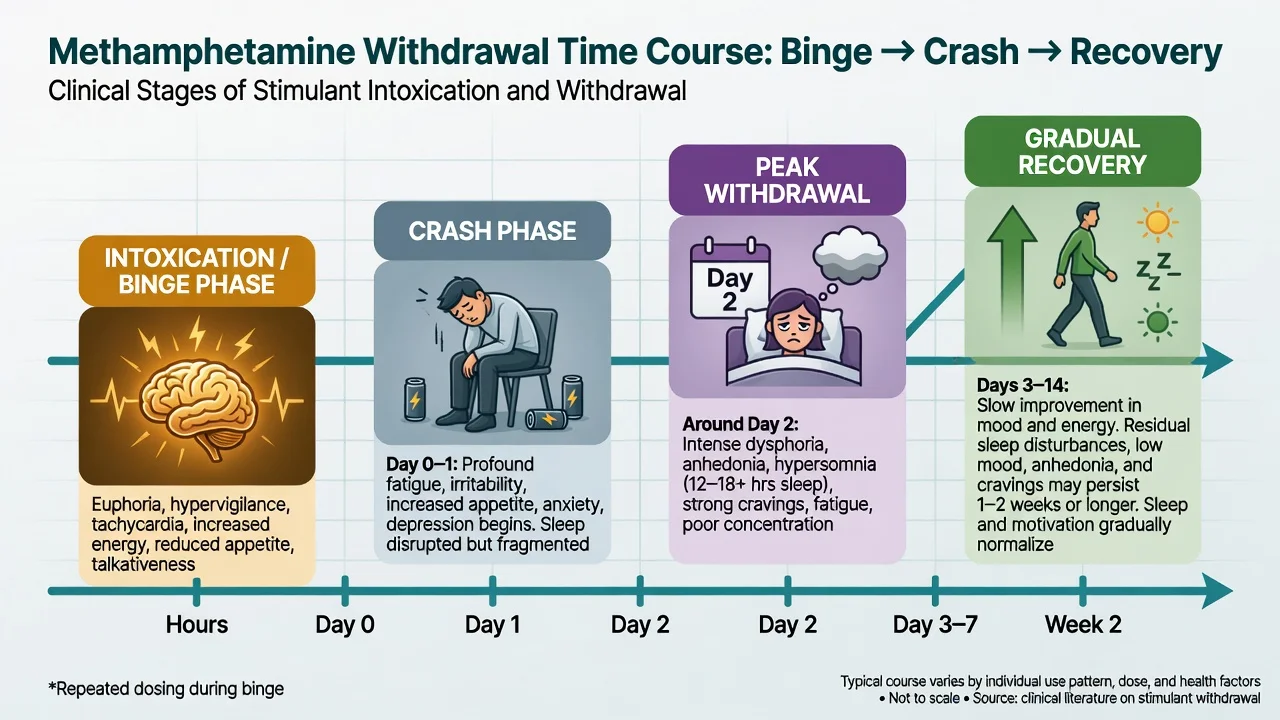
Unlike alcohol or benzodiazepine withdrawal, methamphetamine withdrawal is not typically epileptogenic or autonomically life-threatening, but it is clinically important. Classic description (McGregor et al.): an initial crash with profound fatigue and increased sleep, then a peak of dysphoria, anhedonia, irritability, craving and sleep disturbance around the second day, with symptoms generally improving over about one to two weeks though residual sleep and mood symptoms may linger.[9] Suicide risk can rise in the crash — schedule safety review, not "watch and wait" discharge without a plan.
Methamphetamine-associated psychosis
MAP commonly features persecutory delusions, auditory hallucinations, ideas of reference and formication (tactile "bugs under skin") often with relatively clear consciousness. Symptoms are more likely during high-dose periods and may fluctuate with use intensity.[7] Persistent psychosis after days of abstinence forces careful dual diagnosis work rather than automatic reclassification as lifelong schizophrenia on day one — and equally forbids complacent discharge without follow-up.
Differential diagnosis
| Presentation | Favours MAP / stimulant | Favours alternative | Discriminators |
|---|---|---|---|
| Persecutory psychosis | Clear link to heavy use; improves with abstinence | Primary schizophrenia/bipolar | Timeline, collateral, drug testing limits, family history |
| Agitation + autonomic arousal | Stimulant intoxication | Serotonin toxicity, anticholinergic delirium, thyrotoxicosis | Med list, clonus/hyperreflexia, dry skin vs diaphoresis, fever work-up |
| Chest pain in young adult | Meth-related ACS / demand ischaemia | PE, myocarditis, panic | ECG, troponin, do not psychiatrically dismiss |
| Formication | MAP / intoxication | Primary delusional parasitosis, scabies | Substance history, skin exam |
| Depression post-binge | Stimulant crash | Primary MDD, bipolar depression | Recent use timeline, anhedonia with hypersomnia |
Can't-miss organic differentials: ACS, aortic syndromes, intracranial haemorrhage, seizure, encephalitis, HIV and syphilis-related presentations, rhabdomyolysis with AKI, and hypoglycaemia or other metabolic derangement.[6][17]
Clinical and bedside assessment
Structure the assessment like any high-risk dual-diagnosis encounter:
- Safety first — observations, airway risk if sedated, weapons/means, child protection, vulnerability.
- Substance timeline — agent, route (smoke, inject, snort, oral), quantity/frequency, last use, binge length, polysubstance, prior MAP, prior overdoses.
- MSE with examples — not "paranoid"; e.g. "believes neighbours laser-map his flat and hears third-person commentary; consciousness clear; orientation intact."
- Risk — suicide (especially crash), violence (dynamic with heavy use), absconding, sexual exploitation, driving.
- Capacity and legal status — jurisdiction-specific mental health and emergency detention frameworks; name principles, do not invent section numbers for the wrong country.
- Collateral — family, ambulance, police, GP, AOD services, needle-syringe programmes.
- Dual diagnosis screen — primary psychosis, bipolar, ADHD, PTSD, depression, personality disorder, intellectual disability.
Investigations
| Domain | Tests / actions | Why |
|---|---|---|
| Bedside | HR, BP, temp, SpO2, glucose, ECG | Detect hyperthermia, arrhythmia, ischaemia before psychotropics |
| Bloods | U&E, CK, FBC, LFT, troponin if chest pain | Rhabdomyolysis, AKI, ACS |
| Toxicology | Urine/serum drug screen | Supportive only — false negatives/positives; novel agents missed |
| Infectious | HIV, HBV, HCV, STI panel when indicated | Injecting and sexual risk |
| Imaging / special | CT/MRI, EEG, autoimmune panel if red flags | First psychosis with atypical features, focal neurology, late onset |
| Pregnancy | Test if possible | Changes disposition and drug choices |
Management — resuscitation and acute care
Acute priorities:
- ABC and medical stabilisation — cooling for hyperthermia, cardiac work-up, fluids and CK monitoring for rhabdomyolysis, seizure management per local emergency protocols.
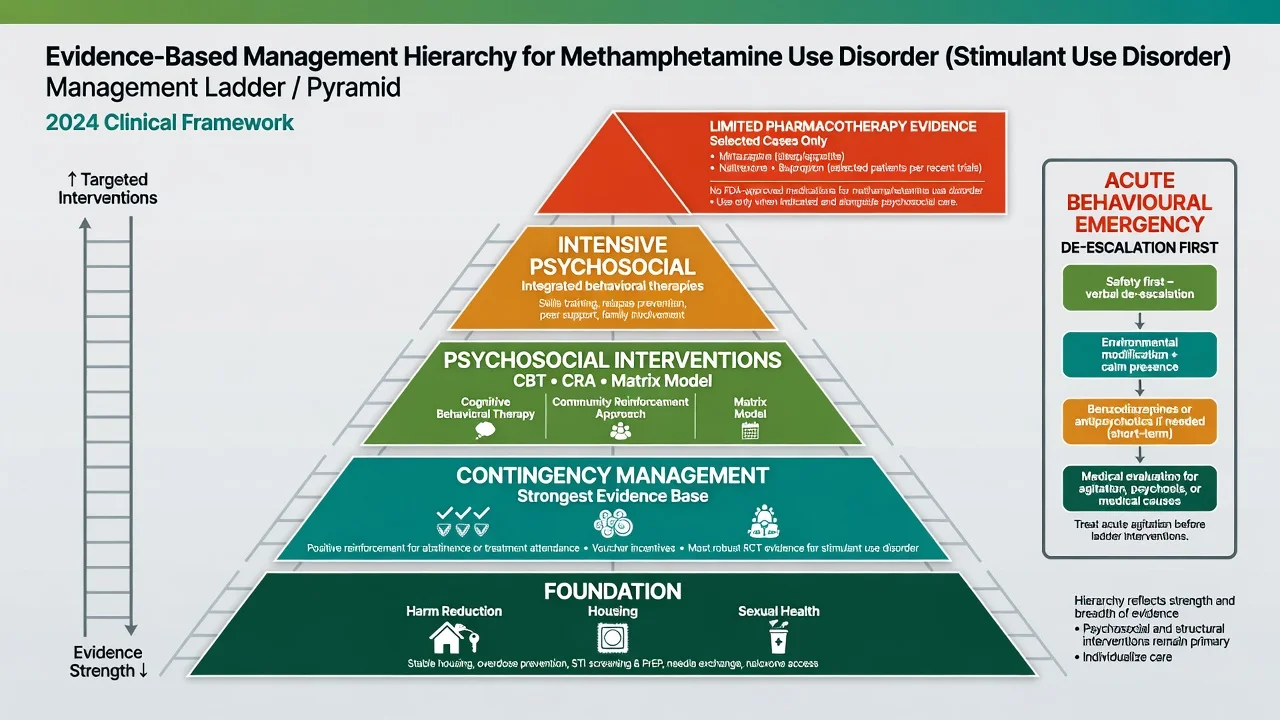
- Behavioural emergency ladder — low-stimulus environment, clear communication, verbal de-escalation, oral medication first when safe, parenteral medication only when needed under local rapid-tranquillisation guidance; avoid unnecessary restraint; continuous observation for deterioration.
- Acute MAP — if psychosis is dangerous or persists and medical causes are addressed, a time-limited antipsychotic can reduce positive symptoms; network meta-analysis supports antipsychotic efficacy signals in MAP with attention to dropout and side-effects. Reassess within days; do not default to indefinite high-dose polypharmacy without dual-diagnosis review.
- Suicide and violence plan — observation level, means restriction, early family contact, crisis pathway.
Management — definitive and stepwise
Psychosocial treatments (first-line)
ASAM/AAAP guidance positions psychosocial interventions as the backbone of stimulant use disorder care. There is no FDA-approved standard pharmacotherapy analogous to opioid agonist treatment.[1] Systematic review-of-reviews work reaches the same practical conclusion: psychosocial approaches carry the most consistent support; medication signals are mixed and context-limited.[2]
Contingency management (CM) — systematic positive reinforcement (e.g. vouchers or prizes contingent on stimulant-negative urine samples or treatment adherence) — has the strongest psychosocial evidence signal across drug use disorders and is repeatedly highlighted for stimulants.[11][12] Australian service reflections note implementation barriers (funding, culture, training) despite clinical interest — viva candidates should name CM and the system barriers, not only the RCT ideal.[18]
CBT, community reinforcement approach (CRA), and the Matrix model multi-element outpatient package (CBT skills, family education, urine monitoring, therapist support) have multi-site methamphetamine programme evidence; Rawson and colleagues showed psychosocial package benefits in methamphetamine dependence treatment settings.[10][11]
Motivational interviewing, peer support, housing first approaches, and sexual health / harm-reduction packages (wound care, safer-use information without moralising, STI/HIV care, naloxone if opioid co-use) are core public-health psychiatry, not optional extras.[1]
Pharmacotherapy — limited evidence, state clearly
Be precise in exams: no agent is a licensed, guideline-mandated first-line anti-craving standard for methamphetamine in the way methadone/buprenorphine is for opioids.[1][16]
| Approach | Evidence snapshot | Exam-level detail |
|---|---|---|
| Mirtazapine | Positive RCTs in selected populations (Colfax 2011; Coffin 2020); more recent large trial data also inform benefit-risk discussion | Trial protocols commonly used mirtazapine 30 mg orally at night; counsel sedation, weight gain, rare agranulocytosis/neutropenia vigilance per product information; adjunct to psychosocial care, not solo cure[4][5][15] |
| Naltrexone XR + bupropion XL (ADAPT-2) | Trivedi et al. NEJM 2021: combination superior to placebo on a response outcome in methamphetamine use disorder | Extended-release injectable naltrexone 380 mg IM every 3 weeks plus extended-release bupropion 450 mg orally daily after staged titration in trial design; exclude contraindication to naltrexone (including anticipated opioid need); monitor BP, seizure risk factors, mood; still not a universal standard of care[3] |
| N-acetylcysteine | McKetin RCT did not establish clear efficacy as a routine treatment | Do not promote as proven anti-craving standard[14] |
| Agonist / other candidates | Network meta-analyses continue to explore options; none displaces psychosocial first-line framing | Quote uncertainty; avoid inventing doses for unproven agents as if guideline-mandated[19][20] |
| Antipsychotics for MAP | Short-term symptom control supported; NMA informs relative efficacy/dropout | Time-limit; review for primary psychosis pathway if symptoms persist offline stimulant use[13] |
Reduced use (not only continuous abstinence) is an emerging trial outcome of clinical relevance; interpret pharmacotherapy literature with that endpoint literacy.[20]
Dual diagnosis and integrated care
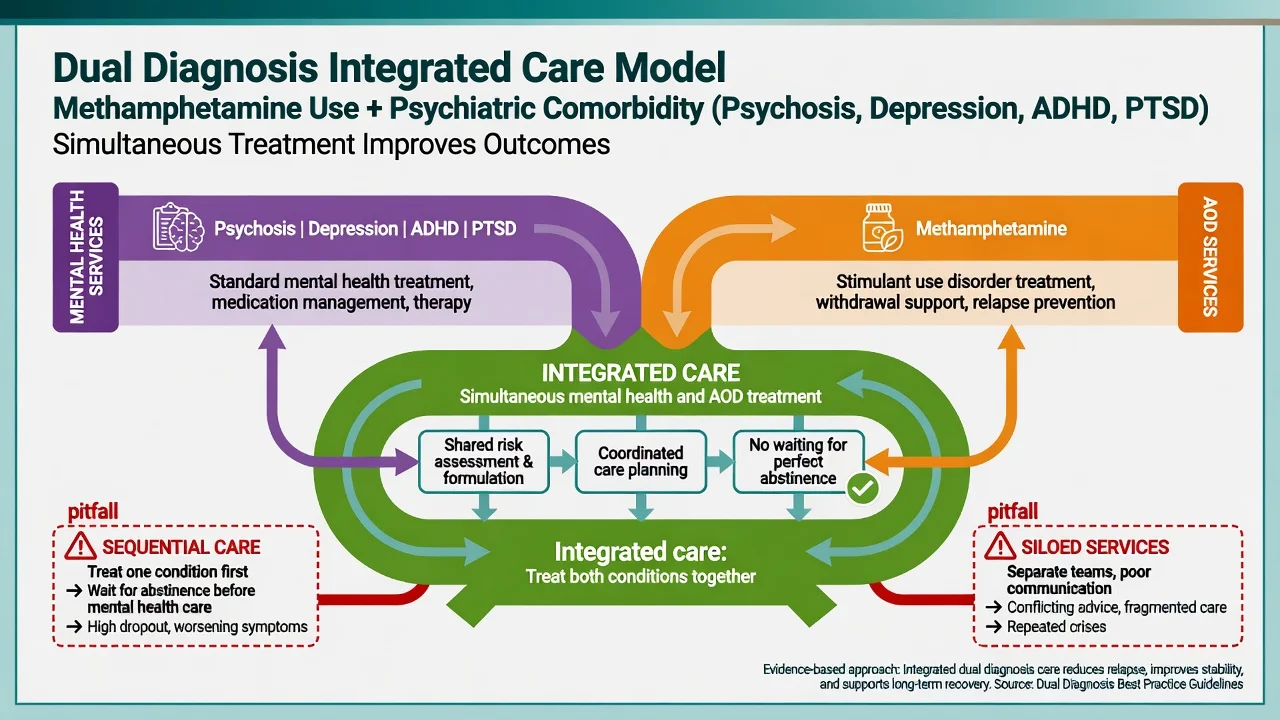
Never withhold treatment of acute psychosis, mania or severe depression pending mythical perfect abstinence. Integrated mental health and alcohol-and-other-drug (AOD) care with shared formulation outperforms sequential "treat one then the other" pathways in principle and in dual-diagnosis guidance culture across ANZ/UK systems.[1][16]
Specific subtypes and scenarios
Crystal meth binge with behavioural disturbance. Medical obs, de-escalation, short-acting sedation per local protocol if needed, MAP assessment, overnight observation for crash suicidality.[17]
Persistent MAP after abstinence. Re-open organic work-up thresholds, family history, cognitive baseline, early intervention or dual-diagnosis follow-up; consider whether criteria for primary psychotic disorder are emerging.[7]
Chemsex (meth ± GHB ± other). Sexual risk, consent capacity while intoxicated, GHB withdrawal risk if dependent, stigma-sensitive engagement, STI/HIV pathways.[1]
Prescription stimulant diversion. Separate legitimate ADHD treatment (supervised, functional gains) from misuse; do not abruptly abandon genuine ADHD care without a plan.[1]
Cocaine interface. Shorter action, intense craving cycles; CM still central; CV risk remains high.[1][12]
Methamphetamine cardiomyopathy. Coordinate cardiology; counsel that continued use worsens prognosis; psychiatric engagement is part of secondary prevention.[6]
Custody / forensic transfer. Document intoxication stage, MAP, risk, medication given, and observation needs at handover.[8][17]
Complications and pitfalls
- Medical: ACS, cardiomyopathy, arrhythmia, stroke, hyperthermia, rhabdomyolysis, dental destruction, skin infections, blood-borne viruses.
- Psychiatric: MAP, crash depression and suicide, anxiety, cognitive complaints, trauma re-enactment.
- Pitfalls: lifelong schizophrenia label after a single MAP episode; refusing antipsychotics when dangerous psychosis is present; inventing a "meth detox protocol" with unproven high-dose polypharmacy; missing ACS in a 28-year-old; discharging a crashing patient without suicide assessment; punitive discharge without AOD follow-up; ignoring CM because "we do not have vouchers" without any reinforcement strategy.
Prognosis and disposition
Prognosis tracks severity and route of use, social capital (housing, relationships), dual diagnosis, treatment access (especially CM-capable services), and engagement. Disposition is a ladder: medical clearance → psychiatric emergency observation or inpatient unit if high risk → community shared care (mental health + AOD) with early review after MAP or suicidal crash. Recovery endpoints include reduced use or abstinence, retained housing, vocational roles and restored relationships — not urine purity alone.[1][20]
Special populations
Youth. High MAP and first-episode psychosis interface; family work; avoid diagnostic fatalism.[1][7]
Pregnancy. Prioritise psychosocial care, obstetric liaison, and harm reduction; do not invent unproven pharmacotherapy as standard; counsel fetal and maternal CV risks of continued meth use.[1]
Older adults. Lower prevalence but high CV vulnerability; covert use possible.[6]
Indigenous and culturally diverse communities (ANZ). Partner with culturally safe and community-controlled services; address social determinants; avoid deficit-only framing.[1][18]
Intellectual disability / autism. Behavioural crisis may reflect pain, fear or sensory load plus intoxication — adapt communication.[1]
Forensic. Dynamic risk, MAP, and medication handover dominate.[8]
Evidence, guidelines and regional differences
| Source | High-yield takeaway |
|---|---|
| ASAM/AAAP 2024 StUD CPG | Psychosocial first-line; structured recommendations on assessment, CM, and cautious pharmacotherapy context[1] |
| Ronsley review-of-reviews 2020 | Psychosocial more consistent than pharmacotherapy across stimulant literature[2] |
| BAP 2026 substance dependence consensus | Contemporary UK pharmacological framing for dependence syndromes including stimulants — read alongside psychosocial primacy[16] |
| ADAPT-2 (Trivedi 2021) | Naltrexone XR + bupropion XL response signal — selected, specialist-context discussion, not universal mandate[3] |
| Mirtazapine RCTs | Colfax, Coffin, and later McKetin trial stream — population-specific benefit-risk counselling[4][5][15] |
| McKetin psychosis and violence cohorts | Dose-related psychosis; dynamic violence association[7][8] |
| McGregor withdrawal 2005 | Time course still taught as classic reference[9] |
| Rawson Matrix multi-site | Multi-element psychosocial package evidence in methamphetamine treatment[10] |
| ANZ implementation | CM desired but operationally constrained in many services — name the gap in systems viva answers[18] |
ANZ: Crystal methamphetamine ("ice") drives much of the acute psychiatry load; dual-diagnosis teams and emergency departments see MAP and behavioural disturbance frequently; CM implementation is uneven.[18] UK: BAP consensus and NICE dual-diagnosis principles emphasise integrated care; stimulant patterns vary by region. US: ASAM/AAAP CPG is the major specialty society reference; CM has a longer research history with periodic policy friction around incentives. State the guideline you are quoting.
Exam pearls
- No methadone equivalent for meth — saying "start substitution therapy" without nuance fails.[1]
- Name contingency management as the highest-yield psychosocial modality for stimulants.[12]
- MAP is dose-related; clear consciousness helps separate from delirium.[7]
- Withdrawal is usually not seizures-like alcohol — but suicide and CV events still kill.[9][6]
- If you quote ADAPT-2, state naltrexone XR 380 mg IM every 3 weeks + bupropion XL 450 mg daily accurately, with exclusions.[3]
- If you quote mirtazapine trials, 30 mg nocte is the common studied dose — cite, do not invent alternatives as if universal protocol.[4][5]
- Violence risk is dynamic with heavy use periods.[8]
- Legal frameworks are jurisdiction-specific — principles yes, invented section numbers no.[1]
- Integrated dual diagnosis: treat both, do not wait for perfect abstinence.[1][16]
METH CARE (acute to definitive)
References
- [1]ASAM/AAAP Clinical Guideline Committee The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder J Addict Med, 2024.PMID 38669101
- [2]Ronsley C, Nolan S, Knight R, et al. Treatment of stimulant use disorder: A systematic review of reviews PLoS One, 2020.PMID 32555667
- [3]Trivedi MH, Walker R, Ling W, et al. Bupropion and Naltrexone in Methamphetamine Use Disorder N Engl J Med, 2021.PMID 33497547
- [4]Coffin PO, Santos GM, Hern J, et al. Effects of Mirtazapine for Methamphetamine Use Disorder Among Cisgender Men and Transgender Women Who Have Sex With Men: A Randomized Clinical Trial JAMA Psychiatry, 2020.PMID 31825466
- [5]Colfax GN, Santos GM, Das M, et al. Mirtazapine to reduce methamphetamine use: a randomized controlled trial Arch Gen Psychiatry, 2011.PMID 22065532
- [6]Kevil CG, Goeders NE, Woolard MD, et al. Methamphetamine Use and Cardiovascular Disease Arterioscler Thromb Vasc Biol, 2019.PMID 31433698
- [7]McKetin R, Lubman DI, Baker AL, et al. Dose-related psychotic symptoms in chronic methamphetamine users: evidence from a prospective longitudinal study JAMA Psychiatry, 2013.PMID 23303471
- [8]McKetin R, Lubman DI, Najman JM, et al. Does methamphetamine use increase violent behaviour? Evidence from a prospective longitudinal study Addiction, 2014.PMID 24400972
- [9]McGregor C, Srisurapanont M, Jittiwutikarn J, et al. The nature, time course and severity of methamphetamine withdrawal Addiction, 2005.PMID 16128721
- [10]Rawson RA, Marinelli-Casey P, Anglin MD, et al. A multi-site comparison of psychosocial approaches for the treatment of methamphetamine dependence Addiction, 2004.PMID 15139869
- [11]Dutra L, Stathopoulou G, Basden SL, et al. A meta-analytic review of psychosocial interventions for substance use disorders Am J Psychiatry, 2008.PMID 18198270
- [12]Pfund RA, Ginley MK, Boness CL, et al. Contingency Management for Drug Use Disorders: Meta-Analysis and Application of Tolin's Criteria Clin Psychol (New York), 2024.PMID 38863566
- [13]Srisurapanont M, Likhitsathian S, Suttajit S, et al. Efficacy and dropout rates of antipsychotic medications for methamphetamine psychosis: A systematic review and network meta-analysis Drug Alcohol Depend, 2021.PMID 33385693
- [14]McKetin R, Dean OM, Turner A, et al. N-acetylcysteine (NAC) for methamphetamine dependence: A randomised controlled trial EClinicalMedicine, 2021.PMID 34308314
- [15]McKetin R, Shoptaw S, Saunders L, et al. Mirtazapine for Methamphetamine Use Disorder: A Randomized Clinical Trial JAMA Psychiatry, 2026.PMID 41920558
- [16]Sinclair JMA, Kalk NJ, Kaar SJ, et al. Evidence-based consensus guidelines for the pharmacological management of substance dependence: Recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2026.PMID 41731947
- [17]Fries A, Christ M, Nickl H, et al. The Diagnosis and Treatment of Stimulant-Related Emergencies Dtsch Arztebl Int, 2025.PMID 40991352
- [18]Clay S, Wilkinson Z, Ginley M, et al. The reflections of health service providers on implementing contingency management for methamphetamine use disorder in Australia Drug Alcohol Rev, 2024.PMID 38704742
- [19]Khalili M, Sadeghirad B, Bach P, et al. Management of Amphetamine and Methamphetamine Use Disorders: A Systematic Review and Network Meta-analysis of Randomized Trials Int J Ment Health Addict, 2025.PMID 41394525
- [20]Amin-Esmaeili M, Farokhnia M, Mojtabai R, et al. Evaluating Reduced Use and Abstinence as Outcomes in Pharmacotherapy Trials for Stimulant Use Disorder: A Meta-Analysis of 12 Randomized Clinical Trials JAMA Psychiatry, 2026.PMID 42234418