Psych · Addiction psychiatry — stimulant intoxication and withdrawal
Stimulant intoxication and withdrawal
Also known as Methamphetamine intoxication · Stimulant toxicity · Ice intoxication · Crystal meth crash · Amphetamine withdrawal · Cocaine intoxication · Methamphetamine-associated psychosis · MAP · Sympathomimetic toxidrome
Fellowship-depth atlas on stimulant intoxication and withdrawal as acute clinical states — medical toxicity (hyperthermia, ACS, rhabdomyolysis, stroke), behavioural disturbance, methamphetamine-associated psychosis, crash time course and suicide risk, supportive care, and the explicit absence of an approved anti-craving or substitution standard of care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Stimulant intoxication and withdrawal are time-limited clinical states, not synonyms for chronic stimulant use disorder. Fellowship work is to recognise the sympathomimetic toxidrome, exclude can't-miss medical toxicity, manage behavioural disturbance and methamphetamine-associated psychosis (MAP) safely, anticipate the crash, and link to evidence-based ongoing care without inventing a methadone-equivalent for stimulants.[1][15]
In DSM-5-TR, stimulant intoxication and stimulant withdrawal are coded syndromes with specified symptom clusters; ICD-11 frames acute intoxication and withdrawal for stimulants including amphetamine-type substances and cocaine. These states sit alongside — but are not identical to — stimulant use disorder severity and substance-induced psychotic disorder. A single positive urine screen neither proves current intoxication nor diagnoses a use disorder.[1]
This leaf topic is the acute bay view. The companion topic on stimulant and methamphetamine use covers chronic disorder treatment in more depth; here the examinable core is toxicity, MAP, withdrawal time course, and the pharmacotherapy vacuum for anti-craving care.[1][7]
Classification
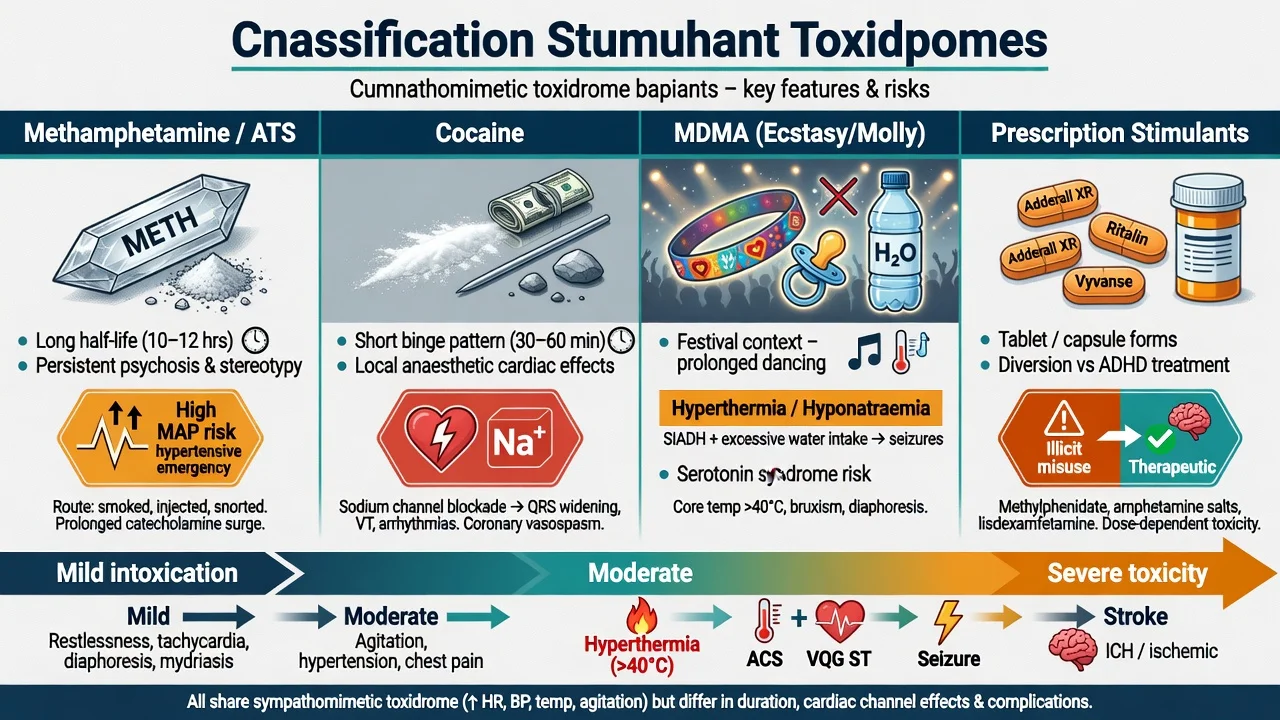
| Class | Examples | Acute exam discriminators |
|---|---|---|
| Amphetamine-type stimulants (ATS) | Methamphetamine (crystal/"ice"), amphetamine, synthetic cathinones | Longer duration; high MAP burden in ANZ; binge-runs |
| Cocaine | Powder, crack | Short action; intense binge-crash; sodium-channel cardiac effects |
| MDMA | Ecstasy/"Molly" | Festival context; hyperthermia; hyponatraemia risk |
| Prescription stimulants | Methylphenidate, dexamfetamine, lisdexamfetamine | Diversion vs legitimate ADHD treatment |
MAP / substance-induced psychotic disorder requires psychotic symptoms temporally linked to intoxication or withdrawal that are not better explained by a primary psychotic disorder. Examiners test timeline, collateral, and course after confirmed abstinence — not day-one lifelong schizophrenia labels after a single ice binge.[3]
Epidemiology and risk factors
Crystal methamphetamine remains a major driver of ED and acute psychiatry presentations in Australia and New Zealand. Severity modifiers include high dose, smoking or injecting routes, multi-day binge duration, hot environments, physical restraint, and polysubstance use (alcohol, cannabis, GHB, opioids).[1][15]
Prospective longitudinal data show dose-related psychotic symptoms during heavier methamphetamine use periods, and elevated violent behaviour during heavy-use windows — risk is dynamic, not a fixed moral attribute.[3][4] Cardiovascular disease (ACS, cardiomyopathy, arrhythmia, stroke) is a core mortality pathway even in younger adults.[5]
Pathophysiology
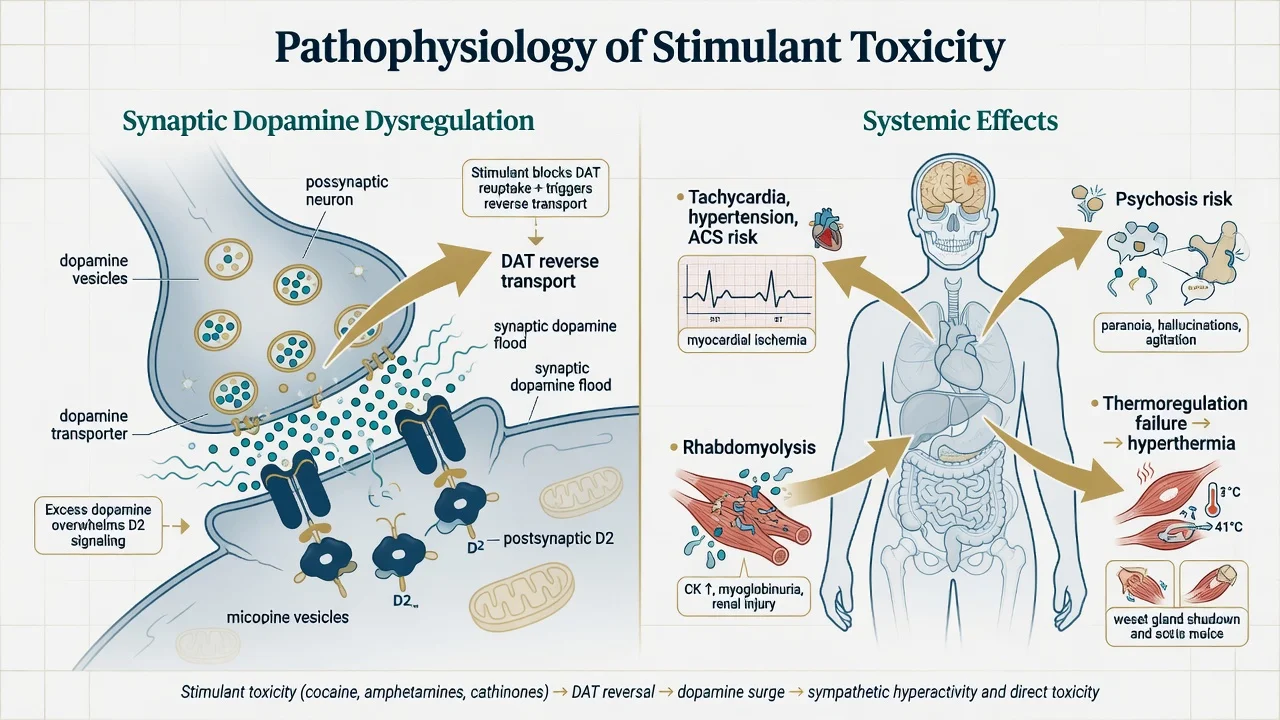
Amphetamine-type stimulants enter monoamine terminals and promote reverse transport at DAT (and affect NET/SERT), flooding synaptic dopamine and noradrenaline. Cocaine primarily blocks reuptake and has local-anaesthetic sodium-channel effects relevant to QRS widening and arrhythmia. The striatal dopamine surge underpins reinforcement and binge re-dosing; sustained monoaminergic stress with methamphetamine contributes to psychosis risk and peripheral toxicity.[5][15]
Peripheral catecholamine excess explains tachycardia, hypertension, vasoconstriction, demand ischaemia, stroke risk, thermoregulatory failure and rhabdomyolysis. Crash and withdrawal reflect monoamine dysregulation: hypersomnia, anhedonia, dysphoria and craving without the life-threatening autonomic withdrawal of alcohol or benzodiazepines.[2][5]
Clinical presentation
Intoxication and medical toxicity
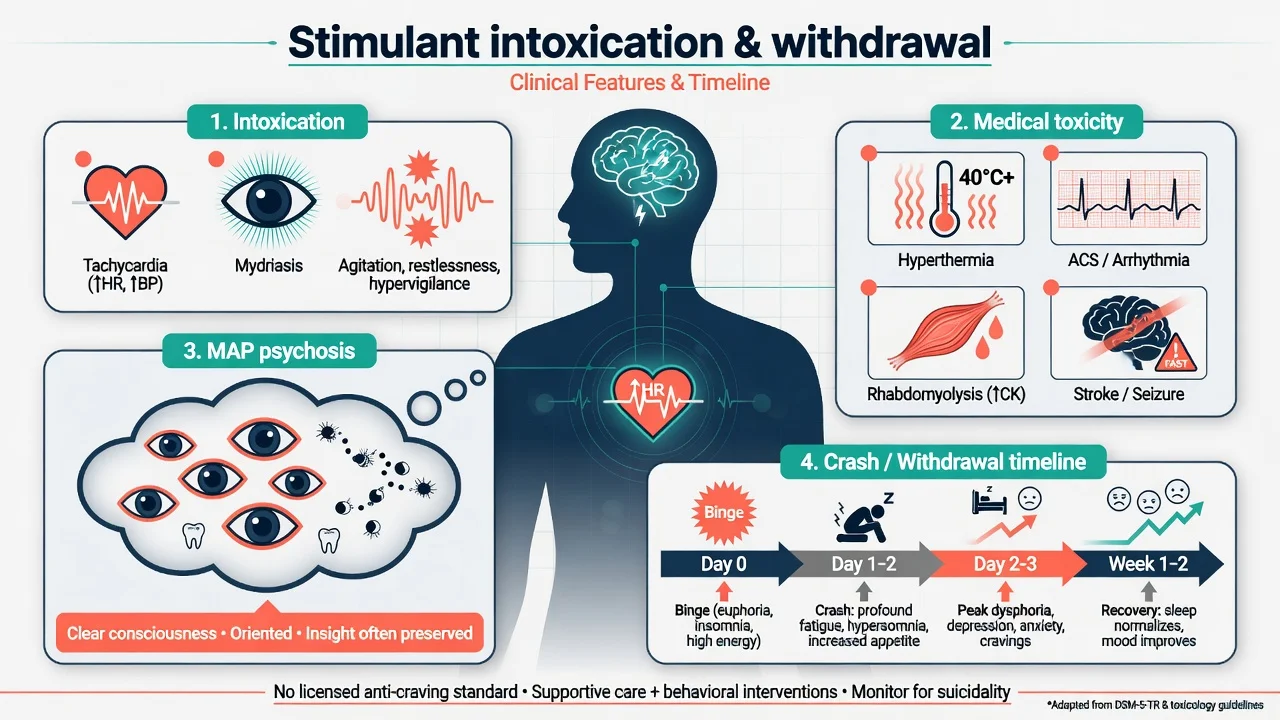
Typical intoxication: euphoria or irritability, increased energy, decreased need for sleep, hypervigilance, mydriasis, tachycardia, hypertension, bruxism, reduced appetite, and at higher doses agitation, paranoia and hallucinations.[15]
Severe toxicity is not "more psychiatry" — it is medicine: hyperthermia, seizures, acute coronary syndromes, intracranial haemorrhage or ischaemic stroke, rhabdomyolysis with AKI, and excited delirium-type presentations with extreme agitation and metabolic derangement. Resuscitation precedes formulation.[5][15]
Methamphetamine-associated psychosis
MAP commonly features persecutory delusions, auditory hallucinations, ideas of reference and formication, often with relatively clear consciousness (helping separate pure delirium). Symptoms track dose and frequency and may fluctuate with use intensity.[3] Persistent psychosis after days of abstinence forces dual formulation with primary psychotic disorder — not automatic reclassification on day one, and not complacent discharge without follow-up.
Withdrawal and crash
Unlike alcohol or benzodiazepine withdrawal, methamphetamine withdrawal is not typically epileptogenic or autonomically life-threatening, but it is clinically important and sometimes fatal via suicide. Classic description (McGregor et al.): initial crash with profound fatigue and increased sleep; peak dysphoria, anhedonia, irritability, craving and sleep disturbance around the second day; general improvement over about one to two weeks with residual sleep and mood symptoms possible.[2] Cocaine's shorter half-life produces a sharper, shorter crash cycle; multi-day ice runs produce longer crash windows.
Differential diagnosis
| Presentation | Favours stimulant state | Favours alternative | Discriminators |
|---|---|---|---|
| Persecutory psychosis | Clear heavy-use link; improves with abstinence | Primary schizophrenia/bipolar | Timeline, collateral, drug testing limits, family history |
| Agitation + autonomic arousal | Stimulant intoxication | Serotonin toxicity, anticholinergic delirium, thyrotoxicosis | Med list, clonus, skin dryness vs diaphoresis, fever work-up |
| Chest pain in young adult | Meth/cocaine ACS or demand ischaemia | PE, myocarditis, panic alone | ECG, troponin — never psychiatrically dismiss |
| Formication | MAP / intoxication | Scabies, primary delusional parasitosis | Substance history, skin exam |
| Depression post-binge | Stimulant crash | Primary MDD, bipolar depression | Recent use timeline, hypersomnia pattern |
| Collapse / low RR | Opioid or GHB co-intoxication | Pure stimulant (usually activated) | Naloxone trial if opioid possible; observe for delayed respiratory depression |
Can't-miss organics: ACS, aortic syndromes, ICH, seizure, encephalitis, HIV/syphilis CNS disease, rhabdomyolysis with AKI, hypoglycaemia and other metabolic derangement.[5][15]
Clinical and bedside assessment
- Safety and ABC first — temperature, HR, BP, SpO2, glucose, airway risk if later sedated, weapons/means, child protection.
- Substance timeline — agent, route, quantity/frequency, last use, binge length, polysubstance, prior MAP, prior ACS/seizure.
- MSE with examples — not "paranoid"; e.g. "believes neighbours laser-map his flat; third-person commentary; consciousness clear; oriented."
- Risk — suicide (especially crash), violence (dynamic with heavy use), absconding, sexual exploitation, driving.
- Capacity and legal status — jurisdiction-specific principles; do not invent foreign section numbers.
- Collateral — ambulance, police, family, GP, AOD and needle-syringe services.
- Dual diagnosis screen — primary psychosis, bipolar, ADHD, PTSD, depression, personality disorder.
Investigations
| Domain | Tests / actions | Why |
|---|---|---|
| Bedside | HR, BP, temp, SpO2, glucose, ECG | Hyperthermia, arrhythmia, ischaemia before psychotropics |
| Bloods | U&E, CK, FBC, LFT, troponin if chest pain | Rhabdomyolysis, AKI, ACS |
| Toxicology | Urine/serum drug screen | Supportive only — false negatives/positives; novel agents missed |
| Infectious | HIV, HBV, HCV, STI when indicated | Injecting and sexual risk |
| Imaging / special | CT/MRI, EEG, autoimmune panel if red flags | Focal neurology, atypical first psychosis, late onset, trauma |
| Pregnancy | Test if possible | Changes disposition and drug choices |
Management — resuscitation and acute care
Acute priorities:
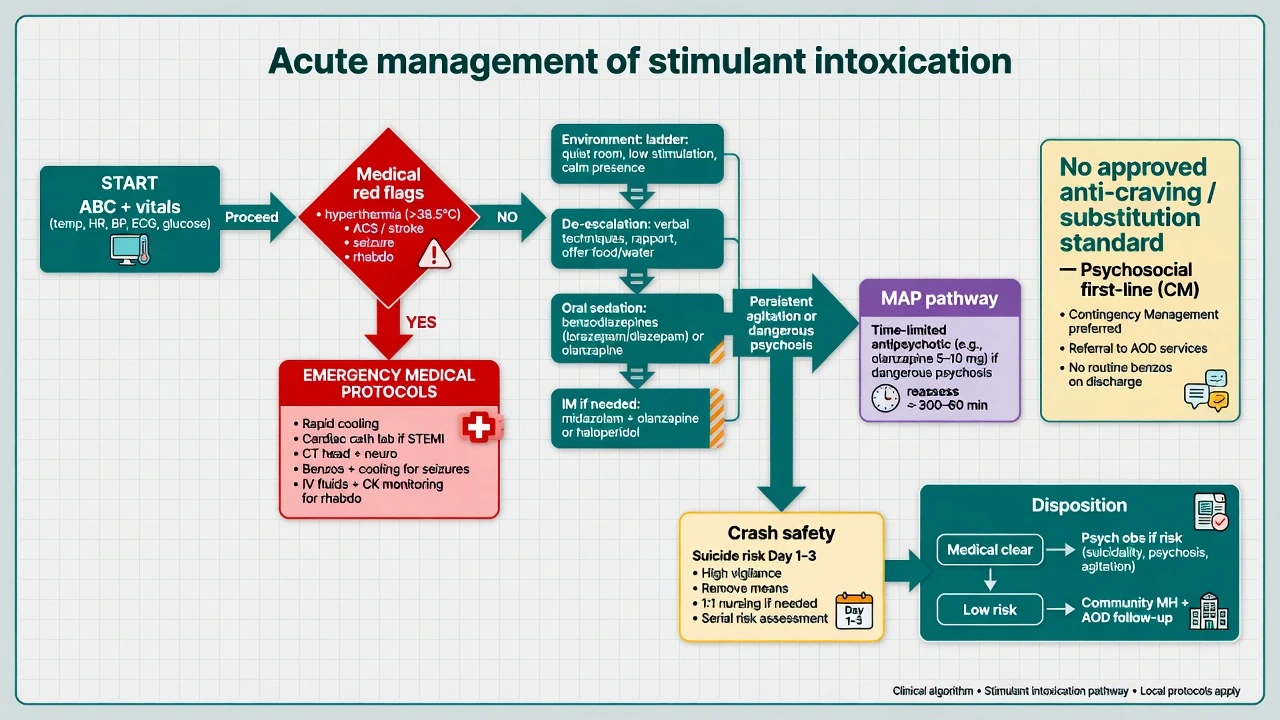
- ABC and medical stabilisation — active cooling for significant hyperthermia per local ED protocol; ACS pathway for chest pain/ECG change; IV fluids and serial CK for rhabdomyolysis; seizure management per emergency protocols; avoid unnecessary restraint that worsens hyperthermia.
- Behavioural emergency ladder — low-stimulus environment, clear communication, verbal de-escalation, oral medication first when safe; parenteral medication only when required under local rapid-tranquillisation guidance with continuous observation.
- Acute MAP — if psychosis is dangerous or persists after medical screen, a time-limited antipsychotic can reduce positive symptoms; network meta-analysis supports antipsychotic efficacy signals in methamphetamine psychosis with attention to dropout and side-effects. Reassess within days; avoid indefinite high-dose polypharmacy without dual-diagnosis review.[6]
- Example acute psychotropic dosing (local protocol always overrides) — many ANZ ED pathways use oral olanzapine 5–10 mg (or equivalent) for agitation/psychosis when oral route is safe; parenteral options (e.g. IM olanzapine or midazolam combinations) only per local RT policy with airway and ECG awareness. Cite and time-limit; monitor for oversedation if co-intoxicants present.[6][15]
- Suicide and violence plan — observation level, means restriction, early family contact, crisis pathway — especially into the crash window.
- Opioid co-intoxication — if hypoventilation or known opioid co-use, titrate naloxone to ventilation (typical teaching increments 0.4–2 mg IV/IM/IN, repeated as needed) and observe for re-sedation.[15]
Management — definitive, withdrawal support and anti-craving vacuum
Supportive care for withdrawal (what is standard)
There is no mandatory multi-drug "stimulant detox protocol." Standard care is supportive: hydration, nutrition, sleep opportunity, brief motivational engagement, treatment of concurrent medical illness, and active suicide monitoring through the crash. Symptomatic treatment of severe insomnia or anxiety may be considered short-term with caution (sedative load, diversion, interaction with residual stimulants) — never as a substitute for safety planning.[1][2]
No approved anti-craving / substitution standard
Be precise in exams: ASAM/AAAP 2024 positions psychosocial interventions as the backbone of stimulant use disorder care. There is no FDA-approved standard pharmacotherapy analogous to opioid agonist treatment. Saying "start substitution therapy" for methamphetamine as if methadone-equivalent exists is an exam fail.[1][7][16]
| Approach | Role in acute/post-acute care | Exam-level precision |
|---|---|---|
| Contingency management | Strongest psychosocial signal for reducing stimulant use | Name CM for ongoing care after the acute episode; implementation barriers exist in many ANZ services[11][12] |
| CBT / CRA / Matrix | Structured outpatient psychosocial packages | Rawson multi-site methamphetamine programme evidence[13] |
| Mirtazapine | Selected trial signal for reducing meth use — not acute withdrawal standard | Common studied dose mirtazapine 30 mg orally at night; counsel sedation/weight gain; specialist context after acute stabilisation[9][10] |
| Naltrexone XR + bupropion XL (ADAPT-2) | Response signal in methamphetamine use disorder | Trial regimen: extended-release injectable naltrexone 380 mg IM every 3 weeks plus extended-release bupropion 450 mg orally daily after staged titration; exclusions (anticipated opioid need, seizure risk, BP); not universal acute standard of care[8] |
| N-acetylcysteine | Negative/limited routine efficacy signal | Do not promote as proven anti-craving standard[14] |
| Antipsychotics for MAP | Short-term symptom control | Time-limit; review if symptoms persist offline stimulant use[6] |
Dual diagnosis and discharge
Never withhold treatment of dangerous psychosis or severe depression pending mythical perfect abstinence. Before discharge: medical clearance, documented suicide/violence plan, AOD and mental-health follow-up, harm-reduction advice (safer-use information without moralising, wound care, STI/HIV pathways, take-home naloxone if opioid co-use), and housing/peer support where available.[1][16]
Specific subtypes and scenarios
Crystal meth binge with MAP and behavioural disturbance. Obs, de-escalation, short time-limited antipsychotic if dangerous psychosis, overnight observation into crash for suicidality.[3][15]
Cocaine chest pain. ACS work-up first; do not diagnose "just anxiety" in a 28-year-old with crack use and diaphoresis.[5]
MDMA festival presentation. Hyperthermia and hyponatraemia pathways; serotonin toxicity differential if polypharmacy.[15]
Crash day 2 after multi-day ice run. Peak dysphoria window — safety plan, not "he's fine now that he's sleepy."[2]
Meth + GHB or meth + opioids. Mixed toxidrome; delayed respiratory depression risk; naloxone if opioids possible.[15]
Persistent psychosis after abstinence. Dual formulation; early intervention or dual-diagnosis follow-up; reopen organic work-up thresholds if atypical.[3]
Custody transfer. Document intoxication stage, MAP features, medications given, observation needs and outstanding medical results.[4][15]
Complications and pitfalls
- Medical: ACS, cardiomyopathy, arrhythmia, stroke, hyperthermia, rhabdomyolysis, dental destruction, skin infections, blood-borne viruses.
- Psychiatric: MAP, crash depression and suicide, anxiety, cognitive complaints, trauma re-enactment.
- Pitfalls: missing ACS in a young adult; lifelong schizophrenia label after a single MAP episode; treating stimulant withdrawal as alcohol-like seizure risk while ignoring crash suicide; inventing an approved anti-craving standard; indefinite high-dose antipsychotics without review; punitive discharge without AOD follow-up; restraint without cooling in hyperthermia.
Prognosis and disposition
Most uncomplicated intoxication settles with time and supportive care once medical complications are controlled. MAP may remit with abstinence or persist — disposition must secure follow-up either way. Crash suicide risk peaks early. Disposition ladder: medical clearance → psychiatric emergency observation or inpatient unit if high risk → community shared care (mental health + AOD) with early review after MAP or suicidal crash.[1][2][3]
Special populations
Youth. High MAP and first-episode psychosis interface; family work; avoid diagnostic fatalism.[3]
Pregnancy. Medical stabilisation and obstetric liaison first; do not invent unproven mandatory anti-craving drugs as standard; counsel maternal-fetal risks of continued stimulant use.[1]
Chemsex networks. Sexual risk, consent capacity while intoxicated, GHB co-use, stigma-sensitive engagement, STI/HIV pathways.[1]
Known cardiomyopathy / IHD. Cardiology co-management; continued methamphetamine use worsens cardiac prognosis.[5]
Forensic / custody. Dynamic risk, MAP, medication and observation handover dominate.[4]
Indigenous and culturally diverse communities (ANZ). Partner with culturally safe services; address social determinants; avoid deficit-only framing.[1]
Evidence, guidelines and regional differences
| Source | High-yield takeaway |
|---|---|
| ASAM/AAAP 2024 StUD CPG | Psychosocial first-line; no FDA-approved standard anti-craving pharmacotherapy[1] |
| McGregor 2005 | Classic methamphetamine withdrawal time course still taught as reference[2] |
| McKetin psychosis and violence cohorts | Dose-related psychosis; dynamic violence association[3][4] |
| Kevil 2019 | Cardiovascular toxicity pathway for methamphetamine[5] |
| Srisurapanont 2021 NMA | Antipsychotics for MAP — efficacy signals; time-limit in practice[6] |
| Ronsley 2020; Dutra 2008; Pfund 2024 | Psychosocial more consistent than pharmacotherapy; CM strongest reinforcement signal[7][11][12] |
| ADAPT-2 / mirtazapine RCTs | Selected pharmacotherapy signals — not acute mandatory standards[8][9][10] |
| BAP substance dependence consensus | Contemporary UK pharmacological framing read alongside psychosocial primacy[16] |
| Stimulant-related emergencies reviews | Medical-first acute algorithms for ED and acute psychiatry interface[15] |
ANZ: Crystal methamphetamine ("ice") drives much of the acute psychiatry and ED load; MAP and behavioural disturbance are routine dual-diagnosis presentations; CM implementation is uneven despite evidence. UK: BAP consensus and NICE dual-diagnosis principles emphasise integrated care; stimulant patterns vary by region. US: ASAM/AAAP CPG is the major specialty society reference; CM has a longer research history with periodic policy friction around incentives. State the guideline you are quoting.[1][16]
Exam pearls
- Medical before mental-health label — hyperthermia, ACS, stroke, rhabdomyolysis first.[5][15]
- No licensed anti-craving/substitution standard for stimulants — "start OAT-like replacement" fails.[1]
- Withdrawal is usually not seizures-like alcohol — but crash suicide and CV events still kill.[2][5]
- MAP is dose-related; clear consciousness helps separate from delirium.[3]
- Violence risk is dynamic with heavy-use periods.[4]
- Time-limit antipsychotics for MAP; reassess after an abstinence window.[6]
- Name contingency management for post-acute use-disorder care.[12]
- If you quote ADAPT-2, state naltrexone XR 380 mg IM every 3 weeks + bupropion XL 450 mg daily accurately, with exclusions — and that it is not the acute ED standard.[8]
- If you quote mirtazapine trials, 30 mg nocte is the common studied dose — specialist adjunct after stabilisation.[9][10]
- Legal frameworks are jurisdiction-specific — principles yes, invented section numbers no.[1]
References
- [1]ASAM/AAAP Clinical Guideline Committee The ASAM/AAAP Clinical Practice Guideline on the Management of Stimulant Use Disorder J Addict Med, 2024.PMID 38669101
- [2]McGregor C, Srisurapanont M, Jittiwutikarn J, et al. The nature, time course and severity of methamphetamine withdrawal Addiction, 2005.PMID 16128721
- [3]McKetin R, Lubman DI, Baker AL, et al. Dose-related psychotic symptoms in chronic methamphetamine users: evidence from a prospective longitudinal study JAMA Psychiatry, 2013.PMID 23303471
- [4]McKetin R, Lubman DI, Najman JM, et al. Does methamphetamine use increase violent behaviour? Evidence from a prospective longitudinal study Addiction, 2014.PMID 24400972
- [5]Kevil CG, Goeders NE, Woolard MD, et al. Methamphetamine Use and Cardiovascular Disease Arterioscler Thromb Vasc Biol, 2019.PMID 31433698
- [6]Srisurapanont M, Likhitsathian S, Suttajit S, et al. Efficacy and dropout rates of antipsychotic medications for methamphetamine psychosis: A systematic review and network meta-analysis Drug Alcohol Depend, 2021.PMID 33385693
- [7]Ronsley C, Nolan S, Knight R, et al. Treatment of stimulant use disorder: A systematic review of reviews PLoS One, 2020.PMID 32555667
- [8]Trivedi MH, Walker R, Ling W, et al. Bupropion and Naltrexone in Methamphetamine Use Disorder N Engl J Med, 2021.PMID 33497547
- [9]Coffin PO, Santos GM, Hern J, et al. Effects of Mirtazapine for Methamphetamine Use Disorder Among Cisgender Men and Transgender Women Who Have Sex With Men: A Randomized Clinical Trial JAMA Psychiatry, 2020.PMID 31825466
- [10]Colfax GN, Santos GM, Das M, et al. Mirtazapine to reduce methamphetamine use: a randomized controlled trial Arch Gen Psychiatry, 2011.PMID 22065532
- [11]Dutra L, Stathopoulou G, Basden SL, et al. A meta-analytic review of psychosocial interventions for substance use disorders Am J Psychiatry, 2008.PMID 18198270
- [12]Pfund RA, Ginley MK, Boness CL, et al. Contingency Management for Drug Use Disorders: Meta-Analysis and Application of Tolin's Criteria Clin Psychol (New York), 2024.PMID 38863566
- [13]Rawson RA, Marinelli-Casey P, Anglin MD, et al. A multi-site comparison of psychosocial approaches for the treatment of methamphetamine dependence Addiction, 2004.PMID 15139869
- [14]McKetin R, Dean OM, Turner A, et al. N-acetylcysteine (NAC) for methamphetamine dependence: A randomised controlled trial EClinicalMedicine, 2021.PMID 34308314
- [15]Fries A, Christ M, Nickl H, et al. The Diagnosis and Treatment of Stimulant-Related Emergencies Dtsch Arztebl Int, 2025.PMID 40991352
- [16]Sinclair JMA, Kalk NJ, Kaar SJ, et al. Evidence-based consensus guidelines for the pharmacological management of substance dependence: Recommendations from the British Association for Psychopharmacology J Psychopharmacol, 2026.PMID 41731947