Psych · Addiction psychiatry — substance-induced mood and anxiety disorders
Substance-induced mood and anxiety disorders
Also known as Substance-induced depressive disorder · Substance/medication-induced depressive disorder · Substance-induced bipolar disorder · Substance-induced anxiety disorder · Alcohol-induced depression · Stimulant crash dysphoria · Cannabis-induced anxiety · Medication-induced mood disorder · Secondary depression substance use · Induced vs independent depression
Exam-exhaustive fellowship reference on substance/medication-induced mood and anxiety disorders — DSM-5-TR and ICD-11 timing rules, alcohol stimulant and cannabis pathways, discriminators from independent mood/anxiety disorders, suicide risk windows, watchful waiting versus early antidepressant, dual-diagnosis management with named doses, and board discriminators. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Substance-induced mood and anxiety disorders sit at the core of addiction and dual-diagnosis exams. Examiners do not want a lay list of “drugs that make you sad or jumpy.” They want a registrar who can rebuild the timeline, apply DSM-5-TR/ICD-11 timing rules, separate induced versus independent syndromes, name alcohol, stimulant and cannabis patterns, protect the stimulant-crash and withdrawal suicide windows, and deliver dose-levelled dual management without the twin errors of “just substances — discharge” and “lifelong antidepressant on night one of intoxication.”[1][4][8][17]
Overview and definition
DSM-5-TR skeleton (depressive). Substance/medication-induced depressive disorder requires: (1) a prominent and persistent disturbance in mood characterised by depressed mood and/or markedly diminished interest or pleasure; (2) evidence from history, examination or labs that the symptoms developed during or soon after substance intoxication or withdrawal, or after exposure to a medication capable of producing the symptoms; (3) the disturbance is not better explained by an independent depressive disorder (for example symptoms preceded onset of use, or persist for a substantial period after cessation of acute intoxication/withdrawal effects); (4) the disturbance does not occur exclusively during delirium; and (5) the disturbance causes clinically significant distress or impairment.[1][8][17]
Bipolar and anxiety analogues. The same timeline logic applies to substance/medication-induced bipolar and related disorder (elevated, expansive or irritable mood with or without depressed mood) and substance/medication-induced anxiety disorder (panic attacks, anxiety, obsessions/compulsions, or other anxiety features predominant in the clinical picture). Specifiers commonly taught: onset during intoxication versus withdrawal; name the substance or medication.[8][10][18]
ICD-11 places substance-induced mood and anxiety disorders among substance-induced mental disorders with the substance coded. Medication-induced presentations (glucocorticoids, interferons, isotretinoin and others) use the same timeline discipline on medical wards.[16][18]
What it is not. A positive urine drug screen is not a diagnosis. Transient intoxication dysphoria or panic that resolves as the drug clears is not automatically a full induced disorder of clinical severity. Independent major depression with concurrent alcohol use is not “proved induced” because the breath alcohol is positive today.[1][4]
Classification and the four-layer model
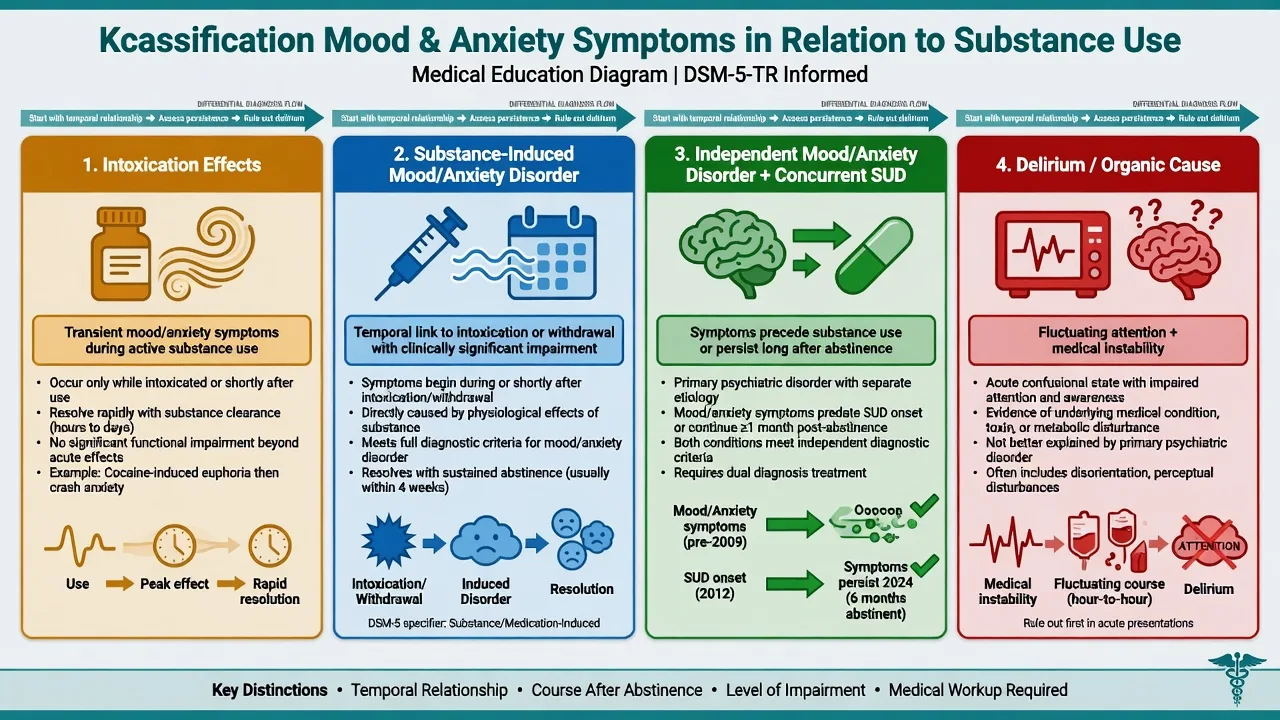
Intoxication effects
- During/shortly after use
- Often partial insight recovering as drug clears
- Supportive care may suffice if mild
- Still assess suicide and other substances
Substance/medication-induced mood or anxiety disorder
- Temporal link to intoxication/withdrawal/medication
- Impairment with full syndrome features
- Often remits with abstinence if purely induced
- Dual follow-up and risk plan mandatory
Independent mood/anxiety + SUD
- Symptoms precede heavy use or persist offline
- Family history and prior independent episodes common
- Full guideline mood/anxiety care plus SUD treatment
- Do not wait for mythical perfect abstinence
Delirium / medical
- Fluctuating attention and awareness
- Withdrawal, Wernicke, hypoxia, infection
- Treat underlying cause first
- Do not lock a pure induced label
Timing rules (exam discriminator)
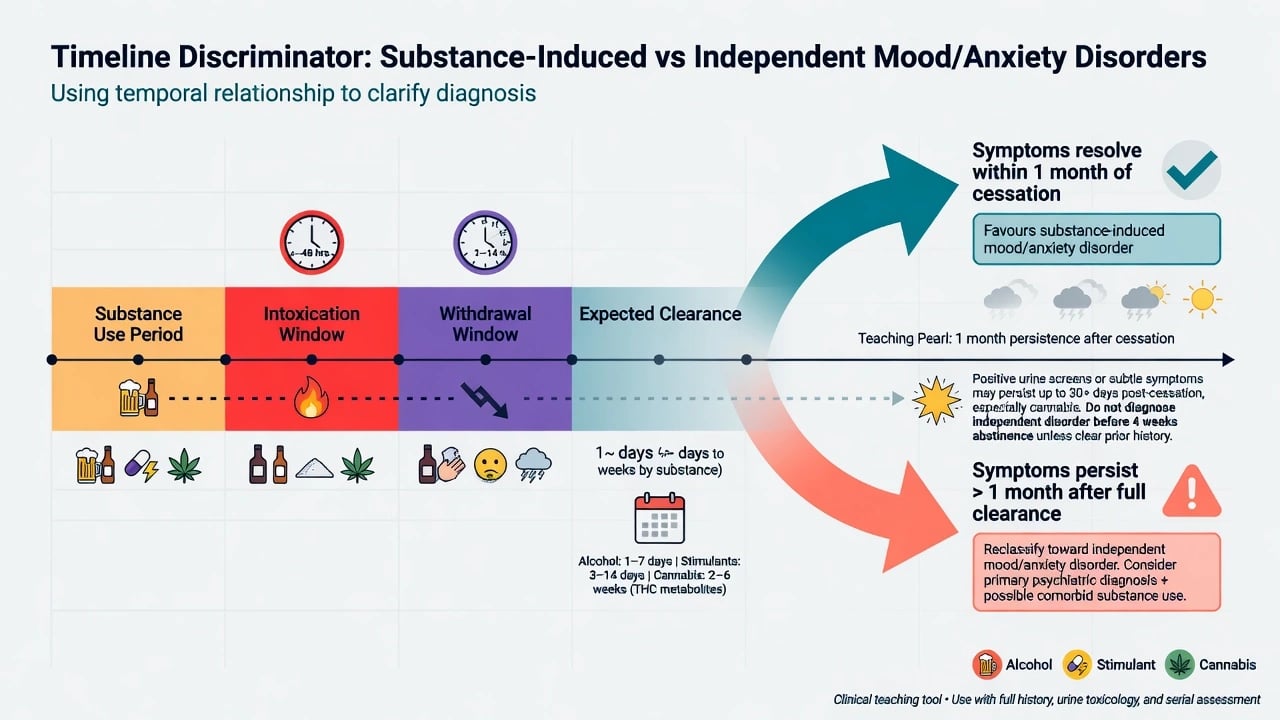
Nosology uses clinical judgment, not a universal stopwatch. Teaching pearl used across boards: if depressive or anxiety symptoms persist substantially beyond the expected physiological window of intoxication or withdrawal for that substance (commonly framed in teaching as roughly about 1 month of persistence after cessation for many substances, with shorter windows for some short-acting agents), reclassify toward an independent mood or anxiety disorder rather than pure substance-induced illness. Always pair the calendar with premorbid course, family history, and prior independent episodes — not the clock alone.[1][2][8][17]
Practical timing checklist
- Did mood/anxiety begin during heavy use, acute intoxication, withdrawal, or after starting a culprit medication?[1]
- Did symptoms precede the substance pattern (favours independent)?[1][3]
- After confirmed abstinence, are symptoms remitting (favours induced) or persisting (favours independent or dual pathway)? Brown and Schuckit showed marked reduction in depressive symptoms among abstinent alcoholics within the first weeks of abstinence — largest change often early.[2]
- Is there a prior independent major depression or anxiety disorder when not using?[1][3]
- Is a medication (for example high-dose glucocorticoid) the more plausible cause than the recreational substance alone?[18]
Epidemiology and risk
Headline dual-epidemiology numbers
NESARC-era work (Grant and colleagues) showed strong associations between substance use disorders and independent mood and anxiety disorders, while exclusive substance-induced mood/anxiety episodes were relatively uncommon at population level — clinical services nevertheless see high rates of affective and anxiety symptoms during active use, and the induced/independent distinction remains a treatment-planning tool rather than a reason to dismiss distress.[4][8]
Alcohol use disorders and major depression are tightly linked with evidence for causal pathways as well as shared liability; co-occurrence worsens prognosis for both axes.[8][9] Anxiety disorders and alcohol use disorders likewise co-occur frequently, with reciprocal initiation and maintenance models (self-medication, withdrawal-negative reinforcement, shared trauma/stress pathways).[10][11]
Pathophysiology (viva depth)
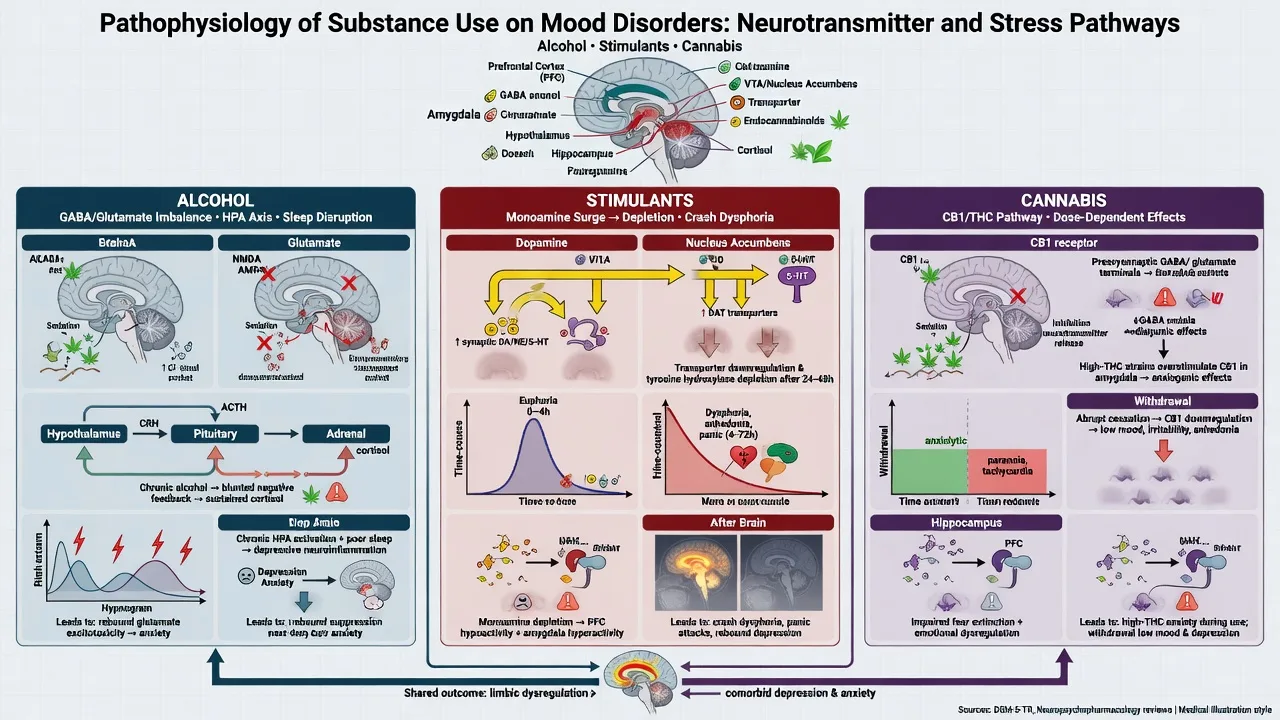
Alcohol. Chronic heavy use drives GABA/glutamate neuroadaptation, sleep architecture collapse, HPA dysregulation and nutritional/medical insults that generate depressive and anxiety phenotypes during use and withdrawal. Early abstinence removes the toxic driver — hence the classic improvement curve — but protracted anxiety and insomnia can persist and feed relapse.[2][8][11]
Stimulants (amphetamine-type, cocaine). Intoxication elevates monoamines with anxiety, panic, irritability and sometimes mania-like elevation; the crash reflects relative monoamine depletion with profound dysphoria, anhedonia and suicidality. Dose–symptom relationships are well documented in chronic methamphetamine cohorts for psychotic phenomena and support a general dose-sensitive neuropsychiatric model examiners expect you to name.[13]
Cannabis. High-THC products are often anxiogenic; systematic review evidence links cannabis use to psychotic and affective mental health outcomes. Cannabis withdrawal includes irritability, anxiety, sleep disturbance and depressed mood — timeline these against last use rather than diagnosing lifelong GAD on day two of a detox bed.[12]
Medications. Systemic corticosteroids produce a spectrum from insomnia and irritability through mania to depression and psychosis; risk rises with dose. Always check the drug chart on CL wards.[18]
Clinical presentation by substance
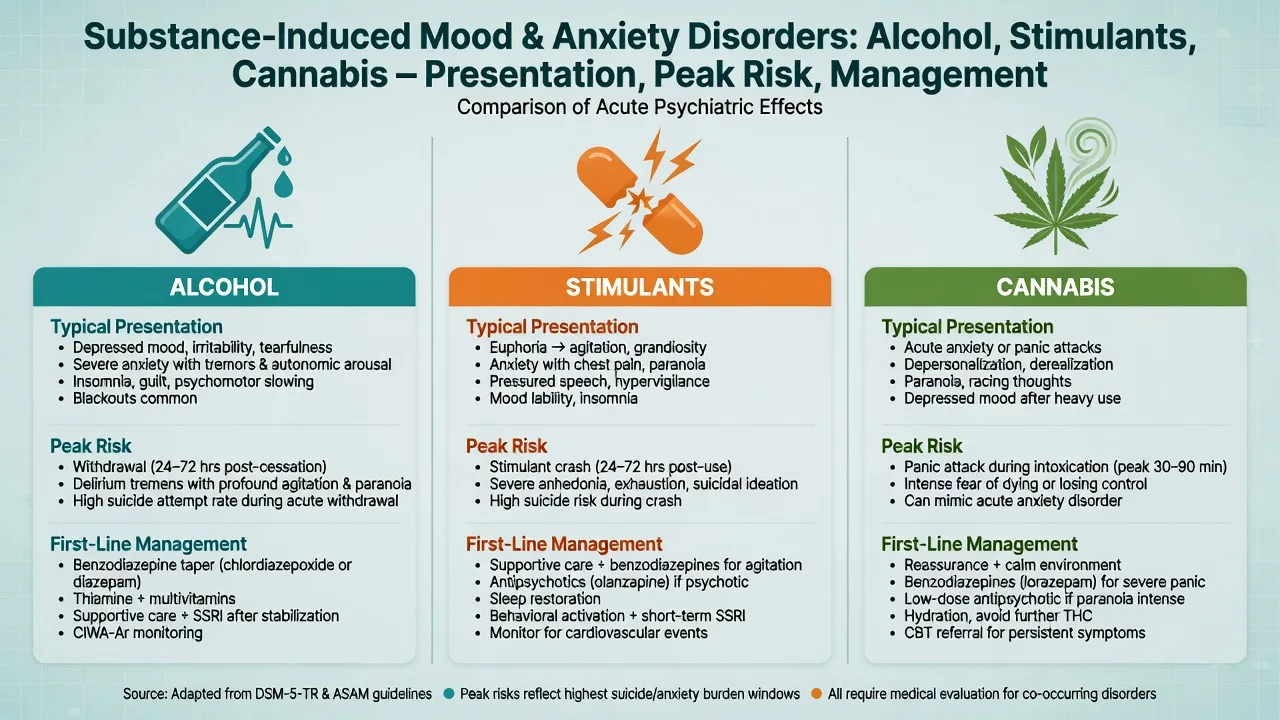
Alcohol
- Induced depression: anhedonia, guilt, insomnia, psychomotor change and suicidality during heavy use or early abstinence; many cases improve substantially with sustained abstinence and medical stabilisation.[1][2][8]
- Anxiety: marked during withdrawal (autonomic arousal, panic-like surges); may also appear as protracted post-detox anxiety. Separate medical withdrawal from primary panic disorder.[10][11][16]
- Independent MDD hidden in drinkers: prior episodes off alcohol, strong family history, persistence after weeks of abstinence — treat as full depressive illness plus AUD care.[1][3][17]
Stimulants
- Intoxication: anxiety, panic, irritability, insomnia, grandiosity or mixed elevation; medical toxicity may dominate (hypertension, hyperthermia, cardiac risk).[13]
- Crash: severe dysphoria, anhedonia, hypersomnia or inverted sleep, craving and high suicide risk — this is an examinable emergency window, not “just coming down.”[13][8]
- Recurrent binges kindle repeated crash depressions; dual formulation required every presentation.[13][14]
Cannabis
- Intoxication panic/anxiety especially with high-THC products in naive or vulnerable users; paranoia may blur into psychotic presentations (cross-link SIP topic).[12]
- Withdrawal: irritability, anxiety, depressed mood, sleep disturbance — usually time-limited with supportive care and cessation support.[12]
- Affective outcomes in systematic reviews support taking heavy use seriously as a modifier of mood course, not a moral aside.[12]
Medication-induced (CL high-yield)
High-dose glucocorticoids, interferons and selected other agents produce affective change; co-manage taper or switch with the treating team and bridge with psychotropics when severity demands.[18][17]
Differential diagnosis — discriminators, not lists
| Feature | Favours substance-induced | Favours independent mood/anxiety + use | Favours delirium / organic |
|---|---|---|---|
| Onset | Close temporal link to use/med | Premorbid episodes; use secondary | Hours–days with medical insult |
| After abstinence | Clears within expected window | Persists weeks+ | Tracks medical course |
| Family history of mood disorder | Less often decisive | More often | Variable |
| Withdrawal signs | May dominate anxiety picture | Anxiety independent of autonomic withdrawal | Fluctuating attention |
| Prior independent episodes | Absent | Present | Variable |
| Exam red flags | Intoxication/withdrawal signs | Classic MDD/GAD course offline | Fever, focal neurology, Wernicke signs |
| Schuckit’s induced versus independent framework remains the cleanest exam scaffold for alcohol; extend the same logic to stimulants, cannabis and medications.[1][2][3] |
Also exclude: bipolar disorder unmasked by stimulants or steroids; primary panic/GAD/social anxiety with self-medication; PTSD with substance use; personality disorder affective instability without major episode thresholds; substance-induced psychosis with secondary mood colouring.[10][13][17][18]
Assessment
Structure the interview as a reconstruction: timeline (first use, pattern, last use clock time, route, estimated dose/potency, onset of mood/anxiety relative to use, prior induced and independent episodes); premorbid function; collateral (family, friends, ambulance, records); MSE with documented affective and anxiety examples, cognition and insight; suicide and violence risk including means, post-stimulant crash intent, and alcohol-related impulsivity; withdrawal scoring (for example CIWA-Ar principles for alcohol) when indicated; diagnose the SUD axis independently; apply local Mental Health Act principles for involuntary treatment when risk and capacity criteria are met — do not invent section numbers for the wrong jurisdiction.[1][8][16]
Investigations
- Vital signs, capillary glucose, focused neurological exam; UDS/serum toxicology are supportive, not dispositive.[16]
- FBC, U&E, LFT, TFT, B12/folate as indicated; pregnancy test when applicable; thiamine risk assessment in alcohol use.[16]
- ECG before selected antidepressants and when polypharmacy/QT risk is relevant; baseline metabolic panel before longer-term psychotropics.[17]
- Escalate neuroimaging and organic work-up for late-onset first depression, seizures, focal signs, rapid cognitive decline or delirium features.[17]
- Full medication review for iatrogenic culprits (steroids and others).[18]
Acute / emergency management
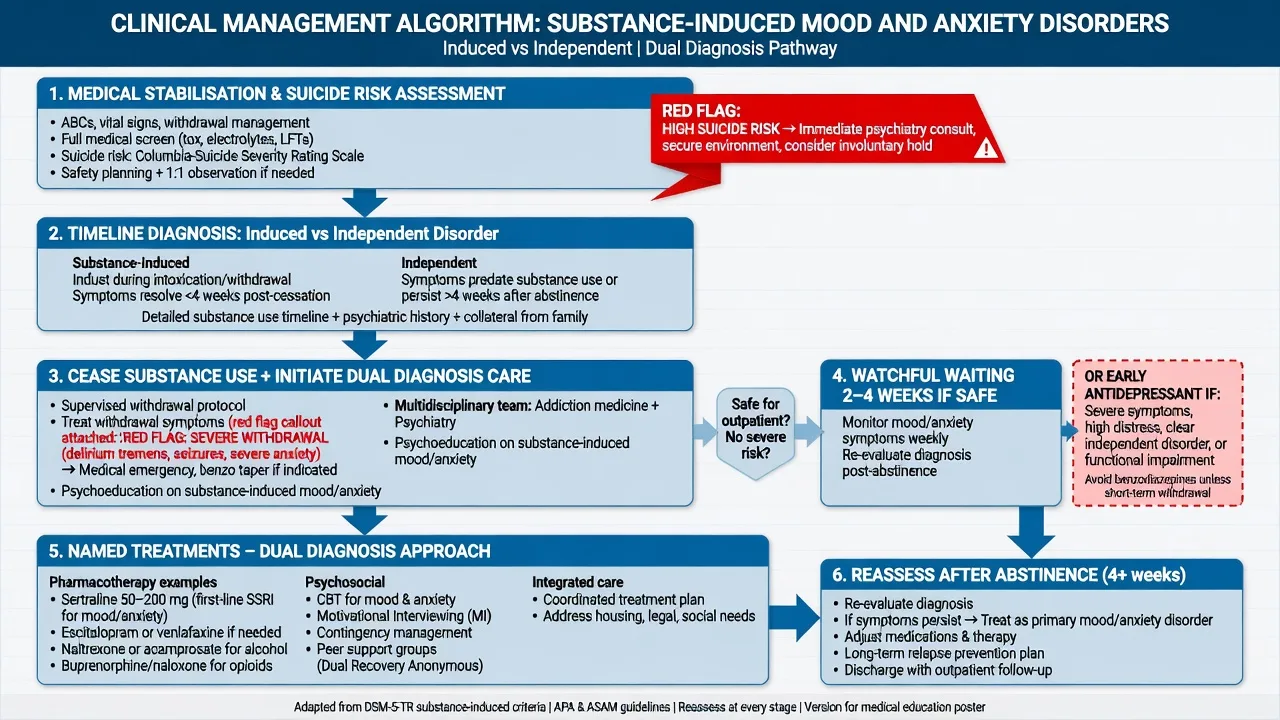
Acute sequence: medical first for alcohol/benzodiazepine withdrawal risk, stimulant toxicity, head injury, hypoxia or hypoglycaemia; Wernicke prevention with parenteral thiamine when alcohol risk is present per local protocol; low-stimulus environment; suicide risk management with observation level and means restriction; short supervised benzodiazepines only within withdrawal protocols — avoid converting dual anxiety into iatrogenic benzo dependence; do not dump high-dose antidepressant polypharmacy on night one of heavy intoxication as a substitute for timeline thinking.[8][11][16]
Definitive management
Core disease-modifying step: the substance axis
- Cease or substantially reduce the culprit substance using motivational interviewing, brief intervention, CBT-based packages, contingency management for stimulants, and structured AUD care including pharmacotherapy when indicated.[14][16]
- Alcohol pharmacotherapy examples examiners expect you to name (individualise, check interactions and local formulary): naltrexone 50 mg oral daily (opioid-free patients; monitor LFTs and counsel on blockade of opioid analgesia); acamprosate 666 mg oral three times daily (renally adjust; supports abstinence); disulfiram only with informed consent and reliable abstinence plan. These treat the AUD axis that drives many induced mood/anxiety syndromes.[16][8]
Watchful waiting versus early antidepressant
Watchful waiting (~2–4 weeks of abstinence) is reasonable for many pure substance-induced depressive pictures when suicide risk is contained, medical detox is safe, supports are present, and history suggests symptoms track heavy use — because classic abstinence data show substantial early remission of depressive symptoms.[2][8]
Start antidepressant earlier when: independent MDD is likely (prior offline episodes, family history, persistence already beyond expected window); depression is severe with melancholic features or psychosis; suicide risk cannot be safely contained with psychosocial measures alone; or functioning collapses. Meta-analytic evidence shows antidepressants can help selected depressed patients with alcohol or other drug dependence, with modest overall effects and greater clarity when depression is carefully diagnosed — not every intoxicated sad patient needs an SSRI on day one, and not every dual patient should be denied one.[5][6][17]
Named SSRI example: sertraline 50 mg oral daily, titrate toward 50–150 mg daily as tolerated after baseline review; counsel on onset lag (often 2–4 weeks for full effect), GI upset, activation/akathisia, sexual side-effects, hyponatraemia risk in older adults, and rare serotonin toxicity with interacting drugs; review at 1–2 weeks for suicide risk and tolerability, then monthly early on. Combine with AUD care rather than monotherapy fantasies.[5][7][17]
Combination dual pharmacotherapy. Pettinati and colleagues showed that in depressed alcohol-dependent patients, sertraline plus naltrexone produced higher abstinence rates than either strategy alone in a key RCT — examiners love this as a concrete “treat both axes” example (still individualise; not every patient is a trial clone).[7]
Anxiety-focused care
- Prefer CBT, exposure principles for panic/phobia, and MI for the substance that maintains anxiety.[10][11]
- Treat alcohol withdrawal medically; do not prescribe open-ended benzodiazepines for dual alcohol–anxiety outpatients.[11][16]
- SSRIs may help independent anxiety disorders once induced components and withdrawal are clarified; timeline first.[10][17]
Dual diagnosis interface
Sequential care (“treat addiction first only” or “treat depression only after perfect abstinence”) fails patients and fails exams. Integrated models emphasise concurrent treatment of mental illness and substance misuse, stage-matched motivational work, and no-wrong-door systems. Cochrane synthesis of psychosocial interventions for SMI plus substance misuse shows complex/modest average effects — clinically you still deliver concurrent, coordinated care rather than eligibility ping-pong.[14][15]
Psychosocial and recovery
Sleep, nutrition, housing, employment and family psychoeducation are not optional soft extras. Written early-warning plans should cover mood relapse, anxiety surge, and substance binge as linked risks.[14][17]
Subtypes and high-yield scenarios
- Alcohol-induced depressive disorder — timeline, abstinence curve, suicide plan, AUD pharmacotherapy, delayed vs early SSRI.[1][2][7]
- Alcohol withdrawal and protracted anxiety — medical detox, no chronic benzos, CBT/MI, reassess for independent anxiety.[10][11][16]
- Stimulant crash dysphoria — suicide window, medical clearance, short observation, dual follow-up, stimulant SUD psychosocial package.[13][14]
- Cannabis-induced anxiety/panic and withdrawal mood symptoms — potency counselling, cessation support, avoid over-diagnosing lifelong GAD on day two.[12]
- Steroid/medication-induced affective syndrome — drug chart, co-managed taper, psychotropic bridge.[18]
- Independent MDD unmasked after detox — reclassify; full RANZCP-aligned mood care plus ongoing SUD treatment.[3][17]
Complications and pitfalls
Classic examinable errors: discharging severe dual depression as “just alcohol”; automatic lifelong antidepressant without timeline; missing independent bipolar after stimulant-induced elevation; chronic benzodiazepines for dual anxiety; missing Wernicke and medical withdrawal; ignoring stimulant-crash suicide risk; sequential service exclusion; and failing to reassess diagnosis after sustained abstinence.[1][2][8][11][14][16]
Prognosis and disposition
Better: clear temporal link, rapid abstinence, good premorbid function, no family history of mood disorder, short episode, contained suicide risk.[1][2]
Worse: independent MDD/bipolar, ongoing use, trauma, prior attempts, poor supports, stimulant crash with intent, untreated AUD with repeated detox only.[3][8][9]
Disposition ladder: medical resus/detox → psychiatric inpatient when risk/incapacity → community dual-diagnosis step-down with written crisis plan. Reassess diagnosis at roughly 2–4 weeks and again after sustained abstinence.[2][8][14]
Special populations
Adolescents need family engagement, high-THC counselling and careful separation of developmental anxiety from induced panic; perinatal needs capacity, safeguarding and specialist liaison for both substances and antidepressants; older adults need intensified organic work-up, medication review and alcohol under-recognition vigilance; cultural/Indigenous contexts need non-stigmatising dual formulation without moralising use while holding risk; forensic interface uses intoxication and risk principles without invented statutes.[8][12][17]
Evidence and guidelines (named)
- Schuckit 1997; Brown & Schuckit 1988; Schuckit 2013 — induced versus independent depression and abstinence trajectories.[1][2][3]
- Grant NESARC 2004 — independent mood/anxiety and SUD co-occurrence at population level.[4]
- Nunes & Levin 2004; Torrens 2005 — antidepressant efficacy in depressed SUD populations (modest, diagnosis-sensitive).[5][6]
- Pettinati 2010 — sertraline + naltrexone dual-axis RCT signal.[7]
- McHugh & Weiss 2019; Boden 2011 — AUD–depression clinical and causal framing.[8][9]
- Kushner 2000; Anker & Kushner 2019 — anxiety–alcohol comorbidity models.[10][11]
- Moore 2007; McKetin 2013 — cannabis affective risk and stimulant dose-linked neuropsychiatry.[12][13]
- Drake integrated dual care; Hunt Cochrane 2019 — concurrent dual treatment principles.[14][15]
- BAP Lingford-Hughes 2012; RANZCP Malhi mood 2020/21; Brown & Chandler steroids — pharmacology, mood guidelines, medication-induced affective change.[16][17][18]
Regional deltas. RANZCP mood guidance frames comprehensive assessment including substance context. NICE dual-diagnosis principles stress concurrent care and avoiding exclusion. BAP guidance is high-yield for pharmacological SUD management in UK-facing exams. APA dual-disorder framing similarly rejects sequential “treat one only” systems. Local Mental Health Act and detox protocols vary — state principles and cite local protocol in practice.[14][16][17]
Exam pearls
- Timeline + collateral + abstinence window beat a single UDS or a single depression score.[1]
- Teaching pearl: persistence substantially beyond expected substance window (often framed ~1 month) → reclassify toward independent disorder.[1][2][17]
- Many alcohol-induced depressive symptoms remit with abstinence — do not automatic lifelong AD on day one, and never ignore suicide risk.[2][8]
- Stimulant crash = high suicide window.[13]
- Name agent, dose, route, monitoring for any antidepressant or AUD medicine started.[7][16]
- Integrated dual care; treat both axes (Pettinati-style thinking).[7][14]
- Check the drug chart for steroids and other culprits.[18]
- Do not invent Mental Health Act section numbers across jurisdictions.[16]
Region notes
ANZ (primary). Use RANZCP mood disorder guidance for depressive/bipolar assessment and substance-context formulation; local dual-diagnosis and detox pathways; jurisdiction-specific Mental Health Act for involuntary treatment. Methamphetamine crash and alcohol dual depression are high-yield Australian ED psychiatry presentations.[13][17]
UK. MRCPsych expects induced versus independent discriminators, BAP-aligned SUD pharmacology, NICE concurrent dual-care language, and CASC communication without moralising.[14][16]
US / ABPN. DSM-5-TR criteria language; NESARC-informed comorbidity framing; integrated dual disorder treatment concepts; medication-induced mood (steroids).[4][14][18]
India / MD-DNB / NEET-SS. Classic viva on alcohol-induced depression, stimulant crash, cannabis anxiety, steroid mania/depression, and named SSRI plus naltrexone answers.[1][7][18]
References
- [1]Schuckit MA, Tipp JE, Bergman M, et al. Comparison of induced and independent major depressive disorders in 2,945 alcoholics Am J Psychiatry, 1997.PMID 9210745
- [2]Brown SA, Schuckit MA Changes in depression among abstinent alcoholics J Stud Alcohol, 1988.PMID 3216643
- [3]Schuckit MA, Smith TL, Kalmijn J Relationships among independent major depressions, alcohol use, and other substance use and related problems over 30 years in 397 families J Stud Alcohol Drugs, 2013.PMID 23384375
- [4]Grant BF, Stinson FS, Dawson DA, et al. Prevalence and co-occurrence of substance use disorders and independent mood and anxiety disorders: results from the National Epidemiologic Survey on Alcohol and Related Conditions Arch Gen Psychiatry, 2004.PMID 15289279
- [5]Nunes EV, Levin FR Treatment of depression in patients with alcohol or other drug dependence: a meta-analysis JAMA, 2004.PMID 15100209
- [6]Torrens M, Fonseca F, Mateu G, et al. Efficacy of antidepressants in substance use disorders with and without comorbid depression. A systematic review and meta-analysis Drug Alcohol Depend, 2005.PMID 15769553
- [7]Pettinati HM, Oslin DW, Kampman KM, et al. A double-blind, placebo-controlled trial combining sertraline and naltrexone for treating co-occurring depression and alcohol dependence Am J Psychiatry, 2010.PMID 20231324
- [8]McHugh RK, Weiss RD Alcohol Use Disorder and Depressive Disorders Alcohol Res, 2019.PMID 31649834
- [9]Boden JM, Fergusson DM Alcohol and depression Addiction, 2011.PMID 21382111
- [10]Kushner MG, Abrams K, Borchardt C The relationship between anxiety disorders and alcohol use disorders: a review of major perspectives and findings Clin Psychol Rev, 2000.PMID 10721495
- [11]Anker JJ, Kushner MG Co-Occurring Alcohol Use Disorder and Anxiety: Bridging Psychiatric, Psychological, and Neurobiological Perspectives Alcohol Res, 2019.PMID 31886106
- [12]Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review Lancet, 2007.PMID 17662880
- [13]McKetin R, Lubman DI, Baker AL, et al. Dose-related psychotic symptoms in chronic methamphetamine users: evidence from a prospective longitudinal study JAMA Psychiatry, 2013.PMID 23303471
- [14]Drake RE, Mercer-McFadden C, Mueser KT, et al. Review of integrated mental health and substance abuse treatment for patients with dual disorders Schizophr Bull, 1998.PMID 9853791
- [15]Hunt GE, Siegfried N, Morley K, et al. Psychosocial interventions for people with both severe mental illness and substance misuse Cochrane Database Syst Rev, 2019.PMID 31829430
- [16]Lingford-Hughes AR, Welch S, Peters L, et al. BAP updated guidelines: evidence-based guidelines for the pharmacological management of substance abuse, harmful use, addiction and comorbidity J Psychopharmacol, 2012.PMID 22628390
- [17]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [18]Brown ES, Chandler PA Mood and cognitive changes during systemic corticosteroid therapy Prim Care Companion J Clin Psychiatry, 2001.PMID 15014624