Psych · Child and adolescent psychiatry — neurodevelopmental
ADHD across the lifespan
Also known as Attention-deficit/hyperactivity disorder · Attention deficit hyperactivity disorder · ADHD · Adult ADHD · Hyperkinetic disorder · ADD · Attention deficit disorder
Exam-exhaustive fellowship reference on ADHD from childhood through adulthood — DSM-5-TR and ICD-11 criteria; multi-informant assessment; differentials; MTA and Cortese NMA evidence; stimulant and non-stimulant doses with monitoring; CBT/coaching; substance misuse and driving risk. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Attention-deficit/hyperactivity disorder (ADHD) is a high-yield child-and-adolescent and general adult topic across FRANZCP, MRCPsych, ABPN and MD/DNB. Examiners test DSM thresholds and age-of-onset changes, multi-informant assessment, differentials that look like "inattention," MTA and network meta-analysis logic, named agents with doses and monitoring, substance and driving risk, and adult first diagnosis without neat school reports. This topic is written so a candidate who has read nothing else can answer those questions at consultant depth.[1][3][4][17]
Overview and definition
ADHD is a neurodevelopmental syndrome of persistent inattention and/or hyperactivity-impulsivity that is inconsistent with developmental level, present in two or more settings, causes clinically significant impairment, and is not better explained by another mental disorder, substance, or medical condition. It is not a moral failure, exclusive childhood label, or rating-scale score alone. The modern exam stance is operational criteria plus developmental formulation: criteria gate the diagnosis; formulation explains heritability, environment, comorbidity, and the functional plan across home, school/work and community.[17][18]
DSM-5-TR structure you must reproduce. Criterion A requires a persistent pattern of inattention and/or hyperactivity-impulsivity that interferes with functioning or development, with a threshold of six or more inattention symptoms and/or six or more hyperactivity-impulsivity symptoms for at least 6 months (for older adolescents and adults, five or more symptoms in a domain is the threshold). Symptoms must have been present before age 12, occur in two or more settings, cause clear interference, and not occur exclusively during schizophrenia or another psychotic disorder, and are not better explained by another mental disorder. Specifiers capture presentation (combined; predominantly inattentive; predominantly hyperactive-impulsive), severity, and partial remission when full criteria are no longer met but impairment continues.[17][19]
ICD-11. ADHD is retained as a neurodevelopmental disorder with inattentive, hyperactive-impulsive or combined presentations. ICD-11 is more explicit that the diagnosis can be made in adulthood when a careful developmental history supports childhood onset even if contemporaneous records are incomplete — still requiring clinical judgment, not self-label alone. State which manual you are using when age-of-onset language is examined.[18][19]
Historical trap. DSM-IV required onset before age 7. DSM-5/DSM-5-TR moved the threshold to before 12. Candidates who still quote "before 7" lose easy marks.[17]
Classification and presentations
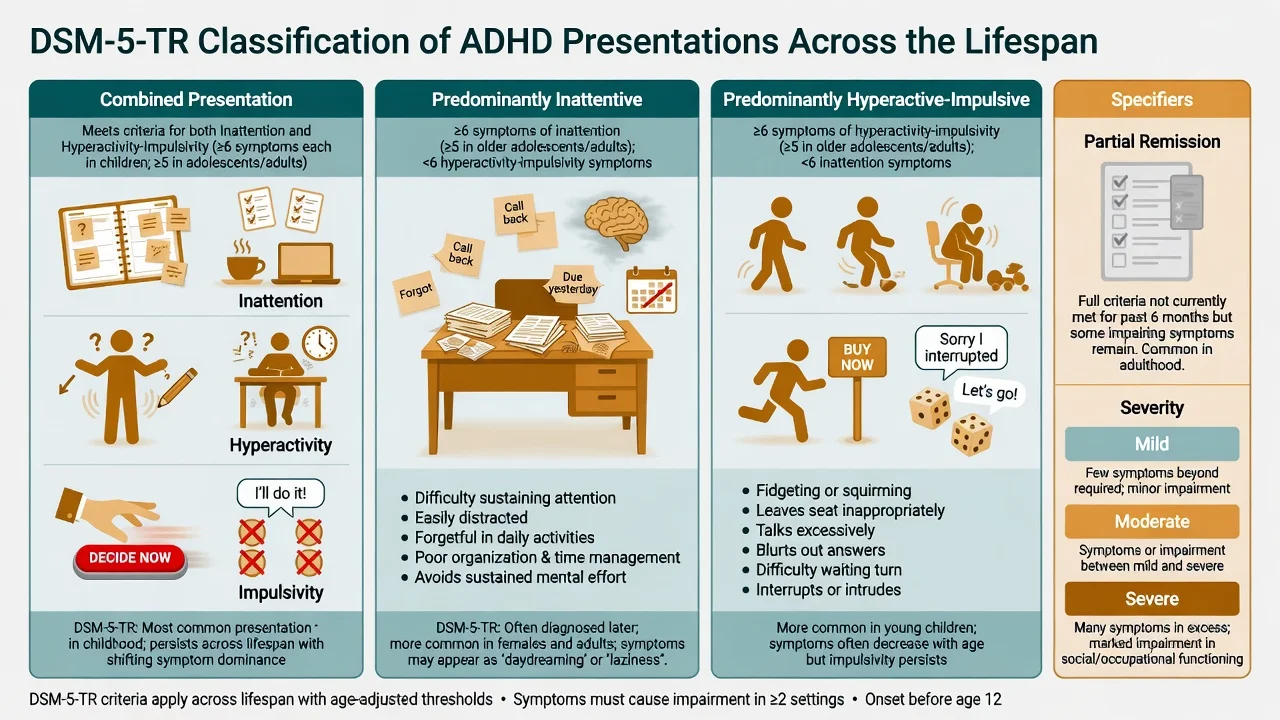
Combined
- Meets inattention and hyperactivity-impulsivity thresholds
- Commonest childhood clinical presentation
- Often the MTA-style phenotype
- Hyperactivity may internalise with age
Predominantly inattentive
- Inattention threshold met; hyperactivity below threshold
- More often missed in girls
- Daydreaming, unfinished work, time-blindness
- Common adult residual phenotype
Predominantly hyperactive-impulsive
- Hyperactivity-impulsivity threshold met
- More common in younger children
- Often evolves toward combined or residual inattentive features
- Impulsivity drives injury and social friction
Course labels
- Partial remission: full criteria no longer met, impairment remains
- Mild / moderate / severe by symptom load and impairment
- Not the same as cured
- Reassess at school and workplace transitions
Presentation type is a current cross-section, not a lifetime identity. Many adults with childhood combined ADHD present later with predominantly inattentive and organisational impairment plus inner restlessness rather than leaving their seat in meetings.[4][18]
Epidemiology and risk factors
Headline numbers every candidate must own
Polanczyk and colleagues estimated a worldwide ADHD prevalence near 5% in children and adolescents after accounting for methodological heterogeneity — exam answers should quote the range, not a false precision to one decimal place from a single clinic.[5] Adult community prevalence is lower but clinically substantial: Kessler and colleagues found meaningful rates of adult ADHD in the National Comorbidity Survey Replication with high comorbidity and role impairment; Simon and colleagues' meta-analysis supports adult prevalence in a similar ballpark depending on criteria and informants.[4][6]
Risk factors. Strong family history; prematurity and low birth weight; prenatal tobacco exposure; early psychosocial adversity. ADHD is highly heritable; molecular genetics is polygenic with small effect sizes at individual loci rather than a single gene test.[7] Functional risks include academic underachievement, occupational instability, relationship strain, elevated accident risk, and higher contact with justice systems — absolute risks are moderated by comorbidity, treatment, and environment.[13][15]
Pathophysiology
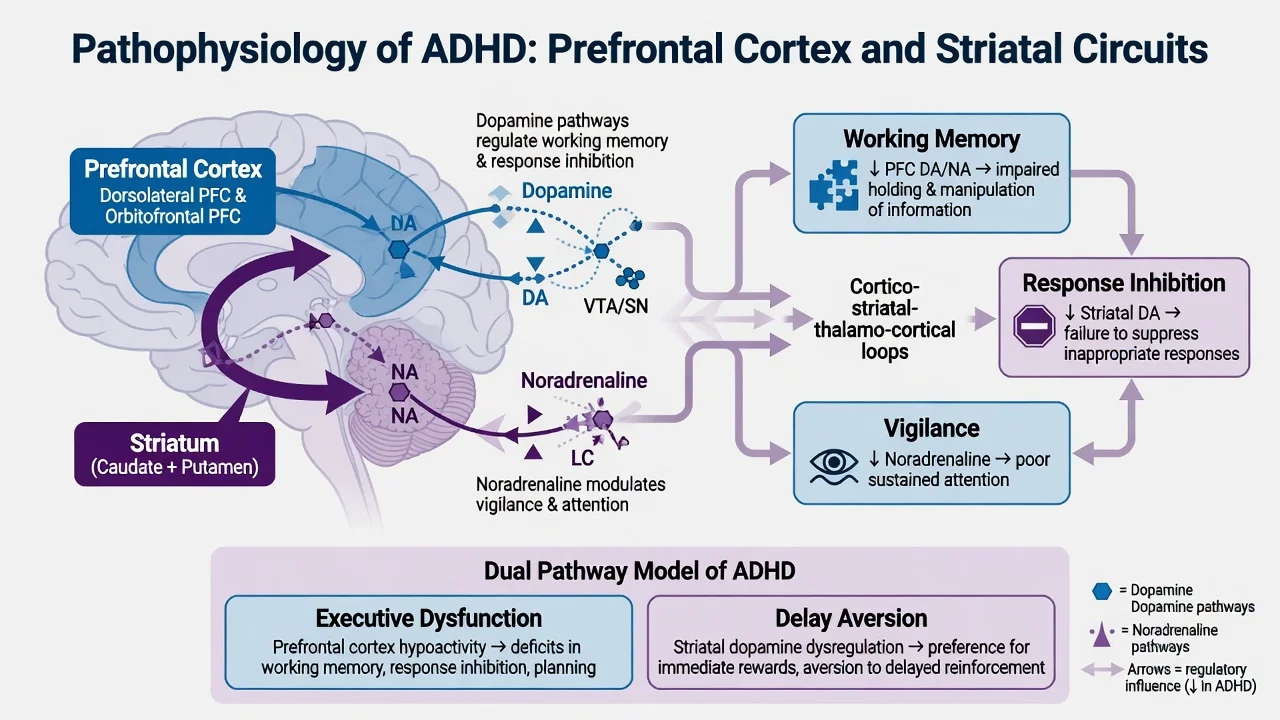
Catecholamine model (working clinical model). Prefrontal and striatal circuits that support sustained attention, working memory and response inhibition depend on balanced dopamine and noradrenaline signalling. Stimulants increase synaptic catecholamines; atomoxetine is a selective noradrenaline reuptake inhibitor. This is a pharmacological and circuit model, not proof of a single primary "chemical imbalance."[3][9]
Executive function theory. Meta-analysis supports medium group differences in response inhibition, vigilance and working memory — but no single executive deficit is pathognomonic, and many people with ADHD perform in the normal range on laboratory tasks while still failing real-world organisation.[8]
Dual-pathway framing. Combine executive dysfunction with delay aversion (preference for immediate over delayed rewards) to explain why behavioural interventions, environmental scaffolding and medication each help different slices of impairment.[8]
Genetics. Twin and family data show high heritability; candidate genes historically discussed include dopaminergic pathway variants with small odds ratios. Do not invent a clinical genetic panel for routine diagnosis.[7]
Clinical presentation across the lifespan
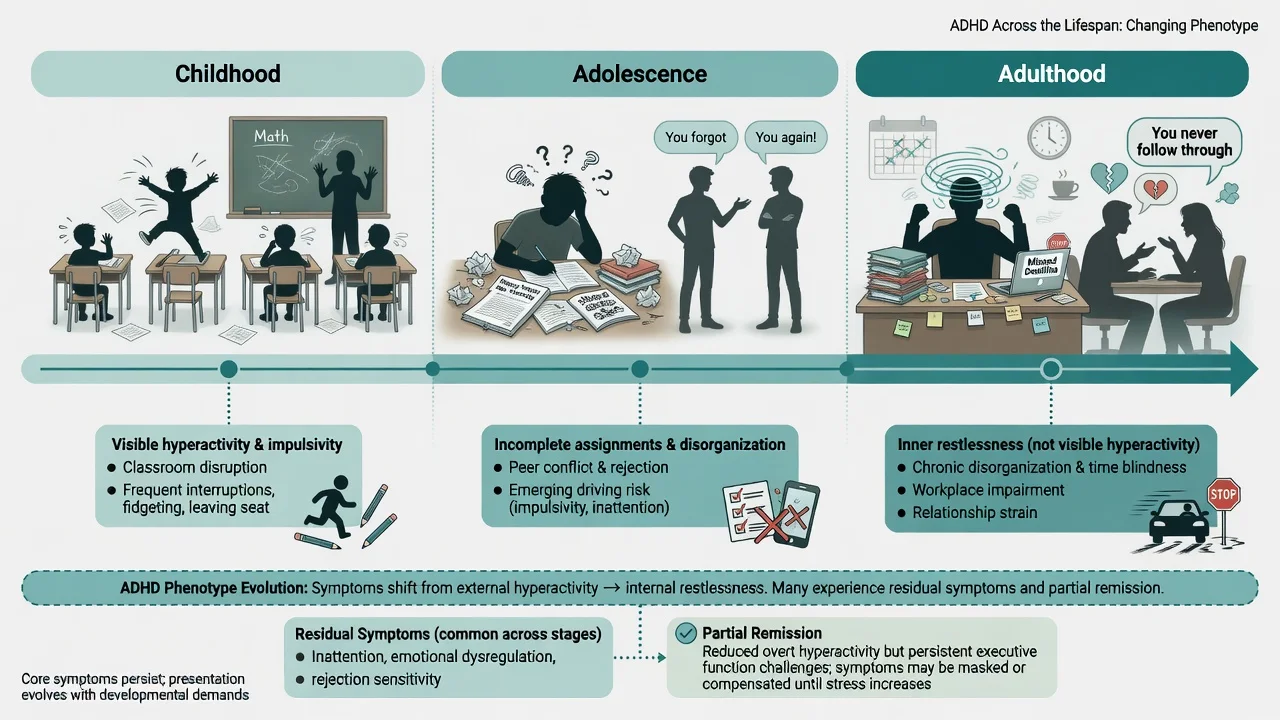
Childhood. Off-task classroom behaviour, incomplete work, losing materials, impulsive interruptions, difficulty waiting turns, risk-taking play, sleep resistance, and parent–teacher conflict. Teachers often supply the second setting that home-only history misses.[17]
Adolescence. Incomplete assignments, conflict with peers and authority, emerging driving risk, substance experimentation, and declining adherence. Hyperactivity may lessen while academic and social demands rise — impairment can worsen even if the child "seems calmer."[16][17]
Adulthood. Chronic disorganisation, time-blindness, job hopping or underemployment, relationship conflict, emotional dysregulation (common though not required for diagnosis), and inner restlessness. Adults may present for depression, anxiety, or burnout until a developmental history is taken.[4][18][19]
Female presentation. More inattentive and internalising features; later referral; higher risk of missed diagnosis until tertiary education or parenting demands expose executive limits.[4][19]
MSE language. Restlessness, distractibility mid-interview, topic-switching that is not formal thought disorder, and difficulty sustaining attention to lengthy history-taking. Quote functional examples rather than only checklist jargon.[18]
Differential diagnosis

Anxiety
- Worry-driven distraction and restlessness
- Symptoms worsen with uncertainty
- May improve when anxiety treated
- Can co-occur — treat both
Depression
- Episodic low mood and anhedonia
- Concentration fails with low energy
- Lifelong multi-setting pattern argues against pure MDD
- Demoralisation from untreated ADHD is common
Bipolar spectrum
- Episodic elevated energy and reduced sleep need
- Grandiosity, risky spending, decreased need for sleep
- Not chronic baseline from childhood
- Stimulants can destabilise unrecognised bipolar
ASD / LD / medical
- ASD: core social communication and restricted interests
- Learning disorder: skill-specific underachievement
- OSA, hearing loss, thyroid, substances, medications
- Trauma hyperarousal can mimic restlessness
Also keep ODD/CD (often comorbid), borderline personality (affective instability and identity vs executive dysregulation — may co-occur), and intellectual disability (adapted assessment) on the board.[17][18]
Clinical and bedside assessment
Structure the interview as developmental history + multi-informant + multi-setting + functional impairment + comorbidity + risk.[17][18][19]
- Symptom map using DSM domains with age-appropriate examples.
- Onset and course — evidence before age 12; school reports, report cards, parent recall, partner collateral for adults.
- Settings — home, school/work, peers, driving, finances.
- Comorbidity screen — anxiety, mood, ASD traits, tics, learning, sleep, substances, trauma.
- Risk — self-harm, aggression, child protection if parenting impaired, driving, diversion.
- Prior treatments — what was tried, dose, duration, adherence, side-effects, diversion.[17][18][19]
Tools support diagnosis; they do not make it. Common instruments: ADHD Rating Scale, Conners, SNAP-IV, Vanderbilt (primary care/school contexts), ASRS for adult screening, structured adult interviews such as DIVA-5 in specialist settings. Use scales for baseline and response tracking.[17][19]
Consent and young people. Shared decision-making with the child/adolescent developmentally appropriate; involve caregivers; mature-minor principles are jurisdiction-specific — state principles, do not invent statute numbers.[17]
Investigations
There is no diagnostic blood test or brain scan for ADHD.[17][19]
Before medication (exam checklist). Height, weight, BMI/centiles in youth; blood pressure and pulse; personal cardiac history (syncope, chest pain on exertion, congenital heart disease) and family history of sudden cardiac death or serious arrhythmia; review of current medications and substances. ECG when history or examination raises cardiac concern — large cohorts have not shown a clear excess of serious cardiovascular events with ADHD drugs at population level, but individual risk assessment still matters.[14][17]
Consider TSH, ferritin/FBC, and sleep evaluation when clinically indicated; urine drug screen when SUD is plausible; formal psychoeducational testing when learning disorder or intellectual disability is suspected. Neuroimaging or EEG only for neurological red flags (seizures, focal signs, regression) — not routine.[17][19]
Management — acute and safety priorities
ADHD is rarely an isolated medical emergency. Acute priorities are usually comorbid crises: suicidal ideation with depression, severe aggression, stimulant intoxication or diversion crisis, and high-risk driving while impaired.[12][16]
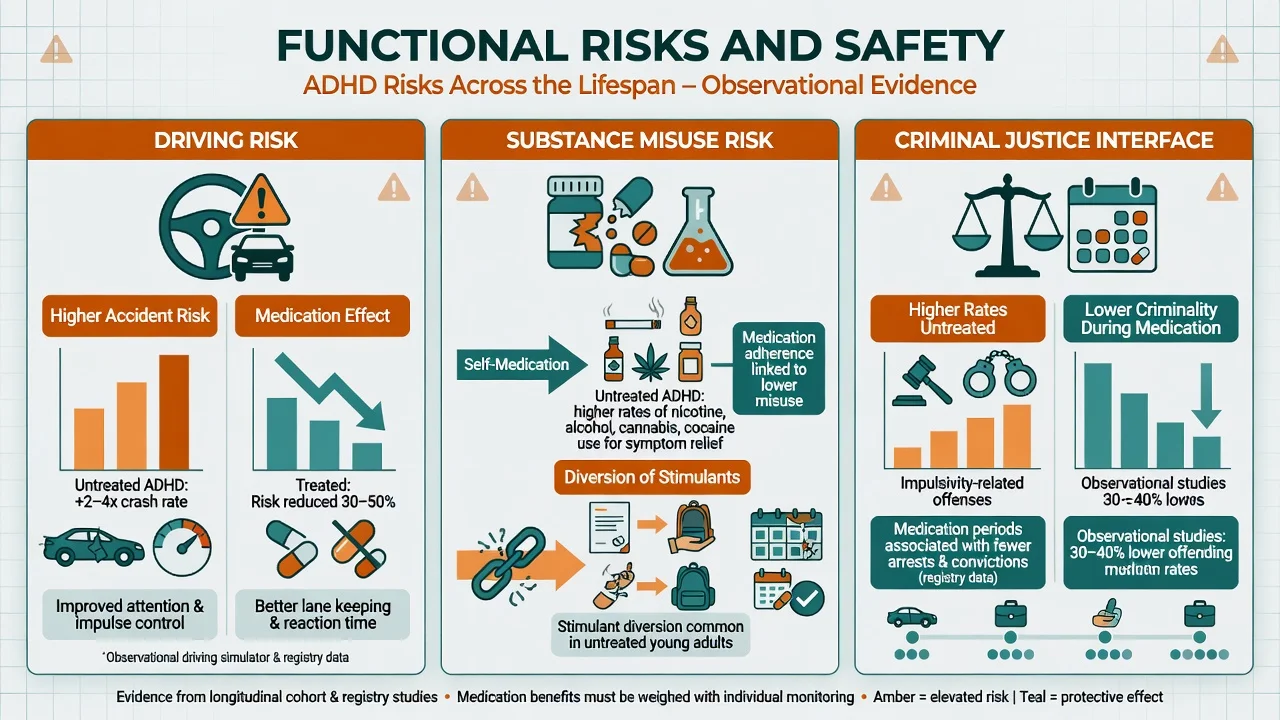
Driving. Untreated ADHD associates with higher relative risk of traffic accidents in meta-analytic and review literature; counsel on distraction, impulsivity, sleep, substances and medication timing; document advice; licensing notification duties are jurisdiction-specific.[15][16]
Management — definitive and stepwise
Stepped care principles
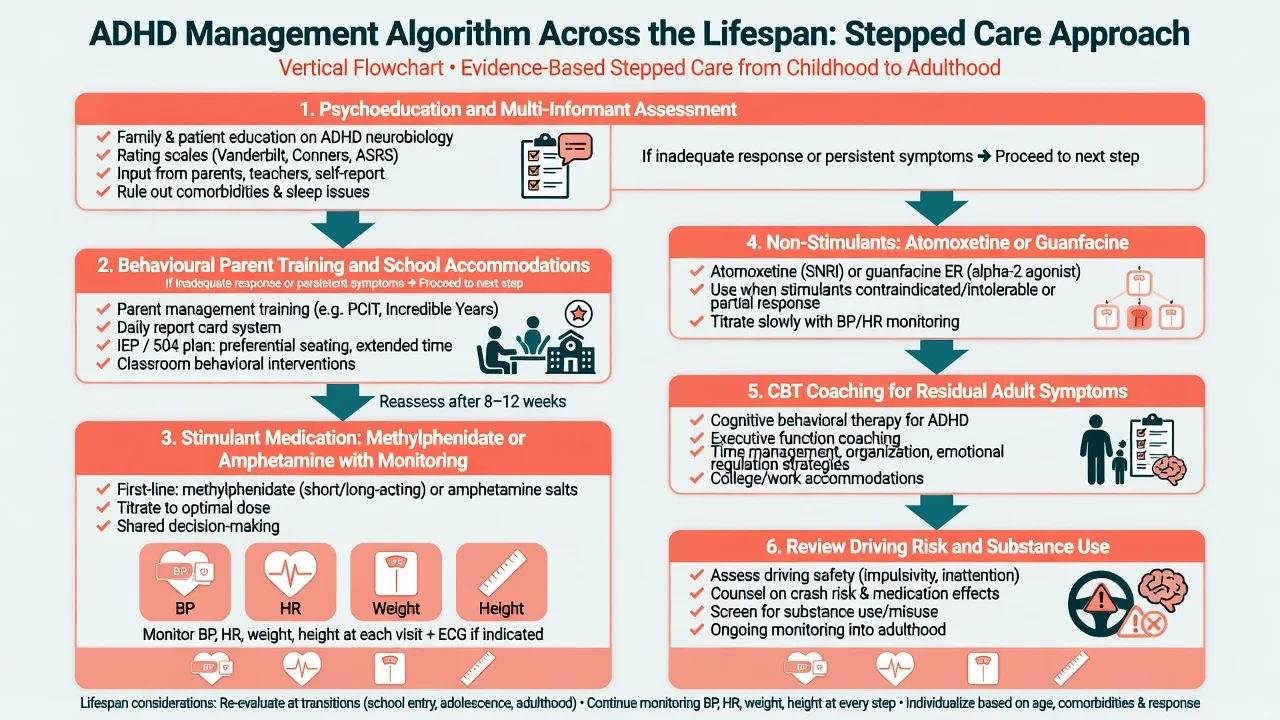
Psychoeducation for the patient and family is non-optional. Behavioural parent training and classroom interventions are foundational in children; school accommodations (preferential seating, chunked tasks, extended time) reduce impairment even when medication is used. For moderate to severe impairing ADHD, carefully managed medication has the strongest short-term effect on core symptoms.[1][17]
Australian and New Zealand practice follows local stimulant prescribing regulations (authority/PBS constraints vary by jurisdiction and age), shared care with GPs, and specialist initiation/review norms. Always check current local prescribing rules rather than memorising a single national form number for exams outside your state.[17]
Stimulants — agent, dose, monitoring
Network meta-analysis shows most ADHD medications outperform placebo for core symptoms at about 12 weeks; stimulants generally show the largest effect sizes, with amphetamines performing particularly well in adults and methylphenidate highly effective in children and adolescents in the Cortese NMA.[3]
Doses below are typical exam-level starting and titration frameworks — always individualise for age, formulation, hepatic/renal function and local product information.[3][17]
| Agent (examples) | Typical start (guide) | Common titration / range | Key notes |
|---|---|---|---|
| Methylphenidate IR | Child: often 5 mg orally 2–3 times daily | Titrate weekly; many product max around 60 mg/day (check label) | Short duration; diversion risk higher than long-acting |
| Methylphenidate long-acting (various) | Product-specific morning dose | Titrate to response; cover school/work day | Prefer for adherence and lower diversion |
| Lisdexamfetamine | Often 20–30 mg orally each morning | Titrate weekly; common max 70 mg/day | Prodrug; useful adult option |
| Mixed amphetamine salts / dexamfetamine | Low morning start; product-specific | Titrate; divide IR doses | Strong efficacy signal in adult NMA |
| Typical frameworks for exam answers; verify local product information and authority rules.[3][17] |
Onset. Stimulant benefit on core symptoms is often evident the same day at an adequate dose — unlike atomoxetine. Use that fact in viva when asked how you judge an early trial.[3][17]
Atomoxetine
Atomoxetine is a non-stimulant noradrenaline reuptake inhibitor useful when stimulants are poorly tolerated, contraindicated, diversion risk is high, or continuous day-long coverage without a controlled drug is preferred. In the pivotal once-daily RCT, atomoxetine separated from placebo on ADHD rating scales over weeks, not hours.[9]
Dosing (exam framework). Approximate start 0.5 mg/kg/day orally for at least 3 days, then increase toward a target near 1.2 mg/kg/day; usual maximum about 1.4 mg/kg/day or 100 mg/day (whichever is less) in many product labels — confirm local PI. Adults often start 40 mg daily and titrate toward 80 mg, max 100 mg depending on label. Counsel on GI upset, fatigue, sexual side-effects, rare hepatic injury (stop if jaundice/dark urine), and monitoring of suicidality especially early in treatment in youth.[9][17][19]
Guanfacine XR and clonidine
Extended-release guanfacine is an alpha-2A agonist with RCT evidence versus placebo in children and adolescents; useful as monotherapy alternative or adjunct, and particularly discussed when tics, aggression, or sleep-onset problems complicate the picture.[10]
Guanfacine XR dosing (exam framework). Often start 1 mg orally once daily, increase by 1 mg/week as tolerated; trial ranges commonly 1–4 mg/day (higher adolescent maxima exist on some labels). Monitor for sedation, hypotension and bradycardia; taper rather than abrupt stop after prolonged use. Clonidine (including extended-release where available) is a related alpha-2 option with more sedation; cardiac monitoring principles are similar.[10][17]
Monitoring schedule
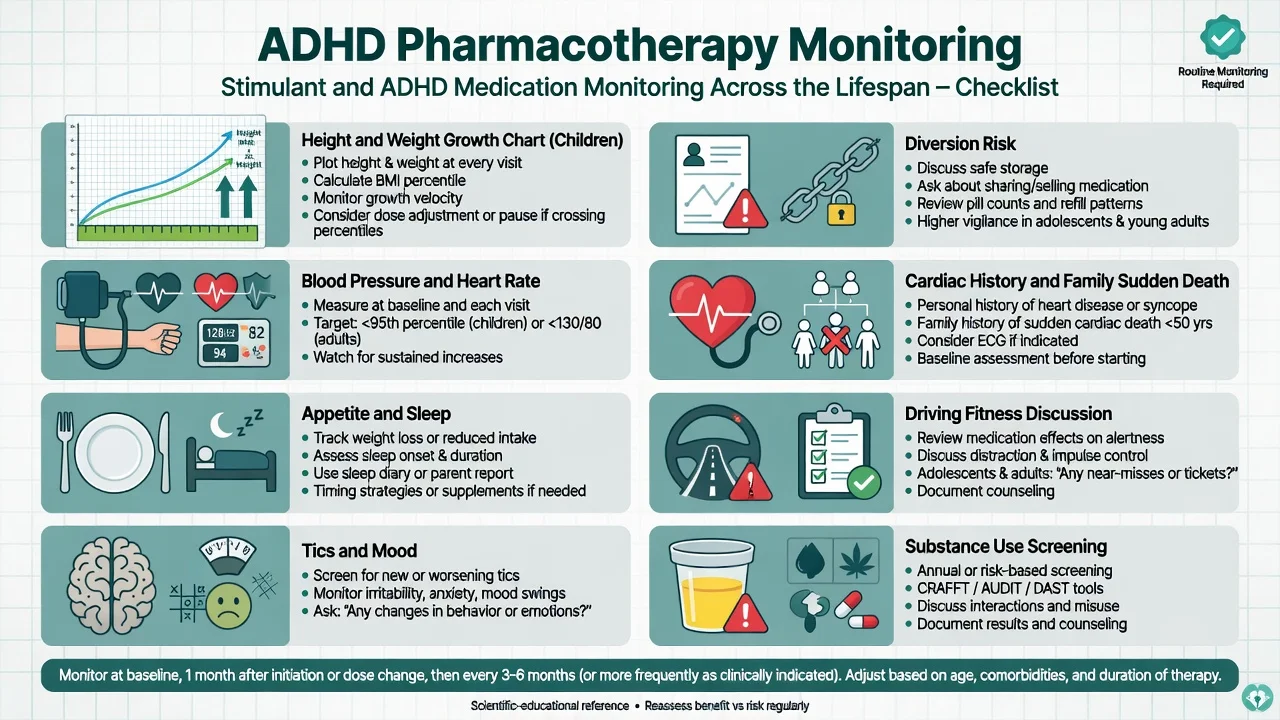
At baseline and follow-up: height/weight (children), BP, HR, appetite, sleep, tics, mood/anxiety/irritability, adherence, diversion (pill counts, early refill requests), driving, and substance use. Reassess after initiation or dose changes more frequently, then space reviews when stable.[14][17]
Psychological interventions and coaching
Behavioural parent training and school-based behavioural strategies are first-line psychosocial tools in childhood. For adults with residual symptoms despite medication, structured CBT targeting organisation, distractibility and adaptive thinking outperformed relaxation with educational support in a randomised trial by Safren and colleagues — so do not dismiss psychotherapy as "not biological enough."[11] Coaching, organisational skills training, and workplace/academic accommodations complement medication.[18][19]
Landmark trial logic examiners want
MTA (14 months). For children with combined-type ADHD, carefully delivered medication management and combined medication-plus-behavioural treatment were superior to behavioural treatment alone and to community care for core ADHD symptoms; combination offered advantages for non-ADHD domains and lower medication dose in some analyses.[1]
MTA at 8 years. Initial randomisation advantages attenuated; many youths remained symptomatic; naturalistic treatment intensity varied. Lesson: early gains do not guarantee lifelong automatic remission — ongoing needs assessment matters.[2]
Cortese 2018 NMA. Supports stimulants as highly efficacious short-term medications across ages, with tolerability and preference nuances by age group guiding shared choice.[3]
Specific subtypes and scenarios
Preschool. Prioritise parent training and environmental measures; medication is specialist-only after careful diagnosis and failure of behavioural approaches when impairment is severe.[17]
Adolescent transition. Plan adherence, driving counselling, substance education, and transfer to adult services before crisis.[16][19]
Adult first diagnosis. Demand developmental history and collateral; ASRS can screen but does not diagnose; exclude bipolar, SUD and medical mimics; document multi-setting impairment.[18][19]
ADHD + SUD. Higher lifetime SUD risk; untreated ADHD may promote self-medication; stimulant diversion is a real risk. Treat both conditions; consider non-stimulants or supervised long-acting stimulants; integrate addiction services.[12]
ADHD + tics. Stimulants are often still usable with monitoring; alpha-2 agonists can help both ADHD and tics in selected patients.[10][17]
ADHD + anxiety/depression. Treat active mood/anxiety syndromes; ADHD medication may still be indicated; watch activation and suicidality when combining treatments.[17][19]
Pregnancy. Shared decision with obstetric and perinatal psychiatry input; do not invent a universal "always stop" or "always continue" rule — individualise risk of untreated impairment versus medication exposure using current local guidance.[19]
Complications and pitfalls
Classic errors: diagnosing ADHD from a single questionnaire; missing learning disorder; mistaking bipolar for ADHD; prescribing short-acting stimulants into a diversion network without safeguards; ignoring growth charts; promising a "cure"; stopping treatment the week exams finish without functional review; omitting driving advice.[12][16][17]
Within-individual Swedish registry analyses found lower rates of criminality during periods of ADHD medication use versus non-medication periods — useful for discussing functional benefits, not for claiming medication alone prevents all crime.[13]
Prognosis and disposition
A substantial minority remit; many have partial remission with residual inattention and executive impairment into adulthood. Severity, comorbidity and adversity predict worse trajectories. Disposition ranges from shared-care primary care on stable long-acting medication to specialist clinics for complex comorbidity, SUD, or diagnostic uncertainty. Plan follow-up intensity around titration, then maintenance monitoring, with open access for crisis comorbidity.[2][4][19]
Special populations
Girls and women: active case-finding for inattentive presentations. Intellectual disability: adapted tools and higher medical comorbidity. Older adults: late presentation needs careful differential with cognitive disorders and polypharmacy. Cultural and Indigenous contexts in ANZ require culturally safe assessment and attention to service access, not stereotype-based diagnosis.[4][18]
Evidence, guidelines and regional differences
Large cohort work did not demonstrate increased serious cardiovascular events with ADHD drugs overall, though confidence intervals leave residual uncertainty and clinical cardiac screening remains indicated.[14]
Exam pearls
FOCUS
Self-test: name a first-line child plan with monitoring
For moderate-severe school-age ADHD after assessment: psychoeducation + school strategies + e.g. long-acting methylphenidate product-specific morning start with weekly titration, monitoring height/weight, BP, HR, appetite, sleep, mood/tics and diversion; review function with parent and teacher scales. If stimulants fail or are unsuitable: atomoxetine toward ~1.2 mg/kg/day or guanfacine XR from 1 mg with BP/HR/sedation checks.[3][9][10][17]
References
- [1]The MTA Cooperative Group A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. The MTA Cooperative Group. Multimodal Treatment Study of Children with ADHD Arch Gen Psychiatry, 1999.PMID 10591283
- [2]Molina BSG, Hinshaw SP, Swanson JM, Arnold LE, et al. The MTA at 8 years: prospective follow-up of children treated for combined-type ADHD in a multisite study J Am Acad Child Adolesc Psychiatry, 2009.PMID 19318991
- [3]Cortese S, Adamo N, Del Giovane C, Mohr-Jensen C, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis Lancet Psychiatry, 2018.PMID 30097390
- [4]Kessler RC, Adler L, Barkley R, Biederman J, et al. The prevalence and correlates of adult ADHD in the United States: results from the National Comorbidity Survey Replication Am J Psychiatry, 2006.PMID 16585449
- [5]Polanczyk G, de Lima MS, Horta BL, Biederman J, Rohde LA The worldwide prevalence of ADHD: a systematic review and metaregression analysis Am J Psychiatry, 2007.PMID 17541055
- [6]Simon V, Czobor P, Bálint S, Mészáros A, Bitter I Prevalence and correlates of adult attention-deficit hyperactivity disorder: meta-analysis Br J Psychiatry, 2009.PMID 19252145
- [7]Faraone SV, Perlis RH, Doyle AE, Smoller JW, et al. Molecular genetics of attention-deficit/hyperactivity disorder Biol Psychiatry, 2005.PMID 15950004
- [8]Willcutt EG, Doyle AE, Nigg JT, Faraone SV, Pennington BF Validity of the executive function theory of attention-deficit/hyperactivity disorder: a meta-analytic review Biol Psychiatry, 2005.PMID 15950006
- [9]Michelson D, Allen AJ, Busner J, Casat C, et al. Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: a randomized, placebo-controlled study Am J Psychiatry, 2002.PMID 12411225
- [10]Sallee FR, McGough J, Wigal T, Donahue J, et al. Guanfacine extended release in children and adolescents with attention-deficit/hyperactivity disorder: a placebo-controlled trial J Am Acad Child Adolesc Psychiatry, 2009.PMID 19106767
- [11]Safren SA, Sprich S, Mimiaga MJ, Surman C, et al. Cognitive behavioral therapy vs relaxation with educational support for medication-treated adults with ADHD and persistent symptoms: a randomized controlled trial JAMA, 2010.PMID 20736471
- [12]Wilens TE Attention deficit hyperactivity disorder and substance use disorders Am J Psychiatry, 2006.PMID 17151154
- [13]Lichtenstein P, Halldner L, Zetterqvist J, Sjölander A, et al. Medication for attention deficit-hyperactivity disorder and criminality N Engl J Med, 2012.PMID 23171097
- [14]Cooper WO, Habel LA, Sox CM, Chan KA, et al. ADHD drugs and serious cardiovascular events in children and young adults N Engl J Med, 2011.PMID 22043968
- [15]Vaa T ADHD and relative risk of accidents in road traffic: a meta-analysis Accid Anal Prev, 2014.PMID 24238842
- [16]Jerome L, Habinski L, Segal A Attention-deficit/hyperactivity disorder (ADHD) and driving risk: a review of the literature and a methodological critique Curr Psychiatry Rep, 2006.PMID 16968625
- [17]Pliszka S; AACAP Work Group on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder J Am Acad Child Adolesc Psychiatry, 2007.PMID 17581453
- [18]Kooij SJ, Bejerot S, Blackwell A, Caci H, et al. European consensus statement on diagnosis and treatment of adult ADHD: The European Network Adult ADHD BMC Psychiatry, 2010.PMID 20815868
- [19]Kooij JJS, Bijlenga D, Salerno L, Jaeschke R, et al. Updated European Consensus Statement on diagnosis and treatment of adult ADHD Eur Psychiatry, 2019.PMID 30453134