Psych · Child and adolescent psychiatry — adolescent substance use
Adolescent substance use
Also known as Youth substance use · Adolescent SUD · Teen drug and alcohol use · CAMHS addiction · Adolescent cannabis alcohol stimulants · Youth dual diagnosis · Adolescent substance misuse · Paediatric substance use disorder
Exam-exhaustive fellowship reference on adolescent substance use — developmental epidemiology, cannabis/alcohol/stimulants, dual diagnosis, CRAFFT and comprehensive assessment with private interview plus family and school, motivational interviewing, family-based therapies (MDFT, CYT), brief interventions, harm reduction, youth pharmacotherapy limits including buprenorphine-naloxone evidence, disposition, and regional guideline framing. Distinct from adult AUD/OUD and adult dual-diagnosis topics. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Adolescent substance use is a core child and adolescent psychiatry and CAMHS–AOD interface skillset: clarifying pattern and function of use, mapping developmental risk and protection, treating medical and psychiatric emergencies, and delivering psychosocial treatments with family systems at the centre.[1][2][4]
This topic is related to but distinct from adult alcohol-use-disorder, opioid-use-disorder, cannabis-use-and-psychosis, stimulant-and-methamphetamine-use, and general dual-diagnosis-and-integrated-care. Here the centre of gravity is developmental neurobiology, family-based therapy evidence, school and legal interfaces, Gillick/developmental competence and confidentiality limits, and youth-specific pharmacotherapy evidence (notably limited outside opioid agonist treatment trials).[4][14][17]
Language is clinical and ethical. Prefer substance use, substance use disorder (SUD), risky use, and recovery. Avoid pejorative labels (addict, junkie, dirty urine). Harm reduction is clinical risk management, not moral surrender.[2][4]
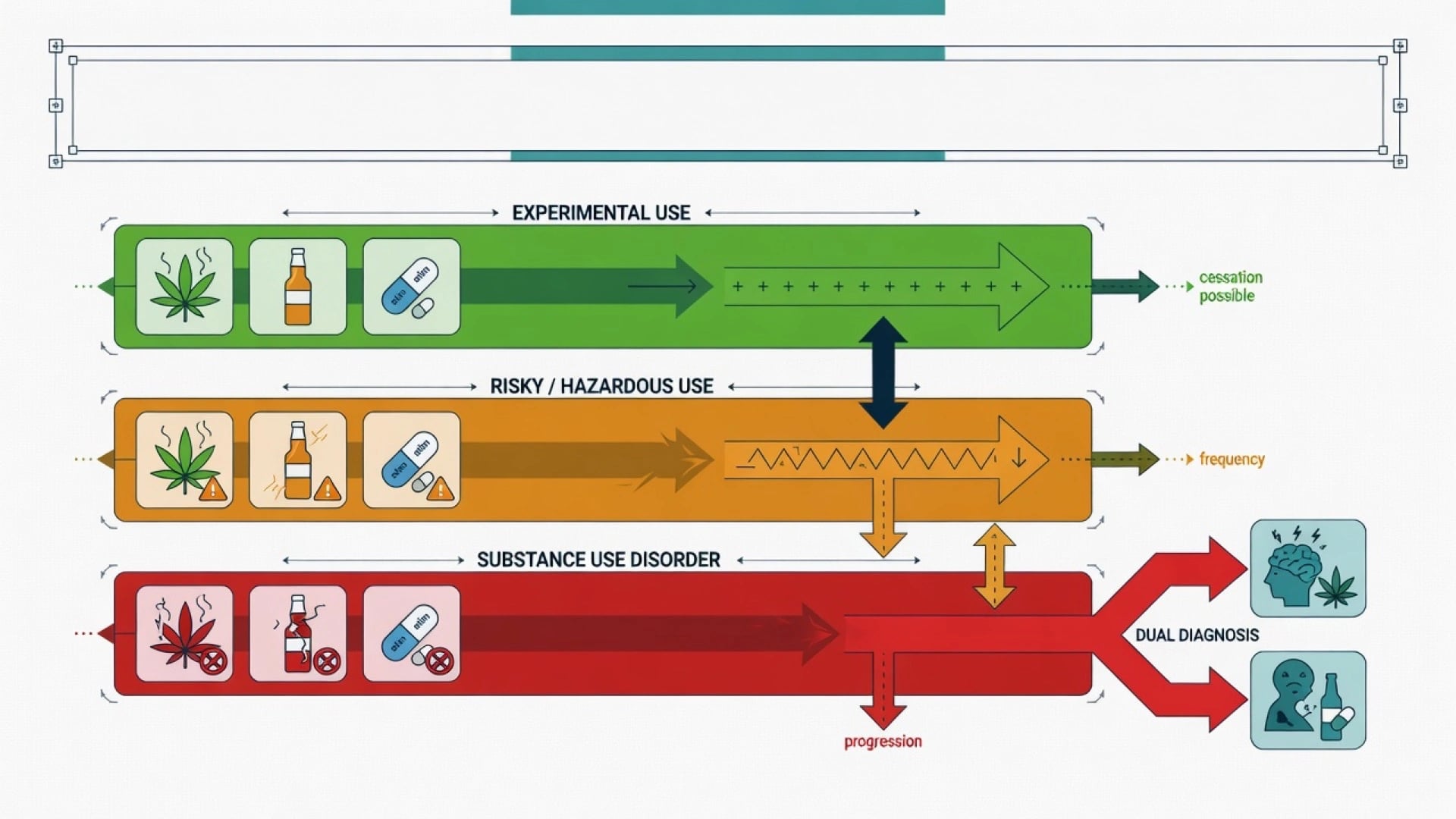
| Pattern | Working meaning in youth practice |
|---|---|
| Experimental / occasional | Limited episodes; still assess harm (injury, sex, driving, school) |
| Risky / hazardous | Pattern elevating acute harm (binges, high-THC daily, stimulant weekends) |
| Harmful use | Clear medical, psychiatric, social, or legal harm |
| SUD (DSM-5-TR) | Control, craving, tolerance/withdrawal, role failure, continued use despite harm — apply criteria developmentally |
| Dual diagnosis | Concurrent mental illness and substance use needing concurrent care |
Classification — substance classes and dual diagnosis
Primary classes examiners test: alcohol (binge pattern dominates adolescent harm), cannabis (THC potency and early onset matter), stimulants (methamphetamine, MDMA, cocaine, non-medical ADHD stimulants), opioids (including non-medical pharmaceuticals), nicotine/vaping, and polysubstance weekend patterns.[1][2][7]
Dual diagnosis means co-occurring mental illness and substance use. Etiological models include common vulnerability, self-medication, substance-induced psychiatric syndromes, and bidirectional worsening — fellowship answers avoid a single-model oversimplification and still insist on concurrent treatment.[20][21]
- High-THC products amplify risk
- Psychosis dose–response signals
- School/cognition impact
- Family therapy evidence base
- SIP vs primary psychosis work
- Binge pattern common
- Injury, blackouts, sexual risk
- Brief interventions help
- Withdrawal less common but serious
- Family monitoring critical
- Agitation, paranoia, crash
- Cardiovascular and sleep risk
- ADHD dual formulation
- Psychosis pathway overlap
- Medical first if unstable
Epidemiology and risk factors
Global burden attributable to substance use rises sharply through adolescence and young adulthood; alcohol and illicit substances contribute substantially to health loss in young men in many datasets.[1] Earlier onset of regular use predicts heavier young-adult sequelae and SUD risk — prevention and delayed initiation are therefore clinical, not only public-health, goals.[1][2][6]
Risk factors cluster as family SUD and low parental monitoring, peer use, trauma and adverse childhood experiences, ADHD and conduct problems, depression and anxiety, early school disengagement, LGBTQ+ minority stress, poverty and availability, and community norms favouring heavy use.[1][2][4] Protective factors include parental monitoring and warmth, school engagement, delayed first use, extracurricular belonging, cultural identity supports, and access to responsive youth-friendly care.[2][4]
Pathophysiology and developmental mechanisms
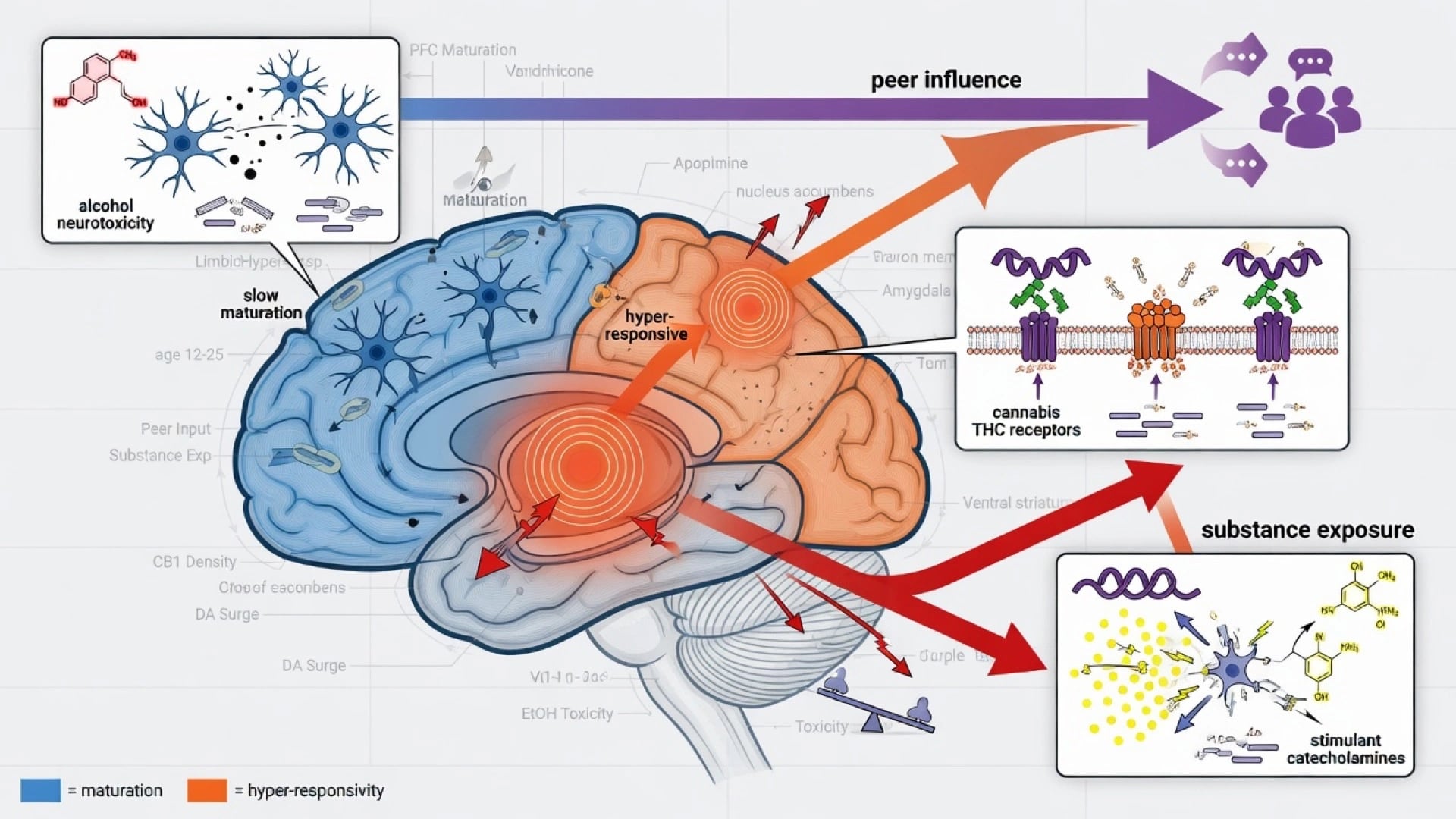
Adolescent brains show ongoing prefrontal maturation with relatively heightened limbic/reward reactivity; substance exposure during this window associates with neurocognitive differences in observational research (directionality is complex, but clinical caution is warranted).[5]
Alcohol binge patterns drive acute injury, blackouts, and cumulative neurodevelopmental concern.[2][5] Cannabis risk is dose-, frequency-, potency-, and age-of-onset-related: integrative cohort analyses show dose–response links between adolescent cannabis frequency and multiple young-adult adverse outcomes; reviews and longitudinal work support elevated psychotic outcome risk with early and heavy use; high-potency cannabis contributes to population psychosis incidence variation and first-episode case burden in high-use settings.[6][7][8][9][10][11] Continued cannabis after psychosis onset associates with worse relapse trajectories.[12] Stimulants produce catecholamine surge with agitation, paranoia, insomnia, cardiovascular strain, and crash dysphoria — dual formulation with primary psychosis or mania is essential.[1][4]
Clinical presentation
Presentations include ED intoxication or injury, parental discovery of vapes or cannabis products, school decline and truancy, CAMHS referral for mood/psychosis with concurrent use, youth justice diversion, and sexual health or sexual exploitation pathways.[1][4]
MSE themes: minimisation, peer-normalisation ("everyone does it"), externalising blame, intoxication vs withdrawal vs primary mood/psychosis, shame after blackouts, and fluctuating readiness for change.[18][19] Substance-specific patterns: cannabis-related amotivation, anxiety, or paranoia; alcohol blackouts and risk-taking; stimulant agitation and crash; opioid sedation and overdose risk.[4][7]
Differential diagnosis
Substance-induced mood, anxiety, or psychotic syndromes vs primary disorders with concurrent use — timeline relative to last use, family history, premorbid decline, and persistence after abstinence windows matter, but early dual care proceeds while the differential clarifies.[9][12][20] ADHD vs stimulant intoxication/withdrawal; conduct disorder vs SUD-maintained rule-breaking; trauma responses mislabelled as "just behavioural"; medical mimics (head injury, encephalitis, thyrotoxicosis, arrhythmia, seizure).[4][5] Avoid moral-failure formulations that fail CASC standards and destroy alliance.[4][18]
Clinical and bedside assessment
Process principles
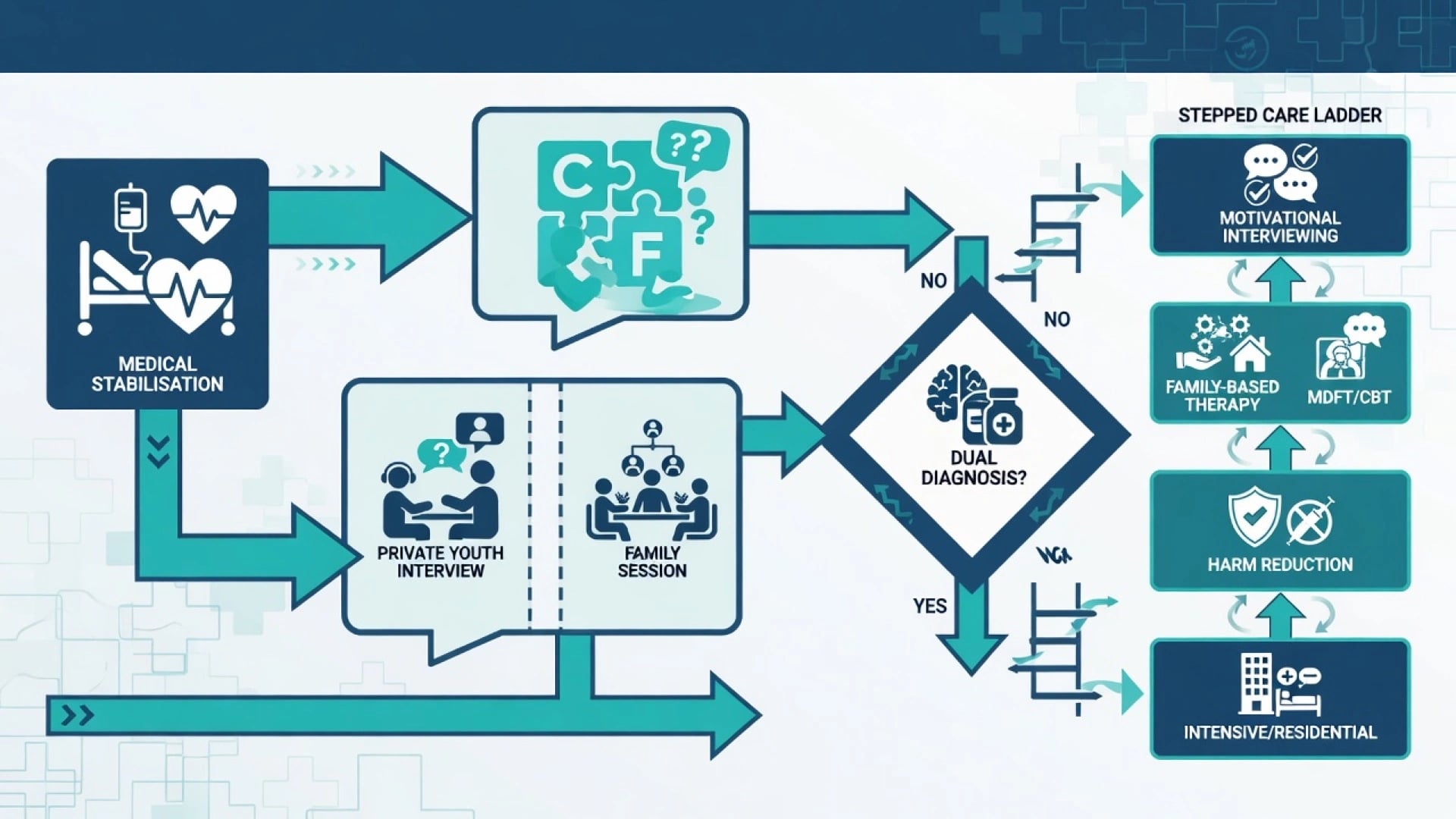
AACAP-style process standards for child/adolescent SUD emphasise comprehensive evaluation of use pattern, co-occurring disorders, family and social context, medical status, and multimodal treatment planning — not a single "drug test then lecture" encounter.[4]
CRAFFT and comprehensive assessment
CRAFFT is a validated brief screen for substance-related problems in adolescent clinic populations; a positive screen triggers fuller assessment, it does not replace diagnostic criteria, risk work, or formulation.[3] Cover first use, current frequency, quantity and potency (especially cannabis), route, context (peers, alone, trauma cues), last use, withdrawal, overdose, functional impact (school, family, legal, sexual risk, driving), and stages of change language.[3][4][19]
Private interview, family, school
Always attempt a private interview with the young person, then a family session. Explain confidentiality-with-safety limits up front. Developmental competence / Gillick-type concepts (jurisdiction-specific) inform consent and information-sharing — do not invent statute numbers; state the principle and apply local law.[4] Collateral from school, GP, AOD services, and youth justice completes the systems picture; safeguarding is always on the differential when exploitation, neglect, or domestic violence is possible.[2][4]
Investigations
Investigations follow the medical presentation: observations; ECG when stimulants, syncope, or cardiotoxic exposures are relevant; LFTs when heavy alcohol use is suspected; pregnancy test when relevant; blood-borne virus and STI testing when injecting or sexual risk is present. Toxicology (urine/oral fluid) is an adjunct with false negatives and positives — never the sole basis of care or discharge decisions.[4] Depression/anxiety scales and CRAFFT scores support measurement-based care but do not replace engagement.[3][4]
Management — immediate (crisis)
Immediate priorities: ABC and medical care for intoxication, overdose, trauma, or withdrawal; naloxone for opioid overdose; environment safety and proportionate observation; treat severe agitation with least-restrictive medical pathways; begin dual formulation if psychosis is present — do not withhold antipsychotics solely because toxicology is cannabis- or stimulant-positive; engage with non-stigmatising language; address acute safety (driving after use, overdose, exploitation).[2][4][7]
Management — definitive and stepwise
Motivational interviewing and brief interventions
Motivational interviewing (MI) is a collaborative, autonomy-supportive style that maps readiness and reduces resistance — foundational for youth who often arrive in precontemplation or ambivalence.[18][19] Meta-analytic evidence supports brief alcohol interventions for adolescents and young adults with modest but meaningful reductions in self-reported use.[16] Stockings and colleagues synthesise prevention, early intervention, harm reduction, and treatment evidence across tobacco, alcohol, and illicit drugs in young people — skills-based prevention beats information-only approaches; policy levers (price, availability, legal age) matter for alcohol and tobacco.[2]
Family-based and psychosocial treatments
Family-based treatments are among the strongest evidence-based psychosocial options for adolescent substance abuse in synthesis reviews; group CBT and other structured packages also show support with heterogeneity across trials.[14] The Cannabis Youth Treatment (CYT) multi-site randomised programme compared several outpatient models (including motivational enhancement/CBT and family-based approaches) and established that structured outpatient packages can reduce cannabis use with broadly comparable main effects across arms in many analyses — examiners use CYT as a landmark youth treatment trial, not as proof that "any contact is equal".[13] Multidimensional Family Therapy (MDFT) reduced cannabis dependence rates versus treatment as usual in a Western European multicentre RCT (INCANT programme).[15]
Harm reduction
Harm reduction goals for youth include delayed initiation, reduced binge intensity and frequency, not driving after use, safer sexual practices, overdose education and naloxone access when opioid risk exists, needle/syringe access where injecting occurs under local policy, school re-engagement, and negotiated partial goals when full abstinence is not immediately acceptable. This is exam-defensible clinical care, not collusion with ongoing harm.[2][4]
Dual diagnosis — concurrent care
Historical sequential models ("treat SUD only after mental health stabilises" or the reverse) worsen outcomes through service ping-pong. Integrated and concurrent dual-disorder principles — shared formulation, coordinated MI and psychosocial care, treating both conditions — remain the fellowship standard, with Cochrane synthesis of psychosocial dual interventions showing mixed but clinically important signals depending on intervention and population.[20][21][22] For high-THC cannabis and early psychosis, continue dual work with early intervention services; ongoing use after psychosis onset worsens relapse risk.[10][11][12]
Pharmacotherapy in youth (exam precision)
Psychosocial and family interventions are first-line for most adolescent SUD. Pharmacotherapy evidence is limited and specialist-framed.[2][4]
- Opioid use disorder: Woody and colleagues showed extended buprenorphine-naloxone improved outcomes versus short-term detoxification in opioid-addicted youth — extended agonist treatment beats brief detox-only pathways when clinically appropriate, with monitoring for diversion and adherence in a youth-capable service.[17] Typical adult-style dosing ranges are adapted under specialist protocols; examine indication, monitoring, and duration philosophy rather than inventing paediatric mg/kg recipes in viva without local formulary.
- Alcohol: naltrexone or acamprosate may be considered in older adolescents with established dependence in specialist settings — evidence is largely adult-extrapolated; combine with psychosocial care.[2][4]
- Cannabis / stimulants: no robust first-line anti-craving medication standard for adolescents; treat co-occurring ADHD, mood, anxiety, or psychosis on their merits with careful stimulant and sedative governance.[4][7]
- Nicotine: behavioural support plus age-appropriate nicotine replacement or other approved options per local guidance.[2][4]
Never use medication as a substitute for family engagement, safety planning, or school reintegration.[2][4]
Specific subtypes and scenarios
| Scenario | Emphasis |
|---|---|
| Cannabis-predominant, school failure | Potency/frequency; family therapy (MDFT/CYT models); cognition and motivation |
| Alcohol bingeing with injury | Brief intervention; family monitoring; injury prevention; MI |
| Methamphetamine with paranoia | Medical stability; dual psychosis pathway; sleep and crash plan |
| Polysubstance weekends | Functional analysis; peer context; harm reduction + family limits |
| Opioid / pharmaceutical opioid use | Overdose plan; naloxone; consider extended BUP/NX pathway |
| Vaping/nicotine co-use | Concurrent nicotine treatment; school policy interface |
| SUD + depression/self-harm | Concurrent mental health care; means and overdose risk |
| SUD + early psychosis / high-THC SIP | EI dual pathway; do not "wait for clean UDS" |
| ADHD + stimulant diversion | Secure storage; consider non-stimulant options; family monitoring |
| Looked-after / justice-involved | Multi-agency; placement stability; trauma-informed care |
Complications and pitfalls
- Interviewing only parents; skipping private youth interview
- Promising absolute confidentiality when safety requires disclosure
- Sequential care barriers between CAMHS and AOD
- Over-relying on toxicology without developmental formulation
- Ignoring family systems, school, and peers
- Withholding indicated psychiatric treatment until mythical abstinence
- Moralising language that destroys alliance
- Missing safeguarding, exploitation, or driving risk
- Assuming all cannabis is "soft" — potency and early onset matter
Prognosis and disposition
Many young people reduce or stop harmful use with delayed initiation, family engagement, and structured outpatient care; earlier onset, polysubstance patterns, untreated dual diagnosis, and ongoing high-potency cannabis after psychosis worsen trajectories.[1][6][12]
Disposition ladder (least restrictive safe option): match intensity to severity, dual diagnosis, home safety, and engagement.[2][4][14]
- Outpatient family-based / MI-CBT package with CAMHS–AOD coordination, school plan, and booked follow-up.[13][14][15]
- Intensive community / day programme when use is severe, dual diagnosis complex, or outpatient intensity insufficient.[2][4]
- Residential or inpatient dual care for medical withdrawal risk, severe psychosis/mania, high suicide/overdose risk, unsafe home, or failure of community intensity.[4][21]
Legal issues (possession, supply, driving) are jurisdiction-specific — state principles and local application; do not invent section numbers across countries.[4] Plan transition to adult AOD/mental health for late adolescents with ongoing need.[1][2]
Special populations
Early adolescents need stronger family control and school involvement; late adolescents may need more autonomy-supportive MI with still-active family work.[4][18] Indigenous and culturally diverse youth require cultural safety and community supports.[2] LGBTQ+ youth face minority stress and family rejection risks — affirming stance without pathologising identity.[1] ADHD/ASD/ID need adapted communication and careful medication governance.[4] Youth in care or justice need multi-agency plans.[2] Pregnant adolescents need obstetric dual care and substance-specific fetal risk counselling without punitive exclusion.[4] Rural/remote youth need telehealth and outreach models within local capacity.[2]
Evidence, guidelines, and regional differences
Landmark named evidence for viva: Degenhardt 2016 youth global burden;[1] Stockings 2016 prevention–treatment review;[2] CRAFFT Knight validation;[3] AACAP Bukstein practice parameter;[4] Squeglia adolescent brain;[5] Silins cannabis young-adult sequelae;[6] Volkow marijuana adverse effects;[7] Arseneault/Moore cannabis–psychosis;[8][9] Di Forti high-potency and EU-GEI;[10][11] Schoeler post-psychosis cannabis continuation;[12] CYT Dennis;[13] Waldron psychosocial synthesis;[14] MDFT Rigter INCANT;[15] Tanner-Smith brief alcohol interventions;[16] Woody buprenorphine-naloxone youth RCT;[17] dual-diagnosis theory and integrated care reviews.[20][21][22]
RANZCP and local CAMHS–AOD operational culture emphasises least-restrictive care, family-inclusive practice, cultural safety (including Aboriginal and Torres Strait Islander and Māori frameworks as applicable), and youth-friendly dual pathways. Exact legal instruments for involuntary care and drug offences are state/territory or national — quote local policy in clinical work; in exams state principles and flag jurisdiction. Core evidence still includes family-based therapy, MI, and concurrent dual care.[2][4][14]
Exam pearls
YOUTHDRUGS
References
- [1]Degenhardt L, Stockings E, Patton G, et al. The increasing global health priority of substance use in young people Lancet Psychiatry, 2016.PMID 26905480
- [2]Stockings E, Hall WD, Lynskey M, et al. Prevention, early intervention, harm reduction, and treatment of substance use in young people Lancet Psychiatry, 2016.PMID 26905481
- [3]Knight JR, Sherritt L, Shrier LA, et al. Validity of the CRAFFT substance abuse screening test among adolescent clinic patients Arch Pediatr Adolesc Med, 2002.PMID 12038895
- [4]Bukstein OG, Bernet W, Arnold V, et al. Practice parameter for the assessment and treatment of children and adolescents with substance use disorders J Am Acad Child Adolesc Psychiatry, 2005.PMID 15908844
- [5]Squeglia LM, Jacobus J, Tapert SF The influence of substance use on adolescent brain development Clin Psychol Rev, 2009.PMID 19278130
- [6]Silins E, Horwood LJ, Patton GC, et al. Young adult sequelae of adolescent cannabis use: an integrative analysis Lancet Psychiatry, 2014.PMID 26360862
- [7]Volkow ND, Baler RD, Compton WM, et al. Adverse health effects of marijuana use N Engl J Med, 2014.PMID 24897085
- [8]Arseneault L, Cannon M, Poulton R, et al. Cannabis use in adolescence and risk for adult psychosis: longitudinal prospective study BMJ, 2002.PMID 12446537
- [9]Moore TH, Zammit S, Lingford-Hughes A, et al. Cannabis use and risk of psychotic or affective mental health outcomes: a systematic review Lancet, 2007.PMID 17662880
- [10]Di Forti M, Marconi A, Carra E, et al. Proportion of patients in south London with first-episode psychosis attributable to use of high potency cannabis: a case-control study Lancet Psychiatry, 2015.PMID 26359901
- [11]Di Forti M, Quattrone D, Freeman TP, et al. The contribution of cannabis use to variation in the incidence of psychotic disorder across Europe (EU-GEI): a multicentre case-control study Lancet Psychiatry, 2019.PMID 30902669
- [12]Schoeler T, Petros N, Di Forti M, et al. Effects of continuation, frequency, and type of cannabis use on relapse in the first 2 years after onset of psychosis: an observational study Lancet Psychiatry, 2016.PMID 27567467
- [13]Dennis M, Godley SH, Diamond G, et al. The Cannabis Youth Treatment (CYT) Study: main findings from two randomized trials J Subst Abuse Treat, 2004.PMID 15501373
- [14]Waldron HB, Turner CW Evidence-based psychosocial treatments for adolescent substance abuse J Clin Child Adolesc Psychol, 2008.PMID 18444060
- [15]Rigter H, Henderson CE, Pelc I, et al. Multidimensional family therapy lowers the rate of cannabis dependence in adolescents: a randomised controlled trial in Western European outpatient settings Drug Alcohol Depend, 2013.PMID 23140805
- [16]Tanner-Smith EE, Lipsey MW Brief alcohol interventions for adolescents and young adults: a systematic review and meta-analysis J Subst Abuse Treat, 2015.PMID 25300577
- [17]Woody GE, Poole SA, Subramaniam G, et al. Extended vs short-term buprenorphine-naloxone for treatment of opioid-addicted youth: a randomized trial JAMA, 2008.PMID 18984887
- [18]Hettema J, Steele J, Miller WR Motivational interviewing Annu Rev Clin Psychol, 2005.PMID 17716083
- [19]Prochaska JO, DiClemente CC Stages and processes of self-change of smoking: toward an integrative model of change J Consult Clin Psychol, 1983.PMID 6863699
- [20]Mueser KT, Drake RE, Wallach MA Dual diagnosis: a review of etiological theories Addict Behav, 1998.PMID 9801712
- [21]Drake RE, Mercer-McFadden C, Mueser KT, et al. Review of integrated mental health and substance abuse treatment for patients with dual disorders Schizophr Bull, 1998.PMID 9853791
- [22]Hunt GE, Siegfried N, Morley K, et al. Psychosocial interventions for people with both severe mental illness and substance misuse Cochrane Database Syst Rev, 2019.PMID 31829430