Psych · Child and adolescent psychiatry — neurodevelopmental
Autism spectrum disorder
Also known as ASD · Autism · Autistic spectrum disorder · Asperger syndrome · Pervasive developmental disorder · PDD-NOS · Neurodevelopmental autism
Exam-exhaustive fellowship reference on autism spectrum disorder — DSM-5-TR criteria and levels, ICD-11 mapping, epidemiology and genetics, differentials (ADHD, intellectual disability, social anxiety, SCD, psychosis), multimodal assessment, behavioural and parent-mediated interventions, psychopharmacology for co-occurring irritability (risperidone and aripiprazole with monitoring), capacity, safeguarding and transition to adult care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Autism spectrum disorder (ASD) is a high-yield child-and-adolescent and adult psychiatry interface topic. Fellowship examiners test whether you can apply DSM-5-TR structure, separate ASD from ADHD, intellectual disability, social anxiety, social (pragmatic) communication disorder and psychosis using discriminators, run a multimodal assessment without delaying intervention, and prescribe for irritability only when indicated with RUPP-level evidence rather than reflex antipsychotics.[1][2][16][17]
Overview and definition
ASD is a neurodevelopmental condition, not a progressive neurodegenerative disease and not a personality style. Core features are (1) persistent deficits in social communication and social interaction across multiple contexts, and (2) restricted, repetitive patterns of behaviour, interests or activities (RRBs). Symptoms are present in the early developmental period (may not fully manifest until social demands exceed capacity), cause clinically significant impairment, and are not better explained by intellectual developmental disorder alone — when both are present, social communication must be below that expected for the general developmental level.[1][2]
DSM-5 collapsed previous categorical labels (autistic disorder, Asperger disorder, PDD-NOS) into a single spectrum with severity levels and specifiers (with/without intellectual impairment; with/without language impairment; associated with known medical/genetic condition; with catatonia).[2]
Classification

DSM-5-TR criteria structure (must be exam-ready)
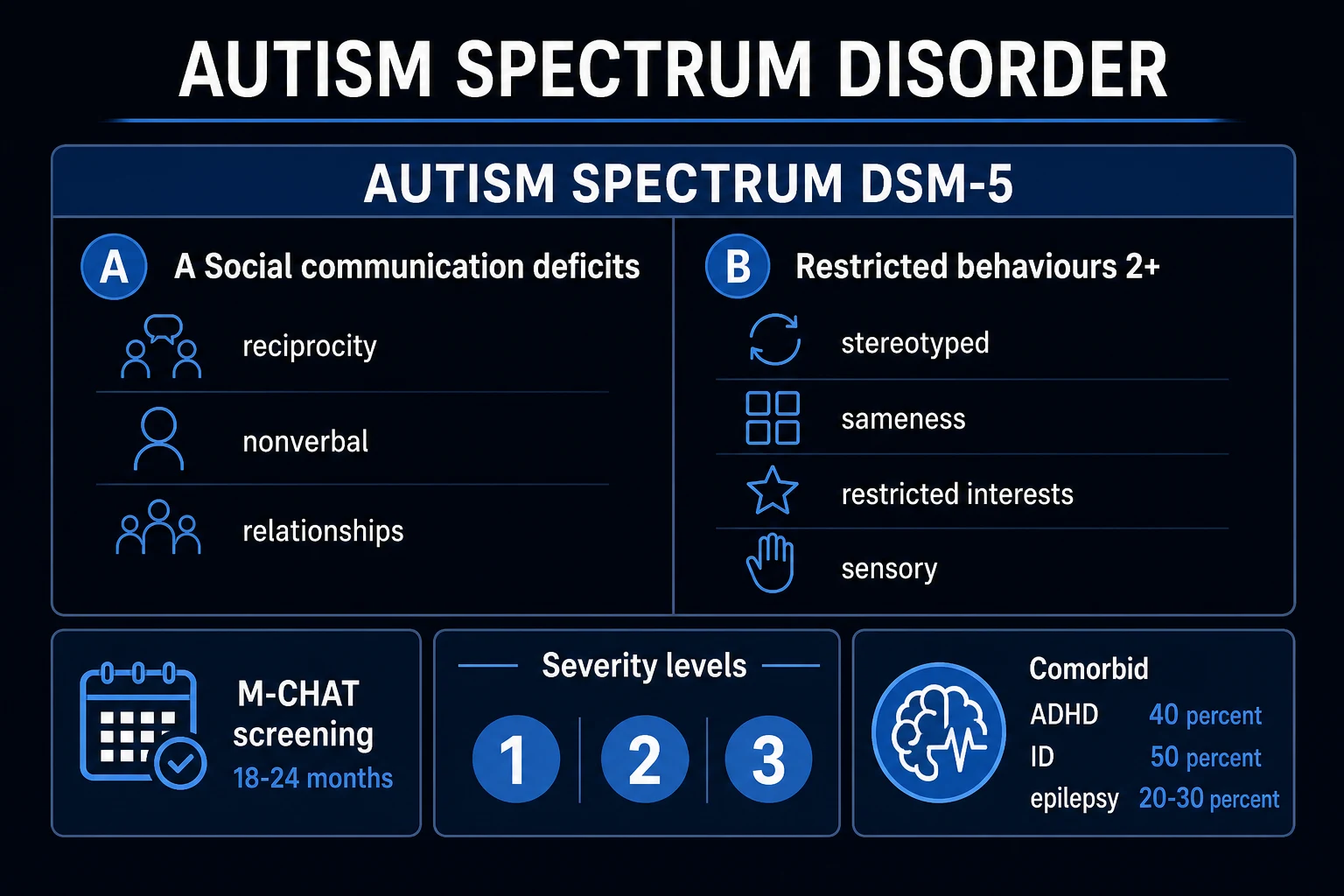
A. Social communication and social interaction — all three required (currently or by history): [1][2]
- Social-emotional reciprocity deficits (e.g. abnormal social approach, reduced sharing of interests/emotions, failure of normal back-and-forth conversation).
- Nonverbal communicative behaviours used for social interaction (e.g. poorly integrated verbal/nonverbal communication; abnormalities of eye contact and body language; deficits in understanding and use of gestures; total lack of facial expression).
- Developing, maintaining and understanding relationships (e.g. difficulties adjusting behaviour to social contexts; difficulties sharing imaginative play or making friends; absence of interest in peers).[1][2]
B. Restricted, repetitive patterns — at least two of four: [1][2]
- Stereotyped or repetitive motor movements, use of objects, or speech (e.g. simple motor stereotypies, lining up toys, echolalia, idiosyncratic phrases).
- Insistence on sameness, inflexible adherence to routines, or ritualised patterns of verbal or nonverbal behaviour.
- Highly restricted, fixated interests abnormal in intensity or focus.
- Hyper- or hyporeactivity to sensory input or unusual interest in sensory aspects of the environment.[1][2]
Severity levels (rate social communication and RRBs separately): Level 1 "requiring support"; Level 2 "requiring substantial support"; Level 3 "requiring very substantial support." Levels describe support need, not worth or intelligence.[1]
ICD-11. Autism spectrum disorder is coded as a neurodevelopmental condition with optional co-occurring intellectual developmental disorder and language impairment — state which manual you are using in multi-board answers.[2][17]
Epidemiology and risk factors
Headline ASD numbers for exams
Recent US Autism and Developmental Disabilities Monitoring (ADDM) Network surveillance estimated ASD prevalence among 8-year-olds on the order of 1 in 36 (about 2.8 percent) in the 2020 surveillance year, with site variation and continuing sex differences.[3] A global systematic review update estimated prevalence around 1 percent, with substantial methodological heterogeneity across regions.[4] Male predominance is robust but girls and women are under-recognised, especially with average or above-average language and camouflaging strategies.[2]
Genetics. Twin and family data support high heritability (on the order of 80 percent in large analyses).[5] Multi-country work supports substantial genetic contribution alongside measurable environmental associations (e.g. advanced parental age, perinatal factors) without a single environmental "cause."[6] Rare syndromic forms (fragile X, tuberous sclerosis complex, and others) matter for investigation after diagnosis.[1][16]
Exam trap: vaccines do not cause autism. Rehearse a calm, evidence-based explanation without shaming parents who have been exposed to misinformation.[1][2]
Pathophysiology
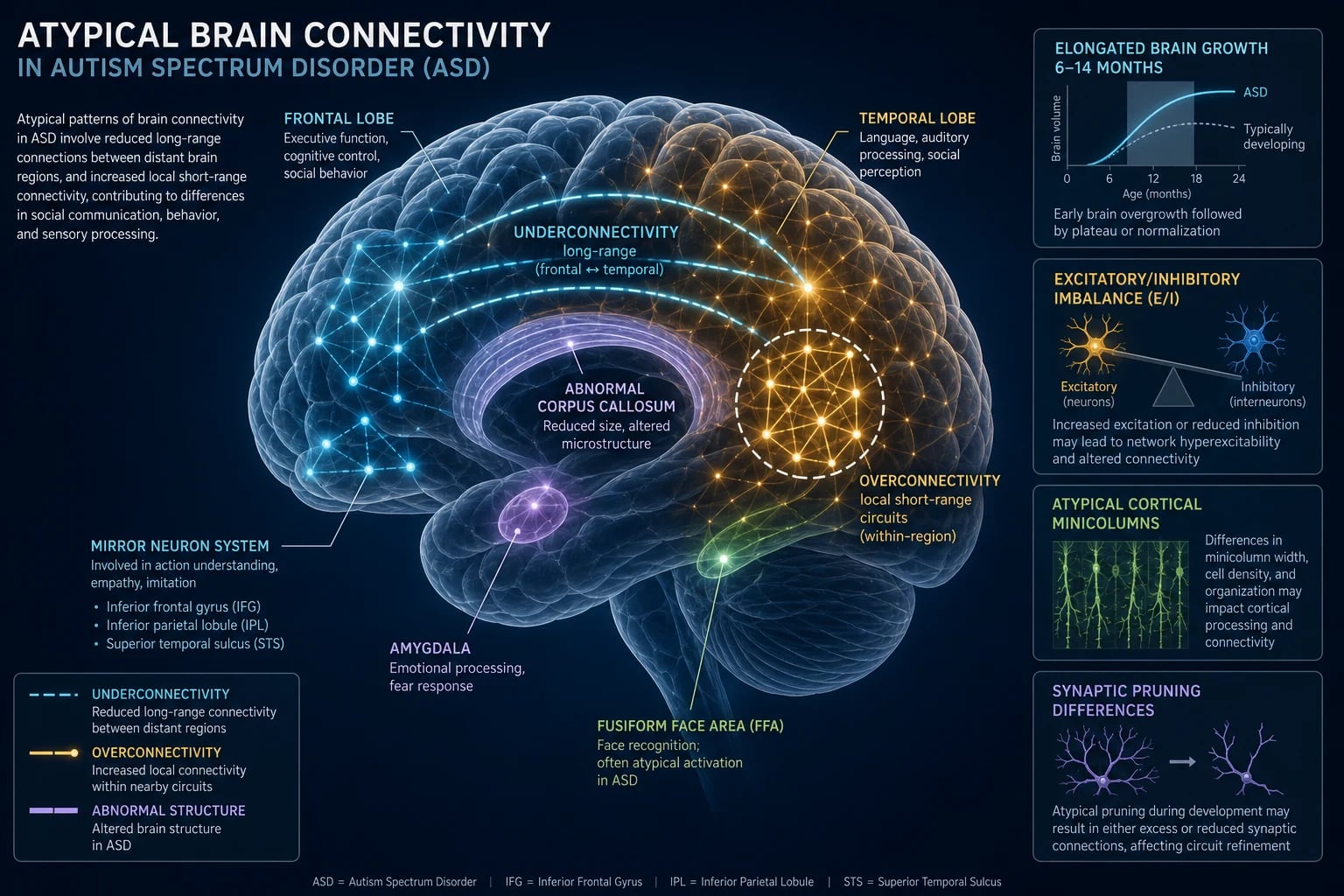
ASD reflects early atypical neurodevelopment affecting social brain networks, sensory processing and executive control. Architecture is polygenic plus rare high-impact variants in a subset; no blood test or MRI pattern diagnoses idiopathic ASD in routine practice.[2][5][6] Clinical diagnosis remains behavioural and developmental. Imaging and EEG are for red flags, not fishing expeditions.[1][16]
Clinical presentation
Toddler red flags. Limited response to name; reduced joint attention (pointing, showing, following gaze); limited eye contact; delayed or atypical language; reduced social smiling; restricted play (lining up, spinning); sensory aversions or seeking; motor stereotypies; distress at minor changes. Regression of language or social skills around 15–24 months is a classic red flag and warrants urgent assessment (still most often ASD pathway, but exclude alternative neurological disease when tempo or neurology is atypical).[1][18]
School age. Peer relationship difficulty, literal language, poor pragmatic conversation, intense special interests, rigid routines, sensory overwhelm in noisy classrooms, meltdowns when demands exceed coping, academic under- or uneven achievement.[1][2]
Adolescence and adult late diagnosis. Camouflaging/masking, social exhaustion ("autistic burnout"), identity questions, secondary anxiety and depression, workplace or university collapse under unstructured social load. History from childhood remains decisive.[2][17]
MSE adaptations. Allow processing time; reduce sensory load; use clear concrete language; do not equate flat affect or reduced eye contact with poor rapport or psychosis; assess risk and mood explicitly because suicidality is elevated in autistic populations.[19][20]
Differential diagnosis
Win differentials on developmental history, social motivation versus skill, ego-dystonicity of rituals, and form of unusual beliefs — not shopping lists.[1][2]
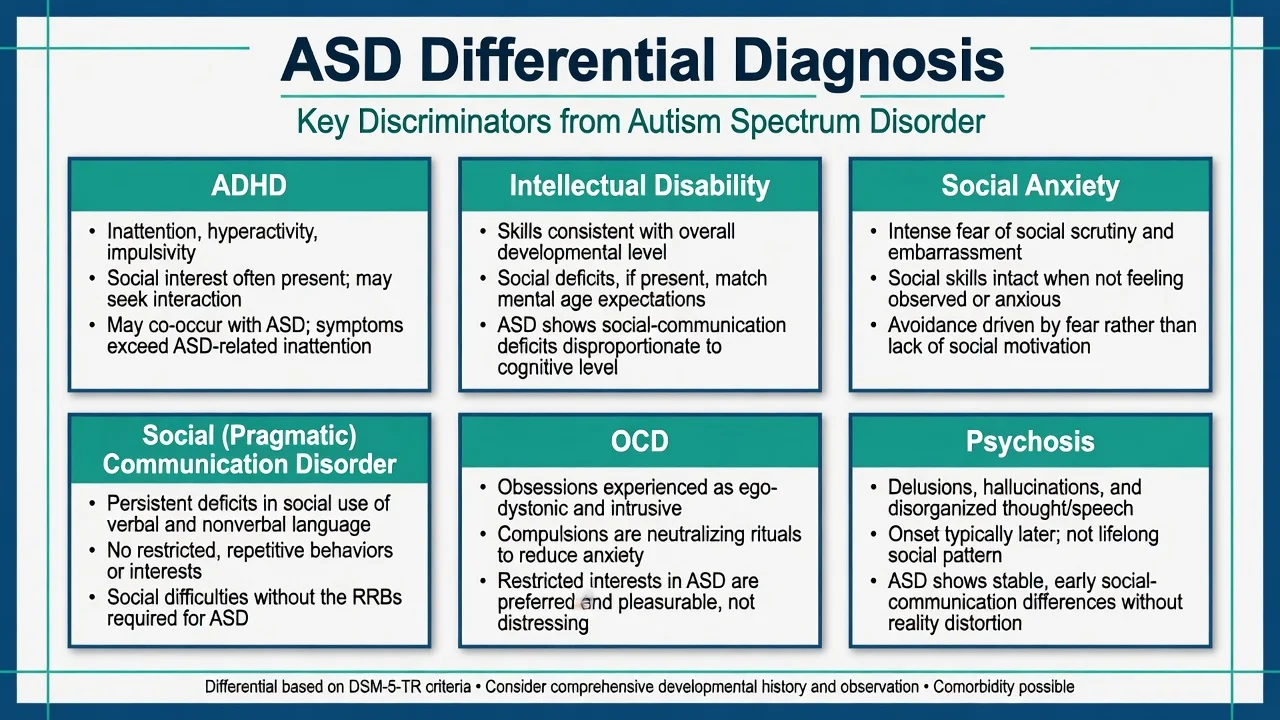
ADHD
- Core: inattention, hyperactivity, impulsivity
- Social interest often present; disruption may be secondary
- High true co-occurrence with ASD — dual diagnosis allowed
- Treat ADHD when criteria met; do not force a single label
Intellectual disability
- Global developmental delay across domains
- Social communication roughly matches developmental level in ID alone
- ASD requires social-communication deficit beyond developmental expectation
- Both can co-occur; assess adaptive function carefully
Social anxiety
- Fear of scrutiny and negative evaluation
- Social skills often intact when comfortable or online
- Onset typically later than lifelong autistic pattern
- Can co-occur — treat anxiety without erasing ASD
Psychosis / SCD / OCD
- SCD: social language deficits without RRBs
- OCD: ego-dystonic obsessions and neutralizing rituals
- Psychosis: delusions, hallucinations, thought disorder, later break
- Do not call lifelong autistic interests 'delusions'
Psychosis interface. Autistic people can develop true psychosis. Discriminate form (conviction, hallucination, thought disorder, functional break) from lifelong restricted interests and social communication style. Developmental history prevents both false-positive schizophrenia and false-negative psychosis via diagnostic overshadowing.[2][16]
Clinical and bedside assessment
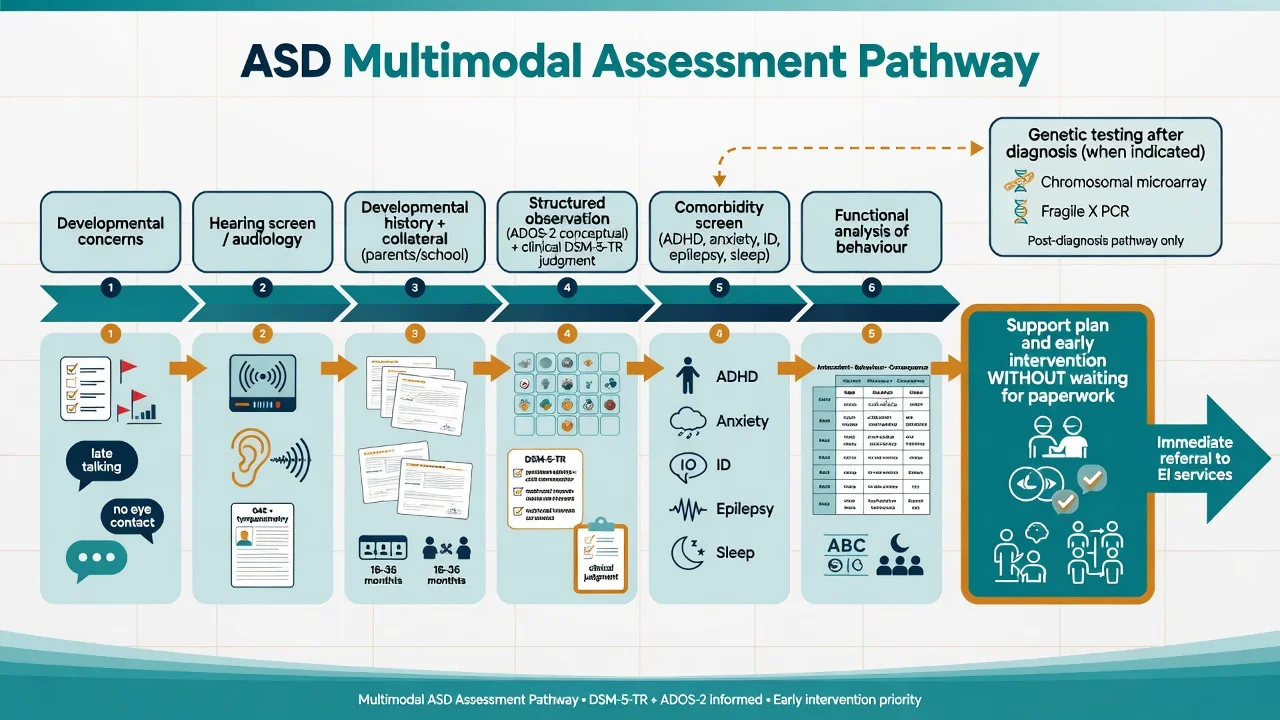
Structure fellowship assessments as follows:[1][16]
- Developmental timeline — pregnancy, birth, milestones, regression, language trajectory.
- Social communication examples — joint attention, peer play, conversation reciprocity, nonverbal behaviour.
- RRB and sensory inventory with concrete examples across settings.
- Collateral — parents/carers, school, previous reports.
- Function — adaptive skills, education, self-care, safety.
- Comorbidity screen — ADHD, anxiety, depression, OCD, ID, epilepsy, sleep, GI, feeding.
- Risk — self-injury, aggression, absconding, exploitation, neglect, suicidality.
- Capacity for specific decisions; legal status under local statute (least restrictive; do not invent foreign section numbers).
- Family system, culture, and carer burden.[1][15][16]
Screening and structured tools. M-CHAT-R/F is a validated toddler screen used in primary care pathways; positive screens need follow-up and referral, not diagnosis by checklist alone.[18] ADOS-2 and ADI-R are structured observational and interview instruments that support clinical judgment; they do not replace a developmental formulation.[1][16]
Functional analysis of challenging behaviour asks what the behaviour achieves (escape, attention, sensory, tangible) and what medical pain or sensory triggers are present before medication for irritability.[12][14]
Investigations
| Indication | Test / action | Note |
|---|---|---|
| Language delay / suspected ASD | Audiology | Do not skip hearing assessment |
| After ASD diagnosis (many guidelines) | Chromosomal microarray; fragile X testing | Especially with ID, dysmorphism, family history |
| Seizure, atypical regression, focal signs | EEG / neurology pathway | Not routine for classic ASD |
| Before antipsychotic for irritability | Weight/BMI, BP, glucose or HbA1c, lipids, FBC, U&E, LFT, ECG as indicated, prolactin baseline for risperidone | Monitor serially |
| Pain/medical drivers of behaviour | Dental, ENT, constipation, reflux, sleep apnoea | Common missed causes |
| [1][7][16] |
MRI is not a routine diagnostic test for typical ASD without neurological red flags.[1][16]
Management — acute crisis
De-escalate: reduce sensory load, use sparse language, offer predictable choices, avoid crowded noisy ED corridors when safe, involve familiar carers. Exclude pain, delirium, seizure, intoxication and catatonia. Use least-restrictive safety measures. Antipsychotics are not first-line for transient meltdowns driven by overload.[14][16]
[16]Management — definitive and stepwise
Core principle
No medication treats core ASD social-communication deficits as a primary indication. Primary treatments are developmental, educational, behavioural and environmental, with targeted pharmacotherapy for comorbidities and severe irritability when criteria are met.[1][14][16]
Early behavioural and developmental intervention
Early Start Denver Model (ESDM). A randomised trial in toddlers with autism showed gains in IQ, adaptive behaviour and diagnostic severity markers versus community intervention referral — the exam landmark for intensive early developmental intervention.[9]
PACT (parent-mediated communication-focused treatment). A randomised trial improved parent-child dyadic social communication; long-term follow-up reported sustained benefits on autism symptom trajectories — key evidence that parent-mediated approaches can alter course markers beyond the active treatment window.[10][11]
Parent training for disruptive behaviour. Structured parent training outperformed parent education alone for reducing disruptive behaviours in children with ASD in a randomised trial — behavioural skill-building for carers is not optional soft care.[12]
Practical package examiners expect: speech and language therapy (including AAC when needed), occupational therapy for sensory/adaptive skills, educational adjustments, structured teaching approaches, and family psychoeducation. Start supports while diagnostic assessment proceeds when clinical concern is high.[1][17]
Psychopharmacology for co-occurring irritability
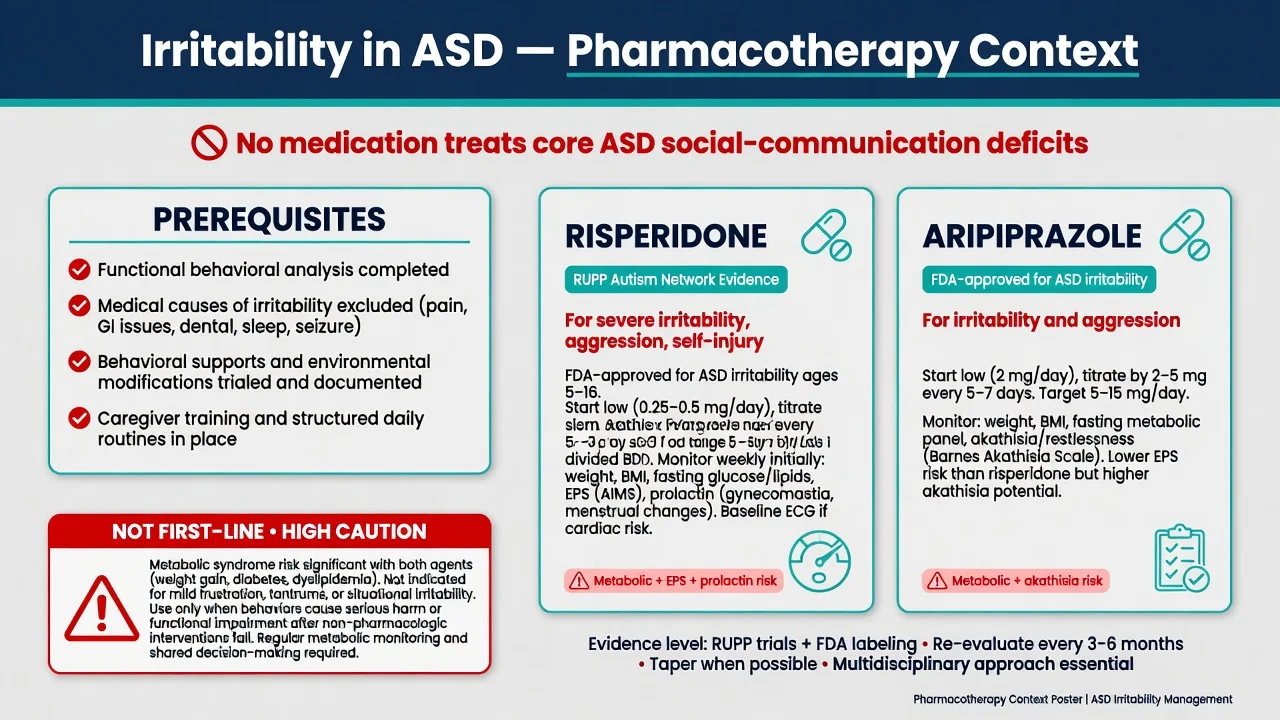
Indication. Severe irritability (aggression, severe tantrums, self-injury) causing safety risk or major impairment after environmental and behavioural measures, not mild frustration or social awkwardness.[7][8][14]
Risperidone — RUPP landmark. In the Research Units on Pediatric Psychopharmacology Autism Network trial, risperidone substantially reduced serious behavioural problems versus placebo in children with autism, at the cost of weight gain and other adverse effects.[7] Practical dosing is weight-based and low-start: for many school-age children, start around 0.25–0.5 mg/day, titrate slowly; RUPP mean doses were typically in the 1–2 mg/day range (higher maximums used under protocol by weight band). Always check current local product information and age licensing.[7][14]
Monitoring for risperidone: weight and BMI every visit initially; fasting glucose/HbA1c and lipids at baseline and serially; EPS examination; prolactin-related symptoms (galactorrhoea, amenorrhoea, gynaecomastia); sedation; ECG if cardiac risk. Plan review for dose minimisation once behaviour stabilises.[7][14][16]
Aripiprazole. Owen and colleagues demonstrated efficacy for irritability in children and adolescents with autistic disorder versus placebo in a randomised controlled trial (fixed-dose design including 5, 10 and 15 mg/day arms in related aripiprazole ASD irritability programmes; use local product information for start and titration).[8] Common clinical start is 2 mg daily with titration toward the effective trial range, watching for akathisia, activation, and metabolic effects (often milder weight gain than risperidone but not free of metabolic risk).[8][14]
Systematic synthesis. Meta-analytic evidence supports risperidone and aripiprazole for severe irritability/problem behaviours, with adverse-effect trade-offs that mandate monitoring and time-limited goals.[14]
What not to do. Do not prescribe SSRIs expecting reduction of core RRBs — citalopram was ineffective for high levels of repetitive behaviour in a large randomised trial and caused more adverse events than placebo.[13] Treat co-occurring anxiety or OCD on their own merits with adapted CBT and careful SSRI use, not as a stealth core-ASD treatment.[13][15]
Comorbidity-targeted care
Population-derived data show very high rates of additional psychiatric diagnoses in children with ASD — ADHD, anxiety, oppositional defiant behaviours and others are common, not exotic.[15] Treat ADHD with behavioural supports and, when indicated, stimulants or non-stimulants with careful titration and side-effect monitoring; treat epilepsy, sleep disorders (including melatonin pathways under local guidance), and depression/anxiety with autism-adapted psychological care.[1][15][16]
Specific subtypes and scenarios
Toddler early identification. Screen, audiology, parallel referral to diagnostic and early intervention services — do not wait months for a single "final" appointment to start support.[1][18]
School-age ASD + ADHD. Dual diagnosis is allowed; educational plan must address both attention and social-communication needs.[15]
Female adolescent late diagnosis. Camouflaging, internalising comorbidity, and mislabeling as pure anxiety or "shy" are classic traps.[2]
Adult first diagnosis. General adult psychiatrists must take developmental history; co-manage employment, housing and mental health; avoid iatrogenic over-medication.[17]
ASD with suspected psychosis. Full FEP work-up when form criteria met; adapt communication; involve carers; do not withhold antipsychotics solely because of ASD label if psychosis is present.[16]
Transition CAMHS to adult services. Plan early (often from mid-teens), written care plan, education/employment pathway, medication review, housing and safeguarding.[17]
Capacity, safeguarding and transition
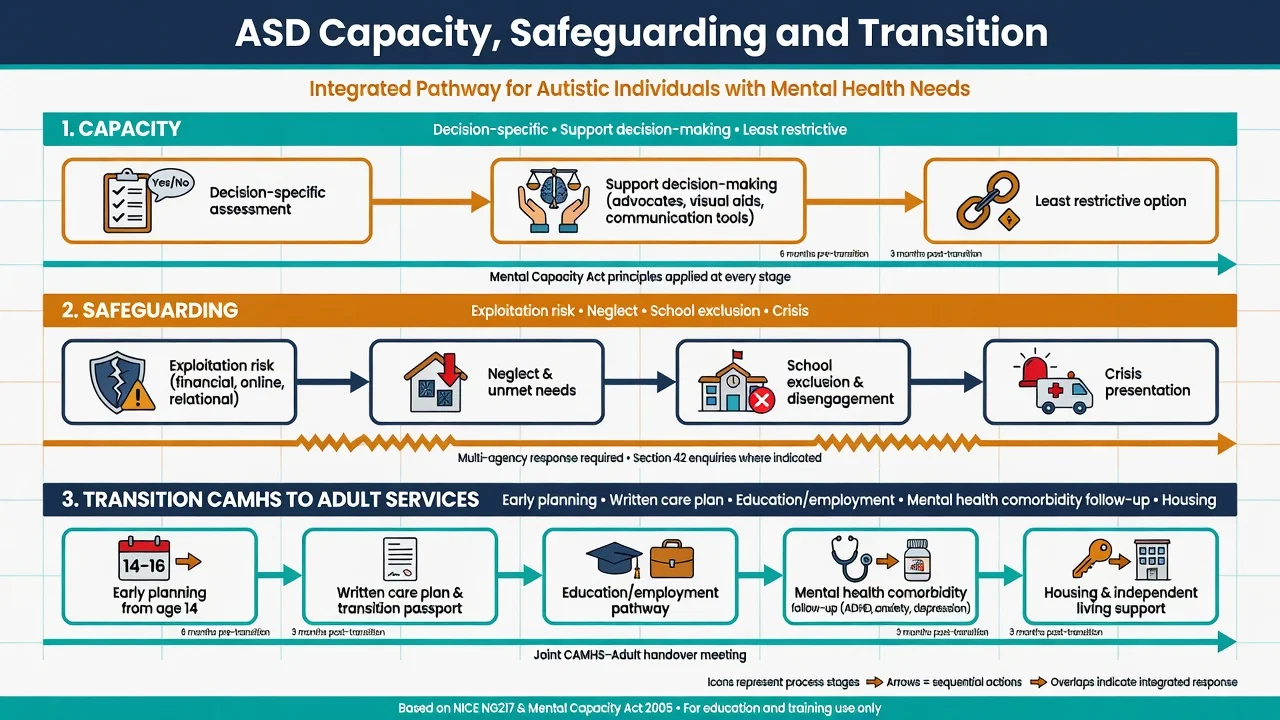
Capacity is decision-specific and time-specific. Support decision-making with plain language, visual aids, extra time and trusted supporters. Least-restrictive principle applies; statutes are jurisdiction-specific — name principles, not invented foreign sections.[17]
Safeguarding. Autistic children and adults face elevated risk of bullying, exploitation (including online), school exclusion, and unmet care needs. Report under local child protection / adult safeguarding duties when thresholds are met.[17][19]
Transition. Abrupt discharge at 18 without adult pathway is a systems failure. Handover should include diagnosis summary, communication profile, risk formulation, medication plan, and named adult service.[17]
Complications and pitfalls
- Diagnostic overshadowing: missing depression, ADHD, abuse, seizures or psychosis because "it is just autism."[15][16]
- Premature antipsychotic for mild behavioural distress without functional analysis.[14]
- Metabolic harm, EPS, hyperprolactinaemia from chronic risperidone without review.[7][14]
- Missing suicide risk — autistic people have elevated premature mortality and suicide-related risk; ask directly and safety-plan.[19][20]
- Vaccine mythology wasting clinical time and trust.[1]
- Withholding intervention while waiting for diagnostic bureaucracy.[1][9]
- Using citalopram/SSRIs as "autism drugs" for RRBs despite negative RUPP evidence.[13]
Prognosis and disposition
Outcomes are highly variable. Better adaptive outcomes associate with stronger early language, higher cognitive ability, earlier access to supports, lower comorbidity burden and stable environments — none of which license therapeutic nihilism for those with higher support needs.[2][17] Population data show premature mortality risk in ASD, with neurological and psychiatric comorbidity contributing — physical health and mental health both matter for lifespan.[19] Disposition is multiagency: health, education, disability supports, and family. Step intensity to risk and function, not to stigma.[17]
Special populations
Intellectual disability co-occurrence. Dual diagnosis is common; adapt communication, capacity assessment and behavioural plans; genetic testing yield is higher.[1][16]
Girls and women. Later diagnosis, internalising presentations, camouflaging — maintain a low threshold for developmental re-evaluation.[2]
Cultural and Indigenous contexts. Tools and social norms are culturally framed; use interpreters, cultural consultation and collateral that understands the child's community without lowering the diagnostic bar for impairment.[17]
Forensic and vulnerability. Suggestibility, exploitation and misunderstanding of autistic communication in justice settings require specialist advocacy.[17]
Evidence, guidelines and regional differences
Practice aligns with multidisciplinary diagnosis, early intervention access (NDIS interface in Australia), educational adjustments, and judicious psychopharmacology. RANZCP-relevant CAP training expects DSM-5-TR fluency, comorbidity management, capacity principles under local mental health and guardianship law, and transition planning. Physical health monitoring with antipsychotics is non-negotiable.[1][16]
Landmark list to name in viva: Hyman AAP 2020; AACAP parameter 2014; Lai Lancet 2014; Maenner ADDM 2023; Zeidan global prevalence 2022; Sandin heritability; McCracken RUPP risperidone; Owen aripiprazole; Dawson ESDM; Green/Pickles PACT; Bearss parent training; King citalopram negative trial; Fung meta-analysis irritability; Simonoff comorbidity; Lord Lancet Commission; Hirvikoski mortality; Cassidy suicide prevention framing.[1][7][8][9][17][19]
Exam pearls
[1] [7] [8] [20]SPECTRUM
Self-test: 7-year-old with ASD, daily aggression and self-hitting
Confirm ASD formulation and current supports. Functional analysis (triggers, function of behaviour). Medical pain screen (dental, constipation, otitis, sleep). Optimise parent training and school plan. If severe ongoing risk after behavioural measures, discuss risperidone or aripiprazole with weight-based low start, consent, baseline metabolic/ECG/prolactin as indicated, and review timeline for dose minimisation. Do not add SSRI for RRBs based on King negative trial. Assess sibling safety and carer burnout.[7][8][12][13]
References
- [1]Hyman SL, Levy SE, Myers SM; Council on Children with Disabilities, Section on Developmental and Behavioral Pediatrics Identification, Evaluation, and Management of Children With Autism Spectrum Disorder Pediatrics, 2020.PMID 31843864
- [2]Lai MC, Lombardo MV, Baron-Cohen S Autism Lancet, 2014.PMID 24074734
- [3]Maenner MJ, Warren Z, Williams AR, et al. Prevalence and Characteristics of Autism Spectrum Disorder Among Children Aged 8 Years - Autism and Developmental Disabilities Monitoring Network, 11 Sites, United States, 2020 MMWR Surveill Summ, 2023.PMID 36952288
- [4]Zeidan J, Fombonne E, Scorah J, et al. Global prevalence of autism: A systematic review update Autism Res, 2022.PMID 35238171
- [5]Sandin S, Lichtenstein P, Kuja-Halkola R, Hultman C, Larsson H, Reichenberg A The Heritability of Autism Spectrum Disorder JAMA, 2017.PMID 28973605
- [6]Bai D, Yip BHK, Windham GC, et al. Association of Genetic and Environmental Factors With Autism in a 5-Country Cohort JAMA Psychiatry, 2019.PMID 31314057
- [7]McCracken JT, McGough J, Shah B, et al.; Research Units on Pediatric Psychopharmacology Autism Network Risperidone in children with autism and serious behavioral problems N Engl J Med, 2002.PMID 12151468
- [8]Owen R, Sikich L, Marcus RN, et al. Aripiprazole in the treatment of irritability in children and adolescents with autistic disorder Pediatrics, 2009.PMID 19948625
- [9]Dawson G, Rogers S, Munson J, et al. Randomized, controlled trial of an intervention for toddlers with autism: the Early Start Denver Model Pediatrics, 2010.PMID 19948568
- [10]Green J, Charman T, McConachie H, et al. Parent-mediated communication-focused treatment in children with autism (PACT): a randomised controlled trial Lancet, 2010.PMID 20494434
- [11]Pickles A, Le Couteur A, Leadbitter K, et al. Parent-mediated social communication therapy for young children with autism (PACT): long-term follow-up of a randomised controlled trial Lancet, 2016.PMID 27793431
- [12]Bearss K, Johnson C, Smith T, et al. Effect of parent training vs parent education on behavioral problems in children with autism spectrum disorder: a randomized clinical trial JAMA, 2015.PMID 25898050
- [13]King BH, Hollander E, Sikich L, et al.; STAART Psychopharmacology Network Lack of efficacy of citalopram in children with autism spectrum disorders and high levels of repetitive behavior: citalopram ineffective in children with autism Arch Gen Psychiatry, 2009.PMID 19487623
- [14]Fung LK, Mahajan R, Nozzolillo A, et al. Pharmacologic Treatment of Severe Irritability and Problem Behaviors in Autism: A Systematic Review and Meta-analysis Pediatrics, 2016.PMID 26908468
- [15]Simonoff E, Pickles A, Charman T, Chandler S, Loucas T, Baird G Psychiatric disorders in children with autism spectrum disorders: prevalence, comorbidity, and associated factors in a population-derived sample J Am Acad Child Adolesc Psychiatry, 2008.PMID 18645422
- [16]Volkmar F, Siegel M, Woodbury-Smith M, King B, McCracken J, State M; American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI) Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder J Am Acad Child Adolesc Psychiatry, 2014.PMID 24472258
- [17]Lord C, Charman T, Havdahl A, et al. The Lancet Commission on the future of care and clinical research in autism Lancet, 2022.PMID 34883054
- [18]Robins DL, Casagrande K, Barton M, Chen CM, Dumont-Mathieu T, Fein D Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F) Pediatrics, 2014.PMID 24366990
- [19]Hirvikoski T, Mittendorfer-Rutz E, Boman M, Larsson H, Lichtenstein P, Bölte S Premature mortality in autism spectrum disorder Br J Psychiatry, 2016.PMID 26541693
- [20]Cassidy S, Rodgers J Understanding and prevention of suicide in autism Lancet Psychiatry, 2017.PMID 28551299