Psych · Child and adolescent psychiatry — anxiety disorders
Child and adolescent anxiety
Also known as Paediatric anxiety · Youth anxiety disorders · Separation anxiety disorder · Child GAD · Adolescent social anxiety · School refusal · Selective mutism · CAMS trial · Coping Cat
Exam-exhaustive fellowship reference on child and adolescent anxiety — separation anxiety, GAD, social anxiety, selective mutism, school refusal functional analysis, exposure-based CBT, SSRI evidence (CAMS, RUPP, fluoxetine, paroxetine, duloxetine), family accommodation, and stepped care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Child and adolescent anxiety is a high-yield FRANZCP CAP domain, MRCPsych CASC/Paper topic, and ABPN blueprint area. Examiners test DSM/ICD distinctions, developmental norms versus disorder, school refusal formulation, CBT mechanics (not brand names alone), SSRI trial names and comparative response rates, family accommodation, and safety monitoring — not superficial “offer CBT” answers.[5][6][12]
Overview and definition
Anxiety disorders are syndromes of excessive fear or anxiety with associated avoidance, physiological arousal, and functional impairment that are developmentally inappropriate in intensity, duration, or context. In youth the same major anxiety constructs used in adult psychiatry apply, but age of onset, somatic presentation, family systems, school function, and consent frameworks reshape assessment and treatment intensity.[5][12]
Normative developmental fears (strangers in toddlers; darkness or animals in preschoolers; social evaluation in adolescents) are not disorders unless they are excessive, persistent, and impairing. Disorder-level anxiety predicts concurrent impairment and elevated adult psychiatric and functional risk if untreated.[12][14][23]
Classification
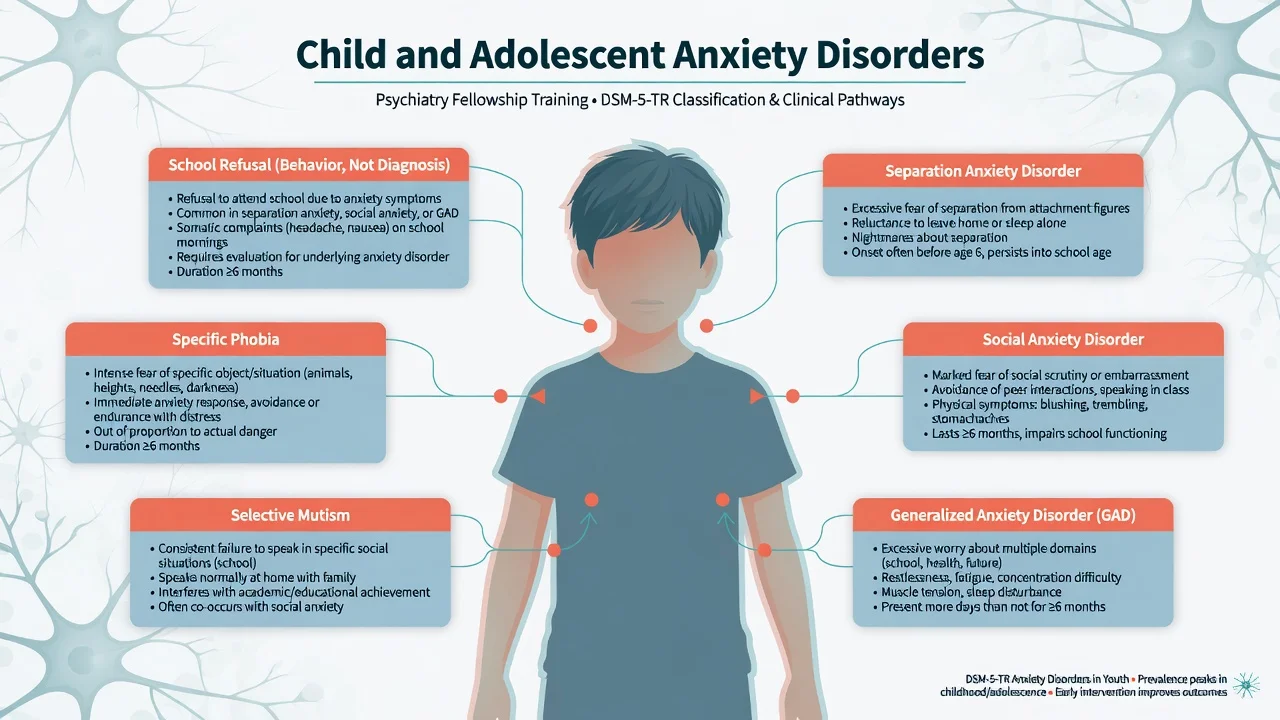
DSM-5-TR anxiety diagnoses most examined in CAP: separation anxiety disorder; selective mutism; specific phobia; social anxiety disorder (social phobia); panic disorder; agoraphobia; generalised anxiety disorder. Obsessive-compulsive disorder and PTSD are classified outside the anxiety chapter in DSM-5-TR but frequently co-occur and appear in differentials.[5][12]
Separation anxiety disorder. Developmentally inappropriate and excessive fear or anxiety concerning separation from attachment figures, with worry about harm to attachment figures or events causing separation, reluctance to leave home or sleep alone, nightmares about separation, and physical symptoms when separation occurs or is anticipated. Impairment is required; duration thresholds differ by age in standard teaching (commonly at least four weeks in children/adolescents).[12][13]
Social anxiety disorder. Marked fear of social situations in which the youth may be scrutinised; fear of negative evaluation; avoidance or endurance with intense distress; out of proportion to actual threat; persistent (typically six months or more in standard criteria teaching).[5][12]
Generalised anxiety disorder (GAD). Excessive anxiety and worry about multiple domains (school performance, family, health, future), difficult to control, with associated symptoms (restlessness, fatigue, concentration difficulty, irritability, muscle tension, sleep disturbance) and impairment. Paediatric GAD often presents with somatic complaints and perfectionistic academic worry.[25]
Selective mutism. Consistent failure to speak in specific social situations (often school) despite speaking in others (usually home), not explained by lack of knowledge of the language, lasting at least one month (not limited to the first month of school), and interfering with educational or social communication.[5][12]
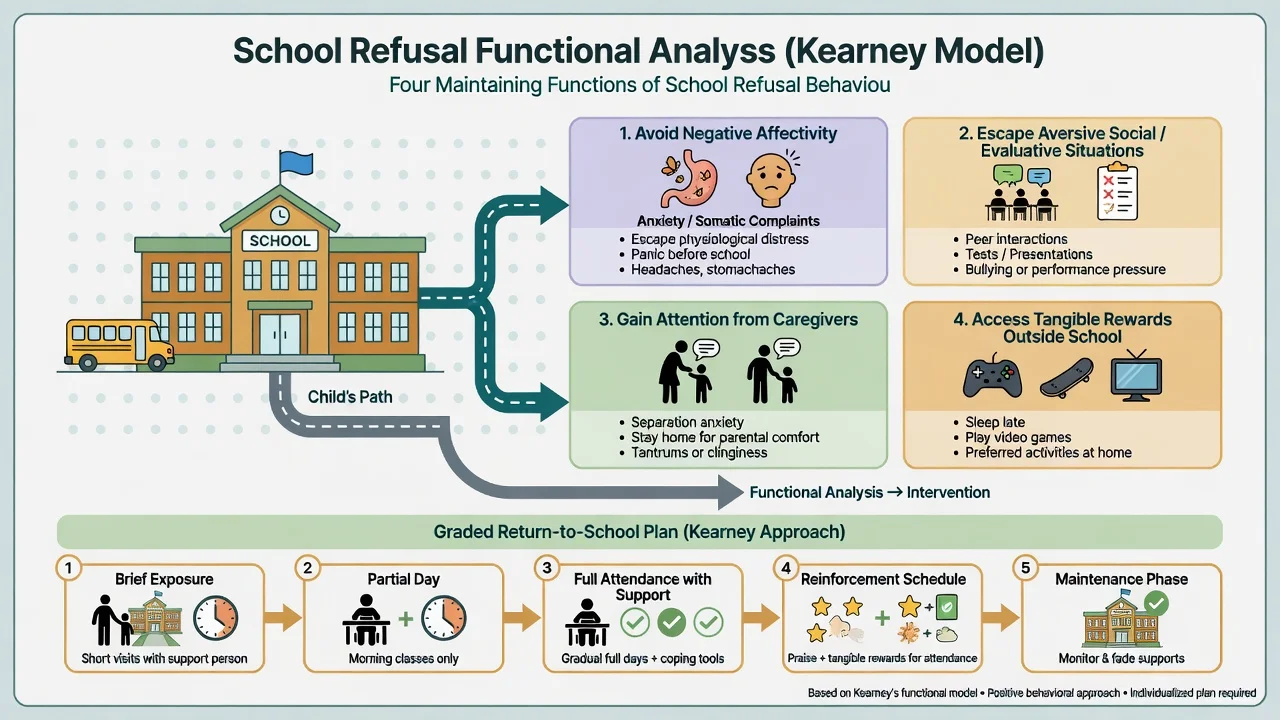
School refusal is not a DSM diagnosis. It is a presentation of non-attendance driven by anxiety, mood, oppositionality, family factors, or mixed functions. Kearney’s functional model distinguishes avoidance of negative affectivity, escape from aversive social/evaluative situations, attention-seeking, and tangible reinforcement outside school.[17][18]
ICD-11 uses closely related anxiety disorder constructs across the lifespan; state which manual you are applying when duration language is probed. Separation anxiety is recognised across ages — adult separation anxiety is examinable via NCS-R data.[13]
Separation
- Fear of separation from attachment figures
- Somatic symptoms on school mornings
- Nightmares about separation
- Can persist into adulthood
Social anxiety
- Fear of scrutiny and negative evaluation
- Class presentations, peers, eating in public
- Blushing, trembling, avoidance
- Paroxetine RCT exists but SSRI choice needs tolerability judgement
GAD
- Worry across multiple domains
- Restlessness, tension, sleep, concentration
- Often somatic and perfectionistic
- Duloxetine has paediatric GAD RCT data
School refusal
- Behaviour not diagnosis
- Functional analysis essential
- Graded return-to-school plan
- Link to separation, social, GAD, depression, bullying
Epidemiology and risk factors
Epidemiology headlines (exam order of magnitude)
Developmental epidemiology shows anxiety disorders are among the earliest-onset and most prevalent mental disorders in children and adolescents, with continuity risk into adult anxiety and mood disorders.[12][23] Separation anxiety has meaningful childhood prevalence and adult correlates in NCS-R analyses — do not treat it as “only a primary-school problem.”[13]
Common childhood psychiatric problems, including anxiety, are associated with poorer adult functional outcomes in prospective work — justifying early recognition and adequate treatment intensity.[14]
Risk factors examiners expect: behavioural inhibition temperament; parental anxiety and modelling of avoidance; adverse childhood experiences and bullying; chronic medical illness; learning difficulties; ASD and ADHD comorbidity; family accommodation that short-circuits exposure. Protective factors include warm consistent parenting that supports approach behaviour, school connectedness, and timely access to exposure-based care.[12][23]
Pathophysiology
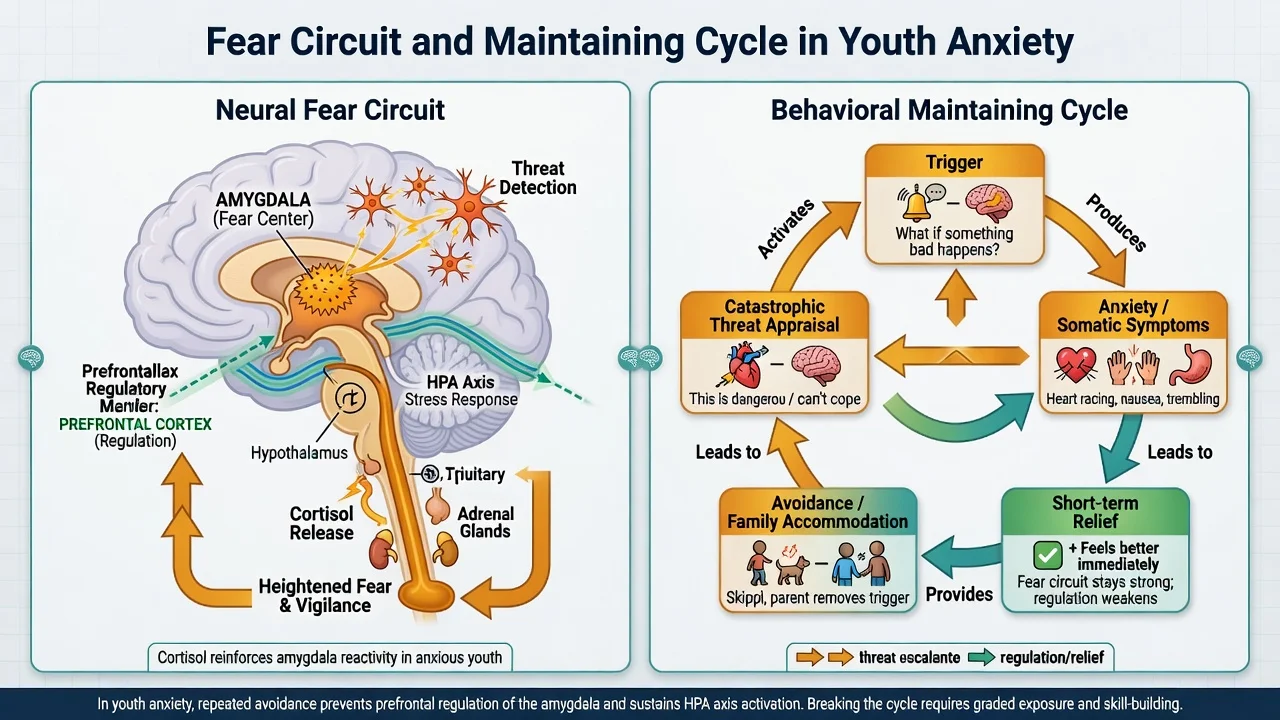
Neurodevelopmental framing. Threat detection involves amygdala-centred circuitry with prefrontal regulatory control that is still maturing in childhood and adolescence. Stress-system (HPA) activation links to somatic anxiety symptoms. Behavioural inhibition is a robust temperamental risk phenotype for later social anxiety and related disorders.[12][23]
Cognitive-behavioural maintaining mechanisms. Catastrophic threat appraisal, intolerance of uncertainty (especially GAD), fear of negative evaluation (social anxiety), safety behaviours, and avoidance maintain disorder via negative reinforcement. Family accommodation (parents answering for the child, allowing school non-attendance without a graded plan, excessive reassurance) is a high-yield maintaining factor in CAP formulations.[4][5]
Clinical presentation
Separation anxiety. Clinginess, distress at school drop-off, refusal to sleep alone, repeated reassurance-seeking about parents’ safety, abdominal pain or nausea on weekday mornings that improves if allowed to stay home, and nightmares about separation.[12][13]
Social anxiety. Avoidance of class presentations, answering questions, eating in the canteen, parties, or phone calls; blushing, trembling, voice freezing; post-event rumination; academic under-performance despite ability.[5][15]
GAD. “What if” chains about grades, family health, world events; restlessness; muscle tension; insomnia; irritability; concentration complaints that mimic ADHD.[25]
Selective mutism. Speaks freely at home; silent or whispers only at school; may use gestures; often co-occurs with social anxiety traits.[5]
MSE language examples. Affect may be tense or restricted in the clinic yet animated with carers; thought content includes anticipated catastrophe; insight often partial (“I know it’s silly but I can’t stop”); behaviour may include whispering, sitting close to parent, or refusing eye contact. Parent–youth discrepancy is common — believe functional impairment from school data even if the youth minimises symptoms.[5][6]
Differential diagnosis
| Differential | Discriminators | Why it matters |
|---|---|---|
| ASD social communication differences | Developmental history, restricted interests, sensory profile | Social skills training alone will not replace exposure if social anxiety coexists |
| ADHD inattention | Onset and setting pattern; anxiety worsens focus under evaluation | Wrong first drug class if pure anxiety |
| Depression | Anhedonia, pervasive low mood, anergia | Comorbidity common; changes risk and SSRI framing |
| OCD | Obsessions/compulsions beyond worry themes | ERP targets differ |
| PTSD | Trauma link, re-experiencing, hyperarousal | Trauma-focused pathway |
| Hyperthyroidism / substance / caffeine | Autonomic signs, history, labs when indicated | Organic mimic of panic/GAD |
| ODD / conduct-driven truancy | Enjoys out-of-school activities without anxiety | Functional analysis prevents wrong family work |
| Psychosis prodrome | Odd beliefs, hallucinations, decline | Do not miss with “just social withdrawal” |
Clinical and bedside assessment
Interview the young person alone and with carers. Structure: onset and course; specific fears and avoidance map; somatic symptoms; sleep; school attendance calendar; bullying (including online); trauma; family psychiatric history; accommodation behaviours; substances; self-harm and suicide; developmental and neurodiversity history.[5][6]
School refusal assessment. Plot days missed; antecedents (Sunday night dread, particular subjects, peers); consequences (parent attention, gaming at home); medical presentations. Apply Kearney functional profiles rather than a single label.[17][18]
Scales (adjuncts, not diagnoses): SCARED, SCAS, RCADS, and clinician-rated severity tools used in trials (for example PARS concept in research settings). Use scores to track change.[5]
Risk and safeguarding. Anxiety does not protect against suicide — assess ideation, intent, plan, means, and prior self-harm, especially if depression coexists or an antidepressant is started.[11] Confidentiality limits must be explained when risk requires carer involvement. Capacity/Gillick-type principles are decision-specific; legal tools are jurisdiction-specific.[5]
Investigations
Targeted, not shotgun. Consider thyroid function and other medical tests when autonomic features, atypical course, or systemic red flags exist. Baseline physical review before medication (height, weight, blood pressure as indicated). ECG when history, dose, combination risk, or local protocol suggests cardiac screening. No routine brain imaging for uncomplicated anxiety disorders.[5][24]
Acute and crisis management
Acute panic: rule out medical emergency when indicated; calm low-stimulus environment; brief grounding and paced breathing as support, not as sole definitive therapy; plan rapid outpatient exposure-based care. Avoid default long-term benzodiazepines in youth for chronic anxiety — dependence, cognitive effects, and weak long-term evidence make them poor fellowship answers for maintenance treatment.[5][24]
Definitive management
Psychological therapy — exposure is the active ingredient
Cognitive behavioural therapy with graded exposure is the first-line psychological treatment for most children and adolescents with anxiety disorders. Cochrane review evidence supports CBT for youth anxiety disorders versus waitlist/controls; network meta-analysis work compares psychotherapy types and acceptability.[4][21]
Core components examiners want named: psychoeducation; emotion identification; cognitive restructuring of threat appraisals; fear hierarchy and graded exposure (in vivo preferred when safe); contingency management; relapse prevention; parent sessions to reduce accommodation and support exposures. Protocol families include Coping Cat–style child CBT used in CAMS.[1][4][5]
Comparative effectiveness meta-analysis supports both CBT and pharmacotherapy as effective options for childhood anxiety disorders, with combination strategies important in moderate–severe illness.[10]
Landmark pharmacotherapy evidence
| Trial / evidence | Population / design | Exam takeaway |
|---|---|---|
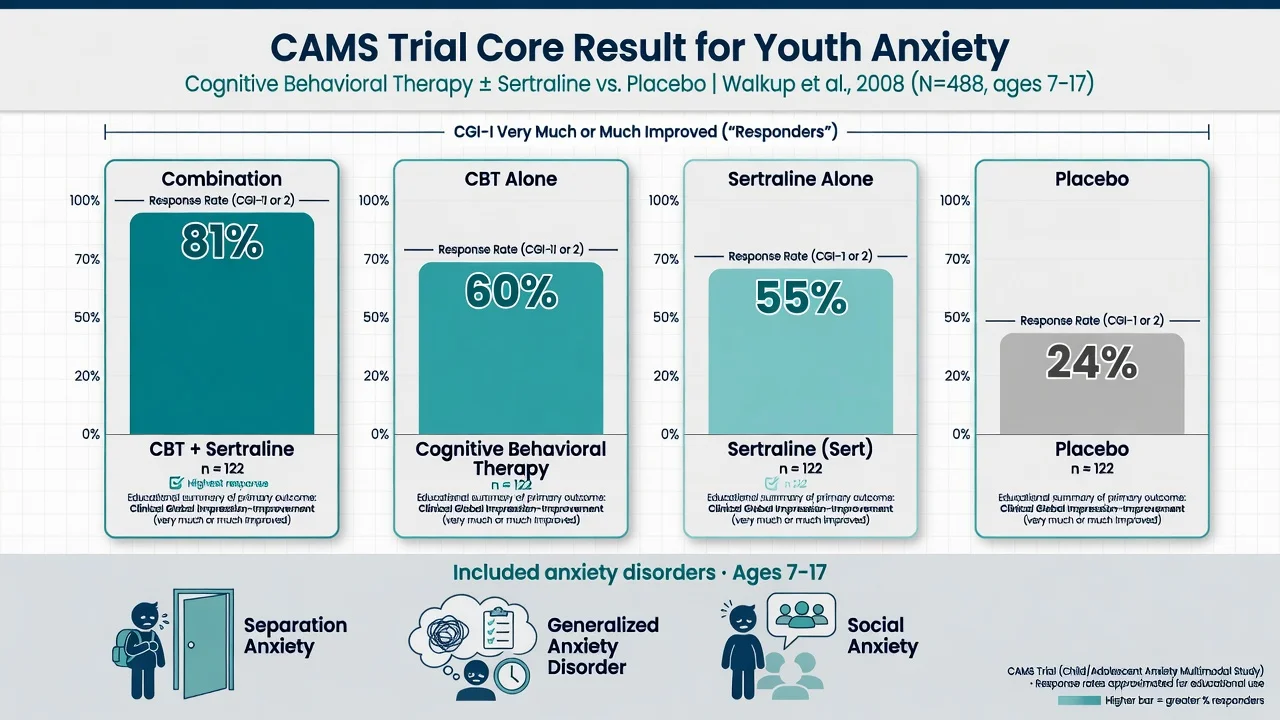
| CAMS Walkup 2008 | Ages 7–17; separation, GAD, social anxiety; CBT vs sertraline vs combo vs placebo | CGI-I much/very much improved approximately 81% combo, 60% CBT, 55% sertraline, 24% placebo |
| RUPP fluvoxamine 2001 | Youth anxiety (separation, social, GAD) | Fluvoxamine superior to placebo (classic ~76% vs ~29% response teaching) |
| Birmaher fluoxetine 2003 | Childhood anxiety disorders RCT | Fluoxetine efficacious vs placebo |
| Wagner paroxetine 2004 | Social anxiety disorder children/adolescents | Paroxetine superior to placebo; weigh tolerability/discontinuation profile in agent choice |
| Strawn duloxetine 2015 | Paediatric GAD | Duloxetine superior to placebo for GAD symptoms |
| CAMS safety Rynn 2015 | Safety analysis of CAMS | Structured adverse-effect and suicidality monitoring framing |
| CAMS remission Ginsburg 2011 | Remission after acute treatment | Remission rates lower than response — aim beyond “a bit better” |
| Long-term Ginsburg 2014 / CAMELS 2018 | Follow-up after CAMS | Relapse and residual symptoms common; maintenance and booster planning matter |
SSRI / SNRI practical prescribing (fellowship detail)
When medication is indicated (moderate–severe impairment, CBT unavailable/ineffective/refused, or combination planned), SSRIs are first-line for non-OCD youth anxiety in major practice guidelines.[5][6][24]
Sertraline (CAMS anchor). Start low (commonly 25 mg oral daily in children; some adolescents start 25–50 mg depending on size/sensitivity), titrate gradually according to response and tolerability toward an effective range; CAMS allowed flexible titration up to 200 mg oral daily. Monitor activation, GI effects, sleep change, headache, and suicidality/self-harm thoughts especially early and after dose increases.[1][22][24]
Fluoxetine. RCT support in childhood anxiety; typical start 10 mg oral daily, increase as needed (often toward 20 mg, higher only with specialist judgement and monitoring). Long half-life can help adherence and reduce discontinuation symptoms relative to shorter-acting agents.[3][24]
Fluvoxamine. RUPP evidence for paediatric anxiety; dose is age/weight guided with titration and CYP interaction awareness (theophylline, some other agents). Use when evidence familiarity and formulary support it.[2][24]
Paroxetine. Effective in adolescent/child social anxiety RCT, but many clinicians prefer other SSRIs first because of discontinuation syndrome risk and side-effect profile — state efficacy honestly and justify agent choice.[15][24]
Duloxetine (SNRI). Randomised placebo-controlled evidence in children and adolescents with GAD; consider when SSRI not suitable or specialist pathway supports SNRI use, with monitoring for side-effects including blood pressure as indicated.[16][24]
Duration. After response, continue for a period of stability (commonly taught as about 6–12 months of wellness before slow taper in uncomplicated cases), with individualisation for relapse history, residual symptoms, and psychosocial stressors. Do not stop abruptly.[5][24]
Black-box / suicidality counselling. Meta-analysis of paediatric antidepressant RCTs shows a small absolute increase in suicidal ideation/behaviour signals versus placebo while also showing clinical response benefits in treated groups — discuss risk–benefit openly, involve carers, and schedule early review rather than withhold indicated treatment from fear alone.[11]
School refusal treatment
Controlled evaluations support CBT for school-refusing children, and trials evaluate child therapy plus caregiver training components. Adolescent-sensitive CBT adaptations exist for school refusal with anxiety.[19][20]
Practical plan: same-week school liaison; medical clearance only when red flags exist (avoid indefinite medical certificates that entrench avoidance); graded exposure to school steps; escort plans; reduce tangible rewards for staying home; treat the underlying anxiety disorder with CBT and/or SSRI as indicated; address bullying and learning needs.[17][18][19]
Family work
Psychoeducation externalises anxiety as a treatable pattern. Train carers to limit excessive reassurance, support planned exposures, and avoid punitive framing. Parent-led and guided CBT models expand access for milder presentations within stepped care.[4][5]
Subtypes and scenarios
Preschool anxiety. Heavier parent guidance and play-based exposure; medication threshold higher and specialist.[5]
Selective mutism. Stimulus fading, shaping speech, contingency management, and treat co-occurring social anxiety; do not force public performance as humiliation.[5]
Anxiety + ASD. Adapt CBT (visual structure, concrete language, sensory load); social communication interventions alone are insufficient if phobic avoidance dominates.[5]
Anxiety + ADHD. Sequence or combine treatments; untreated ADHD can block CBT homework engagement.[5]
Cultural and ANZ context. Explore idioms of distress, family hierarchy, and school engagement barriers; Indigenous cultural safety and interpreter use where needed — avoid one script for all families.[5]
Complications and pitfalls
Pitfalls that fail vivas: calling school refusal a diagnosis; pure reassurance without exposure; benzodiazepines as chronic youth therapy; starting SSRI without monitoring plan; missing depression/suicide risk; colluding with permanent avoidance; ignoring bullying or learning disorders; assuming “shyness” needs no treatment when impairment is clear.[5][11][17]
Prognosis and disposition
Acute response can be excellent, especially with combination treatment in CAMS-level illness, but remission is harder than response and long-term residual anxiety or relapse is common in naturalistic and CAMELS follow-up — plan maintenance, booster CBT sessions, and school supports.[7][8][9]
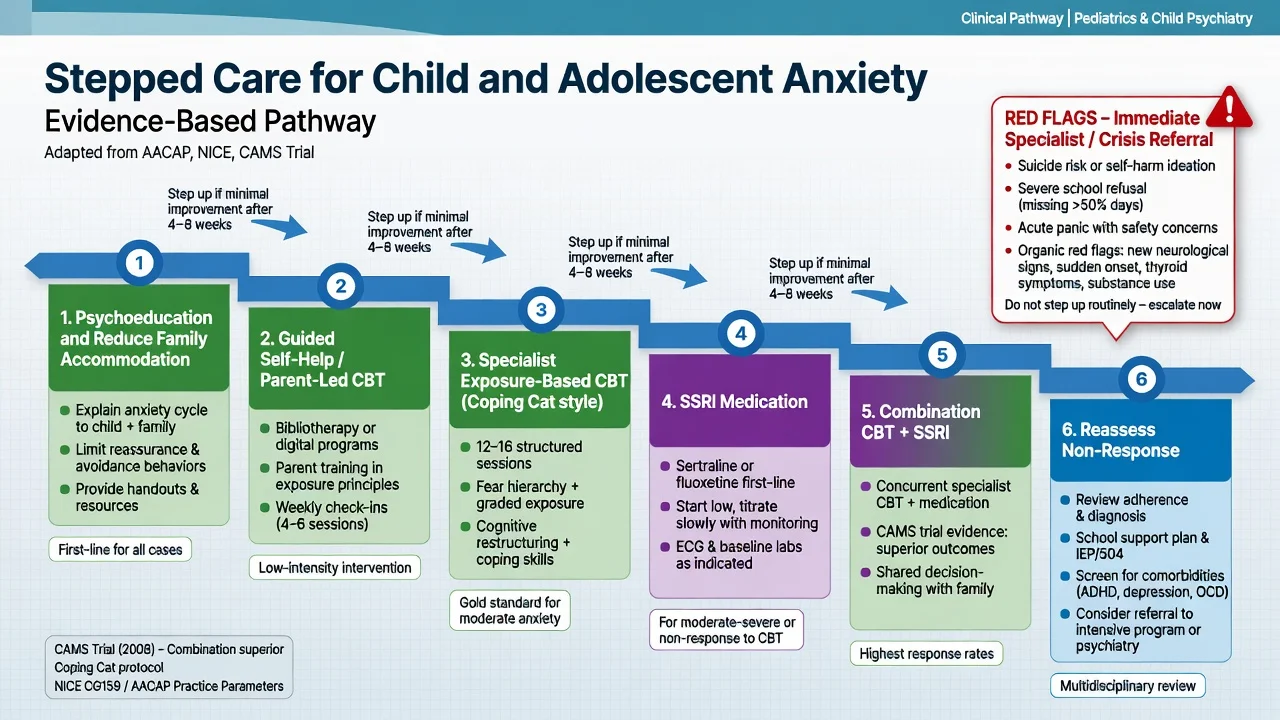
Stepped care disposition: guided self-help/parent-led CBT for mild → specialist CBT for moderate → SSRI or combination for moderate–severe or non-response → intensive community/day programs for entrenched avoidance and school refusal. Transition planning matters for older adolescents with chronic course.[5][10]
Special populations
Neurodevelopmental disorders, intellectual disability (simplified exposure hierarchies), LGBTQ+ minority stress, refugee trauma backgrounds, and medically ill youth require adapted formulation without abandoning exposure principles.[5][12]
Evidence, guidelines and regional differences
US (AACAP). Walter et al. 2020 clinical practice guideline for assessment and treatment of children and adolescents with anxiety disorders; earlier Connolly 2007 practice parameter remains historically cited.[5][6]
UK. NICE anxiety pathway principles: stepped care, CBT-informed interventions for children and young people, careful medication use with monitoring — map to local CAMHS tiers rather than inventing section numbers. CBT systematic review evidence and AACAP guidance inform the same stepped logic internationally.[4][5]
ANZ. FRANZCP-aligned CAP practice uses the same CBT-first psychological logic and SSRI pharmacotherapy evidence base (CAMS/RUPP/fluoxetine), delivered through public CAMHS, private specialists, and school liaison. Cite AACAP/NICE evidence plus local medication and consent frameworks.[1][5]
Landmark names for viva: CAMS (Walkup 2008); RUPP fluvoxamine (2001); Birmaher fluoxetine (2003); Wagner paroxetine social anxiety (2004); Strawn duloxetine GAD (2015); James Cochrane CBT (2020); Wang comparative effectiveness (2017); Ginsburg remission/follow-up/CAMELS.[1][2][3][4][8][10][15][16]
Exam pearls
Youth anxiety treatment stack
- CAMS response order: combo greater than CBT approximately equal to sertraline, both much greater than placebo.[1]
- School refusal = behaviour; use Kearney functions.[17][18]
- Separation anxiety is not only for young children — adult form exists in epidemiological data.[13]
- Always counsel activation and suicidality monitoring with youth antidepressants.[11][22]
- Exposure without reducing family accommodation often fails.[4][5]
References
- [1]Walkup JT, Albano AM, Piacentini J, Birmaher B, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety N Engl J Med, 2008.PMID 18974308
- [2]Research Unit on Pediatric Psychopharmacology Anxiety Study Group. Fluvoxamine for the treatment of anxiety disorders in children and adolescents N Engl J Med, 2001.PMID 11323729
- [3]Birmaher B, Axelson DA, Monk K, Kalas C, et al. Fluoxetine for the treatment of childhood anxiety disorders J Am Acad Child Adolesc Psychiatry, 2003.PMID 12649628
- [4]James AC, Reardon T, Soler A, James G, Creswell C. Cognitive behavioural therapy for anxiety disorders in children and adolescents Cochrane Database Syst Rev, 2020.PMID 33196111
- [5]Walter HJ, Bukstein OG, Abright AR, Keable H, Ramtekkar U, et al. Clinical Practice Guideline for the Assessment and Treatment of Children and Adolescents With Anxiety Disorders J Am Acad Child Adolesc Psychiatry, 2020.PMID 32439401
- [6]Connolly SD, Bernstein GA, Work Group on Quality Issues. Practice parameter for the assessment and treatment of children and adolescents with anxiety disorders J Am Acad Child Adolesc Psychiatry, 2007.PMID 17242630
- [7]Ginsburg GS, Becker EM, Keeton CP, Sakolsky D, et al. Naturalistic follow-up of youths treated for pediatric anxiety disorders JAMA Psychiatry, 2014.PMID 24477837
- [8]Ginsburg GS, Becker-Haimes EM, Keeton C, Kendall PC, et al. Results From the Child/Adolescent Anxiety Multimodal Extended Long-Term Study (CAMELS): Primary Anxiety Outcomes J Am Acad Child Adolesc Psychiatry, 2018.PMID 29960692
- [9]Ginsburg GS, Kendall PC, Sakolsky D, Compton SN, et al. Remission after acute treatment in children and adolescents with anxiety disorders: findings from the CAMS J Consult Clin Psychol, 2011.PMID 22122292
- [10]Wang Z, Whiteside SPH, Sim L, Farah W, et al. Comparative Effectiveness and Safety of Cognitive Behavioral Therapy and Pharmacotherapy for Childhood Anxiety Disorders: A Systematic Review and Meta-analysis JAMA Pediatr, 2017.PMID 28859190
- [11]Bridge JA, Iyengar S, Salary CB, Barbe RP, et al. Clinical response and risk for reported suicidal ideation and suicide attempts in pediatric antidepressant treatment: a meta-analysis of randomized controlled trials JAMA, 2007.PMID 17440145
- [12]Beesdo K, Knappe S, Pine DS. Anxiety and anxiety disorders in children and adolescents: developmental issues and implications for DSM-V Psychiatr Clin North Am, 2009.PMID 19716988
- [13]Shear K, Jin R, Ruscio AM, Walters EE, Kessler RC. Prevalence and correlates of estimated DSM-IV child and adult separation anxiety disorder in the National Comorbidity Survey Replication Am J Psychiatry, 2006.PMID 16741209
- [14]Copeland WE, Wolke D, Shanahan L, Costello EJ. Adult Functional Outcomes of Common Childhood Psychiatric Problems: A Prospective, Longitudinal Study JAMA Psychiatry, 2015.PMID 26176785
- [15]Wagner KD, Berard R, Stein MB, Wetherhold E, et al. A multicenter, randomized, double-blind, placebo-controlled trial of paroxetine in children and adolescents with social anxiety disorder Arch Gen Psychiatry, 2004.PMID 15520363
- [16]Strawn JR, Prakash A, Zhang Q, Pangallo BA, et al. A randomized, placebo-controlled study of duloxetine for the treatment of children and adolescents with generalized anxiety disorder J Am Acad Child Adolesc Psychiatry, 2015.PMID 25791145
- [17]Kearney CA, Albano AM. The functional profiles of school refusal behavior. Diagnostic aspects Behav Modif, 2004.PMID 14710711
- [18]Kearney CA. Forms and functions of school refusal behavior in youth: an empirical analysis of absenteeism severity J Child Psychol Psychiatry, 2007.PMID 17244270
- [19]King NJ, Tonge BJ, Heyne D, Pritchard M, et al. Cognitive-behavioral treatment of school-refusing children: a controlled evaluation J Am Acad Child Adolesc Psychiatry, 1998.PMID 9549960
- [20]Heyne D, King NJ, Tonge BJ, Rollings S, et al. Evaluation of child therapy and caregiver training in the treatment of school refusal J Am Acad Child Adolesc Psychiatry, 2002.PMID 12049443
- [21]Zhou X, Zhang Y, Furukawa TA, Cuijpers P, et al. Different Types and Acceptability of Psychotherapies for Acute Anxiety Disorders in Children and Adolescents: A Network Meta-analysis JAMA Psychiatry, 2019.PMID 30383099
- [22]Rynn MA, Walkup JT, Compton SN, Sakolsky DJ, et al. Child/Adolescent anxiety multimodal study: evaluating safety J Am Acad Child Adolesc Psychiatry, 2015.PMID 25721183
- [23]Pine DS, Fox NA. Childhood antecedents and risk for adult mental disorders Annu Rev Psychol, 2015.PMID 25559116
- [24]Nicotra CM, Strawn JR. Advances in Pharmacotherapy for Pediatric Anxiety Disorders Child Adolesc Psychiatr Clin N Am, 2023.PMID 37201968
- [25]Keeton CP, Kolos AC, Walkup JT. Pediatric generalized anxiety disorder: epidemiology, diagnosis, and management Paediatr Drugs, 2009.PMID 19445546