Psych · Child and adolescent psychiatry — depression
Child and adolescent depression
Also known as Adolescent depression · Paediatric major depression · Youth MDD · Childhood depression · CAMHS depression · Teen depression fluoxetine · TADS depression · Juvenile unipolar depression
Exam-exhaustive fellowship reference on child and adolescent depression — DSM-5-TR/ICD-11 developmental criteria (irritable mood), epidemiology, multi-informant assessment with private youth interview plus family and school, suicide and self-harm risk, organic and bipolar differentials, stepped care, fluoxetine dosing and activation monitoring, CBT/IPT-A/family work, TADS ADAPT TORDIA IMPACT evidence, GLAD-PC/NICE/RANZCP/AACAP framing, Gillick competence and disposition. Distinct from adult major-depressive-disorder and youth-self-harm-and-suicide topics. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Youth depression is high-yield for FRANZCP CAP and generalist interfaces, MRCPsych CASC, ABPN, and MD/DNB viva. Examiners test developmental criteria, risk, family/school systems, SSRI black-box communication, and landmark trial names — not a diluted adult MDD chapter.[6][12][18]
This topic is related to but distinct from adult major-depressive-disorder (STAR*D, adult dosing, ECT-heavy pathways) and youth-self-harm-and-suicide (full NSSI continuum and safety planning depth). Here the centre of gravity is depressive syndrome diagnosis and treatment in under-18s, integrating risk without replacing the dedicated self-harm topic.[12][21]
Definition and classification
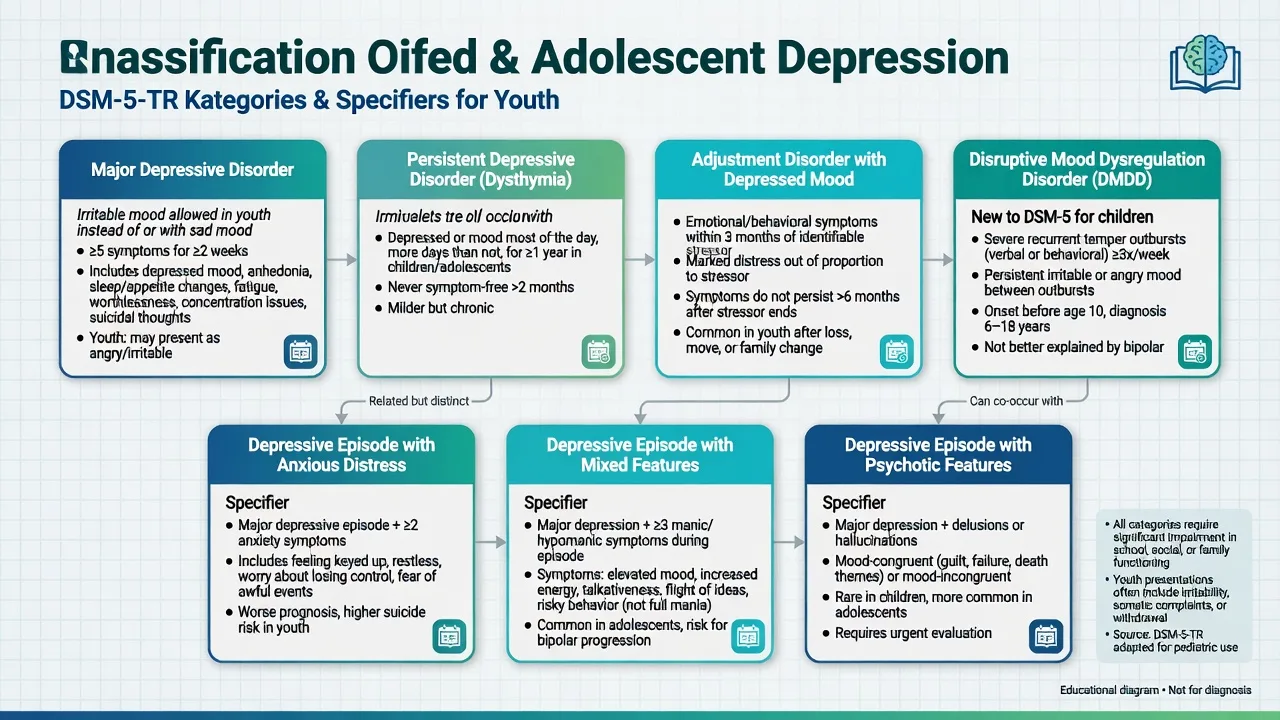
In DSM-5-TR, a major depressive episode requires five or more Criterion A symptoms during the same 2-week period, representing a change from previous functioning, with at least one of depressed mood or anhedonia, plus distress/impairment and exclusions (not better explained by another disorder; not attributable solely to substances/medical condition; not better explained by schizophrenia-spectrum illness). In children and adolescents, irritable mood may substitute for depressed mood as the mood criterion — a classic exam pearl.[6][18]
ICD-11 uses depressive episode/disorder constructs with severity and course modifiers; state which manual you are applying when duration language is probed.[12]
| Construct | Exam discriminators |
|---|---|
| MDD / major depressive episode | Threshold symptom count + 2 weeks + impairment; irritable mood allowed in youth |
| Persistent depressive disorder | Longer chronicity (developmental thresholds differ from adult 2-year teaching — check manual in use) |
| Adjustment disorder with depressed mood | Stressor-linked; does not meet full MDD threshold/duration |
| DMDD | Chronic severe irritability and temper outbursts; not interchangeable with episodic MDD |
| Depressive episode with mixed features | Manic/hypomanic symptoms short of full mania — bipolar risk pathway |
| Psychotic features | Mood-congruent or incongruent delusions/hallucinations — intensity escalates |
Epidemiology and risk
Community surveys such as the NCS-A analyses show major depression is common in adolescence, with substantial unmet treatment need and female predominance after puberty; pre-pubertal depression is less common and more equal by sex in classic teaching.[19][18]
Epidemiology headlines (order of magnitude)
Risk factors examiners expect: first-degree family history of depression or bipolar disorder, prior episode, anxiety disorders, ADHD, trauma/ACE, bullying (including online), LGBTQ+ minority stress and family rejection, chronic medical illness, sleep disruption, substance use, parental mental illness, and academic or peer failure.[18][19][21]
Protective factors: family connectedness, school belonging, help-seeking skills, supportive peers, and effective treatment access. Depression is a major driver of youth suicide risk; hospital-treated self-harm remains a serious long-term risk marker (see dedicated youth self-harm topic for full pathway).[15][21]
Pathophysiology and maintaining mechanisms
Viva-depth models (none is a diagnostic test) integrate developmental stress–diathesis with psychological maintaining cycles.[18]
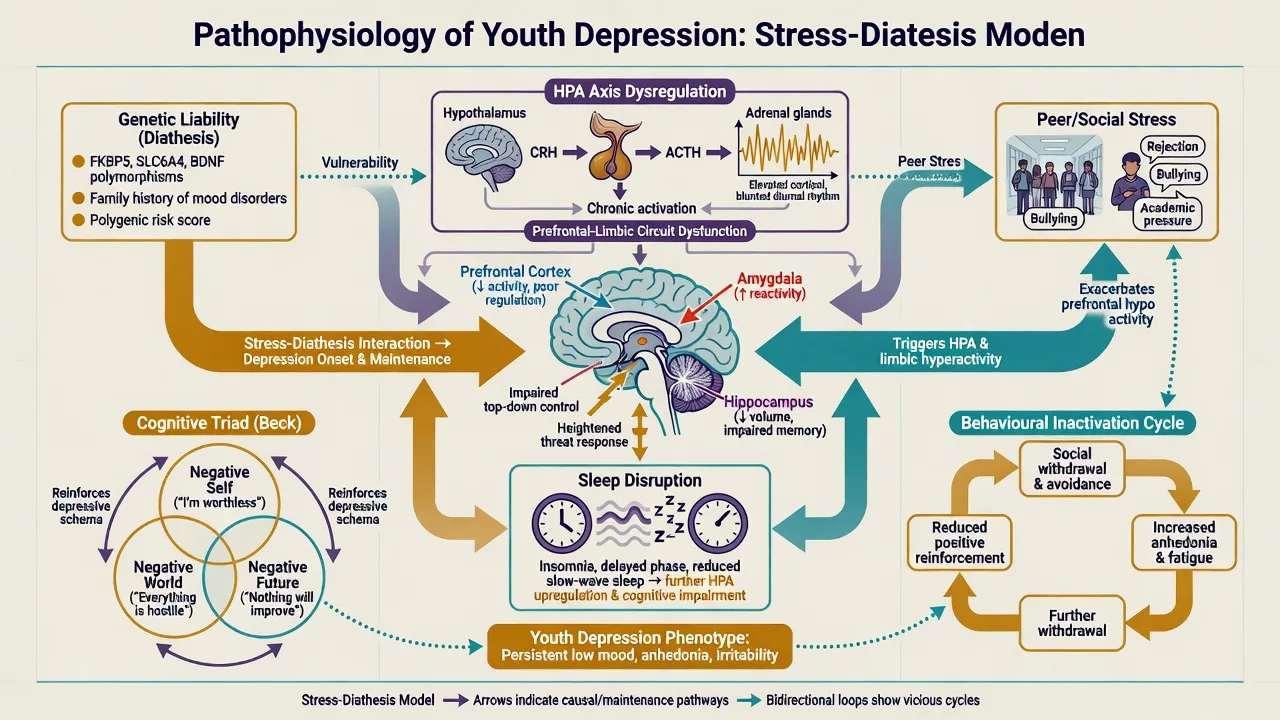
- Stress–diathesis and genetics: polygenic liability plus acute interpersonal stress (break-ups, bullying, family conflict).[18]
- Neurobiology: monoamine, HPA-axis, and prefrontal–limbic regulation models; adolescent reward/peer sensitivity and sleep/circadian disruption amplify vulnerability.[18]
- Cognitive–behavioural: hopelessness, negative triad, rumination, and behavioural inactivation maintain low mood and withdrawal from mastery/pleasure activities.[16][20]
- Interpersonal: role transitions, grief, interpersonal disputes, and skill deficits — IPT-A targets.[6][11]
High placebo response rates in youth antidepressant trials and developmental pharmacokinetics partly explain why drug–placebo differences can look smaller than adult STAR*D-era expectations — another exam-ready nuance.[17]
Clinical presentation
Core features. Low or irritable mood, anhedonia, fatigue, sleep change (hypersomnia or insomnia), appetite/weight change or failure to make expected weight gains, impaired concentration, guilt/worthlessness, psychomotor change, and suicidal ideation. Developmental colouring: boredom, school refusal, falling grades, somatic complaints (headache, abdominal pain), social media withdrawal or conflict, and irritability that carers describe as "attitude".[6][18]
MSE. Document affect range, thought content (guilt, hopelessness, suicidal ideation/plan), cognition, insight, engagement with examiner versus carers, and any psychotic phenomena. Ambivalence about dying is common — do not equate "no active plan today" with zero risk without a full formulation.[14][21]
Comorbidity is the rule in clinic samples: anxiety disorders, ADHD, oppositional behaviours, substance use, eating disorders, and autism spectrum conditions frequently co-travel and change treatment design.[18][19]
Differential diagnosis
| Differential | Discriminators | Why it matters |
|---|---|---|
| Bipolar depression / mixed features | Prior elevated/irritable periods with reduced sleep need, grandiosity, risky acts; strong bipolar FH | Antidepressant monotherapy risk |
| Adjustment disorder | Clear stressor; subthreshold symptom count/duration | Avoid medicalising normal distress — but do not miss MDD |
| DMDD | Chronic severe irritability and outbursts vs discrete depressive episodes | Different longitudinal pathway |
| Substance-induced | Timeline with cannabis, alcohol, stimulants | Dual formulation; toxicology |
| Medical/organic | TSH, anaemia, sleep apnoea, neuro red flags, pregnancy | Missed medical disease harms |
| Grief / trauma disorders | Predominant trauma re-experiencing or grief themes | Therapy target shifts |
| ASD camouflage burnout | Developmental history; sensory load; less classic anhedonia narrative | Adapt communication |
| Primary anxiety with demoralisation | Anxiety primary chronology | Anxiety-first pathway may still need mood treatment |
Always screen for bipolarity before starting an antidepressant and keep the possibility open if activation with elevated mood, decreased need for sleep, or grandiosity appears.[6][12]
Assessment
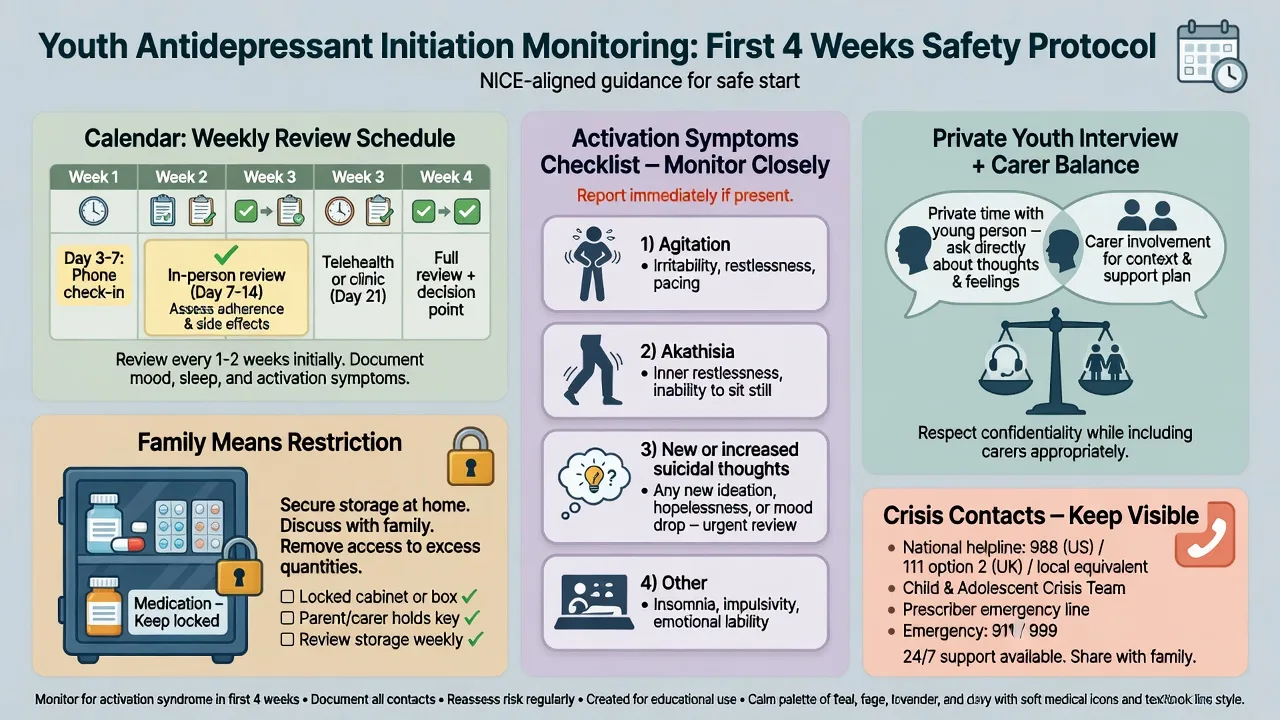
Multi-informant structure. See the young person alone and with carers. Private interview is mandatory for risk, substances, sexual health, online life, and bullying. Collateral from parents/carers and, with consent/appropriate authority, school. Developmental, trauma/safeguarding, and substance histories are core, not optional extras.[6][10]
Risk assessment. Expand passive death wishes into frequency, intent, plan, means access (medications, other means at home), prior attempts, NSSI functions, hopelessness, intoxication, and protective factors. Structured tools such as the C-SSRS support consistency; they do not replace clinical formulation. No-suicide contracts are not a safety plan. Co-create a written safety plan with carers for means restriction and crisis contacts.[14][15][21]
Competence and confidentiality. Apply Gillick/developmental competence principles: assess understanding, voluntariness, and ability to weigh options. Explain confidentiality limits at the start. When risk is high, share necessary information with carers and services; statutes are jurisdiction-specific — name principles (least restrictive care, best interests, safeguarding duties) rather than inventing section numbers.[6][12]
Scales. PHQ-9 / PHQ-A for measurement-based care and severity bands conceptually; item 9 is a screen, not a complete risk assessment. Clinician-rated instruments (e.g. CDRS-R in research) and functional measures (school attendance, CGAS-style function) complement self-report.[10][13]
Investigations
No laboratory test diagnoses depression. Baseline physical review and targeted tests: TSH, FBC, U&E/LFT as indicated, pregnancy test when relevant, urine drug screen when substance use is plausible. ECG when cardiac symptoms/history, overdose risk with particular agents, or other clinical indication. Imaging/EEG/autoimmune work-up is for neurological red flags, atypical psychosis interface, or cognitive decline — not routine for classic MDD.[6][12]
Acute and emergency management
Manage medical complications of overdose first. For severe psychotic depression, catatonia, or life-threatening poor intake, escalate to senior/inpatient care; ECT is uncommon in adolescents but remains examinable for the most severe, treatment-resistant, or life-threatening depressive presentations under specialist protocols and consent frameworks.[6][12]
Definitive management — stepped care
Psychological and social interventions
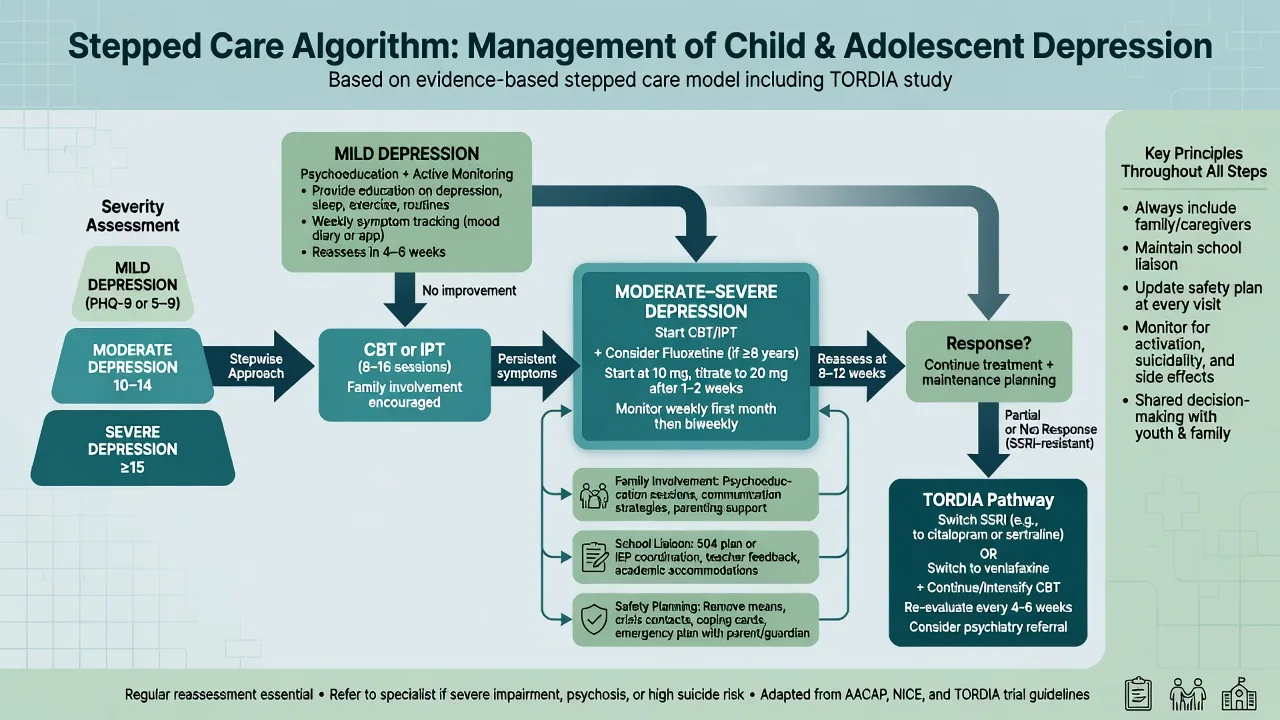
For mild depression, active monitoring, psychoeducation, sleep and activity scheduling, school liaison, and evidence-based psychological therapy (typically CBT or IPT-A) are first-line in major guidelines and primary-care pathways (GLAD-PC; NICE-style stepped care).[6][10][11]
CBT targets cognitive distortions, behavioural activation, problem-solving, and emotion regulation with age-adapted materials and parental sessions as needed. Family engagement is not optional ornamentation — conflict, expressed emotion, and supervision of means/meds are treatment targets. School: graded return, exam accommodations, bullying intervention, and attendance monitoring.[6][11][20]
Pharmacotherapy — fluoxetine first among SSRIs
When medication is indicated (typically moderate–severe depression, inadequate response to psychological care, or limited therapy access with significant impairment/risk), fluoxetine is the best-evidenced first-line antidepressant in children and adolescents.[1][7][17]
Example initiating regimen (fellowship viva style — individualise): fluoxetine 10 mg orally once daily for several days to 1 week if smaller/younger/activation-prone, then increase to 20 mg daily; many trial protocols centre on 20 mg, with selected adolescents titrated toward 40 mg under specialist review if partial response and good tolerability. Use liquid formulations when swallowing or fine titration is an issue. Review early (often within 1 week initially in higher-risk youth, then frequently through the first month) for activation, insomnia, agitation, akathisia, and suicidal thinking. Plan an adequate trial at a therapeutic dose (commonly 4–6 weeks at target) before declaring failure, assuming adherence.[1][7][11]
Monitoring and black-box communication. FDA meta-analytic work (Hammad et al.) found a small absolute increase in suicidal ideation/behaviour signals with antidepressants versus placebo in paediatric trials — not an increase in completed suicide in those short trials. Communicate relative and absolute risk honestly; the clinical implication is closer monitoring and safety planning, not reflexive refusal to treat moderate–severe depression.[5][11]
Other agents. After fluoxetine non-response, TORDIA supports switching to another antidepressant with CBT rather than medication switch alone; venlafaxine was studied in that resistant pathway but tolerability/suicidality signals require caution and specialist oversight. Avoid casual polypharmacy. TCAs are not first-line in youth for depression efficacy/safety balance.[4][17]
Duration. After remission, continue medication for a period informed by episode number and severity (often many months; individualise), then taper gradually with relapse surveillance. Emslie et al. showed fluoxetine continuation reduced relapse versus placebo after acute response in youth.[8][11]
Combination treatment
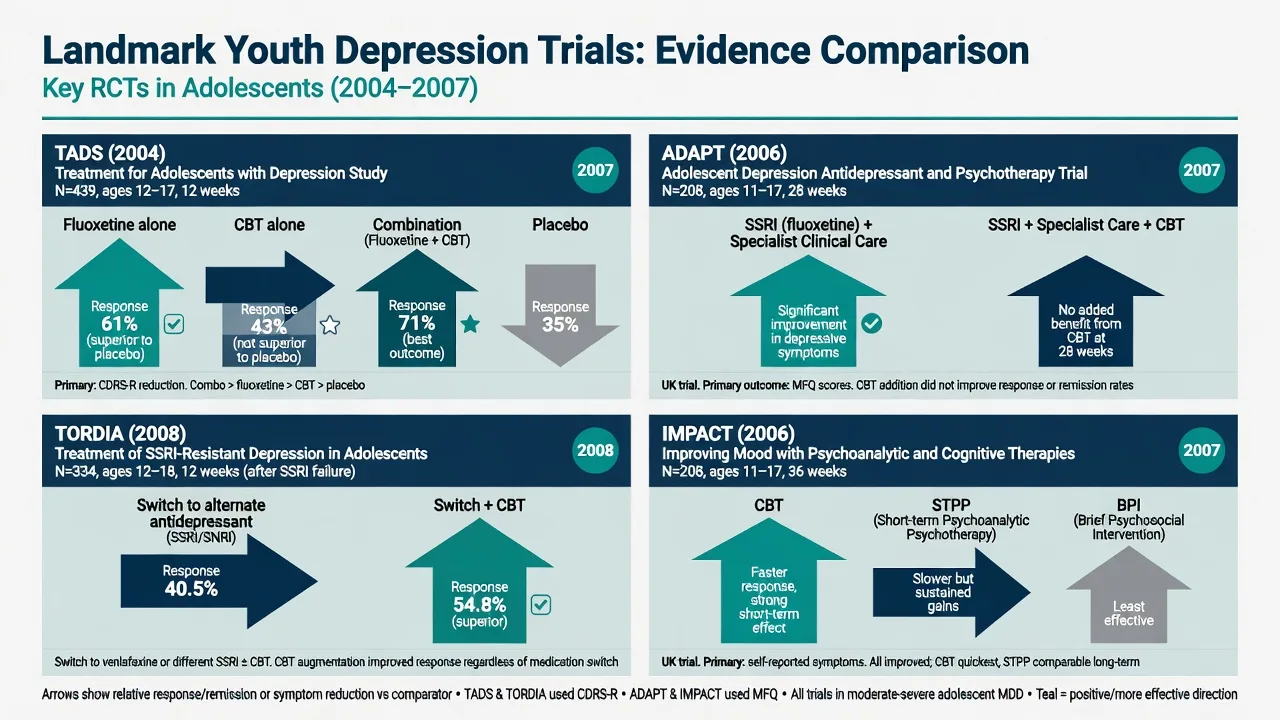
Psychological therapy plus fluoxetine is often preferred for moderate–severe illness when available — TADS acute results favour combination and fluoxetine over CBT alone and placebo on primary endpoints, with longer-term convergence as more youth receive active treatment over time.[1][2][20]
Landmark evidence (exam names)
| Trial | Design takeaway | Clinical pearl |
|---|---|---|
| TADS (March 2004; long-term 2007) | Fluoxetine, CBT, combination, placebo in adolescents | Acute: combo and fluoxetine outperformed CBT alone and placebo on primary outcomes; combination often preferred when feasible; residual symptoms remain common (Kennard) |
| ADAPT (Goodyer 2007) | SSRI + specialist care ± CBT | Adding CBT did not clearly improve primary outcomes beyond good specialist care + SSRI — classic trap against automatic "always add CBT package" slogans without resource context |
| TORDIA (Brent 2008) | SSRI-resistant adolescents: switch ± CBT | Switch + CBT superior to medication switch alone |
| IMPACT (Goodyer 2017) | CBT vs short-term psychoanalytic psychotherapy vs brief psychosocial intervention | Similar effectiveness framing — relationship and structure matter; not only one brand of therapy wins |
| Cipriani NMA 2016 | Antidepressants in children/adolescents | Fluoxetine had the most consistent efficacy/tolerability signal among many agents |
| Hammad 2006 | FDA paediatric antidepressant suicidality | Small absolute risk signal for suicidal ideation/behaviour — monitor; do not abandon indicated treatment |
| Emslie fluoxetine RCTs | Acute efficacy and relapse prevention | Underpins fluoxetine as first-line pharmacotherapy |
| GLAD-PC 2018 | Primary-care identification and treatment | Screening, stepped care, referral thresholds |
| RANZCP mood 2020 | Regional guideline frame | Formulation, risk, and youth-aware mood care principles |
TADS
- 4 arms including placebo
- Combo strongest acute signal
- Fluoxetine > CBT alone acutely
- Longer-term gains converge
ADAPT
- Specialist care + SSRI base
- CBT add-on null primary
- Real-world UK specialist context
- Cost analyses available
TORDIA
- SSRI-resistant youth
- Switch + CBT wins
- Venlafaxine in switch options
- Do not just re-trial same SSRI forever
IMPACT
- Three psychological arms
- No clear superior brand
- Pragmatic multicentre
- Formulation still essential
Subtypes and scenarios
- Mild outpatient: therapy, school plan, safety net; medication not automatic.[10][11]
- Moderate–severe with impairment: combine psychological care and consider fluoxetine early; higher review frequency.[1][11]
- SSRI-resistant: re-check diagnosis (bipolarity, substances, trauma, adherence), then TORDIA-style switch + CBT.[4]
- Comorbid ADHD/anxiety: treat the formulation; sequence carefully; stimulants do not replace depression care when MDD is syndromal.[6][18]
- Emerging bipolar risk: family history education, mood charting, low threshold to specialist mood clinic; avoid aggressive antidepressant stacking.[12]
Complications and pitfalls
Other traps: missed bipolarity; token 10-day half-dose "failed SSRI"; promising absolute confidentiality; ignoring school and family maintaining factors; treating PHQ item 9 as a full risk assessment; polypharmacy without reformulation.[6][13][12]
Prognosis and disposition
Many youth improve with appropriate care, but residual symptoms predict relapse — aim for remission and functional recovery (attendance, peer function, sleep), not mere "a bit better". Disposition ladder: GP/primary care with GLAD-PC-style support → community CAMHS → intensive community/day programmes → inpatient when risk or severity exceeds community containment. Plan transition to adult services for older adolescents with ongoing illness.[2][9][11]
Special populations
Pre-pubertal children have a thinner medication evidence base — family and school interventions dominate; specialist oversight for any pharmacotherapy. Autistic youth need adapted communication and careful separation of autistic shutdown from MDD. LGBTQ+ youth: assess minority stress and family acceptance explicitly. Cultural safety (including Indigenous ANZ contexts) is a FRANZCP expectation — use interpreters, explore explanatory models, and avoid pathologising culturally normative distress. Pregnant adolescents require dual maternal–fetal risk–benefit reasoning under perinatal frameworks.[6][12][18]
Regional guideline deltas
ANZ (RANZCP): formulation-centred mood care, risk assessment, and youth-aware principles within the 2020 mood disorder guidelines; local Mental Health Act processes are state/territory specific.[12]
UK: NICE-style stepped care for depression in children and young people; ADAPT and IMPACT are culturally familiar evidence anchors; CAMHS tier language varies by service redesign era.[3][16]
US: AACAP practice parameters/CPGs and GLAD-PC primary-care guidance; FDA black-box labelling shapes consent conversations; fluoxetine FDA-linked youth depression evidence is repeatedly examined.[6][10][11]
Exam pearls
[6] [18] [1] [3] [4] [1] [7] [17]Mnemonic for first appointment skeleton: RISK-SCHOOL — Risk (suicide/self-harm/safeguarding), Irritability/mood criteria, Substances and sleep, Kin/family function, School function, Collateral and competence, History of bipolar/mania screen, Organic red flags, Offer stepped plan, Liaise and safety-plan, Literature (TADS/ADAPT/TORDIA) ready for viva.[1][5][6]
Summary
Defend youth depression as a developmental multi-system illness: accurate criteria (including irritable mood), multi-informant assessment, relentless attention to suicide risk and family means restriction, CBT/IPT-A and school/family work, and fluoxetine with early monitoring when medication is indicated — sequenced with TADS, ADAPT, TORDIA, and IMPACT literacy rather than adult-only algorithms.[1][3][4][6][16][17]
References
- [1]March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial JAMA, 2004.PMID 15315995
- [2]March JS, Silva S, Petrycki S, et al. The Treatment for Adolescents With Depression Study (TADS): long-term effectiveness and safety outcomes Arch Gen Psychiatry, 2007.PMID 17909125
- [3]Goodyer I, Dubicka B, Wilkinson P, et al. Selective serotonin reuptake inhibitors (SSRIs) and routine specialist care with and without cognitive behaviour therapy in adolescents with major depression: randomised controlled trial BMJ, 2007.PMID 17556431
- [4]Brent D, Emslie G, Clarke G, et al. Switching to another SSRI or to venlafaxine with or without cognitive behavioral therapy for adolescents with SSRI-resistant depression: the TORDIA randomized controlled trial JAMA, 2008.PMID 18314433
- [5]Hammad TA, Laughren T, Racoosin J Suicidality in pediatric patients treated with antidepressant drugs Arch Gen Psychiatry, 2006.PMID 16520440
- [6]Birmaher B, Brent D, AACAP Work Group on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with depressive disorders J Am Acad Child Adolesc Psychiatry, 2007.PMID 18049300
- [7]Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine for acute treatment of depression in children and adolescents: a placebo-controlled, randomized clinical trial J Am Acad Child Adolesc Psychiatry, 2002.PMID 12364842
- [8]Emslie GJ, Heiligenstein JH, Hoog SL, et al. Fluoxetine treatment for prevention of relapse of depression in children and adolescents: a double-blind, placebo-controlled study J Am Acad Child Adolesc Psychiatry, 2004.PMID 15502599
- [9]Kennard B, Silva S, Vitiello B, et al. Remission and residual symptoms after short-term treatment in the Treatment of Adolescents with Depression Study (TADS) J Am Acad Child Adolesc Psychiatry, 2006.PMID 17135985
- [10]Zuckerbrot RA, Cheung A, Jensen PS, et al. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part I. Practice Preparation, Identification, Assessment, and Initial Management Pediatrics, 2018.PMID 29483200
- [11]Cheung AH, Zuckerbrot RA, Jensen PS, et al. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part II. Treatment and Ongoing Management Pediatrics, 2018.PMID 29483201
- [12]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [13]Kroenke K, Spitzer RL, Williams JB The PHQ-9: validity of a brief depression severity measure J Gen Intern Med, 2001.PMID 11556941
- [14]Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults Am J Psychiatry, 2011.PMID 22193671
- [15]Wilkinson P, Kelvin R, Roberts C, et al. Clinical and psychosocial predictors of suicide attempts and nonsuicidal self-injury in the Adolescent Depression Antidepressants and Psychotherapy Trial (ADAPT) Am J Psychiatry, 2011.PMID 21285141
- [16]Goodyer IM, Reynolds S, Barrett B, et al. Cognitive behavioural therapy and short-term psychoanalytical psychotherapy versus a brief psychosocial intervention in adolescents with unipolar major depressive disorder (IMPACT): a multicentre, pragmatic, observer-blind, randomised controlled superiority trial Lancet Psychiatry, 2017.PMID 27914903
- [17]Cipriani A, Zhou X, Del Giovane C, et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: a network meta-analysis Lancet, 2016.PMID 27289172
- [18]Thapar A, Collishaw S, Pine DS, Thapar AK Depression in adolescence Lancet, 2012.PMID 22305766
- [19]Avenevoli S, Swendsen J, He JP, et al. Major depression in the national comorbidity survey-adolescent supplement: prevalence, correlates, and treatment J Am Acad Child Adolesc Psychiatry, 2015.PMID 25524788
- [20]Cox GR, Callahan P, Churchill R, et al. Psychological therapies versus antidepressant medication, alone and in combination for depression in children and adolescents Cochrane Database Syst Rev, 2014.PMID 25433518
- [21]Cha CB, Franz PJ, M Guzmán E, et al. Annual Research Review: Suicide among youth - epidemiology, (potential) etiology, and treatment J Child Psychol Psychiatry, 2018.PMID 29090457
- [22]Loades ME, Midgley N, Herring GT, et al. In Context: Lessons About Adolescent Unipolar Depression From the Improving Mood With Psychoanalytic and Cognitive Therapies Trial J Am Acad Child Adolesc Psychiatry, 2024.PMID 37121393
- [23]Byford S, Barrett B, Roberts C, et al. Cost-effectiveness of selective serotonin reuptake inhibitors and routine specialist care with and without cognitive behavioural therapy in adolescents with major depression Br J Psychiatry, 2007.PMID 18055956
- [24]Domino ME, Foster EM, Vitiello B, et al. Relative cost-effectiveness of treatments for adolescent depression: 36-week results from the TADS randomized trial J Am Acad Child Adolesc Psychiatry, 2009.PMID 19465880