Psych · Child and adolescent psychiatry — risk and safeguarding
Child protection for psychiatrists
Also known as Child safeguarding · Child maltreatment response · Mandatory reporting child abuse · Parental capacity assessment · Multi-agency child protection · Fabricated or induced illness
Exam-exhaustive fellowship reference on child protection for psychiatrists — maltreatment subtypes, reporting thresholds, documentation, multi-agency working, parental capacity principles, fabricated/induced illness interface, trauma sequelae, and legal/exam principles without invented jurisdiction-specific section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Child protection is a high-yield CAP, CASC, and ethics interface topic. Examiners test whether you can name maltreatment subtypes, apply thresholds for report without requiring courtroom proof, document contemporaneously, share information proportionately, assess parental capacity as multi-dimensional rather than diagnostic labelling, and coordinate multi-agency responses while treating the child's mental health needs.[2][3][6]
Overview and definition
Major high-income-country reviews frame child maltreatment as acts of commission or omission by parents, caregivers, or others in positions of responsibility, power, or trust that result in actual or potential harm to a child's health, development, or dignity.[2][3]
Child protection is the statutory and multi-agency response when significant harm is occurring or is likely. It sits above universal prevention and targeted family support, and it is distinct from adult safeguarding. DSM-5-TR and ICD-11 do not replace clinical recognition with a single "child abuse disorder"; the exam task is recognition, threshold reasoning, documentation, multi-agency duty, and mental health care of child and family.[2][3]
Classification — subtypes
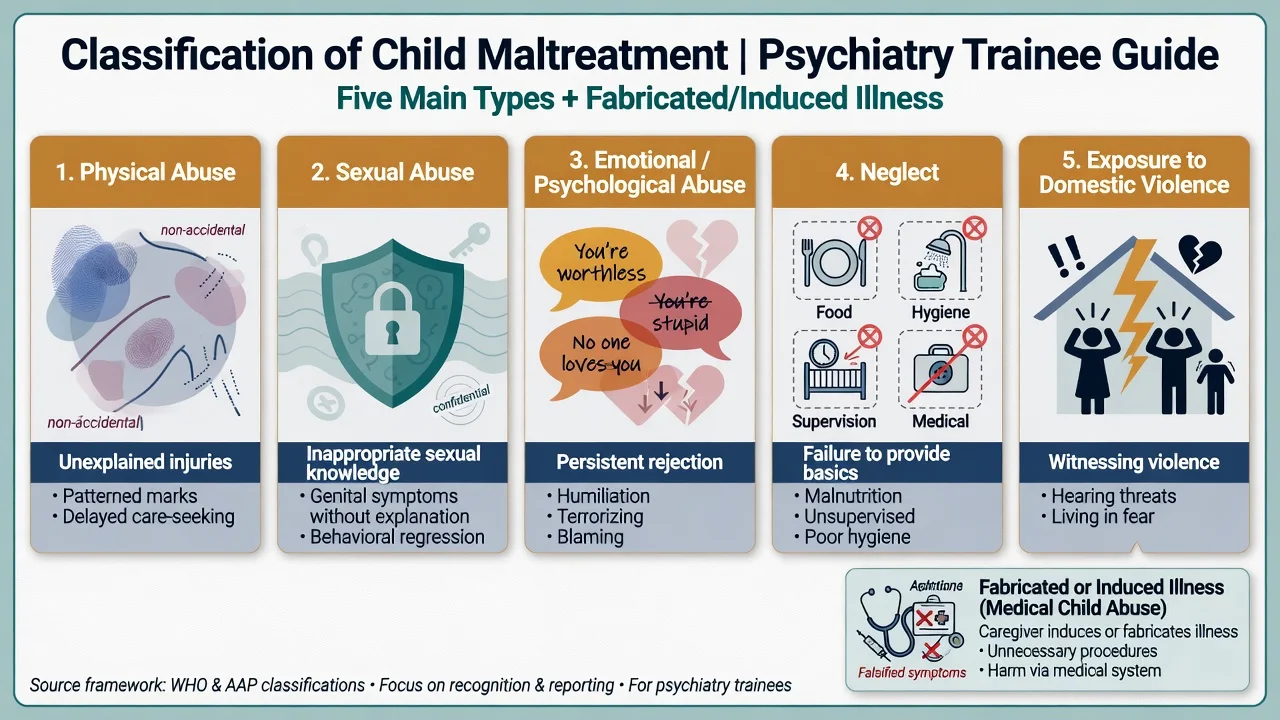
Physical
- Hitting, shaking, burning, poisoning, fabricated injury
- History inconsistent with developmental stage
- Delayed presentation; patterned injuries
Sexual
- Contact and non-contact sexual exploitation
- Often no genital findings
- Disclosure is primary evidence pathway
Emotional
- Persistent denigration, terrorising, isolation
- Corruption; developmentally damaging interactions
- May be invisible without careful history
Neglect
- Failure of basic care, supervision, medical/educational needs
- Emotional unavailability
- Chronic cumulative harm
IPV exposure
- Witnessing or being used in domestic violence
- Secondary trauma symptoms common
- Co-occurs with direct abuse/neglect
FII / medical child abuse
- Fabricated or induced symptoms
- Iatrogenic harm via unnecessary care
- Needs coordinated multi-agency strategy
Emotional abuse and neglect are conceptualised as persistent harmful caregiving interactions that damage the child's developmental potential — not a one-off harsh word.[16] Fabricated or induced illness (FII) (medical child abuse / former MSBP spectrum) involves caregiver fabrication or induction of symptoms leading to unnecessary harmful medical intervention; early recognition protects the child from iatrogenic harm.[15]
Epidemiology and risk
Gilbert and colleagues mapped the burden and consequences of maltreatment in high-income countries: common, often undetected, and linked to major lifelong morbidity.[2] A companion paper on recognising and responding emphasises systems failures and under-response by professionals.[3] Cross-country policy and trend analyses show large variation in official rates that more often reflects system design than true incidence differences alone.[6]
Long-term outcomes: Norman and colleagues' systematic review and meta-analysis demonstrated robust associations of child physical abuse, emotional abuse, and neglect with adult mental disorders, drug use, suicide attempts, and sexually transmitted infections, among other outcomes.[5] The ACE study showed graded relationships between childhood adversity and leading causes of adult morbidity and mortality; later meta-analysis and European/North American cost analyses extend the public-health case.[1][7][8][9]
Global meta-analysis of child sexual abuse prevalence demonstrates high rates with marked sex patterning and methodological heterogeneity — exams test order-of-magnitude awareness and under-disclosure, not a single universal percentage as dogma.[12]
Risk ecology: disability and chronic illness in the child; parental mental illness (especially untreated), substance use, IPV, young parental age, parental history of maltreatment, poverty, housing instability, isolation, and prior statutory involvement. Service risks include fragmented information and failure to interview the child.[2][3]
Mechanisms and psychiatric interface
There is no single neurotransmitter model. Useful frameworks are developmental psychopathology and toxic stress: disrupted attachment, threat-system sensitisation, HPA-axis dysregulation, and structural/functional neural correlates summarised in Teicher and Samson's annual research review.[10][9]
Childhood adversities are associated with increased risk of psychosis in meta-analytic work — a bridge examiners use between CAP trauma history and adult psychiatry formulation.[11] Emotional maltreatment frameworks emphasise persistent relational harm rather than discrete events alone.[16]
Clinical presentation
Presentations span ED, paediatrics, CAMHS clinics, adult services (when the parent is the identified patient), schools, and CASC stations.[2][3]
Interview red flags: caregiver monopolises the narrative; child is unusually silent or looks to adult before answering; histories change across agencies; injuries explained beyond developmental capability; repeated unexplained medical presentations; adolescent self-harm with undisclosed home violence; school reports of chronic hunger or unexplained absences.[3][13]
MSE and risk. Note fear, hypervigilance, dissociation, shame, aggression, sexualised behaviour out of developmental context, developmental delay, and suicidal ideation in older children. Reality-based fear of a caregiver is not a delusion.[2][20]
Differential diagnosis
Accident / medical mimic
- Falls, coagulopathy, bone disease, skin conditions
- Still document and escalate if unexplained
- Specialist paediatric assessment
True chronic illness vs FII
- Medically complex children can be both ill and abused
- Look for incongruent findings and caregiver dynamics
- Avoid unilateral confrontation
Primary psychiatric
- ADHD, ASD, mood, psychosis
- Trauma can mimic or coexist
- Avoid diagnostic overshadowing
Cultural context
- Explain discipline norms carefully
- Culture never excuses significant harm
- Independent interpreter
Physical abuse evaluation requires structured paediatric assessment; many medical differentials exist, but unexplained injury in a non-ambulant infant remains a critical pathway.[13] Sexual abuse evaluation is specialist and often finding-negative; disclosure still drives protection.[14] Cultural competence improves assessment quality but does not lower the harm threshold.[3]
Assessment and documentation
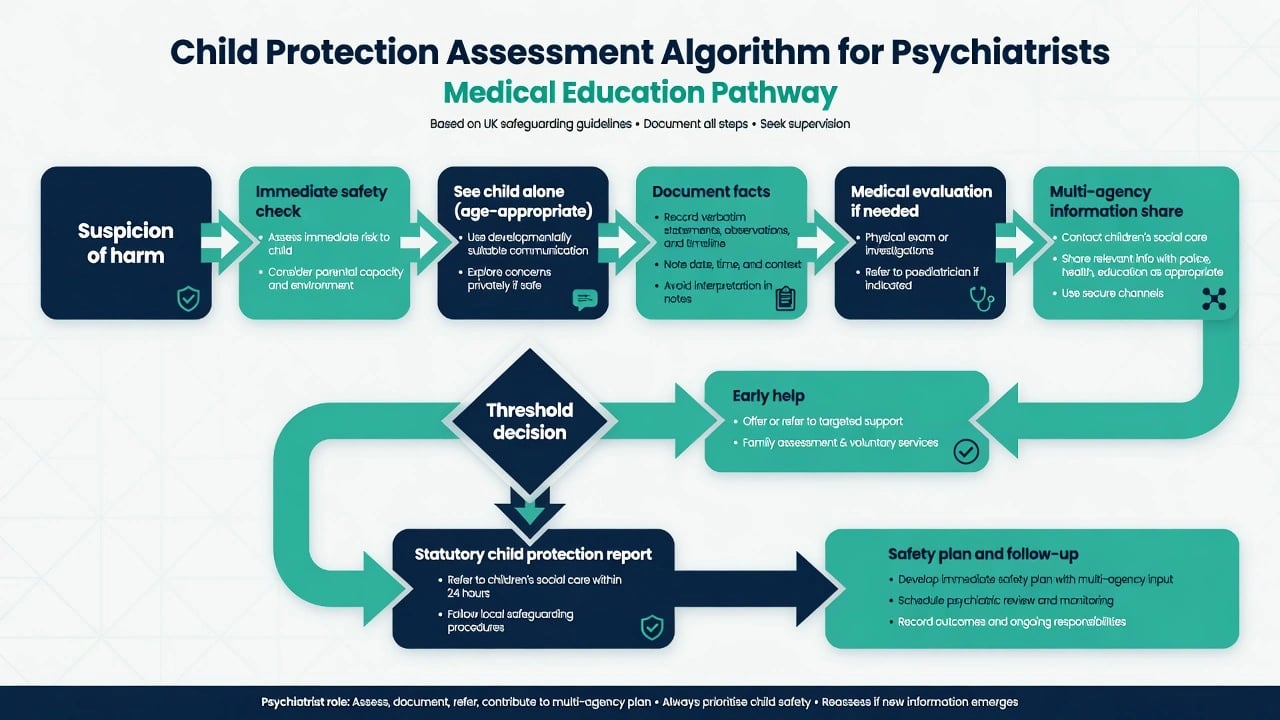
Core bedside rules when child protection concerns arise.[3][13]
- Immediate safety — can this child go home tonight? If no, escalate emergency protective pathways before perfect paperwork.[3]
- See the child alone when developmentally possible; independent interpreter — not a family member.[3]
- Ask openly, not leadingly — free narrative first; avoid coaching or serial interviews that contaminate forensic process.[3][14]
- Document contemporaneously — quotes, who was present, body descriptions of injuries, developmental observations, what was offered and refused. Separate fact, opinion, and plan.[3]
- Medical evaluation for suspected physical or sexual abuse via specialist pathways.[13][14]
- Multi-agency map — school, GP, midwifery, previous CAMHS, statutory services, police; check sibling risk.[3][6]
- Parental mental health and capacity dimensions (see next section) without equating diagnosis with automatic removal.[17]
- Adolescent risk — suicide/self-harm, substance use, exploitation, and mature-minor competence for their own treatment decisions (distinct from whether abuse must be reported).[17][20]
Thresholds for report and legal principles
Threshold language (principle-level, no invented sections): reporting and multi-agency duties are local, but the clinical principles below are examinable across boards.[3][6]
- Significant harm / risk of significant harm is the core statutory concept in many systems — ill-treatment or impairment of health or development compared with that reasonably expected of a similar child.[3]
- Mandatory reporting duties (who must report, what must be reported, to whom) are jurisdiction-specific. In viva, state: identify your local mandated-reporter status, report to the designated child-protection agency, document the basis, and prioritise safety. Do not invent section numbers.[3][6]
- Confidentiality has lawful limits when a child is at risk of serious harm. Share the minimum necessary information for protection, record the basis for sharing, and inform the young person/family when safe and appropriate.[3]
- Dual loyalty: when a parent is your patient, the child's welfare is paramount if protection thresholds are met. Treat the parent, but do not collude with minimisation.[3][17]
- Sibling risk after disclosure is mandatory to consider — one child's report may unmask household risk.[3][14]
Frame answers around state/territory mandatory reporting schemes, child protection departments, health-service child-protection units, and police family-violence pathways. Processes and forms differ; principles do not: report reasonable suspicion, document, multi-agency conference, child-centred safety plan. Avoid fabricated section citations from any single Children's Act.[3][6]
Parental capacity
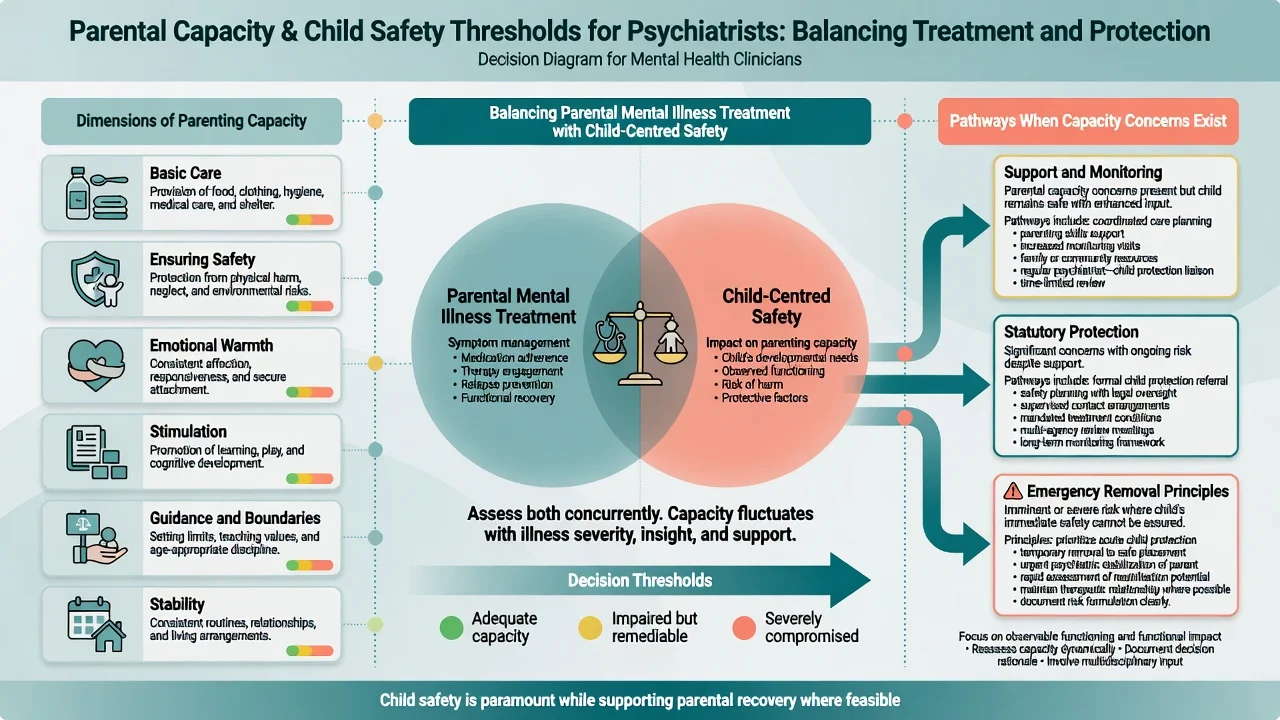
Parenting capacity is the ability to meet a child's needs over time across domains commonly framed as: basic care; ensuring safety; emotional warmth; stimulation; guidance and boundaries; and stability. It is not a global IQ label, a single diagnosis, or a one-off clinic observation.[3][17]
Decision-making capacity of a parent (for their own medical treatment) uses functional abilities to understand, appreciate, reason/weigh, and communicate a choice after material information — the Appelbaum framework.[17] That is related to but not identical with parenting capacity. A parent may have capacity to consent to their own antidepressant yet still be unable to keep a toddler safe while intoxicated.[17][3]
Exam rules: optimise treatable parental factors while keeping child-centred thresholds; temporary incapacity can justify emergency protection; support when safe, statutory action when significant harm is likely despite support.[3][4][17]
- Optimise treatable parental factors (psychosis, depression, substance use, IPV) while maintaining child-centred thresholds.[3][4]
- Insight, engagement, support network, and history of change matter as much as diagnosis name.[3]
- Temporary incapacity (intoxication, untreated mania) can justify emergency protection even if long-term prognosis is better with treatment.[3]
- Supported parenting plans are appropriate when risk is manageable; statutory protection is required when significant harm is likely despite support.[3][4]
Acute management
Medical priorities: stabilise injuries, head trauma, malnutrition, poisoning; involve paediatric forensic pathways early for suspected physical or sexual abuse.[13][14]
Psychiatric priorities: manage acute suicidality, severe agitation, psychosis, or intoxication in parent or adolescent using least-restrictive local mental health law principles — again without invented sections.[17]
Do not discharge a child to unresolved danger with only an outpatient appointment. Admission can be both medical care and a temporary place of safety while multi-agency planning occurs.[3]
Definitive multi-agency management
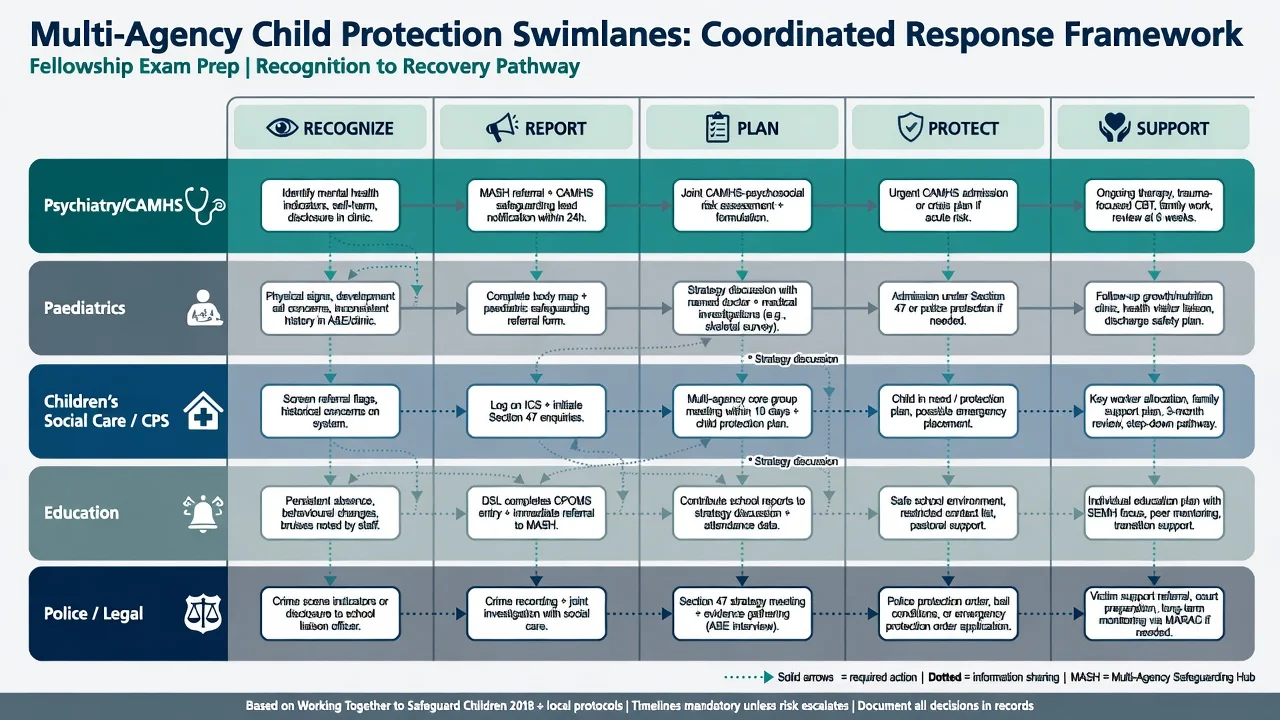
Health/psychiatry lane: trauma-informed assessment and treatment; TF-CBT adaptations for complex trauma when indicated; treat depression, anxiety, PTSD symptoms, and self-harm; provide clear capacity and parenting-risk opinions; write usable reports.[20][4]
Paediatrics: medical evaluation of injury/neglect/sexual abuse concerns.[13][14]
Children's social care / CPS: assessment, child-protection planning, placement decisions under local law.[3][6]
Education: attendance, safeguarding leads, educational neglect signals.[3]
Police/legal: criminal investigation when indicated; protection orders principles; court reports that separate fact and opinion.[3]
Prevention and parenting programmes with evidence examiners may cite: nurse home visitation shows long-term reductions in child abuse/neglect outcomes in classic trial follow-up; parent-child interaction therapy reduced re-reports among physically abusive parents in RCT evidence; broader prevention and treatment interventions are synthesised in the MacMillan Lancet review.[18][19][4]
FII pathway: early multi-agency recognition, limit unnecessary procedures, protect the child, carefully managed caregiver engagement — unilateral confrontation without a plan increases risk.[15]
Special scenarios
Non-ambulant infant injury. Highest-stakes physical abuse pathway; full paediatric evaluation and statutory report with low threshold.[13]
Adolescent sexual abuse disclosure. Believe, protect, report, assess sibling risk, avoid repeated interviewing, offer trauma therapy access, manage confidentiality limits honestly.[14][20]
Parental severe mental illness. Formulate risk from behaviour and functioning, not diagnosis stigma. Support recovery while not minimising neglect or violence.[3][17]
Children with disability. Higher maltreatment risk and harder disclosure; diagnostic overshadowing is common.[2]
Indigenous and culturally diverse families. Historical trauma and over-representation require culturally safe practice and community-informed supports — without lowering the significant-harm threshold.[3]
Looked-after children. Placement instability, cumulative trauma, and high CAMHS need; protection duties continue in care settings.[2][20]
Prognosis and disposition
Maltreatment is associated with lifelong mental and physical health burden and population-level costs; early safe caregiving and evidence-based intervention improve trajectories.[5][7][8] Disposition requires a named safe placement, multi-agency owner, sibling safety check, review date, and clear information-sharing plan. Therapeutic gains collapse if the child returns to ongoing abuse.[3][4][20]
Exam pearls
PROTECT (bedside prompt)
Pitfalls
- Waiting for proof before reporting.[3]
- Inventing statute section numbers in viva.[6]
- Equating parental mental illness with automatic child removal — or the opposite minimisation because the parent is your patient.[17]
- Leading questions that contaminate forensic process.[14]
- Discharging home with unresolved safety and only "CAMHS follow-up."[3]
- Missing emotional abuse because there are no bruises.[16][5]
- Ignoring sibling risk after one disclosure.[3]
- Uncoordinated confrontation in suspected FII.[15]
Fellowship standard: recognise early, protect first, document facts, report on reasonable suspicion under local duty, assess parental capacity properly, treat trauma sequelae, coordinate multi-agency care — and speak about law as jurisdiction-specific principles, never improvised statutes.[2][3][17]
References
- [1]Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study Am J Prev Med, 1998.PMID 9635069
- [2]Gilbert R, Widom CS, Browne K, et al. Burden and consequences of child maltreatment in high-income countries Lancet, 2009.PMID 19056114
- [3]Gilbert R, Kemp A, Thoburn J, et al. Recognising and responding to child maltreatment Lancet, 2009.PMID 19056119
- [4]MacMillan HL, Wathen CN, Barlow J, et al. Interventions to prevent child maltreatment and associated impairment Lancet, 2009.PMID 19056113
- [5]Norman RE, Byambaa M, De R, et al. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis PLoS Med, 2012.PMID 23209385
- [6]Gilbert R, Fluke J, O'Donnell M, et al. Child maltreatment: variation in trends and policies in six developed countries Lancet, 2012.PMID 22169108
- [7]Hughes K, Bellis MA, Hardcastle KA, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis Lancet Public Health, 2017.PMID 29253477
- [8]Bellis MA, Hughes K, Ford K, et al. Life course health consequences and associated annual costs of adverse childhood experiences across Europe and North America Lancet Public Health, 2019.PMID 31492648
- [9]Anda RF, Felitti VJ, Bremner JD, et al. The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology Eur Arch Psychiatry Clin Neurosci, 2006.PMID 16311898
- [10]Teicher MH, Samson JA Annual Research Review: Enduring neurobiological effects of childhood abuse and neglect J Child Psychol Psychiatry, 2016.PMID 26831814
- [11]Varese F, Smeets F, Drukker M, et al. Childhood adversities increase the risk of psychosis: a meta-analysis of patient-control, prospective- and cross-sectional cohort studies Schizophr Bull, 2012.PMID 22461484
- [12]Stoltenborgh M, van Ijzendoorn MH, Euser EM, Bakermans-Kranenburg MJ A global perspective on child sexual abuse: meta-analysis of prevalence around the world Child Maltreat, 2011.PMID 21511741
- [13]Christian CW, Committee on Child Abuse and Neglect, American Academy of Pediatrics The evaluation of suspected child physical abuse Pediatrics, 2015.PMID 25917988
- [14]Kellogg N, American Academy of Pediatrics Committee on Child Abuse and Neglect The evaluation of sexual abuse in children Pediatrics, 2005.PMID 16061610
- [15]Bass C, Glaser D Early recognition and management of fabricated or induced illness in children Lancet, 2014.PMID 24612863
- [16]Glaser D Emotional abuse and neglect (psychological maltreatment): a conceptual framework Child Abuse Negl, 2002.PMID 12201163
- [17]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [18]Olds DL, Eckenrode J, Henderson CR Jr, et al. Long-term effects of home visitation on maternal life course and child abuse and neglect. Fifteen-year follow-up of a randomized trial JAMA, 1997.PMID 9272895
- [19]Chaffin M, Silovsky JF, Funderburk B, et al. Parent-child interaction therapy with physically abusive parents: efficacy for reducing future abuse reports J Consult Clin Psychol, 2004.PMID 15279533
- [20]Cohen JA, Mannarino AP, Kliethermes M, Murray LA Trauma-focused CBT for youth with complex trauma Child Abuse Negl, 2012.PMID 22749612