Psych · Child and adolescent psychiatry — OCRD
Childhood-onset OCD
Also known as Paediatric OCD · Pediatric obsessive-compulsive disorder · Juvenile OCD · Early-onset OCD · Child OCD · Adolescent OCD · CY-BOCS
Exam-exhaustive fellowship reference on childhood-onset OCD — DSM-5-TR criteria, family accommodation, CY-BOCS, ERP and family-based CBT (POTS/POTS Jr), SSRI evidence with paediatric monitoring, tic-related and PANDAS/PANS exam nuance. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Childhood-onset OCD is high-yield across FRANZCP CAP, MRCPsych CASC/Paper, ABPN and MD/DNB. Examiners test ERP by name, family accommodation, paediatric SSRI evidence and monitoring, the POTS / POTS II / POTS Jr trial sequence, tic-related OCRD, and disciplined PANDAS/PANS language without turning every case into a throat swab.[1][2][3][4][11]
Overview and definition
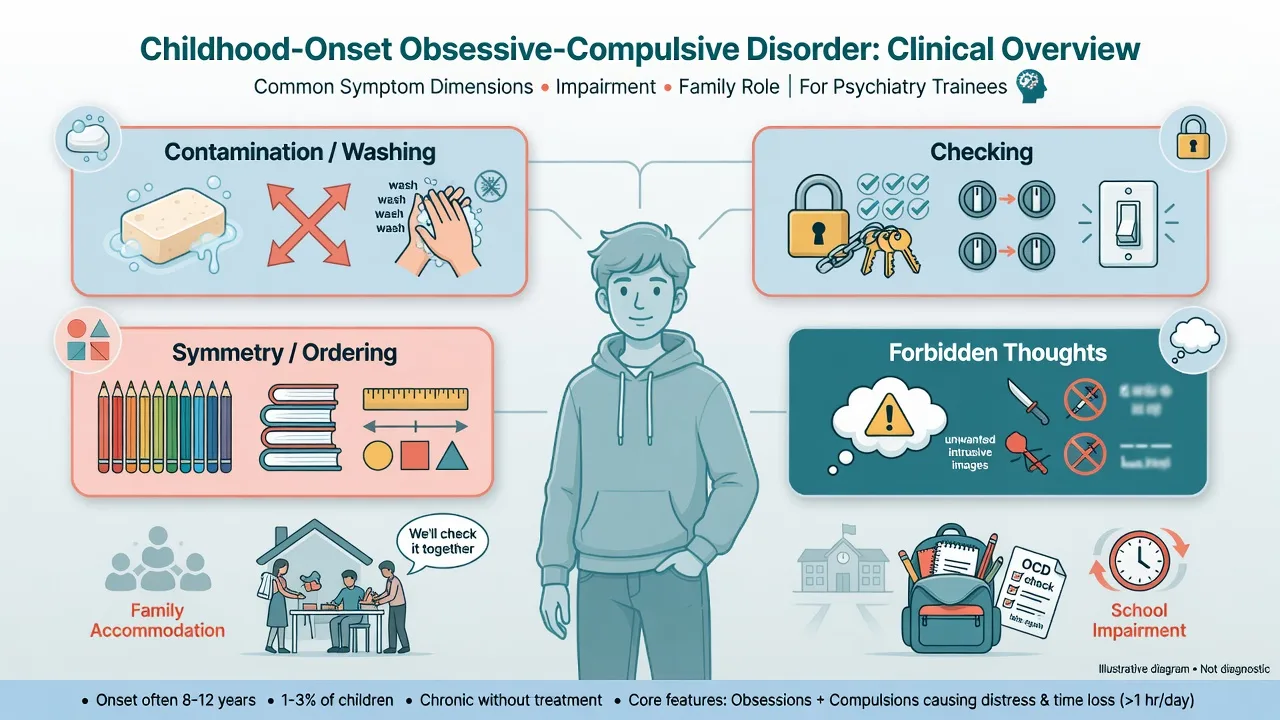
Obsessions are recurrent, intrusive, unwanted thoughts, images or urges that cause marked anxiety or distress. Compulsions are repetitive behaviours or mental acts performed to reduce distress or prevent a dreaded event — even when the link is unrealistic. In children, ego-dystonicity may be poorly verbalised; parents often describe rituals, reassurance-seeking and family routines reorganised around the symptoms.[4][17]
Classic teaching still uses time-consuming symptoms (often framed as more than about 1 hour/day) or marked distress/impairment as the clinical severity threshold, alongside the requirement that symptoms are not better explained by substances, another medical condition, or another mental disorder.[4][17]
Classification
DSM-5-TR skeleton (must own)
| Element | Exam rule of thumb |
|---|---|
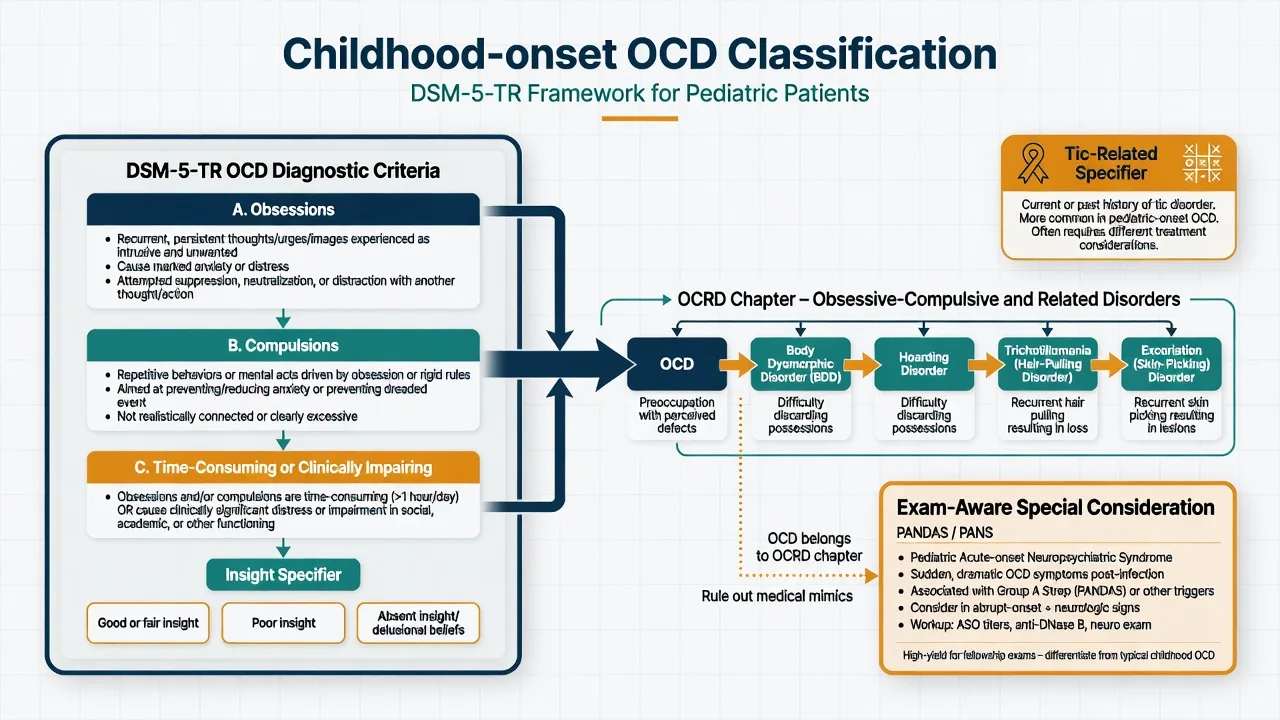
| Obsessions | Intrusive, unwanted, anxiety-linked thoughts/images/urges; attempts to ignore/suppress/neutralise |
| Compulsions | Repetitive behaviours or mental acts aimed at reducing distress or preventing feared outcomes |
| Threshold | Time-consuming (classic greater than about 1 hour/day teaching) or clinically significant distress/impairment |
| Insight specifier | Good/fair; poor; absent insight/delusional beliefs — still OCD, not automatic schizophrenia |
| Tic-related specifier | Current or past history of tic disorder — higher male, earlier-onset flavour |
| OCRD neighbours | BDD, hoarding, trichotillomania, excoriation — related but distinct |
DSM-5-TR places OCD among obsessive-compulsive and related disorders, not merely “an anxiety disorder.” ICD-11 retains OCD with related spectrum concepts; state which manual you apply when thresholds are examined.[4][17][18]
OCD
- Ego-dystonic typically
- Anxiety-driven rituals
- ERP + SSRI evidence
- CY-BOCS severity
ASD routines
- Often preferred sameness
- Less anxiety-neutralisation logic
- Social-communication context
- Adapt ERP carefully
Complex tics
- Premonitory urge
- Brief suppressibility
- Less goal-directed
- CBIT not ERP alone
Psychosis trap
- Poor insight OCD exists
- Primary psychotic process differs
- Do not start with high-dose AP
- Formulate OCRD first
Epidemiology and risk
Numbers candidates should own
Ruscio and colleagues quantified lifetime and 12-month OCD prevalence and age-of-onset distributions in a large US survey — use order-of-magnitude epidemiology, not false clinic precision.[12] Genetic and family studies support substantial heritability with shared liability for tic disorders and related phenotypes rather than a single gene model.[16] Functional burden includes academic delay, family conflict, sleep disruption and elevated suicide risk especially with depression and shame about forbidden thoughts.[4][17]
Pathophysiology
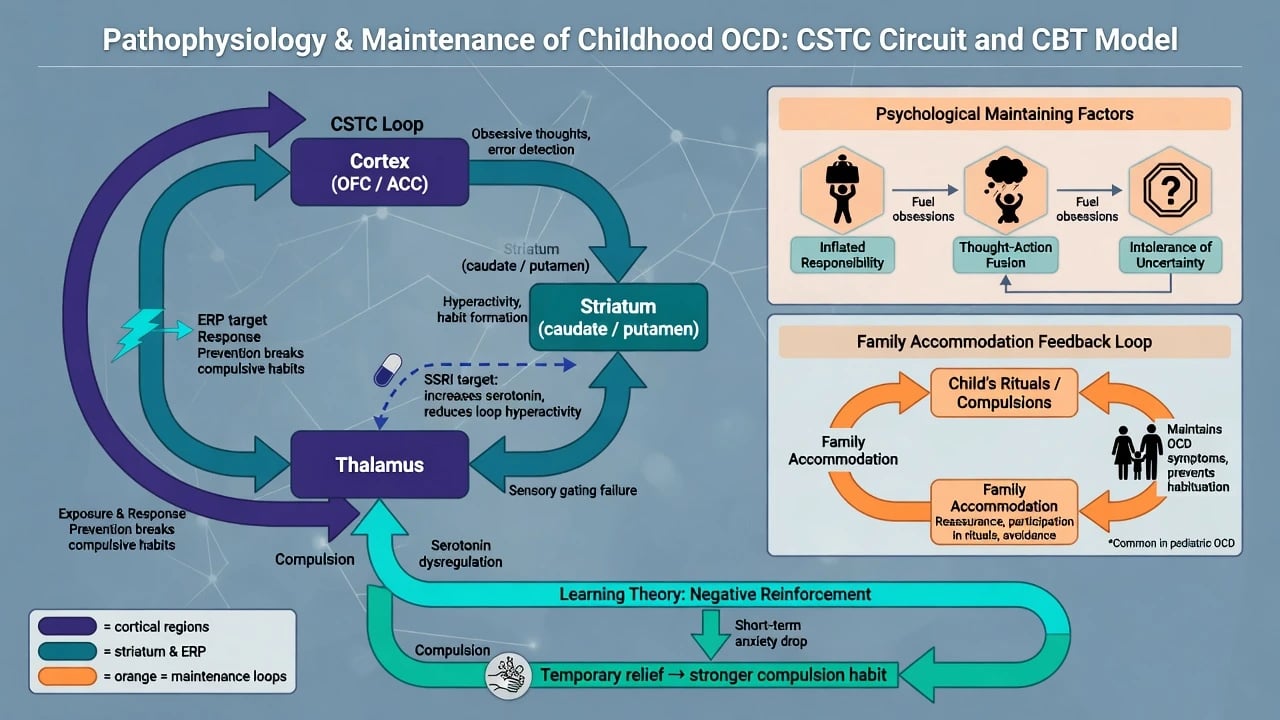
Teaching-level pathophysiology emphasises cortico-striato-thalamo-cortical (CSTC) circuit dysregulation. Serotonergic pharmacology is clinically relevant because SSRIs reduce symptoms with a delayed time course; this is not proof of a simple “serotonin deficiency.” Glutamatergic and dopaminergic pathways appear in specialist refractory discussions.[17][18]
Psychological models that drive ERP targets include inflated responsibility, thought–action fusion, and intolerance of uncertainty. Compulsions produce short-term anxiety reduction and are maintained by negative reinforcement. Family accommodation — participation in rituals, provision of reassurance, and modification of family routines — is a major paediatric maintenance factor linked to severity and poorer outcomes when unaddressed.[10][4]
Clinical presentation
Common paediatric dimensions. Contamination/washing; checking; symmetry/ordering and “just right” feelings; counting/repeating; forbidden aggressive, sexual or religious thoughts with mental reviewing; reassurance-seeking as a covert compulsion.[4][5]
Family system. Parents may re-wash laundry, open doors, answer endless “Are you sure?” questions, or rearrange schedules. Accommodation feels compassionate and often maintains the disorder.[10]
School. Incomplete work from rewriting, bathroom delays, avoidance of art materials or PE equipment, late arrival after morning rituals, and secondary bullying or school refusal.[4]
MSE examples. “I keep thinking I might have hurt someone even though I know I didn’t.” “If the pencils aren’t even I can’t start.” Covert mental rituals may leave little visible motor behaviour — do not dismiss “pure O” presentations in adolescents.[4][17]
Differential diagnosis
- ASD restricted interests/routines — preferred sameness and special interests versus anxiety-driven neutralisation; both can co-occur.[4]
- Tics / Tourette — urge-driven, less purposeful; complex tics can mimic rituals; use tic-related OCD specifier when both exist.[4]
- GAD / separation anxiety / illness anxiety — worry domains without classic OCD ritual structure, though overlap is common.
- PTSD — trauma-linked intrusive memories rather than ego-dystonic obsession themes.
- Psychosis — primary delusional system, thought disorder, negative symptoms; poor-insight OCD remains on the OCRD spectrum.[17]
- PANDAS/PANS — acute, dramatic paediatric neuropsychiatric onset temporally linked to infection in original descriptions; do not force chronic typical OCD into this box without specialist criteria.[11]
- Body dysmorphic disorder / hoarding / hair-pulling — OCRD siblings with distinct primary preoccupations.[17]
Assessment
Structure: phenotype + time occupied + insight + accommodation + school function + comorbidity + risk + prior treatment adequacy.[4]
- Separate and joint interviews with youth and carers; developmental and family OCD/tic/anxiety history.
- Map obsessions/compulsions by dimension; quantify hours and interference.
- Explicitly inventory family accommodation (reassurance, participation, modified routines).[10]
- Screen tics, ADHD, anxiety, mood, ASD, learning difficulties, substances, safeguarding and bullying.
- Risk: suicide/self-harm, severe self-neglect, ability to attend school.
- Shared decision-making; correct “it’s just a phase / they can stop if they try” myths.
CY-BOCS (Children’s Yale–Brown Obsessive Compulsive Scale) is the clinician-rated paediatric gold standard for severity (obsession and compulsion items plus checklist). Use for baseline and measurement-based care; it does not replace clinical diagnosis.[5]
Investigations
Uncomplicated developmental OCD is a clinical diagnosis. Routine MRI/EEG is not indicated without neurological red flags (late abrupt progressive course, focal signs, encephalopathy, seizures, cognitive regression).[4]
Before SSRI: full psychiatric risk assessment, growth parameters, sleep, sexual function discussion in adolescents, drug interactions, and pregnancy risk discussion when relevant. ECG and specialist cardiac history when using clomipramine or high-risk polypharmacy. Serial CY-BOCS for response tracking.[4][5][14]
PANDAS/PANS. Consider when history shows abrupt, dramatic paediatric onset with tics/OCD after infection-compatible course; Swedo and colleagues described the classic streptococcal-associated series. This does not justify ASO titres and antibiotics for every chronic childhood OCD case — formulate carefully and continue standard OCD treatment while seeking specialist paediatric input if indicated.[11][4]
Acute safety
Definitive management
Psychoeducation and family accommodation reduction
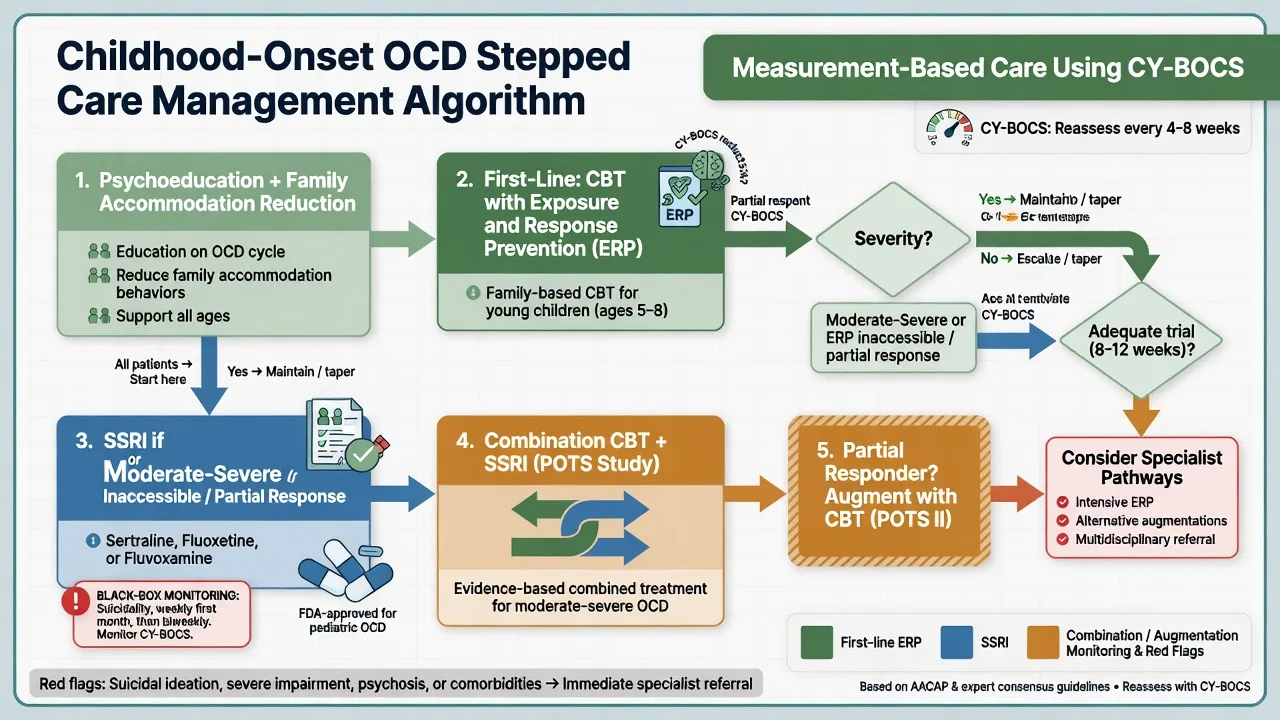
Explain OCD as a treatable neurodevelopmental–cognitive loop, not wilful misbehaviour. Teach carers that reassurance and ritual participation temporarily calm the child and strengthen the disorder. Coaching carers to reduce accommodation is core paediatric CBT, not optional extras.[4][10]
CBT with exposure and response prevention (ERP)
ERP is the first-line psychological treatment: graded exposure to obsession triggers while preventing compulsive rituals (including mental rituals and reassurance). Hierarchy building, therapist-assisted and homework exposures, and relapse prevention are essential components. Watson and Rees’ meta-analysis of paediatric RCTs found both CBT and pharmacotherapy superior to control, with a larger pooled effect size for CBT in the included trials — supporting ERP emphasis when accessible.[9][4]
Young children. Family-based CBT is preferred. The POTS Jr randomised trial showed family-based CBT superior to family-based relaxation for early childhood OCD — name this trial for young-child questions.[3]
Landmark paediatric trials: POTS sequence
POTS (2004). Multicentre RCT in children and adolescents comparing CBT, sertraline, combination and placebo. CBT and sertraline each outperformed placebo; combination was particularly effective, especially for more severe illness. This is the foundational exam trial for paediatric OCD treatment hierarchy.[1]
POTS II (2011). Among partial responders to SRIs, adding instruction in CBT/ERP improved outcomes versus medication management alone — exam lesson: do not abandon ERP when a child is already on an SSRI with incomplete response.[2]
Pharmacotherapy — SSRIs
Medication is indicated for moderate–severe OCD, when ERP is inaccessible/refused/insufficient, or in combination for severe illness per shared decision-making and AACAP parameter framing.[4]
Paediatric RCT evidence supports:
- Sertraline — multicentre RCT efficacy (March et al.) and POTS sertraline arm.[6][1]
- Fluoxetine — placebo-controlled paediatric RCT (Geller et al.).[7]
- Fluvoxamine — multicentre paediatric RCT (Riddle et al.).[8]
Adult OCD meta-analysis by Bloch and colleagues supports higher SSRI dose–response relationships; paediatric practice still starts low and titrates to OCD-therapeutic (often higher than depression starting targets) with an adequate trial typically framed as about 8–12 weeks at a therapeutic dose, not a 10-day judgment.[13][4][14]
Exam-level dosing frameworks (always individualise; check local product information, age limits and specialist advice).[4][6][7][8]
| Agent | Typical paediatric framework | Monitoring |
|---|---|---|
| Sertraline oral | Often start ~25 mg daily (younger/low weight may start lower); titrate toward approximately 50–200 mg/day range used in paediatric OCD trials/practice | Activation, GI, sleep, sexual AEs in adolescents; black-box suicidality; interactions |
| Fluoxetine oral | Start ~10 mg daily then 20 mg; trial titration toward ~20–60 mg/day as in paediatric OCD RCT framework | Long half-life; activation; interactions (CYP); black-box |
| Fluvoxamine oral | Start low (often ~25 mg); titrate toward trial ranges commonly up to ~200 mg/day divided as product allows | Sedation/GI; CYP interactions; black-box |
| Clomipramine | Specialist second-line after SSRI failure — TCA cardiac/seizure/anticholinergic risks | ECG, vitals, toxicity education |
Black-box suicidality monitoring in children and adolescents on antidepressants is mandatory: early review, carer education, clear contact plan for agitation, akathisia-like restlessness, or new self-harm thoughts.[4][6][7][8]
Combination, augmentation, refractory
- Prefer ERP + SSRI for severe paediatric OCD (POTS).[1]
- For SRI partial response, add/intensify CBT (POTS II) before reflexive polypharmacy.[2]
- Antipsychotic augmentation has adult refractory evidence (Bloch systematic review) but is specialist, low-dose, time-limited, and metabolically monitored in youth — not first-line CAP practice.[15][4]
- Intensive ERP programmes, clomipramine, and ultra-specialist adult-style neuromodulation pathways are rare paediatric steps after comprehensive failure.[14][18]
Regional practice notes
Australian and New Zealand CAP practice emphasises family-inclusive ERP, CAMHS stepped care, careful SSRI initiation with black-box monitoring, and school liaison. Access to specialist ERP varies by jurisdiction — name ERP components even when branded programmes are waitlisted.[4]
Comorbidity focus
Tics / Tourette. Use tic-related specifier; discriminate urge-driven tics from goal-directed compulsions; treat both when impairing (ERP for OCD; CBIT/tic meds per tic pathway).[4]
ADHD. Impairs ERP homework adherence and school function — treat deliberately as part of comprehensive CAP care.[4][17]
Anxiety and depression. Common comorbidities; treat depression and suicide risk actively; anxiety may need parallel exposure work alongside ERP for OCD.[4][17]
ASD. Formulate which behaviours are OCD versus restricted interests; adapt ERP with visual supports and caregiver coaching.[4]
Prognosis and disposition
Many youth improve substantially with ERP ± SSRI; residual symptoms and relapse risk remain, so booster sessions and maintenance medication plans matter. Longer duration untreated, high accommodation, comorbidity, and poor insight predict harder courses.[4][9][17]
Disposition: mild cases with skilled ERP access in ambulatory CAMHS; moderate–severe or refractory cases to specialist OCD pathways; intensive/day programmes for severe functional collapse; plan transition to adult services for persistent illness.[4][18]
Complications and pitfalls
- Supportive therapy without ERP.[4][9]
- Under-dosing SSRI or aborting trial at 2–3 weeks.[13]
- Ignoring family accommodation.[10]
- Labelling poor-insight OCD as schizophrenia.[17]
- Omitting black-box monitoring.[4]
- Overcalling PANDAS in chronic gradual OCD.[11]
- Punishing rituals as “attention-seeking.”
Special populations
Preschool / early primary: family-based CBT (POTS Jr); medication exceptional and specialist.[3] Adolescents: autonomy, mental rituals, sexual side-effect discussion, self-harm risk, digital reassurance-seeking. ID/ASD: adapted ERP; careful differential of routines. Cultural/religious scrupulosity: culturally safe formulation with faith leaders only if helpful and consented. PANDAS/PANS pathway: specialist paediatric collaboration; do not delay ERP/SSRI when indicated for OCD itself.[11][4]
Exam pearls
CHILD OCD plan
References
- [1]Pediatric OCD Treatment Study (POTS) Team Cognitive-behavior therapy, sertraline, and their combination for children and adolescents with obsessive-compulsive disorder: the Pediatric OCD Treatment Study (POTS) randomized controlled trial JAMA, 2004.PMID 15507582
- [2]Franklin ME, Sapyta J, Freeman JB, et al. Cognitive behavior therapy augmentation of pharmacotherapy in pediatric obsessive-compulsive disorder: the Pediatric OCD Treatment Study II (POTS II) randomized controlled trial JAMA, 2011.PMID 21934055
- [3]Freeman J, Sapyta J, Garcia A, et al. Family-based treatment of early childhood obsessive-compulsive disorder: the Pediatric Obsessive-Compulsive Disorder Treatment Study for Young Children (POTS Jr)—a randomized clinical trial JAMA Psychiatry, 2014.PMID 24759852
- [4]American Academy of Child and Adolescent Psychiatry Practice parameter for the assessment and treatment of children and adolescents with obsessive-compulsive disorder J Am Acad Child Adolesc Psychiatry, 2012.PMID 22176943
- [5]Scahill L, Riddle MA, McSwiggin-Hardin M, et al. Children's Yale-Brown Obsessive Compulsive Scale: reliability and validity J Am Acad Child Adolesc Psychiatry, 1997.PMID 9183141
- [6]March JS, Biederman J, Wolkow R, et al. Sertraline in children and adolescents with obsessive-compulsive disorder: a multicenter randomized controlled trial JAMA, 1998.PMID 9842950
- [7]Geller DA, Hoog SL, Heiligenstein JH, et al. Fluoxetine treatment for obsessive-compulsive disorder in children and adolescents: a placebo-controlled clinical trial J Am Acad Child Adolesc Psychiatry, 2001.PMID 11437015
- [8]Riddle MA, Reeve EA, Yaryura-Tobias JA, et al. Fluvoxamine for children and adolescents with obsessive-compulsive disorder: a randomized, controlled, multicenter trial J Am Acad Child Adolesc Psychiatry, 2001.PMID 11211371
- [9]Watson HJ, Rees CS Meta-analysis of randomized, controlled treatment trials for pediatric obsessive-compulsive disorder J Child Psychol Psychiatry, 2008.PMID 18400058
- [10]Calvocoressi L, Lewis B, Harris M, et al. Family accommodation in obsessive-compulsive disorder Am J Psychiatry, 1995.PMID 7864273
- [11]Swedo SE, Leonard HL, Garvey M, et al. Pediatric autoimmune neuropsychiatric disorders associated with streptococcal infections: clinical description of the first 50 cases Am J Psychiatry, 1998.PMID 9464208
- [12]Ruscio AM, Stein DJ, Chiu WT, Kessler RC The epidemiology of obsessive-compulsive disorder in the National Comorbidity Survey Replication Mol Psychiatry, 2010.PMID 18725912
- [13]Bloch MH, McGuire J, Landeros-Weisenberger A, Leckman JF, Pittenger C Meta-analysis of the dose-response relationship of SSRI in obsessive-compulsive disorder Mol Psychiatry, 2010.PMID 19468281
- [14]Koran LM, Hanna GL, Hollander E, Nestadt G, Simpson HB, American Psychiatric Association Practice guideline for the treatment of patients with obsessive-compulsive disorder Am J Psychiatry, 2007.PMID 17849776
- [15]Bloch MH, Landeros-Weisenberger A, Kelmendi B, et al. A systematic review: antipsychotic augmentation with treatment refractory obsessive-compulsive disorder Mol Psychiatry, 2006.PMID 16585942
- [16]Pauls DL The genetics of obsessive-compulsive disorder: a review Dialogues Clin Neurosci, 2010.PMID 20623920
- [17]Hirschtritt ME, Bloch MH, Mathews CA Obsessive-Compulsive Disorder: Advances in Diagnosis and Treatment JAMA, 2017.PMID 28384832
- [18]Fineberg NA, Hollander E, Pallanti S, et al. Clinical advances in obsessive-compulsive disorder: a position statement by the International College of Obsessive-Compulsive Spectrum Disorders Int Clin Psychopharmacol, 2020.PMID 32433254