Psych · Child and adolescent psychiatry — childhood trauma and maltreatment
Childhood trauma and maltreatment
Also known as Child abuse and neglect · Adverse childhood experiences · ACE · Childhood maltreatment · TF-CBT · Trauma-focused CBT children · Child protection psychiatry · Developmental trauma · Polyvictimisation
Exam-exhaustive fellowship reference on childhood trauma and maltreatment — types of abuse and neglect, ACE science and graded risk, developmental presentation, trauma-informed assessment, mandatory reporting principles, multi-agency protection, TF-CBT PRACTICE components, adjunct pharmacotherapy concepts, and trauma-informed systems of care. Distinct from adult complex PTSD and child-protection law monographs. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Childhood trauma and maltreatment is high-yield across FRANZCP CAP stations, MRCPsych CASC communication and risk stations, and ABPN child blueprints. Examiners test typology, ACE science without destiny myths, developmental presentations, dual loyalty (confidentiality vs reporting), TF-CBT components by name, and whether "trauma-informed" is genuine safety redesign or empty language.[4][10][12]
Overview and definition
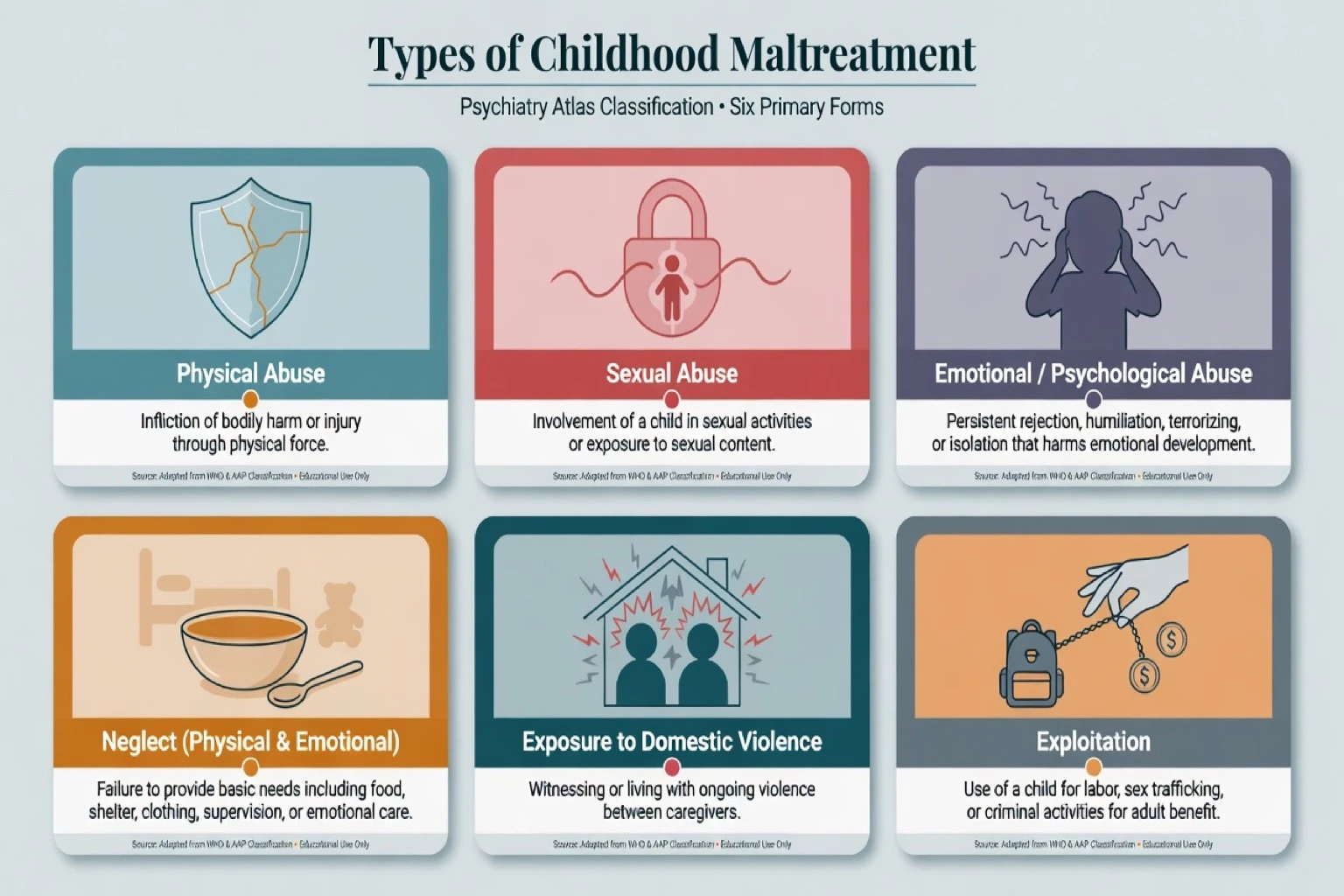
Child maltreatment comprises acts of commission or omission by a caregiver (or person in a caregiving role) that cause actual or potential harm to a child: physical abuse, sexual abuse, emotional/psychological abuse, and neglect (physical, emotional, medical, educational). Exposure to intimate partner violence and other household adversities are tightly interrelated and form part of the broader Adverse Childhood Experiences (ACE) construct used in epidemiology.[1][4]
Maltreatment is an exposure, not a psychiatric diagnosis. Mental disorders that may follow include PTSD, complex presentations under ICD-11, depression, anxiety, attachment disorders, substance use, and self-harm trajectories. Always separate (i) the safeguarding formulation, (ii) the psychiatric diagnosis, and (iii) the multi-agency protection plan.[4][12][15]
Broader childhood trauma includes disasters, community violence, peer assault, medical trauma, and refugee experiences. Those may produce similar symptom patterns without caregiver maltreatment; the protection pathway differs when the caregiver is the source of harm.[4]
Classification and typology
| Type | Core concept (exam language) | Psychiatric interface |
|---|---|---|
| Physical abuse | Non-accidental injury or risk of injury by caregiver | Injury–history mismatch; fear; PTSD; aggression |
| Sexual abuse | Sexual contact/exploitation by adult or older person in power | Delayed disclosure; shame; PTSD; sexualised behaviour |
| Emotional abuse | Chronic hostility, terrorising, rejection, isolation | Shame, attachment disruption, depression |
| Neglect | Failure to meet basic physical, emotional, medical, educational needs | Developmental delay, attachment disorders, failure to thrive |
| IPV exposure | Child witnesses coercive control / violence between carers | Hypervigilance, anxiety, modelling of aggression |
| Polyvictimisation | Multiple types over time | Highest cumulative risk; complex presentations |
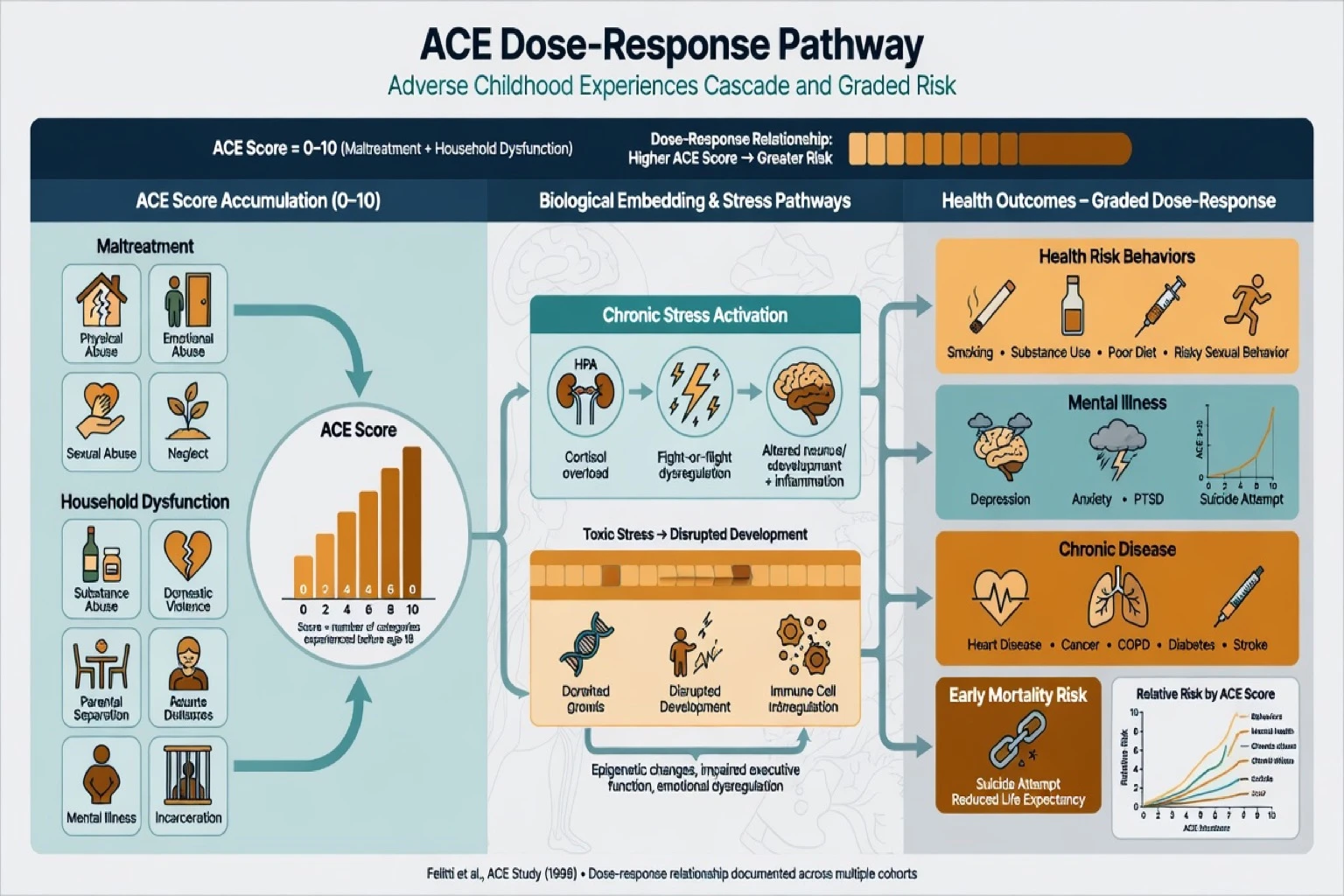
ACE categories (Felitti lineage). Abuse (emotional, physical, sexual), neglect (emotional, physical), and household dysfunction (mental illness, substance use, incarceration of household member, mother treated violently, parental separation/divorce). The ACE score counts categories; it is a population risk indicator with a graded relationship to adult outcomes — not a clinical diagnosis, not destiny, and not a standalone triage tool.[1][3][9]
Nosology of sequelae. DSM-5-TR trauma- and stressor-related disorders (PTSD, acute stress, adjustment, reactive attachment disorder, disinhibited social engagement disorder) may apply. ICD-11 adds formal complex PTSD architecture (PTSD core plus disturbances of self-organisation) relevant when prolonged childhood interpersonal trauma produces that symptom structure — full CPTSD depth is covered in the related adult complex-PTSD topic.[12][15]
Epidemiology and risk factors
Headline patterns candidates must own
Cumulative self-reported childhood maltreatment is common in high-income countries; official substantiation rates are lower because of under-detection and threshold effects. Long-term sequelae include mental disorders, substance use, suicide attempts, risky sexual behaviour, obesity, and criminal justice contact — effects that persist into adulthood.[4][6]
The original ACE study demonstrated a strong graded relationship between number of adverse childhood experiences and multiple adult risk factors for leading causes of death.[1] ACE score also shows a graded relationship to lifetime suicide attempts, with partial mediation by depression, substance use and alcoholism in that cohort analysis.[2] Meta-analytic work confirms that multiple ACEs associate with elevated odds of problematic alcohol use, drug use, interpersonal and self-directed violence, and mental ill-health among other outcomes.[9]
Risk factors for maltreatment. Parental mental illness and substance use, intimate partner violence, poverty and housing instability, social isolation, parental history of abuse, young parental age, child disability, and community deprivation. Protective factors include stable non-offending caregivers, social support, economic security, and timely culturally safe services.[4][5]
Pathophysiology and mechanisms
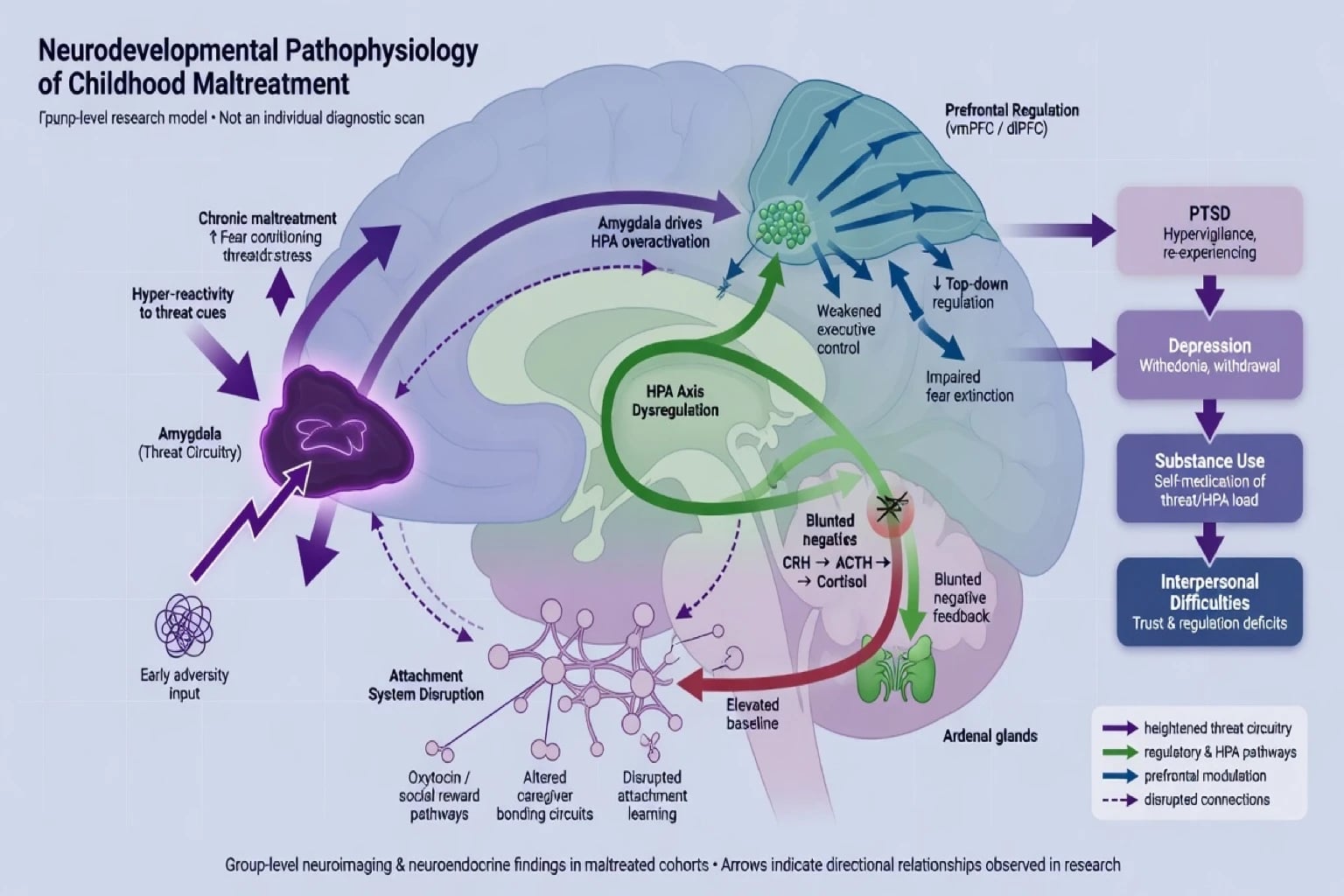
Toxic stress and biological embedding. Chronic or severe maltreatment dysregulates stress-responsive systems (including HPA axis), sensitises threat circuitry, and can alter developmental trajectories of prefrontal regulation and social cognition — synthesised in neurobiological reviews of childhood abuse and neglect.[3][8] State these as group-level findings; they are not bedside diagnostic tests.[8]
Ecophenotype concept. Within categories such as depression, anxiety, substance use and PTSD, maltreated individuals often show earlier onset, greater severity, more comorbidity and different neurobiological correlates than non-maltreated individuals with the same primary diagnosis — an argument for trauma-informed formulation within ordinary diagnoses, not only free-standing PTSD labels.[7]
Psychological mechanisms. Fear conditioning and overgeneralisation of danger; shame-based self-schemas after interpersonal betrayal; attachment disruption impairing co-regulation; modelling of aggression or appeasement; and coping via dissociation, self-harm or substances in adolescence.[3][7]
Clinical presentation
Preschool. Regression, clinginess or indiscriminate sociability, sleep and appetite disturbance, aggression, fearfulness of specific people or settings, developmental plateau. Observation of caregiver–child interaction is often more informative than verbal interview.[4][12]
School-age. Re-experiencing (play re-enactment, nightmares), avoidance, hyperarousal, concentration problems (ADHD mimic), somatic complaints, academic decline, and behavioural outbursts. Shame and secrecy are common after sexual abuse.[12]
Adolescents. PTSD clusters, depression, self-harm, substance use, sexual risk, revictimisation, running away, and distrust of adults/services. Historical childhood abuse may first be disclosed in CAMHS for another presenting problem.[4][6]
MSE focus. Affect may be restricted, irritable or labile; thought content often includes shame, self-blame and foreshortened future; perception may include trauma-related pseudo-hallucinatory flashbacks distinct from primary psychosis; insight into the trauma link varies by age; risk assessment (suicide, self-harm, ongoing abuse, exploitation) is mandatory every contact.[2][12]
Differential diagnosis
| Presentation | Favours maltreatment sequelae | Favours alternative |
|---|---|---|
| Inattention / hyperactivity | Onset after trauma; hypervigilance; nightmares | Lifelong ADHD pattern across settings pre-trauma |
| Mood instability | Trauma-linked triggers; shame; nightmares | Clear mania/hypomania periods |
| Psychosis-like experiences | Trauma content; intact thought form; night-linked | Novel bizarre delusions, thought disorder, negative symptoms |
| Attachment disorder features | Pathogenic care history required for RAD/DSED | Autism social pattern without pathogenic care |
| Conduct problems | Trauma, neglect, modelling of violence context | Instrumental aggression without trauma markers |
Also consider organic injury, medical illness presenting as failure to thrive, factitious disorder imposed on another (rare, high stakes), and cultural practices misread as abuse — use multi-agency paediatric expertise rather than solo cultural guesswork.[4]
Clinical and bedside assessment
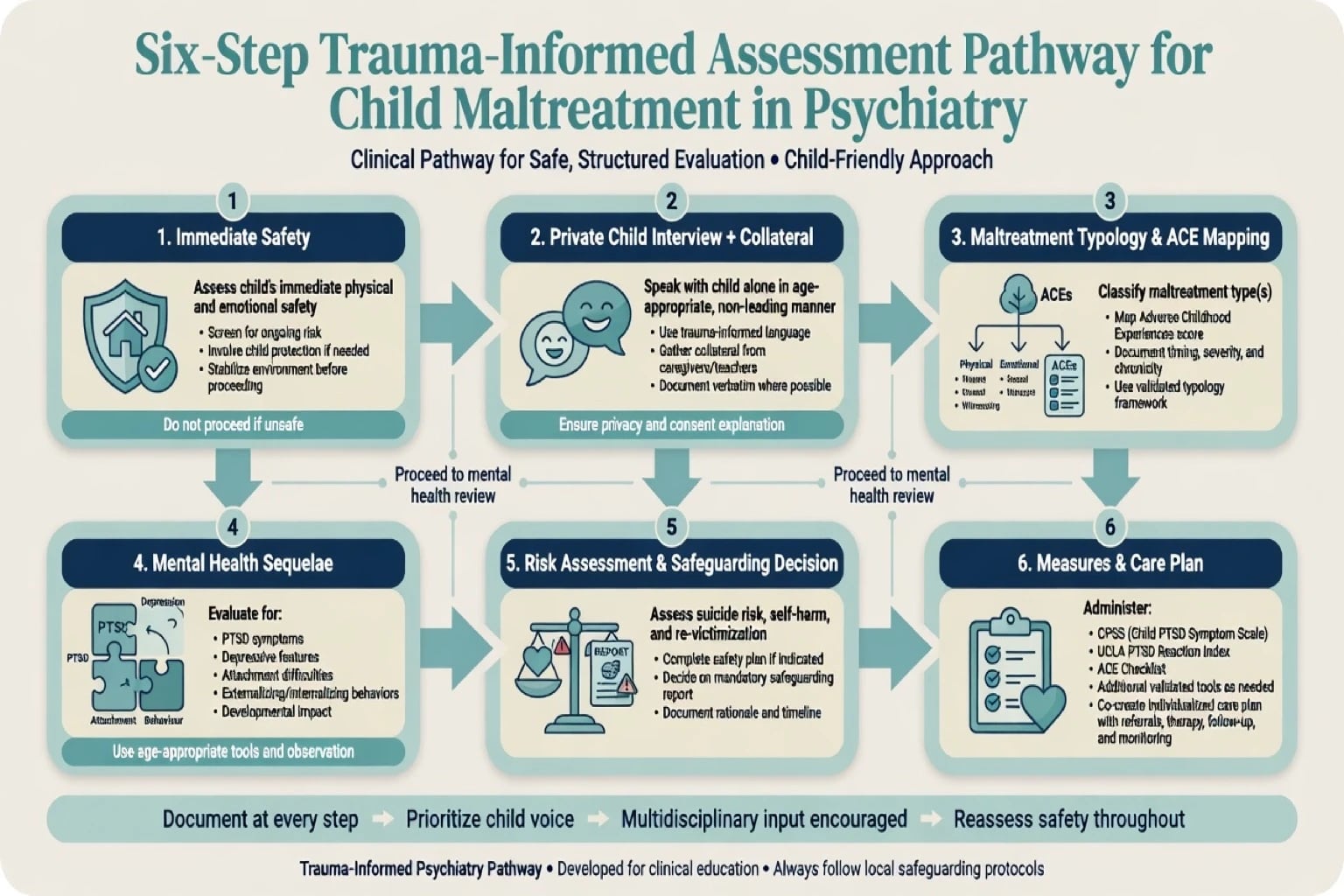
Trauma-informed stance. Safety, trustworthiness, choice, collaboration, empowerment and cultural humility guide every interview and service contact.[13] Obtain enough detail to establish exposure and symptom linkage without forcing a full graphic recount in the first minutes. Offer control over pacing, breaks, and who is in the room.[12][13]
Interview structure.
- Immediate safety and medical needs.
- Private time with the child when developmentally appropriate and safe — essential for many disclosures.
- Non-leading, open questions; document verbatim disclosures.
- Collateral from non-offending carers, school, paediatricians, prior agencies.
- Map maltreatment types and ACE domains for formulation.
- Full psychiatric assessment including suicide/self-harm, substance use, sexual exploitation.
- Explicit safeguarding decision: report / multi-agency strategy / monitor with review time.[4][12]
Measures (support, do not replace clinical judgement). Age-appropriate PTSD scales (e.g. CPSS, UCLA PTSD Reaction Index), broader trauma symptom inventories where validated, depression/anxiety scales, and functional impairment at home and school. ACE checklists can structure history but must not be used as destiny scores or sole risk tools.[1][12]
Investigations
There is no blood test or MRI that diagnoses maltreatment. Coordinate medical examination with paediatric/forensic pathways when physical or sexual abuse is suspected — do not freelance genital exams or unauthorised photography. Baseline metabolic work, ECG, pregnancy test and urine drug screen as indicated before psychotropics. Neuroimaging only for neurological red flags.[4][12]
Management — acute / resuscitation
Immediate priorities. Treat injuries; ensure physical safety; psychological first aid (calm information, contact with safe adults, practical support). Manage acute suicidality and self-harm with CAMHS crisis pathways and means restriction. Avoid forced single-session mandatory debriefing of all survivors as universal prevention.[12]
Mandatory reporting principles (exam language). When there is reasonable suspicion of child abuse or neglect, clinicians have a duty to notify the designated statutory authority under local law. Explain the limit of confidentiality to the family when safe and appropriate. Do not invent jurisdiction-specific section numbers in the exam answer; state the principle, the threshold language, and multi-agency collaboration. Do not investigate alone as an amateur detective or delay reporting to "complete therapy first".[4][12]
Management — definitive and stepwise
Trauma-informed care (systems level)
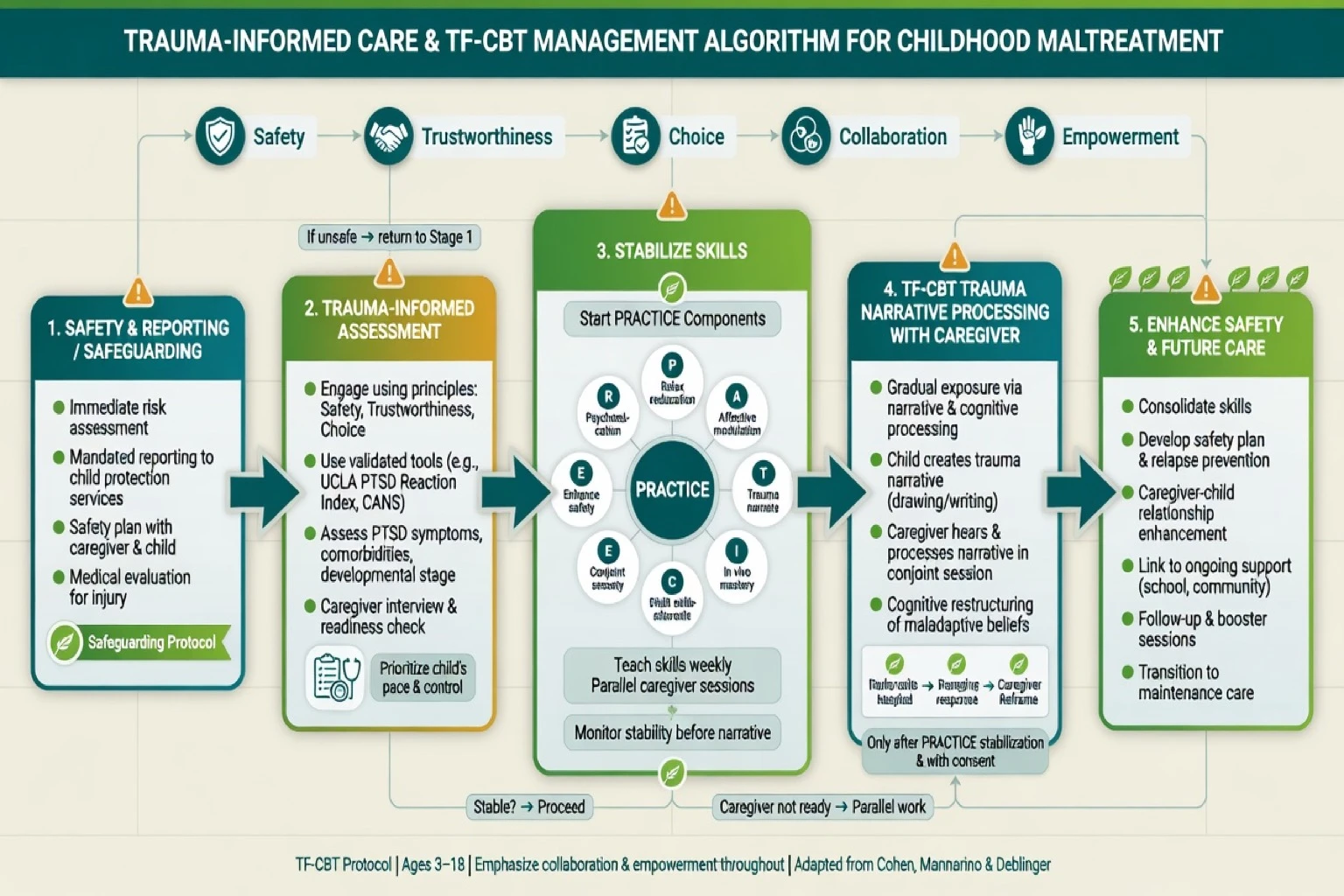
Trauma-informed care redesigns services so they minimise retraumatisation and maximise engagement: transparent processes, predictable appointments, consent and choice about trauma detail, shared decisions, cultural safety, and staff supervision for secondary trauma. It is service design, not a soft alternative to evidence-based trauma therapy.[13]
TF-CBT — first-line trauma-focused treatment
Trauma-Focused Cognitive Behavioral Therapy (TF-CBT) (Cohen, Mannarino, Deblinger) is a components-based treatment for children and adolescents with trauma-related symptoms, typically involving a non-offending caregiver when safe. A multisite RCT in children with sexual-abuse-related PTSD symptoms found TF-CBT superior to child-centred therapy on PTSD and related outcomes.[10][12]
PRACTICE components (memorise for exams):
- Psychoeducation and Parenting skills
- Relaxation
- Affective modulation
- Cognitive coping
- Trauma narrative and cognitive processing
- In vivo mastery of trauma reminders
- Conjoint child–parent sessions
- Enhancing safety and future development
Dosage and trauma-narrative modularity have been studied: both shorter and longer TF-CBT courses and variations with/without full narrative components can help, with clinical judgment about complexity guiding intensity — do not use "no narrative ever" as a permanent avoidance strategy when the child is safe enough to process.[11]
AACAP practice parameters endorse trauma-focused psychological treatments as central for paediatric PTSD, with careful assessment, family involvement and attention to safety.[12]
Other psychological options
- Child–parent psychotherapy and attachment-based models for younger children.
- Adolescent adaptations of prolonged exposure / trauma-focused CBT; EMDR where trained.
- Skills then trauma processing sequences (STAIR-informed concepts) have adult RCT support for childhood-abuse-related PTSD and inform complex adolescent presentations — skills are a bridge, not endless delay.[14]
- Family work, school liaison, and treatment of caregiver mental illness/substance use as part of prevention of recurrence.[5]
Pharmacotherapy — adjunct only
Medication does not replace protection or TF-CBT. When used for comorbid depression, anxiety or PTSD-range symptoms in adolescents, SSRIs may be considered with shared decision-making and close monitoring for activation and suicidality. Adult PTSD pharmacotherapy evidence (e.g. sertraline) informs but does not automatically transfer paediatric dosing — individualise by age, weight, product information and specialist CAMHS practice.[12][16]
| Context | Exam-level example | Monitoring |
|---|---|---|
| Adolescent PTSD/depression adjunct | Sertraline start often discussed around 25–50 mg orally daily, titrate carefully under specialist supervision | Early review for activation, suicidality, GI/sexual effects; parallel therapy |
| Avoid as default | Long-term benzodiazepines for core trauma hyperarousal | Dependence, interference with extinction learning |
| Comorbid ADHD | Stimulant only after safety and trauma formulation — do not miss trauma as "just ADHD" | Appetite, sleep, growth, misuse risk |
Prevention and public health
Selected prevention programmes (notably home-visiting models such as Nurse-Family Partnership in the prevention literature) show signals for reducing maltreatment and associated impairment; parenting programmes and multi-component early support are part of the public-health stack. Secondary prevention after maltreatment includes stable safe care, treatment of caregiver problems, and access to trauma therapy for the child.[5]
Australian and New Zealand practice expects mandatory notification frameworks under state/territory or national child-protection law, cultural safety for Aboriginal and Torres Strait Islander and Māori children (over-representation in protection systems requires both vigilance against bias and refusal to under-protect), and trauma-informed CAMHS models with TF-CBT availability as a quality marker.[4][12]
Specific subtypes and scenarios
Sexual abuse disclosure. Believe, document verbatim, medical/forensic pathway, protect from perpetrator access, minimise repeated interviews, TF-CBT when stable enough.[10][12]
Chronic neglect. Multi-agency support of basic needs, developmental assessment, attachment-focused work; removal only when thresholds and legal processes demand — examine both under- and over-intervention risks.[4][5]
IPV-exposed children. Safety planning for the non-offending parent and child; treatment of child trauma symptoms; do not force contact with a violent parent under a naive "both parents equal" mantra when risk remains.[4]
Out-of-home care. Placement instability is itself traumatic; prioritise relational stability, trauma-informed residential practice, and continuity of schooling and therapy.[4]
Adolescent historical childhood abuse. Assess current risk (is the perpetrator still around younger siblings?), adult-like informed consent concepts with developmental competence, and TF-CBT/trauma-focused options adapted for teens.[12]
Complications and pitfalls
- Failure to report when the legal threshold is met; or reporting without reasonable basis as punitive practice.
- Retraumatising or repeatedly interviewing without multi-agency coordination.
- Treating only symptoms while the child remains in danger.[4]
- ACE score as destiny, stigma, or sole screening without clinical context.[1][9]
- Pathologising poverty as neglect without careful assessment; conversely, ignoring neglect because of "cultural relativism" that abandons the child.
- Endless generic support without access to TF-CBT when indicated.[10][11]
- Secondary trauma and boundary failures in clinicians without supervision.[13]
Prognosis and disposition
Meaningful recovery is achievable when safety is secured and evidence-based trauma therapy is delivered. Worse course associates with ongoing threat, polyvictimisation, untreated caregiver psychopathology, substance use, severe dissociation and placement chaos. Disposition ladder: primary care and community TF-CBT; specialist trauma CAMHS; multi-agency protection plans; intensive outreach; inpatient care when suicide or severe self-harm risk demands. Adult transition planning matters for adolescents with high ACE load and ongoing symptoms.[4][6][9][10]
Special populations
Infants and preschoolers. Observation, caregiver–child intervention, developmental pediatrics interface; limited role for verbal TF-CBT until language capacity allows adapted protocols.[12]
Intellectual disability / communication difference. Higher maltreatment risk; adapted communication; do not dismiss behavioural change as "just the disability".[4]
Indigenous and culturally diverse families. Cultural safety, community supports, interpreter use; examine structural drivers of system contact; neither over-surveil nor under-protect.[4][13]
Refugee and asylum-seeking children. War/torture trauma plus possible maltreatment; interpreter; legal stressors as ongoing threat modifiers.[4]
Evidence, guidelines and controversies
Landmark threads: Felitti ACE study; Dube ACE–suicide; Anda neurobiology–epidemiology convergence; Gilbert Lancet burden series; MacMillan prevention; Norman long-term consequences meta-analysis; Teicher ecophenotype and neurobiology reviews; Hughes multi-ACE meta-analysis; Cohen multisite TF-CBT RCT; Deblinger narrative/dosage trial; AACAP PTSD practice parameter; Harris/Fallot trauma-informed design; Cloitre STAIR for childhood-abuse PTSD; ICD-11 stress disorders proposals.[1][2][3][4][5][6][7][8][9][10][11][12][13][14][15]
Controversies to defend both sides. Universal ACE screening versus targeted trauma assessment; mandatory prolonged "stabilisation only" versus timely TF-CBT when safe; self-report epidemiology versus substantiation rates; how far services should go before statutory removal.[1][5][11]
Exam pearls
PROTECT
- Exposure vs diagnosis: maltreatment is not a DSM code; name the mental disorder and the protection action separately.[12]
- ACE = graded risk, not destiny.[1][9]
- TF-CBT PRACTICE — spell every letter in the viva.[10][11]
- Do not process trauma in an actively unsafe home.[12]
- Sertraline-class adjuncts only for comorbidity with monitoring — never a substitute for safety or TF-CBT.[12][16]
- CASC first moves: calm non-leading language, explain confidentiality limits when reporting, validate the child, name next multi-agency steps.
Self-test: 30-second viva opener
"Childhood maltreatment includes physical, sexual and emotional abuse and neglect, often with polyvictimisation and household adversities counted as ACEs. I assess with a trauma-informed private child interview, collateral and risk, and I notify statutory services when there is reasonable suspicion. Safety first — then TF-CBT using PRACTICE components with a safe non-offending caregiver, multi-agency support, and medication only as an adjunct for comorbidity. ACE scores show graded risk, not destiny, and trauma-informed care is system redesign, not a soft alternative to evidence-based therapy."[1][4][10][12][13]
References
- [1]Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study Am J Prev Med, 1998.PMID 9635069
- [2]Dube SR, Anda RF, Felitti VJ, et al. Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: findings from the Adverse Childhood Experiences Study JAMA, 2001.PMID 11754674
- [3]Anda RF, Felitti VJ, Bremner JD, et al. The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology Eur Arch Psychiatry Clin Neurosci, 2006.PMID 16311898
- [4]Gilbert R, Widom CS, Browne K, et al. Burden and consequences of child maltreatment in high-income countries Lancet, 2009.PMID 19056114
- [5]MacMillan HL, Wathen CN, Barlow J, et al. Interventions to prevent child maltreatment and associated impairment Lancet, 2009.PMID 19056113
- [6]Norman RE, Byambaa M, De R, et al. The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis PLoS Med, 2012.PMID 23209385
- [7]Teicher MH, Samson JA Childhood maltreatment and psychopathology: A case for ecophenotypic variants as clinically and neurobiologically distinct subtypes Am J Psychiatry, 2013.PMID 23982148
- [8]Teicher MH, Samson JA Annual Research Review: Enduring neurobiological effects of childhood abuse and neglect J Child Psychol Psychiatry, 2016.PMID 26831814
- [9]Hughes K, Bellis MA, Hardcastle KA, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis Lancet Public Health, 2017.PMID 29253477
- [10]Cohen JA, Deblinger E, Mannarino AP, Steer RA A multisite, randomized controlled trial for children with sexual abuse-related PTSD symptoms J Am Acad Child Adolesc Psychiatry, 2004.PMID 15187799
- [11]Deblinger E, Mannarino AP, Cohen JA, et al. Trauma-focused cognitive behavioral therapy for children: impact of the trauma narrative and treatment length Depress Anxiety, 2011.PMID 20830695
- [12]Cohen JA, Bukstein O, Walter H, et al. Practice parameter for the assessment and treatment of children and adolescents with posttraumatic stress disorder J Am Acad Child Adolesc Psychiatry, 2010.PMID 20410735
- [13]Harris M, Fallot RD Designing trauma-informed addictions services New Dir Ment Health Serv, 2001.PMID 11291263
- [14]Cloitre M, Stovall-McClough KC, Nooner K, et al. Treatment for PTSD related to childhood abuse: a randomized controlled trial Am J Psychiatry, 2010.PMID 20595411
- [15]Maercker A, Brewin CR, Bryant RA, et al. Diagnosis and classification of disorders specifically associated with stress: proposals for ICD-11 World Psychiatry, 2013.PMID 24096776
- [16]Brady K, Pearlstein T, Asnis GM, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial JAMA, 2000.PMID 10770145