Psych · Child and adolescent psychiatry — family and prevention
Children of parents with mental illness
Also known as COPMI · CPMI · Children of parents with mental illness · Offspring of parents with mental illness · Parental mental illness and child outcomes · Family-focused practice adult mental health
Exam-exhaustive fellowship reference on children of parents with mental illness — epidemiology, multi-pathway risk transmission, assessment of parenting capacity, dual loyalty and child-protection interface, STAR*D-child parental remission effects, Beardslee-style preventive family intervention, and multi-agency care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Children of parents with mental illness sit at the interface of adult mental health, CAP, public health prevention, and safeguarding. Examiners test whether you ask about dependent children, can quote order-of-magnitude prevalence and multi-outcome risk, distinguish parenting capacity from diagnosis, name preventive evidence (STAR*D-child; Beardslee; Siegenthaler), and manage dual loyalty without inventing statute numbers.[1][2][6][7][8]
Overview and definition
COPMI (also CPMI) refers to dependent children living with or cared for by a parent with a diagnosable mental disorder. The construct is ecological, not a single DSM-5-TR or ICD-11 child diagnosis. The child may be well, stressed, parentified, or already disordered.[1]
Family-focused practice means adult mental health services identify parental role, assess impact on children, share information proportionately, and offer or refer to psychoeducation, parenting support, and child services — not treating the identified adult in isolation.[1]
Classification and risk ecology
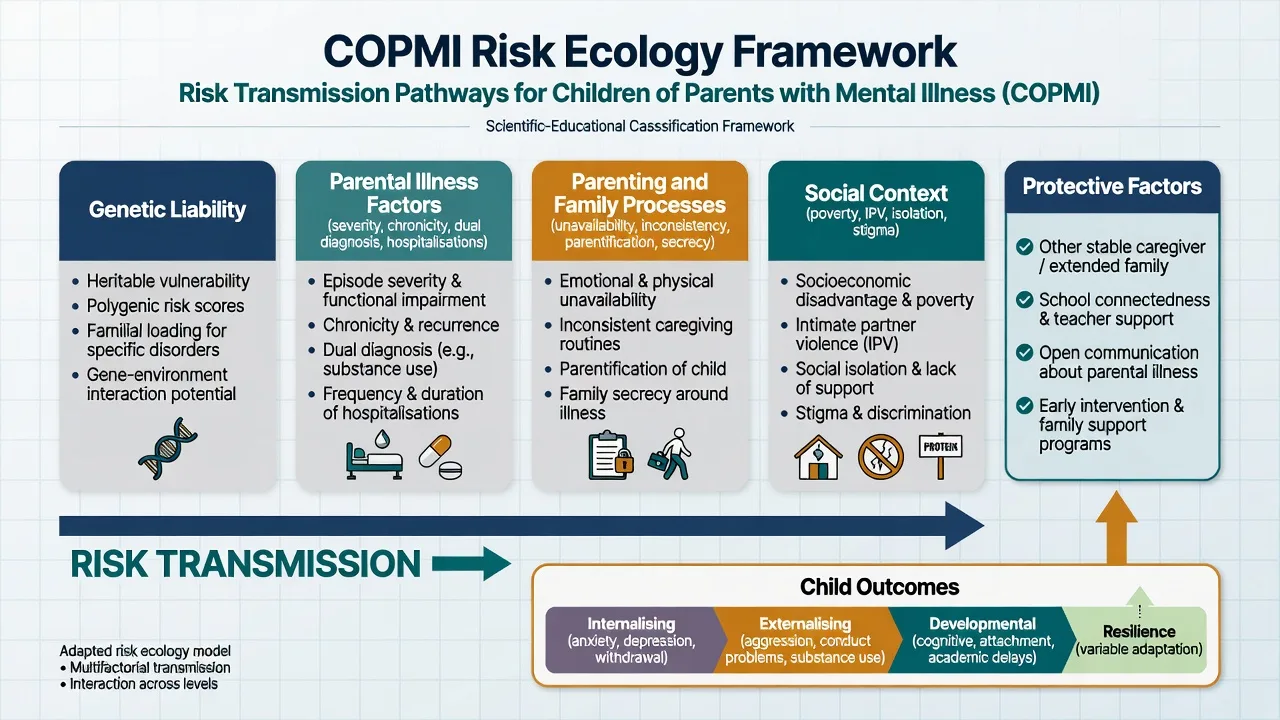
Genetic liability
- Diagnosis-specific and general psychopathology risk
- High-risk offspring designs
- Not destiny alone
Parental illness factors
- Severity, chronicity, dual diagnosis
- Hospitalisations and insight
- Acute vs residual symptoms
Parenting processes
- Emotional unavailability
- Inconsistency, hostility, overprotection
- Parentification and secrecy
Social context
- Poverty, housing, isolation
- IPV and substance co-use
- Stigma and service barriers
Protective factors
- Other competent caregiver
- School connectedness
- Open age-appropriate communication
- Early family intervention
Epidemiology and risk
Australian work synthesised by Reupert and colleagues frames up to about one in five young people living in families with a parent who has a mental illness, with substantial unmet need for family-inclusive care.[1] Population estimates in related Australian analyses place roughly one in four to one in five children in households with parental non-substance mental illness — use as order-of-magnitude exam knowledge, not a single universal percentage dogma.[1]
Family high-risk meta-analysis (Rasic): offspring of parents with schizophrenia, bipolar disorder, or major depressive disorder show substantially increased risk across a range of psychiatric disorders; synthesis of high-risk literature emphasises that a large minority may develop severe mental illness by early adulthood — elevated risk, not certainty.[2]
Transdiagnostic risk (Uher 2023): large meta-analysis of family high-risk and registry studies shows increased same-disorder and cross-disorder risk in offspring of parents with anxiety, psychotic, bipolar, depressive, and substance-use disorders.[3]
Registry spectrum (Dean): parental mental disorder history associates with a full spectrum of offspring psychiatric outcomes, not only the parent's diagnosis.[4]
Multigenerational depression (Weissman): three-generation high-risk studies show elevated depression risk across generations and earlier onset patterns in high-risk lineages — long clinical horizons for surveillance and prevention.[11]
Mechanisms of transmission
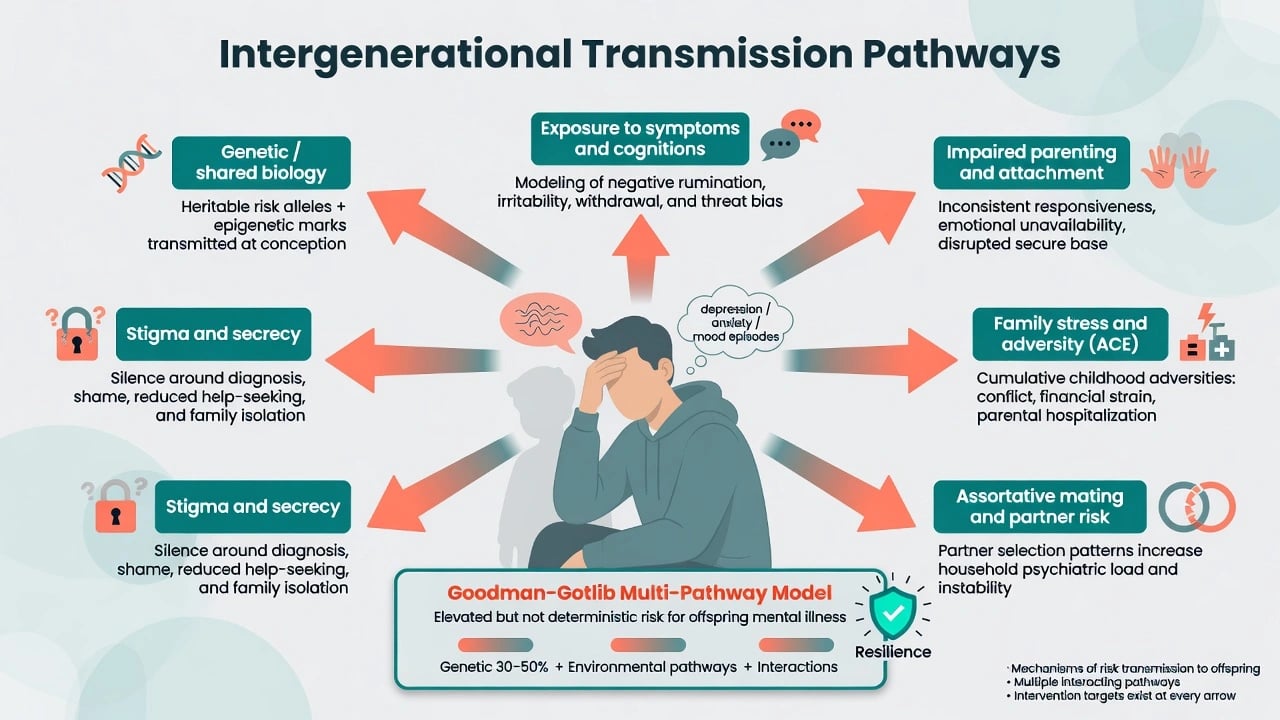
Goodman and Gotlib's developmental model for children of depressed mothers remains the exam-ready mechanism scaffold: heritability; exposure to parental negative affect, cognitions, and behaviours; stress generation; and family and contextual disruption. Extend the same multi-pathway logic to other parental disorders.[5]
Adversity literature links household mental illness and related dysfunction to long-term health risk (ACE framework) and to neurodevelopmental stress pathways summarised in adversity neuroscience reviews.[9][12] When parenting becomes persistently harmful (emotional abuse or neglect), Glaser's psychological maltreatment framework and broader maltreatment burden literature become relevant to threshold reasoning.[10][16]
Clinical presentation
Presentations span adult inpatient wards, community adult MH, CAMHS, schools, ED, and perinatal services.[1]
Child and adolescent signals: anxiety and low mood; somatic complaints; school decline; sleep change; hypervigilance to parental mood; secrecy; role reversal (young carer); caretaking of siblings; externalising behaviour; adolescent self-harm or substance use.[1][5]
Adult service signals: parent never asked about children; notes silent on childcare during admission; partner or grandparents covertly providing all care; child brought to adult appointments and used as emotional support.[1]
MSE caveat. A single normal MSE in a well-dressed schoolchild does not exclude cumulative risk. Longitudinal ecology and multi-agency information matter.[1][5]
Differential diagnosis
Primary child disorder
- ADHD, ASD, mood, anxiety can co-occur
- Family history raises prior probability
- Treat the child's disorder on merits
Stress / adjustment
- Parental admission, relapse, conflict
- May remit with stabilisation and support
- Still assess safety
Maltreatment threshold
- Significant harm from neglect/abuse
- Not every suboptimal parent meets threshold
- Emotional abuse can be invisible
Cultural caregiving
- Collective care is not pathology
- Culture never excuses significant harm
- Independent interpreter
Avoid equating parental diagnosis with child disorder, and avoid dismissing child symptoms as "just the family." Both false negatives and false positives fail exams.[1][10][16]
Assessment
Core questions in every adult assessment. Do you have children under 18? Who lives with them? Who provides day-to-day care? Does anyone else know about your illness? What happens if you need admission? Any concerns about safety, school, or the child's mood?[1]
Parenting capacity is multi-dimensional (basic care, safety, emotional warmth, stimulation, guidance and boundaries, stability). It is time-varying and can improve with treatment. It is not the same construct as medical decision-making capacity (understand, appreciate, reason, communicate), though both may need assessment.[14][1]
See the child when indicated and developmentally appropriate; use open, non-leading enquiry; document facts; map school and GP information; assess sibling risk and parentification.[1][10]
Investigations
There is no laboratory marker of COPMI risk. Investigate medically when neglect, injury, failure to thrive, or fabricated illness is suspected. Use age-appropriate symptom scales as adjuncts for the child. Optimising parental diagnosis (including substance use and medical differentials) is part of secondary prevention for the child.[1][6][10]
Acute and emergency management
Coordinate parental psychiatric emergency care with explicit childcare arrangements (other parent, kinship, emergency placement principles under local law). Assess adolescent self-harm risk in parallel. Report on reasonable suspicion of significant harm via designated channels — jurisdiction-specific duties; do not invent statute section numbers.[1][10][14]
Definitive management
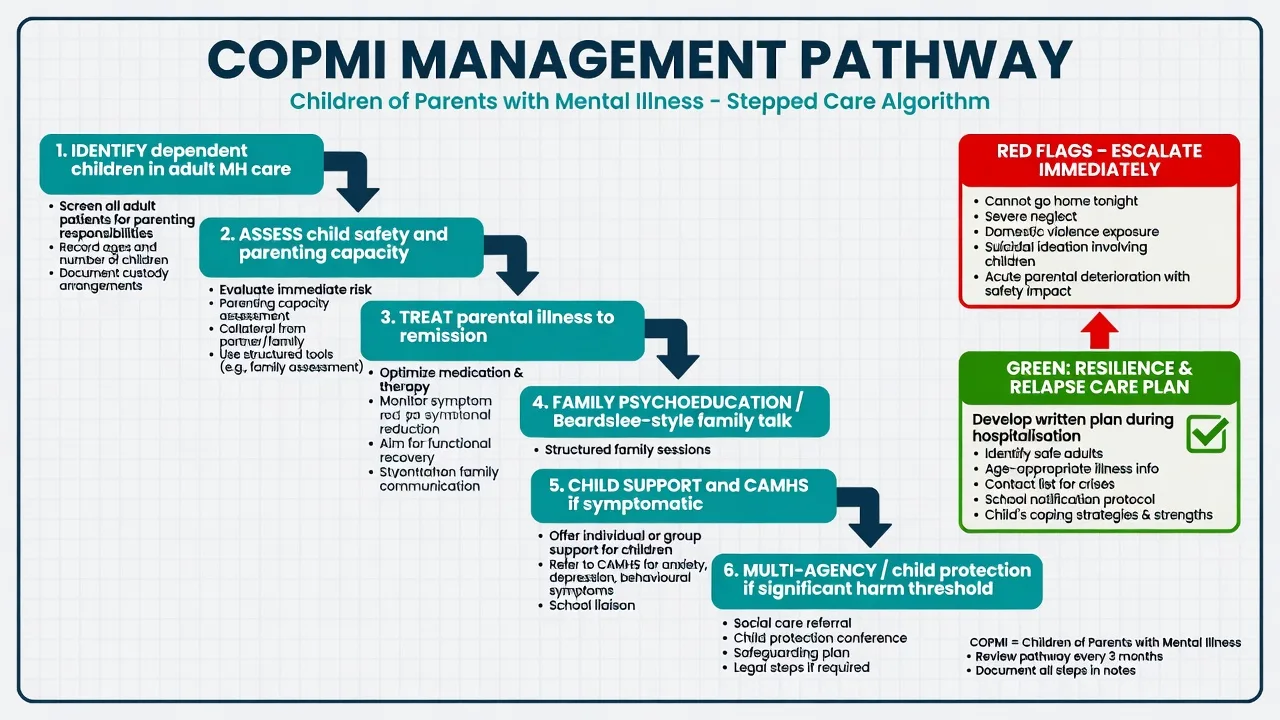
1. Treat the parent — child-facing prevention
STAR*D-child demonstrated that remission of maternal depression was associated with reductions in child psychopathology compared with non-remission — treating parental illness is a child mental health intervention, not only adult care.[6] Apply the principle across disorders: optimise parental treatment, adherence, and relapse prevention with the children's ecology in mind.[1][6]
2. Family-focused preventive intervention
Beardslee's family-based clinician-facilitated approach (Family Talk tradition) targets parental and child change through psychoeducation, linking parental illness to family life, and fostering resilience narratives in at-risk children of depressed parents.[7]
Siegenthaler and colleagues' systematic review and meta-analysis found that preventive interventions for mentally ill parents can reduce mental disorders and psychological symptoms in offspring — exam-nameable evidence that prevention is not hand-waving.[8]
3. Parenting and early adversity support
Where neglect risk and early adversity are high, nurse home-visitation models (Olds) have randomised long-term evidence on maternal life course and reduced child abuse reports — cite as principle-level prevention architecture alongside mental health treatment.[15]
4. Child-directed care when symptomatic
Treat emerging anxiety, depression, trauma symptoms, and self-harm on their own evidence bases. Trauma-focused CBT adaptations are relevant when maltreatment or complex trauma coexists.[13] School liaison and young-carer supports reduce load.
5. Stepped multi-agency intensity
| Level | Actions | When |
|---|---|---|
| Universal family-inclusive | Ask about children; psychoeducation; relapse childcare plan | All adult MH patients with dependents |
| Targeted prevention | Beardslee-style family work; parenting support; school link | Elevated risk, still below statutory threshold |
| Child treatment | CAMHS/primary care for symptomatic child | Emerging disorder or impairment |
| Statutory protection | Multi-agency report and plan | Significant harm occurring or likely |
| Framework for exams; follow local governance.[1][7][8][10] |
RANZCP and local COPMI programme traditions emphasise family-inclusive adult mental health, prevention, and culturally safe practice including for Aboriginal and Torres Strait Islander and Maori families. Child-protection duties remain state/territory and jurisdiction-specific — describe principles, not invented sections. Australian prevalence teaching commonly uses the "around one in five" Reupert/Maybery framing.[1]
Subtypes and high-yield scenarios
Parental psychosis/schizophrenia. Genetic elevation plus positive-symptom disruption of caregiving; always plan childcare for admission; monitor offspring for broad psychopathology, not only psychosis.[2][3]
Parental bipolar. Mood-congruent shifts in energy, impulsivity, and overnight care quality; educate families about early relapse signs that affect parenting.[2][3]
Parental depression. Highest volume pathway; STAR*D-child and Beardslee prevention are core citations.[6][7]
Personality disorder / complex trauma in parent. Emotional dysregulation, boundary violations, attachment impact; assess emotional abuse thresholds carefully.[16][10]
Dual diagnosis (substance + mental illness). Compounding neglect and IPV risk; integrated care and higher safeguarding vigilance.[3][10]
Perinatal parental illness. Mother–baby unit interface, bonding, and infant safety; treat parental illness while protecting the infant.[1][6]
Complications and pitfalls
- Never asking about children in adult assessments.[1]
- Equating diagnosis with automatic permanent removal — or minimising clear risk to preserve alliance.[1][14]
- Colluding with secrecy that leaves children unsupported.[1][7]
- Treating parent only, or child only, without a family plan.[1][6]
- Missing siblings after one disclosure; missing young-carer burden.[1]
- Inventing legal section numbers; or ignoring real mandatory reporting principles.[10]
- Fatalism ("genetic destiny") that blocks prevention that has meta-analytic support.[8][2]
Prognosis and disposition
Risk is elevated across homotypic and heterotypic outcomes but many offspring remain well. Resilience factors (other caregiver, open communication, school connectedness, early intervention, parental remission) matter clinically and in viva answers.[1][2][3][6][8]
Disposition requires named adult and child supports, a relapse childcare plan, review intensity matched to risk, and multi-agency ownership when a protection plan is active. Multigenerational data justify long-horizon prevention thinking without therapeutic nihilism.[11][1]
Special populations
Infants: observation, attachment, developmental surveillance, urgent safety if care collapses.[1][12] School-age: academic and peer impacts; school as key informant.[1] Adolescents / young carers: self-harm risk, confidentiality limits when significant harm, carer burden support.[1][13] Disability/ID in child: higher vulnerability; harder disclosure.[10] Looked-after / kinship after parental illness: placement stability and trauma care.[10][13] Indigenous and CALD families: culturally safe practice and independent interpreters; still protect from significant harm.[1][10]
Exam pearls
COPMI SAFE plan
References
- [1]Reupert AE, Maybery DJ, Kowalenko NM Children whose parents have a mental illness: prevalence, need and treatment Med J Aust, 2013.PMID 25369850
- [2]Rasic D, Hajek T, Alda M, Uher R Risk of mental illness in offspring of parents with schizophrenia, bipolar disorder, and major depressive disorder: a meta-analysis of family high-risk studies Schizophr Bull, 2014.PMID 23960245
- [3]Uher R, Pavlova B, Radua J, et al. Transdiagnostic risk of mental disorders in offspring of affected parents: a meta-analysis of family high-risk and registry studies World Psychiatry, 2023.PMID 37713573
- [4]Dean K, Stevens H, Mortensen PB, et al. Full spectrum of psychiatric outcomes among offspring with parental history of mental disorder Arch Gen Psychiatry, 2010.PMID 20679590
- [5]Goodman SH, Gotlib IH Risk for psychopathology in the children of depressed mothers: a developmental model for understanding mechanisms of transmission Psychol Rev, 1999.PMID 10467895
- [6]Weissman MM, Pilowsky DJ, Wickramaratne PJ, et al. Remissions in maternal depression and child psychopathology: a STAR*D-child report JAMA, 2006.PMID 16551710
- [7]Beardslee WR, Gladstone TR, Wright EJ, Cooper AB A family-based approach to the prevention of depressive symptoms in children at risk: evidence of parental and child change Pediatrics, 2003.PMID 12897317
- [8]Siegenthaler E, Munder T, Egger M Effect of preventive interventions in mentally ill parents on the mental health of the offspring: systematic review and meta-analysis J Am Acad Child Adolesc Psychiatry, 2012.PMID 22176935
- [9]Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults. The Adverse Childhood Experiences (ACE) Study Am J Prev Med, 1998.PMID 9635069
- [10]Gilbert R, Widom CS, Browne K, et al. Burden and consequences of child maltreatment in high-income countries Lancet, 2009.PMID 19056114
- [11]Weissman MM, Berry OO, Warner V, et al. A 30-year study of 3 generations at high risk and low risk for depression JAMA Psychiatry, 2016.PMID 27532344
- [12]Teicher MH, Samson JA Annual Research Review: Enduring neurobiological effects of childhood abuse and neglect J Child Psychol Psychiatry, 2016.PMID 26831814
- [13]Cohen JA, Mannarino AP, Kliethermes M, Murray LA Trauma-focused CBT for youth with complex trauma Child Abuse Negl, 2012.PMID 22749612
- [14]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [15]Olds DL, Eckenrode J, Henderson CR Jr, et al. Long-term effects of home visitation on maternal life course and child abuse and neglect. Fifteen-year follow-up of a randomized trial JAMA, 1997.PMID 9272895
- [16]Glaser D Emotional abuse and neglect (psychological maltreatment): a conceptual framework Child Abuse Negl, 2002.PMID 12201163