Psych · Child and adolescent psychiatry — disruptive behaviour
Conduct and oppositional defiant disorders
Also known as Oppositional defiant disorder · ODD · Conduct disorder · CD · Disruptive behaviour disorders · Disruptive behavior disorders · Antisocial behaviour in youth · Callous-unemotional traits · Limited prosocial emotions
Exam-exhaustive fellowship reference on oppositional defiant disorder and conduct disorder — DSM-5-TR and ICD-11 criteria, Moffitt trajectories, ADHD and ASPD interfaces, multi-informant assessment, parent management training, multisystemic therapy concepts, and the limited evidence-based role of medication for severe aggression. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Oppositional defiant disorder (ODD) and conduct disorder (CD) are high-yield child and adolescent psychiatry topics across FRANZCP, MRCPsych, ABPN and MD/DNB. Examiners test operational criteria, the ODD–CD–ADHD–ASPD developmental story, callous-unemotional / limited prosocial emotions language, multi-informant assessment, parenting and multisystemic psychosocial interventions by name, and the disciplined, limited use of medication for aggression. This topic is written so a candidate who has read nothing else can defend those points at consultant depth.[1][4][6][11]
Overview and definition
ODD and CD sit within the disruptive, impulse-control and conduct disorders. They are not moral verdicts and not interchangeable labels. ODD captures a persistent pattern of angry/irritable mood, argumentative/defiant behaviour, and/or vindictiveness that is developmentally inappropriate and impairing. CD captures a repetitive and persistent pattern of behaviour that violates the basic rights of others or major age-appropriate societal norms or rules — aggression, destruction of property, deceit or theft, and serious violations of rules.[4][5][6]
Formulation first. Criteria open the diagnostic gate; formulation explains coercive family cycles, peer ecology, neurodevelopmental comorbidity (especially ADHD), trauma, and the developmental pathway (life-course-persistent versus adolescence-limited).[1][12][22]
Classification: ODD versus CD
DSM-5-TR — ODD (exam skeleton)
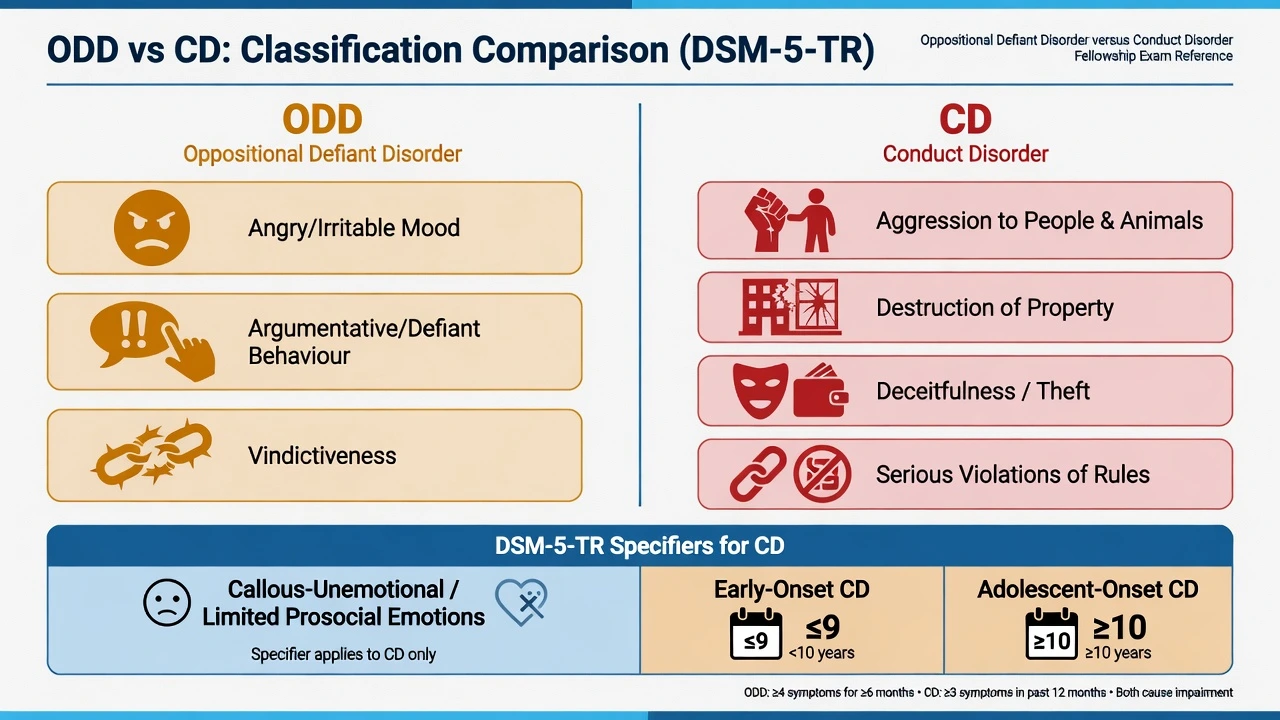
A pattern of angry/irritable mood, argumentative/defiant behaviour, or vindictiveness lasting at least 6 months, evidenced by at least four symptoms from these categories, exhibited during interaction with at least one individual who is not a sibling (wording detail matters in stems), with distress or impairment, and not occurring exclusively during a psychotic, substance, depressive or bipolar episode. Severity is graded by the number of settings (mild one, moderate two, severe three or more).[4]
DSM-5-TR — CD (exam skeleton)
A repetitive and persistent pattern of behaviour in which the basic rights of others or major age-appropriate societal norms or rules are violated, as manifested by the presence of at least three of fifteen criteria in the past 12 months, with at least one criterion present in the past 6 months, across four groups: aggression to people and animals; destruction of property; deceitfulness or theft; serious violations of rules. Specifiers: childhood-onset (at least one criterion before age 10) versus adolescent-onset; severity; and with limited prosocial emotions (lack of remorse or guilt, callous lack of empathy, unconcerned about performance, shallow or deficient affect) when two or more characteristics persist over 12 months in multiple relationships/settings.[5][11]
ICD-11. Oppositional defiant disorder and conduct-dissocial disorder remain related categories; examiners accept that manuals use slightly different wording and that limited prosocial emotions / callous-unemotional features shape risk stratification in both systems. State which manual you are applying when thresholds are examined.[3][12]
ODD can precede or co-occur with CD but is not automatic conversion. Many children with ODD never meet full CD criteria, especially when parenting and ADHD are addressed early.[6][4]
ODD
- Angry/irritable, argumentative, vindictive
- Often home/school authority conflict
- May lack clear criminality
- Parent training highly relevant
Conduct disorder
- Rights of others / major norms violated
- Aggression, theft, destruction, rule-breaking
- Onset and limited prosocial emotions matter
- Higher multiagency intensity
ADHD interface
- Impulsivity fuels oppositionality
- Often comorbid, not differential only
- Treat ADHD when present
- Stimulants can reduce secondary ODD symptoms
ASPD trajectory
- Adult diagnosis ≥18 with CD before 15 (DSM)
- Not inevitable after childhood CD
- LCP + CU + adversity raise risk
- Desistance remains possible
Epidemiology and risk
Numbers and patterns candidates should own
Nock and colleagues estimated substantial lifetime ODD prevalence in the National Comorbidity Survey Replication with high comorbidity and role impairment — exam answers should cite order of magnitude and comorbidity, not false precision from a single clinic sample.[2] Canino and colleagues concluded that methodological factors, more than geography alone, drive much of the cross-cultural variability in CD/ODD prevalence estimates.[3]
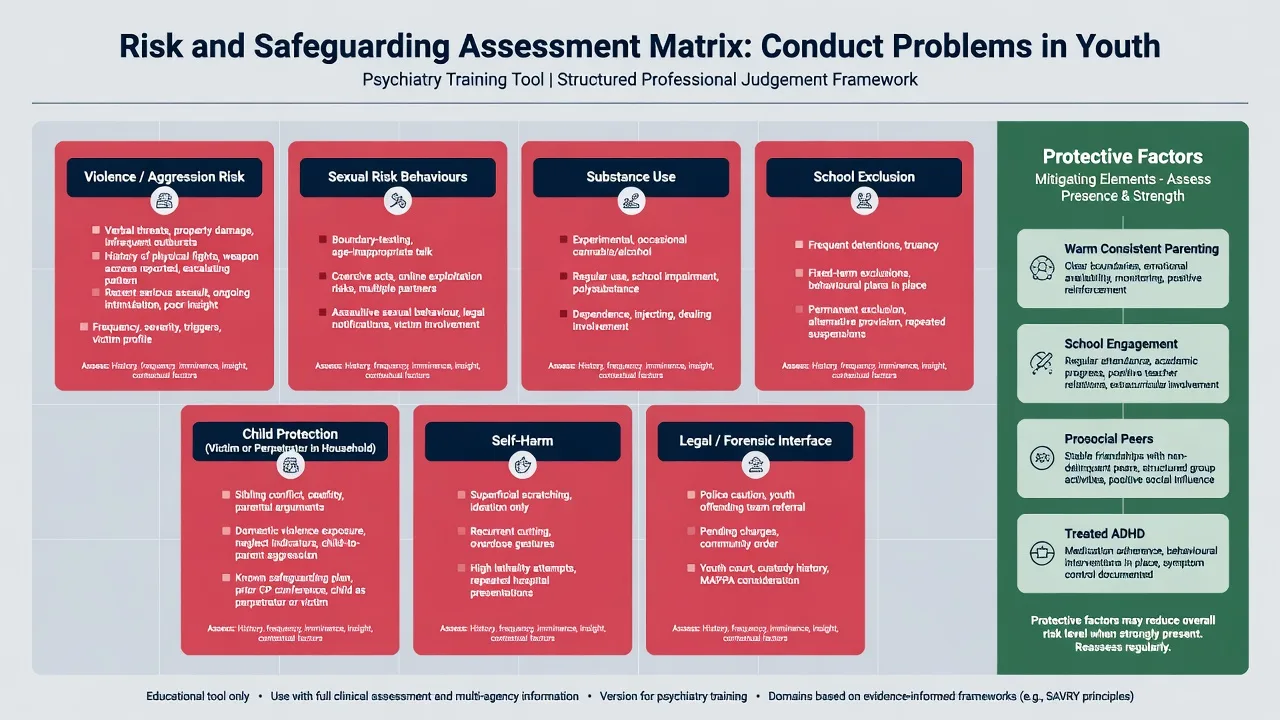
Risk factors. Harsh, inconsistent, or coercive parenting; parental mental illness and substance use; peer delinquency; school failure/exclusion; neighbourhood disadvantage; prenatal smoking and other early neurodevelopmental hits; maltreatment; and ADHD. Protective factors include warm consistent parenting, school engagement, and prosocial peers.[6][8][22]
Pathophysiology and developmental pathways
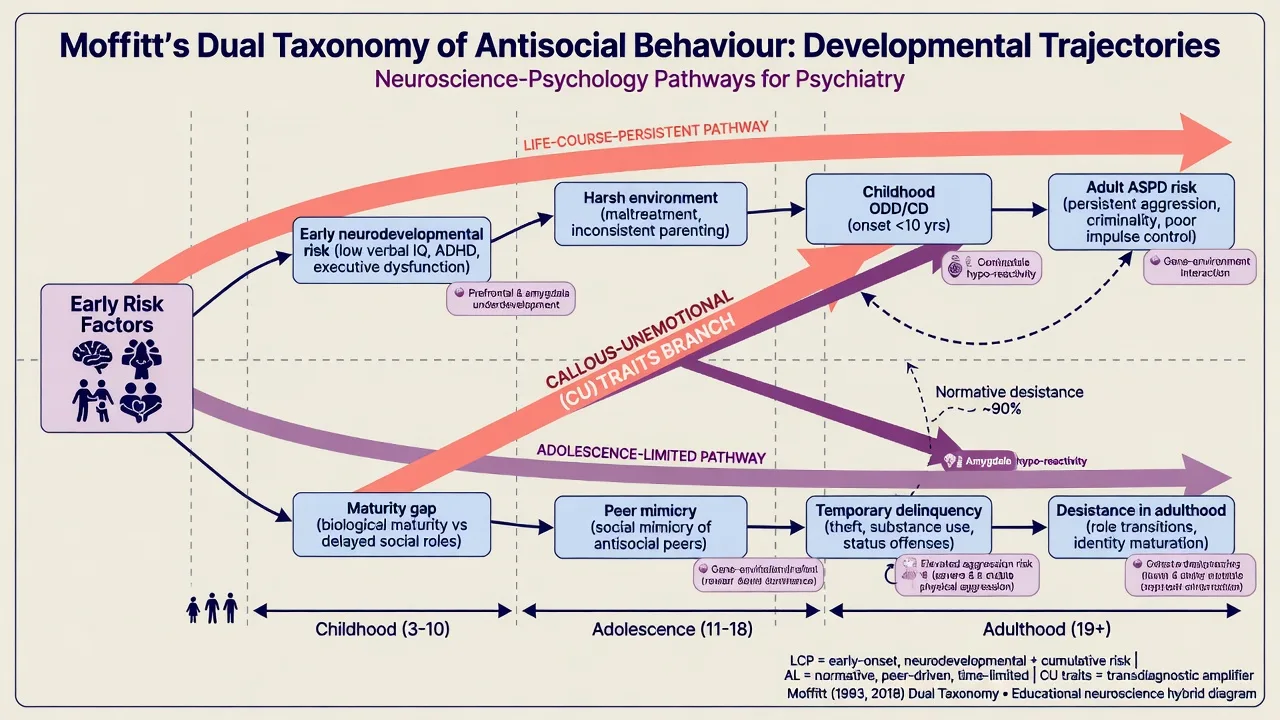
Moffitt dual taxonomy. Life-course-persistent antisocial behaviour begins early, is rooted in the interaction of neuropsychological vulnerability and criminogenic environments, and carries higher risk of adult antisocial outcomes. Adolescence-limited antisocial behaviour is more common, linked to the maturity gap and peer mimicry, and often desists as adult roles open. This remains a viva classic.[1]
Multiple pathways to CD. Pardini and Frick summarise conceptualisations including CU-trait pathways, ADHD/impulsivity pathways, and environmental/coercive pathways — clinically useful because treatment targets differ (empathy/conscience scaffolding and reward contingencies versus impulse control versus parenting ecology).[12][11]
Callous-unemotional traits. Reduced guilt, empathy and concern about performance predict a more severe, stable aggressive phenotype; neurobiological reviews implicate atypical processing of fear and distress cues at group level (not a diagnostic scan).[11][20]
Stringaris dimensions. Oppositionality is not unitary: irritable, headstrong and hurtful dimensions have distinctive longitudinal associations — irritable features track toward emotional disorders; headstrong toward ADHD-type outcomes; hurtful toward more aggressive/conduct outcomes. Use this language when examiners push beyond checklist ODD.[13][14]
Coercive family process. Escape-conditioned cycles (child escalates → parent withdraws demand → negative reinforcement for both) are a core mechanism targeted by parent management training and Oregon-model interventions.[22][8]
Clinical presentation
ODD. Frequent temper loss, touchiness, anger, arguing with adults, active defiance, deliberately annoying others, blaming others, spitefulness. Impairment shows as family conflict, school disciplinary action, and peer rejection — without necessarily meeting CD criterion behaviours.[4]
CD. Fighting, bullying, weapon use, physical cruelty, forced sexual activity, fire-setting, property destruction, breaking and entering, lying for goods/favours, stealing, staying out overnight despite prohibitions (onset before 13 for that criterion), running away, truancy. Severity and onset age frame risk talk with families and multiagency partners.[5][6]
MSE / observation. Hostile attributional bias, limited remorse versus reactive guilt after cooling, superficial charm with CU traits, or chaotic impulsivity with ADHD. Collateral from school and welfare often contradicts a minimising young person.[11][5]
Differential diagnosis
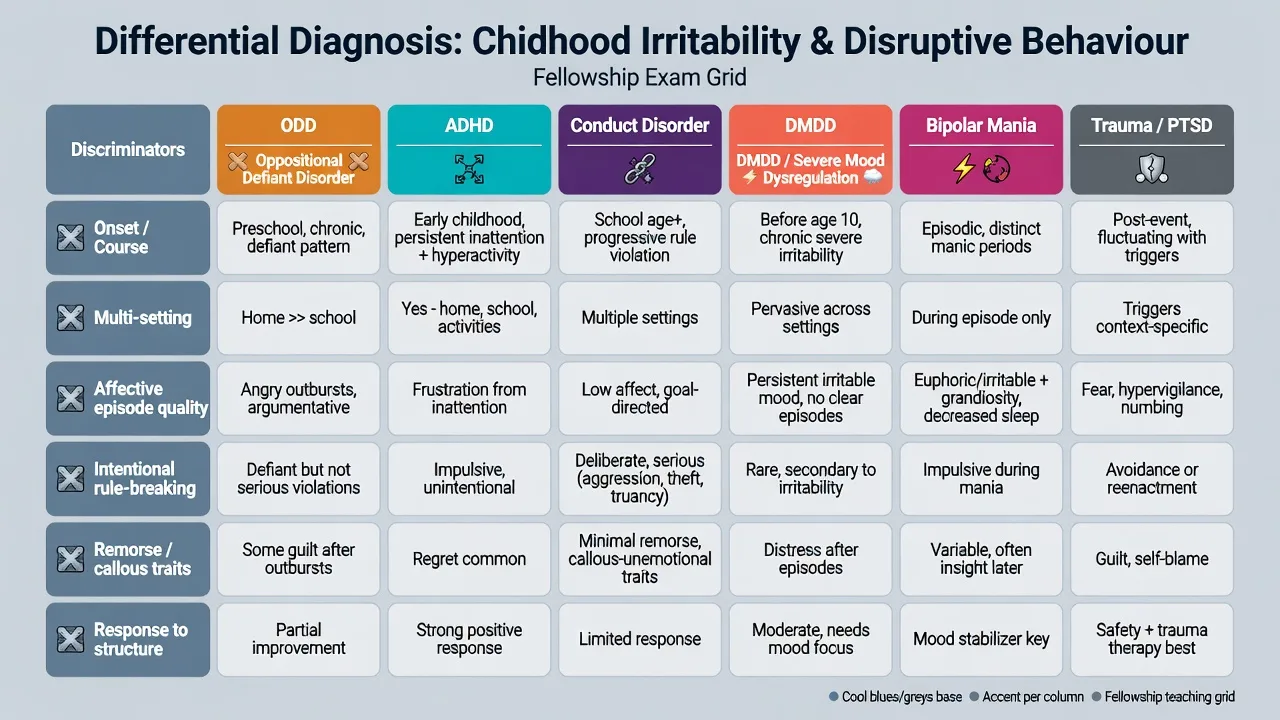
ADHD
- Off-task impulsivity, not only authority defiance
- Often comorbid — treat both
- Stimulant response supports ADHD contribution
- Does not exclude ODD
DMDD / severe mood dysregulation
- Chronic severe temper outbursts + persistent irritability
- Not episodic mania
- Overlaps ODD irritability — hierarchy rules apply in DSM
- Leibenluft boundary literature
Bipolar mania
- Episodic elevated/expansive mood
- Decreased need for sleep, grandiosity
- Not chronic baseline from early childhood alone
- Do not start antipsychotics only for 'mood swings' without formulation
Trauma / ASD / LD
- PTSD hyperarousal and avoidance
- ASD: rigidity and sensory meltdowns
- Language/learning frustration
- Always screen maltreatment
Also keep substance-induced behavioural change, psychosis, intermittent explosive disorder, and culturally contextualised authority conflict on the board. Antisocial personality disorder is an adult diagnosis: DSM requires age 18 or older with evidence of conduct disorder with onset before age 15 — childhood CD raises risk but does not equal inevitable ASPD.[16][21][15]
Assessment
Structure as multi-informant + multi-setting + onset + comorbidity + risk + parenting ecology + legal/safeguarding.[4][5]
- Map ODD and CD criteria with concrete examples and timelines.
- Obtain school reports, attendance, exclusions, and prior assessments.
- Screen ADHD, learning, language, mood, anxiety, ASD traits, substances, sleep.
- Map coercive cycles, parental mental health, domestic violence, and peer network.
- Risk: violence (who/what/when/weapons), sexual harm, fire-setting, self-harm, exploitation, absconding.
- Capacity, consent, and reporting duties — jurisdiction-specific statutes; state principles, do not invent section numbers.[4][5][24]
Rating scales (SDQ, Conners, CBCL externalising, Inventory of Callous-Unemotional Traits in research/specialist settings) support severity tracking; they do not replace clinical diagnosis.[4][11]
Investigations
There is no diagnostic blood test or scan for ODD/CD.[4][5]
Before pharmacotherapy for aggression: height/weight/BMI, BP, fasting metabolic parameters as indicated, review of movement side-effects baseline, and awareness of prolactin-related symptoms if using risperidone; ECG when cardiac history or other risk factors warrant. Urine drug screen when SUD is plausible. Psychoeducational testing when learning disorder is suspected. Imaging/EEG only for neurological red flags.[17][18]
Acute safety and safeguarding
Acute severe aggression uses standard de-escalation and local rapid tranquillisation pathways only when clinically indicated for acute behavioural emergency — not as routine "discipline." Document risk formulation and crisis plan with family and school.[17]
Definitive management
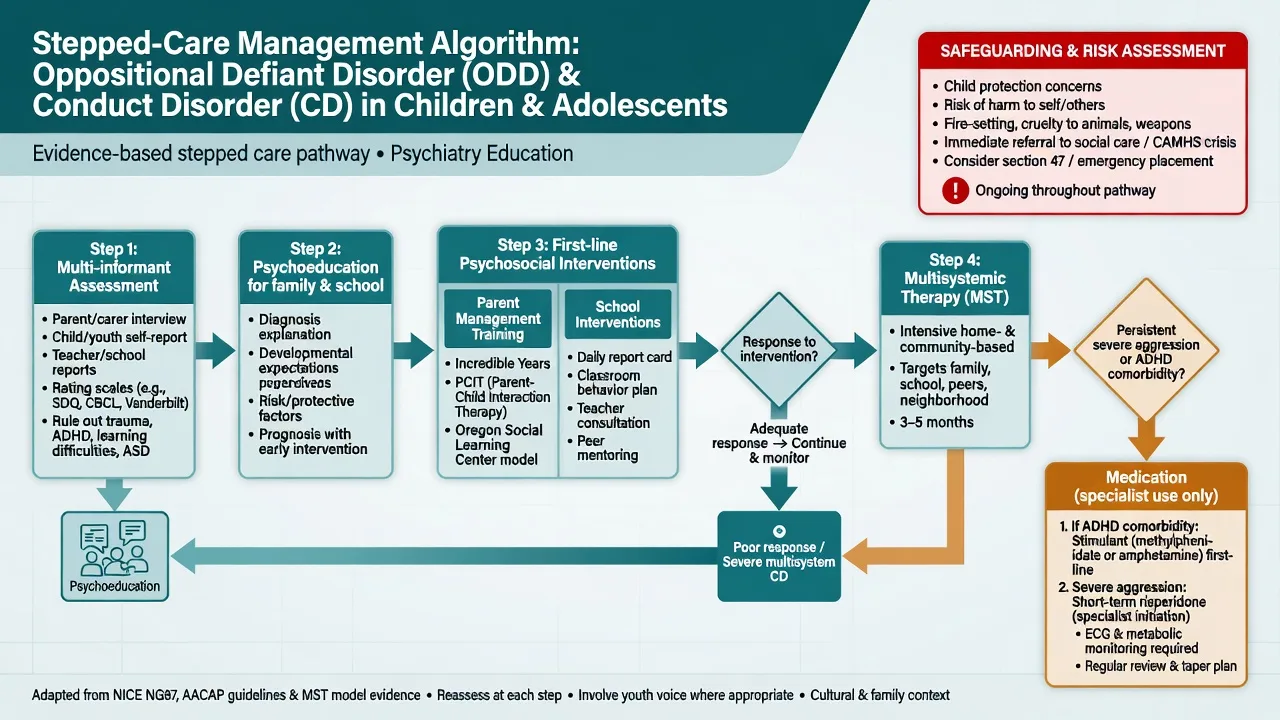
Parenting and behavioural interventions (first-line)
Behavioural parent management training (PMT) and related programmes are the backbone for ODD and early-onset conduct problems: clear instructions, contingent praise, consistent consequences, reduced harsh coercion, and planned ignoring of minor provocations. The Oregon model of behaviour family therapy and Incredible Years–lineage programmes have substantial outcome literature; mediators include improved parenting practices.[7][8][22]
Scott and colleagues showed that parenting groups for childhood antisocial behaviour can work in real clinical practice, not only in efficacy labs — a key exam point against therapeutic nihilism.[7]
Parent–child interaction therapy (PCIT) is particularly relevant for younger children (roughly preschool to early primary): live-coached child-directed and parent-directed interaction sequences targeting attachment warmth and effective discipline.[4]
School interventions (behavioural classroom strategies, consistent expectations, collaborative problem-solving, attendance recovery) should run in parallel; home-only gains often fail at the classroom door.[4][5]
Multisystemic therapy (MST)
For severe, multi-domain adolescent antisocial behaviour — especially justice-involved youth — MST is a high-intensity, home- and community-based ecological intervention targeting family, peers, school and neighbourhood drivers of behaviour, with therapists on call and strong quality-assurance structures. Henggeler's programme of research describes efficacy, transportability and implementation lessons: fidelity matters; "MST-lite" is not the evidence base.[9][10]
Know the concept for exams even if local commissioning differs: ecological assessment, caregivers as primary change agents, removal of antisocial peer reinforcement, and continuous outcome monitoring.[9][10]
Australian and New Zealand CAMHS practice emphasises family-based behavioural work, school liaison, and multiagency care for complex CD, with access to branded MST or functional family therapy varying by jurisdiction and commissioning. Youth justice interfaces and mandatory reporting follow state/territory law — quote principles and local process, not invented national section numbers.[4][24]
Medication — limited, targeted, monitored
Core teaching: There is no specific "ODD pill." Pharmacotherapy is adjunctive for (1) treated comorbidity that drives behaviour (especially ADHD), and/or (2) severe aggression/explosive dyscontrol when psychosocial measures are insufficient and risk is high.[17][4]
ADHD comorbidity. When ADHD is present, optimised stimulant or other ADHD treatment often reduces oppositional symptoms secondary to impulsivity and should be prioritised before chronic antipsychotic exposure for "attitude."[17][6]
Risperidone and related agents for severe aggression. Controlled data support risperidone reducing disruptive and aggressive behaviour in selected populations (including children with subaverage IQ and disruptive behaviour disorders). Typical exam-level frameworks discuss low total daily doses (commonly in the order of 0.25–2 mg/day oral in divided or evening-weighted dosing in paediatric disruptive behaviour trials, titrated slowly) with mandatory monitoring of weight, metabolic parameters, extrapyramidal symptoms, sedation and prolactin-related effects. Always individualise and check local product information.[18][17]
TOSCA lessons. Integration of findings from the Treatment of Severe Childhood Aggression programme supports that in children with ADHD plus severe aggression, optimising stimulant treatment and adding psychosocial intervention is foundational; adjunctive risperidone can help residual severe aggression in selected cases but brings adverse-effect trade-offs — so limit duration, review indication, and do not start dual pharmacotherapy casually.[19]
Canadian guidance on pharmacotherapy for disruptive and aggressive behaviour synthesises a stepped approach: psychosocial first; treat ADHD; consider atypical antipsychotic for severe aggression with monitoring; avoid benzodiazepines as behaviour management tools.[17]
| Target | Prefer | Avoid as first-line |
|---|---|---|
| ODD without severe aggression | PMT / family behavioural work | Antipsychotic for "defiance" |
| ADHD + ODD | Optimise ADHD treatment + PMT | Ignoring ADHD |
| Severe multi-domain CD | MST / intensive multiagency + PMT elements | Outpatient "chat" alone |
| Severe aggression residual | Time-limited risperidone (specialist) with monitoring | Indefinite high-dose antipsychotic without review |
| Acute crisis | De-escalation, safety, local RT pathway if needed | Chronic benzo behaviour control |
| Framework for exams; verify local PI and governance.[7][9][17][18][19] |
Prognosis and trajectory to adult outcomes
Many children with ODD improve substantially with effective parenting interventions. A subset progresses to CD. Childhood-onset CD, especially with CU traits, ADHD, and cumulative adversity, maps onto Moffitt's life-course-persistent pathway and elevates risk of adult antisocial behaviour, substance use, and other psychiatric disorders — but risk is not destiny.[1][11][21][23]
Longitudinal developmental work (including Robins' classic follow-up tradition and modern cohort follow-backs such as Kim-Cohen and Copeland) shows that adult psychiatric disorder often has juvenile antecedents, and that externalising pathways predict later externalising and mixed outcomes — supporting early multi-domain intervention rather than watchful neglect.[15][21][23]
Real-world multi-country data continue to show variation in recognition and management of CD, reinforcing the need for structured assessment rather than informal labelling.[24]
Complications and pitfalls
- Calling cultural assertiveness or trauma-driven defiance "ODD" without multi-setting impairment analysis.[4]
- Missing ADHD, language disorder, or maltreatment.[6]
- Prescribing antipsychotics for mild–moderate ODD without psychosocial work.[17]
- Failing to address peer group and school exclusion drivers (MST logic).[9]
- Assuming all adolescent rule-breaking is life-course-persistent ASPD-in-waiting.[1]
- Neglecting metabolic monitoring once risperidone "works."[18][17]
Special populations
Looked-after and maltreated youth need trauma-informed formulation and care-system stability; behaviour labels without placement and attachment context fail. Intellectual disability populations feature in much of the risperidone disruptive-behaviour trial literature — generalise carefully to typically developing youth. Indigenous and culturally diverse families require culturally safe, non-stigmatising parenting support and partnership with community services. Transition planning is essential when late-adolescent CD with CU traits and justice involvement approaches adult forensic or personality-disorder pathways — still offering desistance-focused interventions.[18][9][21]
Exam pearls
ODD CARE plan
References
- [1]Moffitt TE Adolescence-limited and life-course-persistent antisocial behavior: a developmental taxonomy Psychol Rev, 1993.PMID 8255953
- [2]Nock MK, Kazdin AE, Hiripi E, Kessler RC Lifetime prevalence, correlates, and persistence of oppositional defiant disorder: results from the National Comorbidity Survey Replication J Child Psychol Psychiatry, 2007.PMID 17593151
- [3]Canino G, Polanczyk G, Bauermeister JJ, Rohde LA, et al. Does the prevalence of CD and ODD vary across cultures? Soc Psychiatry Psychiatr Epidemiol, 2010.PMID 20532864
- [4]Steiner H, Remsing L; Work Group on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with oppositional defiant disorder J Am Acad Child Adolesc Psychiatry, 2007.PMID 17195736
- [5]Steiner H Practice parameters for the assessment and treatment of children and adolescents with conduct disorder. American Academy of Child and Adolescent Psychiatry J Am Acad Child Adolesc Psychiatry, 1997.PMID 9334568
- [6]Loeber R, Burke JD, Lahey BB, et al. Oppositional defiant and conduct disorder: a review of the past 10 years, part I J Am Acad Child Adolesc Psychiatry, 2000.PMID 11128323
- [7]Scott S, Spender Q, Doolan M, et al. Multicentre controlled trial of parenting groups for childhood antisocial behaviour in clinical practice BMJ, 2001.PMID 11473908
- [8]Beauchaine TP, Webster-Stratton C, Reid MJ Mediators, moderators, and predictors of 1-year outcomes among children treated for early-onset conduct problems: a latent growth curve analysis J Consult Clin Psychol, 2005.PMID 15982136
- [9]Henggeler SW, Schaeffer CM Multisystemic Therapy: Clinical Overview, Outcomes, and Implementation Research Fam Process, 2016.PMID 27370172
- [10]Henggeler SW Efficacy studies to large-scale transport: the development and validation of multisystemic therapy programs Annu Rev Clin Psychol, 2011.PMID 21443449
- [11]Frick PJ, White SF Research review: the importance of callous-unemotional traits for developmental models of aggressive and antisocial behavior J Child Psychol Psychiatry, 2008.PMID 18221345
- [12]Pardini D, Frick PJ Multiple developmental pathways to conduct disorder: current conceptualizations and clinical implications J Can Acad Child Adolesc Psychiatry, 2013.PMID 23390429
- [13]Stringaris A, Goodman R Three dimensions of oppositionality in youth J Child Psychol Psychiatry, 2009.PMID 19166573
- [14]Stringaris A, Goodman R Longitudinal outcome of youth oppositionality: irritable, headstrong, and hurtful behaviors have distinctive predictions J Am Acad Child Adolesc Psychiatry, 2009.PMID 19318881
- [15]Kim-Cohen J, Caspi A, Moffitt TE, et al. Prior juvenile diagnoses in adults with mental disorder: developmental follow-back of a prospective-longitudinal cohort Arch Gen Psychiatry, 2003.PMID 12860775
- [16]Leibenluft E Severe mood dysregulation, irritability, and the diagnostic boundaries of bipolar disorder in youths Am J Psychiatry, 2011.PMID 21123313
- [17]Gorman DA, Gardner DM, Murphy AL, et al. Canadian guidelines on pharmacotherapy for disruptive and aggressive behaviour in children and adolescents with attention-deficit hyperactivity disorder, oppositional defiant disorder, or conduct disorder Can J Psychiatry, 2015.PMID 25886657
- [18]Snyder R, Turgay A, Aman M, et al. Effects of risperidone on conduct and disruptive behavior disorders in children with subaverage IQs J Am Acad Child Adolesc Psychiatry, 2002.PMID 12218423
- [19]Barterian JA, Arnold LE, Brown NV, et al. Clinical Implications From the Treatment of Severe Childhood Aggression (TOSCA) Study: A Re-Analysis and Integration of Findings J Am Acad Child Adolesc Psychiatry, 2017.PMID 29173736
- [20]Blair RJ The neurobiology of psychopathic traits in youths Nat Rev Neurosci, 2013.PMID 24105343
- [21]Robins LN Deviant children grown up Eur Child Adolesc Psychiatry, 1996.PMID 9010663
- [22]Dishion T, Forgatch M, Chamberlain P, et al. The Oregon Model of Behavior Family Therapy: From Intervention Design to Promoting Large-Scale System Change Behav Ther, 2016.PMID 27993335
- [23]Copeland WE, Shanahan L, Costello EJ, Angold A Childhood and adolescent psychiatric disorders as predictors of young adult disorders Arch Gen Psychiatry, 2009.PMID 19581568
- [24]Bachmann CJ, Scholle O, Bliddal M, et al. Recognition and management of children and adolescents with conduct disorder: a real-world data study from four western countries Child Adolesc Psychiatry Ment Health, 2024.PMID 38281951