Psych · Child and adolescent psychiatry — developmental assessment
Developmental assessment in child psychiatry
Also known as Developmental history · Milestone assessment · Adaptive functioning assessment · Developmental surveillance · Developmental screening · Psychometric assessment CAP · Global developmental delay assessment · Intellectual disability assessment children
Exam-exhaustive fellowship reference on developmental assessment in CAP — structured history, domain milestones, adaptive function co-equal with IQ, screening versus diagnostic psychometrics, multi-source formulation, and multiagency early intervention. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Developmental assessment is high-yield across FRANZCP CAP, MRCPsych, ABPN and MD/DNB because examiners test whether you can take a developmental history, map milestones, treat adaptive function as co-equal with intellectual testing for ID, use tools without confusing screens for diagnoses, and write a formulation that links trajectory to plan. This topic is written so a candidate who has read nothing else can defend those points at consultant depth.[1][5][8][9]
Overview and definition
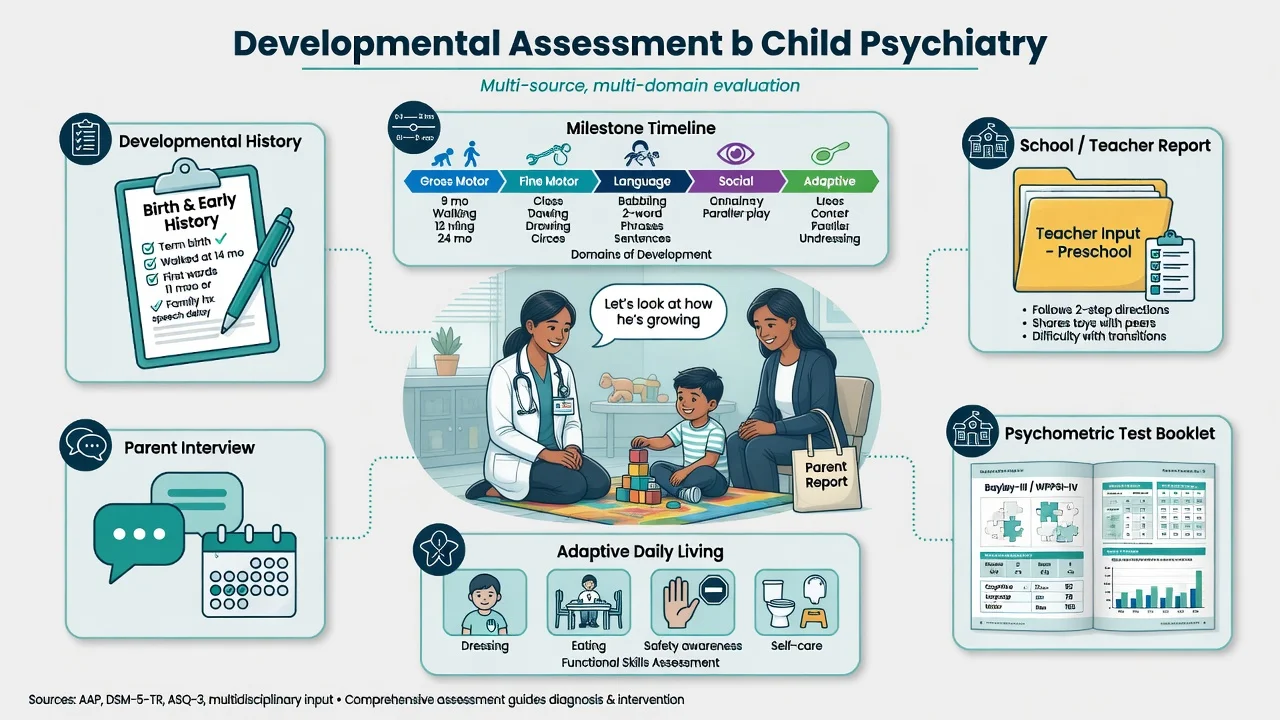
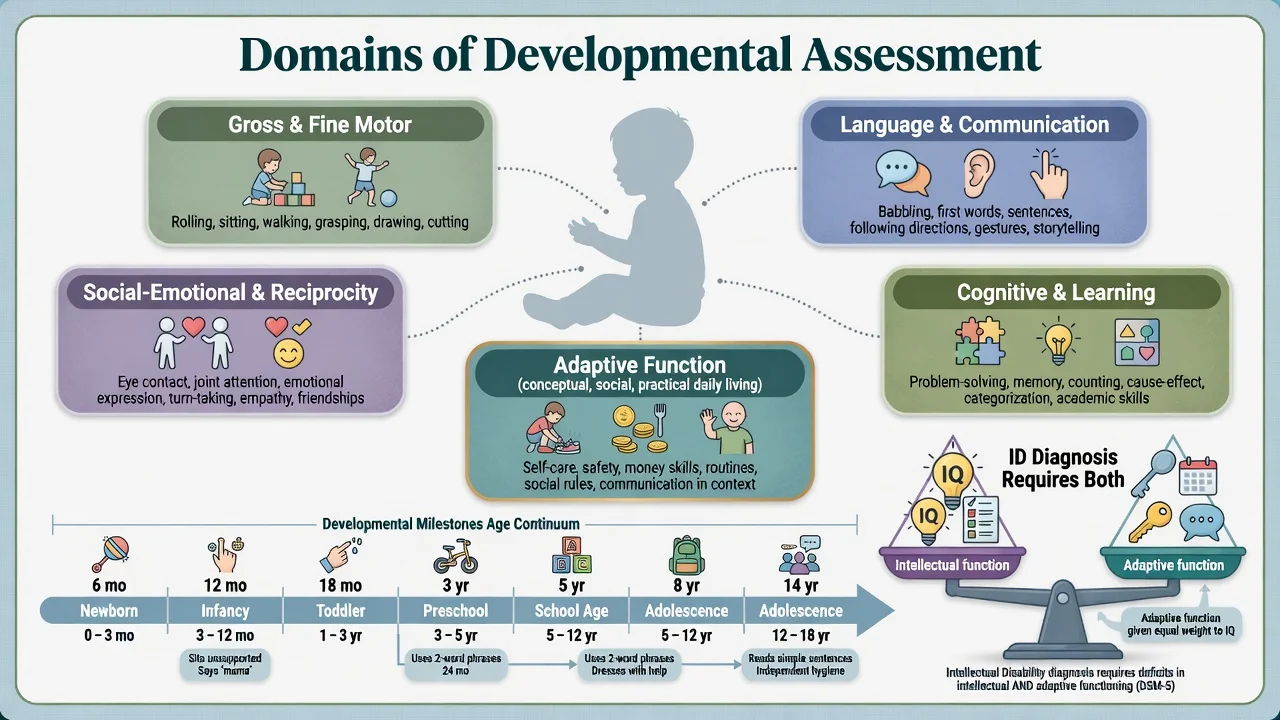
Developmental assessment evaluates a child's trajectory across interrelated domains — gross and fine motor, language and communication, cognitive/learning, social-emotional reciprocity, and adaptive behaviour (conceptual, social, practical skills used in everyday life). It answers: where is this child relative to age expectations, in which domains, with what functional impact, and why? It is not synonymous with "doing a WISC."[1][4][17]
Formulation first. Psychometrics open and close gates; formulation explains aetiology hypotheses, caregiving and school ecology, strengths, cultural-linguistic context, risk, and what to do next. Winters and colleagues frame CAP formulation as the organising clinical product that integrates diagnosis with systems data.[8][9]
Classification framework: surveillance, screening, testing
Three processes examiners expect you to separate
Developmental surveillance is the longitudinal clinical process at every contact: eliciting parental concerns, updating milestones, observing the child, and integrating risk factors. Developmental screening uses standardised instruments at recommended ages (classically including 9, 18 and 30 months in AAP algorithms) or when concerns arise. Diagnostic developmental/psychometric testing is specialist-administered formal assessment (for example Bayley, age-banded Wechsler scales, Vineland/ABAS adaptive measures) that supports diagnostic formulation.[1][3][15]
Screening tools do not equal diagnosis. A positive M-CHAT-R/F warrants ASD evaluation; it does not itself confirm autism spectrum disorder.[5][7]
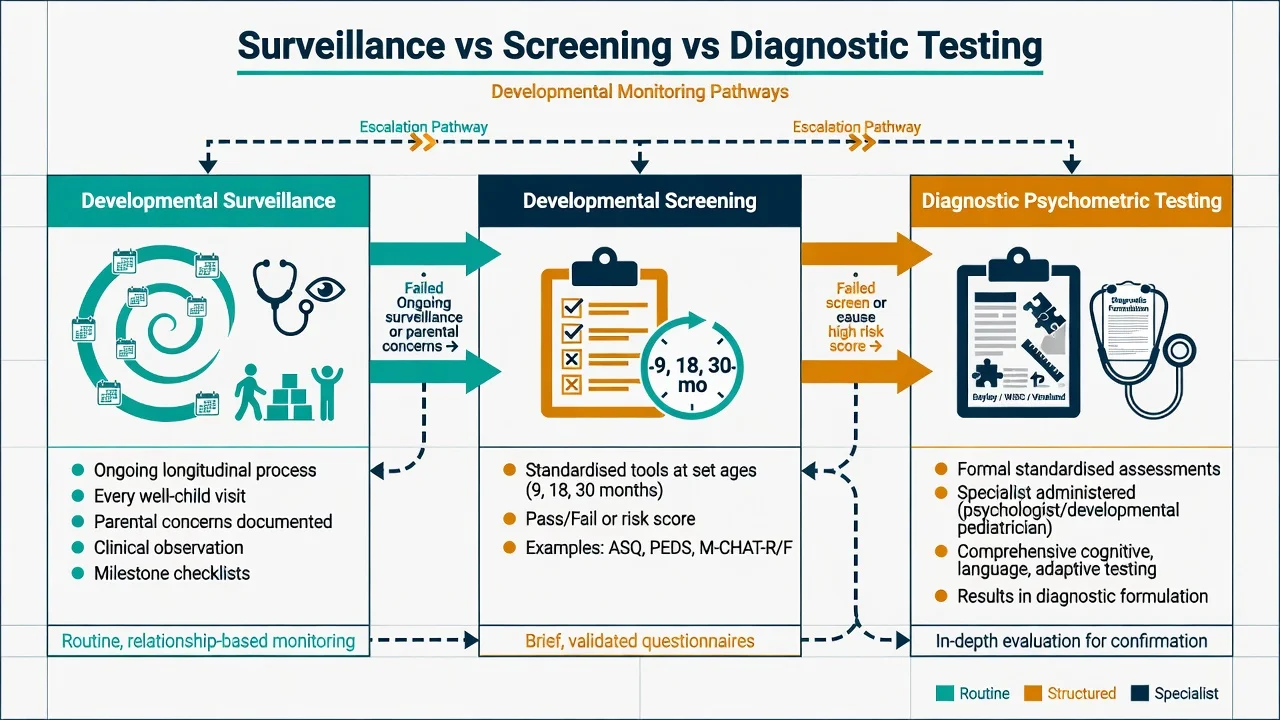
Surveillance
- Every clinical contact
- Parental concerns + observation
- Milestone update
- Longitudinal risk integration
Screening
- Standardised tools / set ages
- Pass–fail or risk bands
- ASQ / PEDS / M-CHAT-R/F class
- Triggers referral if failed
Diagnostic testing
- Specialist administered
- Bayley / WISC / Vineland etc.
- Confidence intervals matter
- Supports ID/ASD/learning Dx
Formulation
- Integrates all data sources
- 4Ps / biopsychosocial
- Drives multiagency plan
- Not a score dump
Nosology anchors
Global developmental delay (GDD) describes significant delay in two or more domains in children typically under about 5 years when standardised IQ testing is not yet reliable. Intellectual developmental disorder (ID/IDD) requires deficits in intellectual functions and adaptive functioning, with onset during the developmental period. Adaptive deficits — not IQ alone — determine the everyday disability and support needs.[4][6][17]
Related neurodevelopmental conditions (ASD, ADHD, language disorder, specific learning disorder) require the same developmental framing even when full-scale IQ is average. AACAP parameters for ASD and ID emphasise multi-source developmental evaluation rather than single-setting impressions.[4][5]
Epidemiology and risk
Patterns candidates should own
Developmental concerns are common in primary care and CAP intake; confirmed ID and ASD are less prevalent but high-impact. Risk concentrates after preterm birth, congenital and genetic syndromes, epilepsy, sensory impairment, severe early psychosocial deprivation, prenatal alcohol/substance exposure, and strong family neurodevelopmental history.[1][6]
Childhood psychiatric and developmental disorders substantially elevate risk of adult psychiatric disorder in longitudinal community cohorts — a rationale for thorough early assessment rather than dismissive "he'll grow out of it" when functional impairment is clear.[18]
Implementation science shows practices can adopt screening tools successfully, but referral completion after a failed screen is the frequent system failure — examiners reward candidates who close the loop to early intervention.[15]
Pathophysiology and developmental mechanisms
Development reflects gene–brain–environment interaction across sensitive periods. Motor systems, language networks, social-communication circuits, and executive control have overlapping but non-identical windows; insults (hypoxia, toxins, extreme deprivation, untreated hearing loss) produce domain-weighted profiles rather than uniform global delay in every case.[1][6][16]
Adaptive behaviour is the functional expression of cognitive capacity in conceptual (language, literacy, money/time concepts), social (relationships, gullibility, social problem-solving), and practical (self-care, safety, school/work routines) domains. Contemporary ID diagnostic teaching treats adaptive behaviour as essential and not merely confirmatory decoration around an IQ score.[4][17]
Clinical presentation and milestones
Taking a developmental history (exam skeleton)
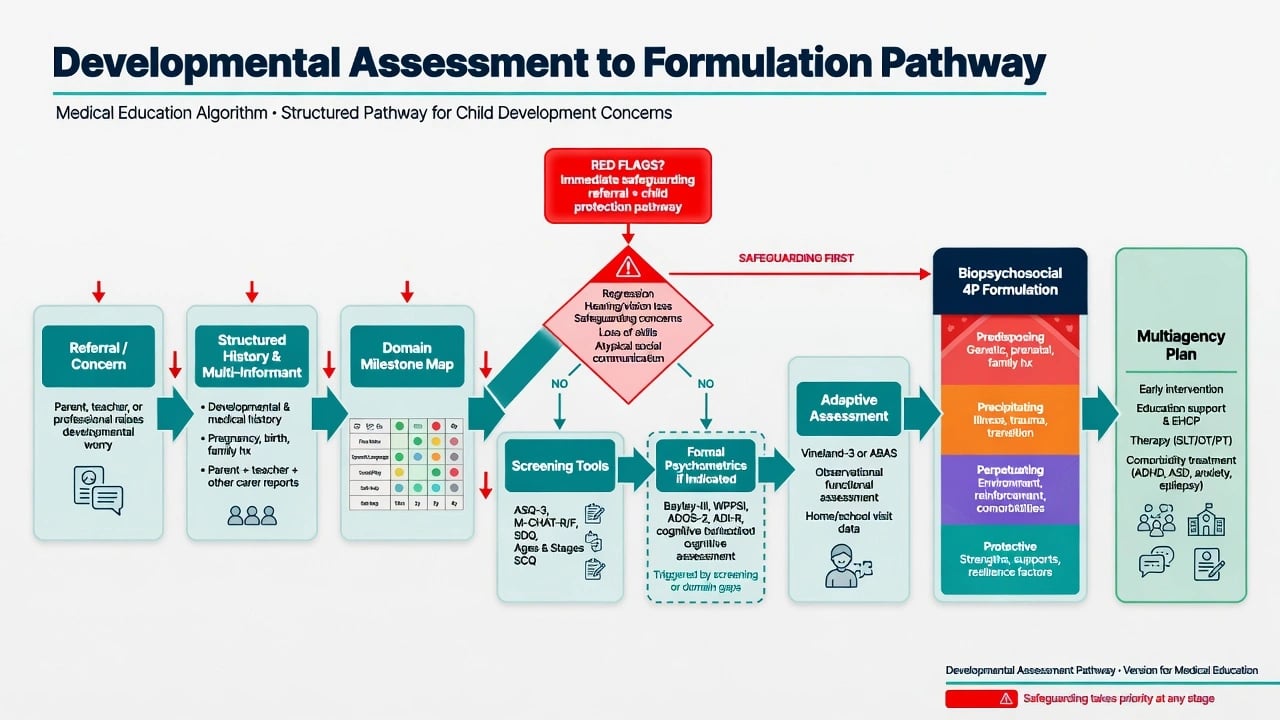
Structure pregnancy (infections, substances, growth), birth and neonatal course, early feeding/sleep, milestones by domain with approximate ages, any regression or plateau, intercurrent illness and seizures, hearing and vision checks, family developmental and psychiatric history, schooling trajectory, prior therapies, and safeguarding/care history. AACAP psychiatric assessment parameters and CAP formulation teaching both centre multi-informant, developmental history as core skill.[8][9]
Parental concern is data. Glascoe's work supports that carefully elicited parental concerns function as an efficient prescreen and identify many children with developmental and behavioural problems — never dismiss "I'm worried about speech" without structured follow-through.[13][14]
Milestone mapping (domain checklist)
Use age-banded expectations informed by contemporary evidence-informed milestone tools that emphasise what most children achieve by a given age, discouraging passive wait-and-see when a child is behind the majority threshold.[2]
| Domain | High-yield probes (examples, not exhaustive) |
|---|---|
| Gross motor | Sit, crawl, walk, run, stairs, coordination sports |
| Fine motor | Pincer, scribble, stack, buttons, pencil grasp, writing |
| Receptive language | Name response, follows commands, understands questions |
| Expressive language | Babble, words, phrases, conversation, narrative |
| Social-emotional | Joint attention, reciprocity, peer play, empathy |
| Adaptive | Feeding, toileting, dressing, safety, money/time (age-fit) |
| Cognitive/learning | Problem-solving play, pre-academic and school progress |
| Domain probes for milestone mapping; interpret against evidence-informed ages when most children achieve skills.[2] |
Motor delay specifically warrants structured neuromotor evaluation pathways rather than assuming "laziness."[16]
Age banding
Infancy: social engagement, attachment behaviours, early motor/language. Preschool: language explosion, pretend play, toileting, peer entry. School-age: literacy/numeracy, attention regulation, friendship quality. Adolescence: executive function, adaptive independence, identity, vocational readiness — mild ID often surfaces when adaptive demands rise.[1][4][9]
Differential diagnosis
- Hearing or vision impairment mimicking language or social delay — assess senses early.[1][6]
- ASD versus GDD/ID versus language disorder versus social (pragmatic) communication disorder — multi-source ASD evaluation principles apply.[5]
- ADHD versus learning disorder versus sleep/medical contribution versus mild ID presenting as "behaviour."[4]
- Trauma, neglect, attachment disruption altering social-emotional and cognitive presentation without being primary ID.[9]
- Selective mutism / anxiety versus primary language disorder — anxiety presentation with intact language elsewhere does not equal primary developmental language disorder.[9]
- Regression — metabolic, epileptic encephalopathy, neurodegenerative, severe psychosocial, late-onset neurological process — investigate, do not only watch.[6]
- Cultural-linguistic difference and dual-language exposure versus true disorder — use interpreters and culturally fair interpretation of tools.[1][5]
Bedside assessment
- Multi-informant history (carers, child as able, teachers).
- Domain milestone map with regression screen.
- Structured observation: reciprocity, joint attention, play level, speech intelligibility, motor, attention.
- Adaptive function interview across conceptual, social, practical domains with real-life examples.
- Select screening tools appropriate to age/question (milestone questionnaires; parental-concern tools such as PEDS; ASD risk screens such as M-CHAT-R/F; dimensional emotional-behavioural screens such as SDQ or CBCL systems).
- Risk: safeguarding, absconding/exploitation in cognitively vulnerable youth, self-harm with academic failure.
- Consent, assent, and interpreter use — state principles, quote local process rather than invented statutes.[1][7][9][10][11][13]
Psychometrics overview (what fellowship candidates must own)
Measurement hierarchy
| Layer | Examples (class of tool) | Role |
|---|---|---|
| Parental concern / prescreen | PEDS-style concern elicitation | Efficient case-finding |
| Milestone / broad screens | ASQ-class tools | Domain sampling at ages |
| ASD risk screens | M-CHAT-R/F | Toddler autism risk pathway |
| Emotional-behavioural dimensions | SDQ, CBCL/ASEBA | Symptom dimensions multi-informant |
| Cognitive batteries | Bayley (infants/toddlers); WPPSI/WISC/WAIS by age | Intellectual profile |
| Adaptive behaviour | Vineland, ABAS class | Essential for ID severity/supports |
| Tool classes for exams — choose by age and clinical question; screens never replace multi-source diagnosis.[1][7][10][11][14] |
Interpret standard scores, confidence intervals, floor/ceiling effects, practice effects, and cultural-linguistic fairness. Never treat a screening cut-off as a diagnosis. SDQ and CBCL systems provide dimensional and multi-informant behavioural data that complement — not replace — developmental cognitive testing.[7][10][11][12][14]
Adaptive function is not optional
For intellectual disability, contemporary diagnostic frameworks require concurrent adaptive deficits. Tassé and colleagues emphasise the conceptual relation between intellectual functioning and adaptive behaviour in ID diagnosis — candidates who report only IQ fail the exam standard.[4][17]
Investigations
There is no single laboratory test for developmental delay. Investigation is aetiology-directed after clinical phenotyping.[6]
- Hearing and vision whenever language/social concerns.
- Consider iron deficiency, lead, thyroid and other metabolic tests based on history and local epidemiology.
- Genetic evaluation for ID/GDD following paediatric genetics guidance (chromosomal microarray and subsequent tiers as indicated).[6]
- EEG/neuroimaging for neurological red flags (seizures, focal signs, progressive course) — not routine for pure behavioural referral without red flags.[6][16]
- Formal psychometrics and allied health assessments as indicated.
Acute safety
Definitive management and multiagency plan
Early intervention and supports
When delay or high suspicion is established, refer to early intervention and educational supports without waiting for a perfect complete battery if functional need is clear. Close the referral loop — screening without completed referral is a documented system failure mode.[1][15]
Multiagency plan typically includes developmental paediatrics as indicated, speech-language therapy, occupational and/or physiotherapy, education supports (local IEP/NCCD/EHCP-type mechanisms), and CAMHS for psychiatric comorbidity. Psychoeducation centres strengths, realistic expectations, and family advocacy skills.[1][4][5]
Psychiatric comorbidity
Treat ADHD, anxiety, depression, sleep disorders, and other comorbidity on disorder-specific evidence with developmental adaptations (communication supports, simplified psychoeducation, caregiver involvement). AACAP ID parameter principles: careful diagnosis, multi-modal care, cautious prescribing with monitoring, and avoidance of excess polypharmacy.[4]
Formulation-driven care
Link each intervention to predisposing, precipitating, perpetuating and protective factors (and biological/psychological/social levels). A list of test scores without a plan is not a completed assessment.[8]
Australian and New Zealand practice pairs developmental surveillance in primary care and child health services with CAMHS specialist assessment for complex neurodevelopmental and psychiatric presentations. Use state/territory education disability supports and child-protection pathways as applicable; do not invent national section numbers. Cultural safety for Aboriginal and Torres Strait Islander and Māori children is mandatory — bilingual development and collective caregiving are not pathology.[1][5]
| Target | Prefer | Avoid |
|---|---|---|
| Identification | Surveillance + timed screens + concern-led tools | Wait-and-see with clear red flags |
| ID diagnosis | IQ profile + adaptive assessment + developmental onset | IQ-only labels |
| ASD concern | Multi-source developmental evaluation after risk screen | Equating M-CHAT with diagnosis |
| Language delay | Hearing check early | Jumping to "will catch up" without data |
| Behaviour crisis in ID | Medical/pain/communication first | Immediate antipsychotic for convenience |
| Plan | Formulation + multiagency early help | Score dump without supports |
| Framework for exams; individualise and follow local governance.[1][4][7][17] |
Formulation (exam product)
A complete developmental formulation typically includes: identifying data and developmental trajectory (onset, domains affected, regression yes/no); biological factors (perinatal risk, genetics, epilepsy, sensory impairment, sleep, prenatal substances); psychological factors (cognitive profile, language, attachment/trauma, emotion regulation, self-concept); social/systemic factors (caregiving quality, school fit, peers, culture/language, poverty, protection status); 4Ps (predisposing, precipitating, perpetuating, protective); risk and capacity issues as relevant; and working diagnoses (provisional if incomplete testing) with a plan mapped to factors.[8][9]
Prognosis and disposition
Earlier identification and intervention improve functional trajectories for many developmental problems; prognosis still depends on aetiology, severity, comorbidity, and quality of supports.[1][6] Mild ID and specific learning disorders may present late when academic and adaptive demands rise. Longitudinal data link childhood disorders with adult psychiatric burden — plan transitions thoughtfully.[18]
Disposition intensity tracks adaptive need, risk, and comorbidity: enhanced primary surveillance, developmental clinic, CAMHS, education support, and specialist genetics/neurology as indicated.[4][6]
Complications and pitfalls
- IQ without adaptive function (or vice versa) for ID claims.[17]
- Using screens as diagnoses.[7]
- Cultural-linguistic misinterpretation of tools.[1][5]
- Wait-and-see delay after red flags or failed screens.[2][15]
- Missing hearing loss, epilepsy, or treatable medical contributors.[6][16]
- Parent-blame for neurodevelopmental disorders.[5]
- Incomplete formulation that lists symptoms without trajectory or systems context.[8]
Special populations
Preterm and medically complex infants need structured developmental follow-up. Looked-after and adopted children may show deprivation-related delays plus trauma — assess both. Deaf/hard-of-hearing and vision-impaired children require sensory-appropriate language and tools. Indigenous and culturally diverse children need cultural safety. Transition-age youth need adaptive and functional assessments for adult service eligibility and capacity planning.[1][4][6]
Exam pearls
DEVELOP map
References
- [1]Lipkin PH, Macias MM; Council on Children With Disabilities, Section on Developmental and Behavioral Pediatrics Promoting Optimal Development: Identifying Infants and Young Children With Developmental Disorders Through Developmental Surveillance and Screening Pediatrics, 2020.PMID 31843861
- [2]Zubler JM, Wiggins LD, Macias MM, Whitaker TM, et al. Evidence-Informed Milestones for Developmental Surveillance Tools Pediatrics, 2022.PMID 35132439
- [3]Council on Children With Disabilities; Section on Developmental Behavioral Pediatrics; Bright Futures Steering Committee; Medical Home Initiatives for Children With Special Needs Project Advisory Committee Identifying infants and young children with developmental disorders in the medical home: an algorithm for developmental surveillance and screening Pediatrics, 2006.PMID 16818591
- [4]Siegel M, McGuire K, Veenstra-VanderWeele J, Stratigos K, et al. Practice Parameter for the Assessment and Treatment of Psychiatric Disorders in Children and Adolescents With Intellectual Disability (Intellectual Developmental Disorder) J Am Acad Child Adolesc Psychiatry, 2020.PMID 33928910
- [5]Volkmar F, Siegel M, Woodbury-Smith M, King B, et al. Practice parameter for the assessment and treatment of children and adolescents with autism spectrum disorder J Am Acad Child Adolesc Psychiatry, 2014.PMID 24472258
- [6]Moeschler JB, Shevell M; Committee on Genetics Comprehensive evaluation of the child with intellectual disability or global developmental delays Pediatrics, 2014.PMID 25157020
- [7]Robins DL, Casagrande K, Barton M, Chen CM, et al. Validation of the modified checklist for Autism in toddlers, revised with follow-up (M-CHAT-R/F) Pediatrics, 2014.PMID 24366990
- [8]Winters NC, Hanson G, Stoyanova V The case formulation in child and adolescent psychiatry Child Adolesc Psychiatr Clin N Am, 2007.PMID 17141121
- [9]King RA; American Academy of Child and Adolescent Psychiatry Practice parameters for the psychiatric assessment of children and adolescents J Am Acad Child Adolesc Psychiatry, 1997.PMID 9606102
- [10]Achenbach TM, Ruffle TM The Child Behavior Checklist and related forms for assessing behavioral/emotional problems and competencies Pediatr Rev, 2000.PMID 10922023
- [11]Goodman R The Strengths and Difficulties Questionnaire: a research note J Child Psychol Psychiatry, 1997.PMID 9255702
- [12]Goodman A, Goodman R Strengths and difficulties questionnaire as a dimensional measure of child mental health J Am Acad Child Adolesc Psychiatry, 2009.PMID 19242383
- [13]Glascoe FP Parents' concerns about children's development: prescreening technique or screening test? Pediatrics, 1997.PMID 9093291
- [14]Glascoe FP Parents' evaluation of developmental status: how well do parents' concerns identify children with behavioral and emotional problems? Clin Pediatr (Phila), 2003.PMID 12659386
- [15]King TM, Tandon SD, Macias MM, Healy JA, et al. Implementing developmental screening and referrals: lessons learned from a national project Pediatrics, 2010.PMID 20100754
- [16]Noritz GH, Murphy NA; Neuromotor Screening Expert Panel Motor delays: early identification and evaluation Pediatrics, 2013.PMID 23713113
- [17]Tassé MJ, Luckasson R, Schalock RL The Relation Between Intellectual Functioning and Adaptive Behavior in the Diagnosis of Intellectual Disability Intellect Dev Disabil, 2016.PMID 27893317
- [18]Copeland WE, Shanahan L, Costello EJ, Angold A Childhood and adolescent psychiatric disorders as predictors of young adult disorders Arch Gen Psychiatry, 2009.PMID 19581568