Psych · Child and adolescent psychiatry — chronic irritability / DMDD
Disruptive mood dysregulation disorder
Also known as DMDD · Severe mood dysregulation · SMD · Chronic severe irritability children · Pediatric chronic irritability · Temper outbursts mood disorder · Nonepisodic irritability youth
Exam-exhaustive fellowship reference on disruptive mood dysregulation disorder — DSM-5-TR criteria and age rules, SMD historical construct, Copeland epidemiology and adult outcomes, multi-informant assessment, bipolar/ODD/ADHD differentials and hierarchy, psychosocial first-line care (parent training, Waxmonsky group therapy, DBT-C), medication limits (Dickstein lithium-negative; Towbin citalopram+stimulant signal), school and safeguarding, FRANZCP/MRCPsych/ABPN framing. Distinct from ODD/CD, youth depression, and bipolar topics.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Disruptive mood dysregulation disorder (DMDD) is high-yield wherever examiners probe the pediatric bipolar overdiagnosis controversy, chronic irritability, and ODD hierarchy. FRANZCP CAP, MRCPsych CASC, ABPN, and MD/DNB viva all reward precise criteria, longitudinal outcome literacy, and refusal to treat every explosive child as bipolar.[1][4][13][15]
This topic is related to but distinct from conduct-and-oppositional-disorders (ODD/CD criteria and MST depth), child-and-adolescent-depression (episodic MDD and fluoxetine pathways), and bipolar-affective-disorder (episodic mania/hypomania). Here the centre of gravity is the nonepisodic chronic irritability pathway that DSM-5 named DMDD after the severe mood dysregulation (SMD) research construct.[1][4][14]
Definition and classification
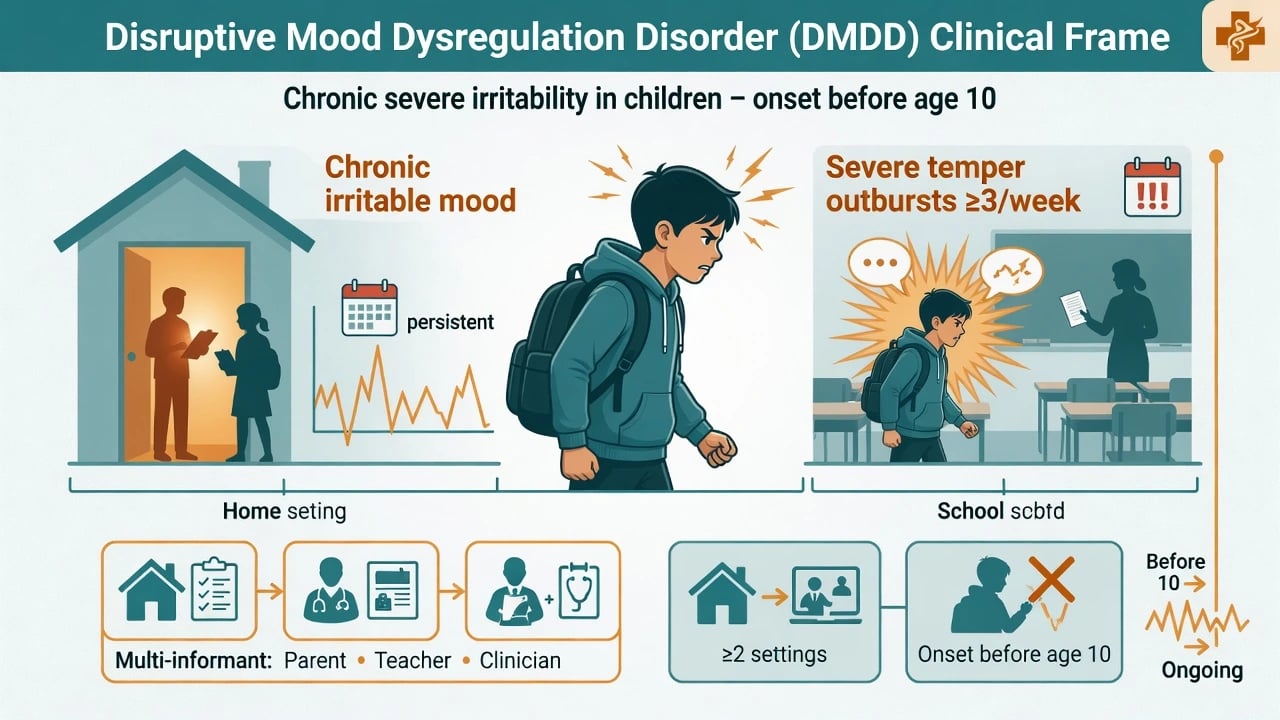
DSM-5-TR skeleton (exam-ready). Severe recurrent temper outbursts (verbal rages and/or behavioural aggression toward people or property) that are grossly out of proportion in intensity or duration to the situation or provocation, inconsistent with developmental level, and occurring on average three or more times per week. Between outbursts, mood is persistently irritable or angry most of the day, nearly every day, and observable by others (e.g. parents, teachers, peers). Symptoms have been present for 12 or more months without a period of 3 or more consecutive months free of all criteria; present in at least two settings and severe in at least one; chronological age at least 6 years and not first diagnosed after age 18; onset of symptoms before age 10.[4][13][14]
Critical exclusions and hierarchy
| Rule | Practical meaning |
|---|---|
| No full manic/hypomanic episode lasting more than 1 day | Distinct elevated/expansive periods re-open bipolar pathway |
| Not only during MDD episode | Separate chronic irritability pattern from discrete depression |
| Cannot coexist with ODD, IED, or bipolar | If ODD + DMDD both met → diagnose DMDD only |
| Not better explained by ASD, PTSD, separation anxiety, etc. | Reformulate when another primary story fits better |
| Can coexist with MDD, ADHD, CD, substance use | Comorbidity is expected — treat the formulation |
Historical bridge — SMD. Leibenluft and colleagues defined severe mood dysregulation to study children with chronic, nonepisodic irritability and hyperarousal who were often misclassified as bipolar in community practice. DSM-5 operationalised a related phenotype as DMDD (with refinements on age, duration, and exclusions). In viva, say: SMD is the research parent; DMDD is the DSM clinical category.[1][4]
ICD-11. Name the manual you are applying when duration language is probed; examiners accept that chronic irritability constructs sit near mood and disruptive behaviour boundaries and that wording is not identical across systems.[14][16]
Epidemiology and risk
Community analyses of the proposed DSM-5 phenotype (Copeland et al.) found 3-month prevalence roughly 0.8% to 3.3%, highest in preschool samples and sensitive to how strictly exclusions are applied — quote order of magnitude and method-sensitivity, not false clinic precision.[2]
Epidemiology headlines candidates should own
Risk and correlates. Family adversity, parental psychopathology, peer rejection, school failure/exclusion, and socioeconomic disadvantage co-travel with the phenotype. Comorbidity is the rule: ADHD, oppositional behaviours, anxiety, and depressive symptoms dominate clinical samples; Axelson and the LAMS group showed how often proposed DMDD co-occurs with other disorders in children already selected for elevated manic symptoms — reinforcing that DMDD is not a pure, isolated label in real clinics.[2][5][13]
Adult outcomes. Childhood DMDD symptoms predict elevated adult anxiety and depression and broader functional impairment (health, financial/educational, social domains) rather than a clean conversion to classic bipolar disorder — a core exam pearl that undercuts bipolar overpathologising of chronic irritability.[3][6]
Pathophysiology and maintaining mechanisms
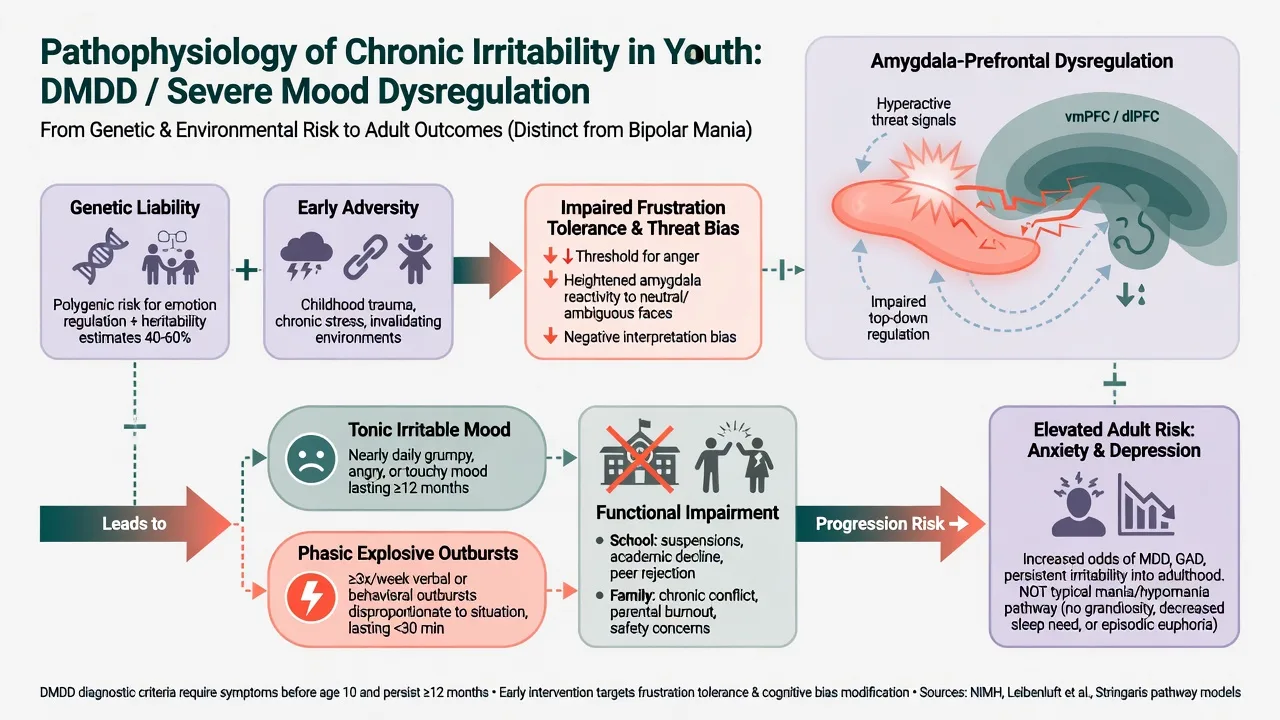
- Tonic vs phasic irritability. Tonic = persistent angry/irritable baseline; phasic = explosive outbursts. Both are required for the clinical DMDD picture; research and treatment targets may emphasise one or both.[1][13]
- Frustration intolerance and threat bias. Youth with severe irritability show exaggerated responses to blocked goals and biased threat processing at group level — not a diagnostic imaging test.[1][4]
- Stringaris oppositionality dimensions. Irritable, headstrong, and hurtful dimensions have different longitudinal correlates; the irritable dimension tracks emotional (internalising) outcomes, supporting why DMDD sits near mood nosology rather than pure conduct pathology.[8][6]
- Coercive family cycles. Escape-conditioned escalations maintain outbursts and parental inconsistency — primary target of parent management training.[11][13]
- Bipolar boundary science. On follow-up, SMD youth develop (hypo)manic or mixed episodes far less often than youth with narrowly defined bipolar disorder — empirical backbone for not equating chronic irritability with mania.[7][1]
Clinical presentation
Core. Frequent severe tantrums or rages (screaming, slamming, hitting, property damage) out of proportion to triggers, with a baseline of nearly continuous crankiness, anger, or touchiness that teachers and parents independently recognise. Impairment shows as classroom removal, peer isolation, exhausted carers, and secondary low self-worth.[4][13]
MSE / observation. Hostile attributional bias, short frustration tolerance, reactive aggression that cools (unlike planned callous cruelty), absence of sustained elevated mood, grandiosity, or decreased need for sleep as distinct episodes. Document what a "good day" looks like — DMDD still has bad baseline mood on good days.[1][4]
Comorbidity colouring. ADHD impulsivity fuels collision with limits; anxiety can present as explosive avoidance; learning disorders fuel school meltdowns; autistic sensory overload can mimic outbursts — always map the developmental story.[5][13][14]
Differential diagnosis
| Differential | Discriminators | Why it matters |
|---|---|---|
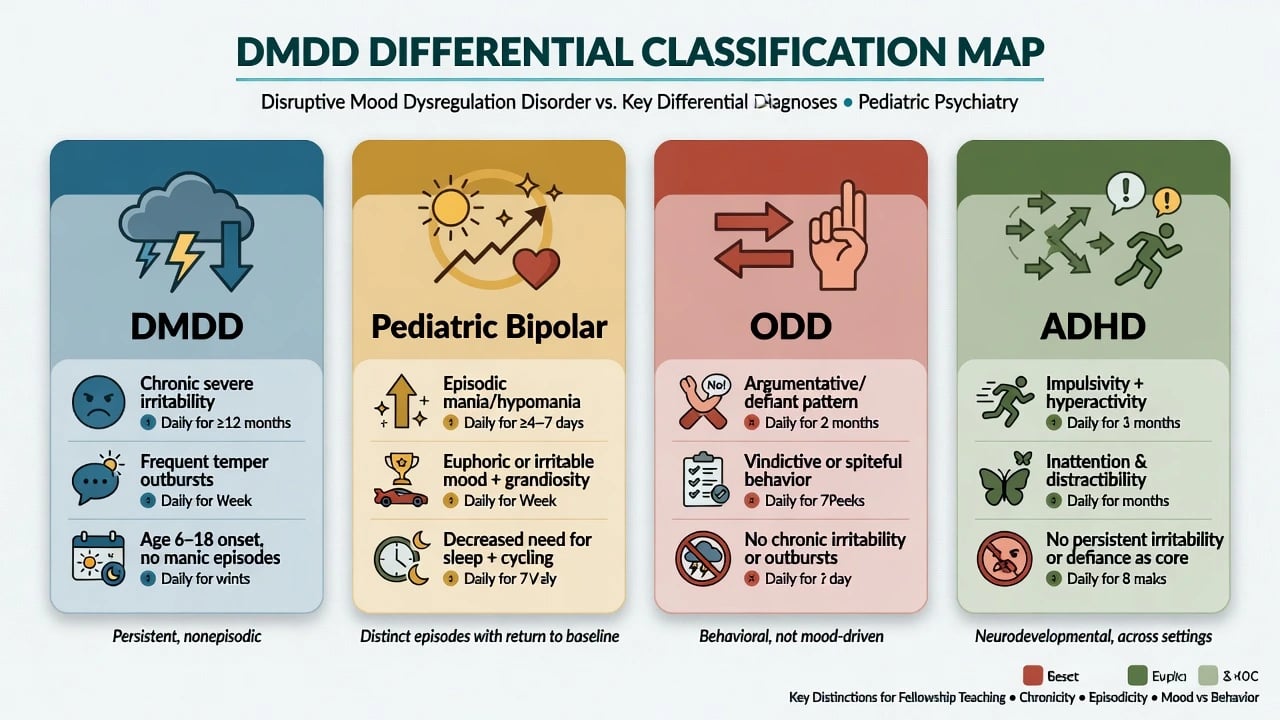
| Pediatric bipolar / mania | Episodic elevated/expansive (or distinct irritable) periods with manic symptom cluster; decreased need for sleep, grandiosity | Wrong pathway → wrong meds |
| ODD | Argumentative/defiant pattern; if full DMDD criteria also met, DMDD only | Hierarchy exam trap |
| IED | Discrete aggressive outbursts without persistent inter-outburst irritable mood requirement | Different construct |
| ADHD alone | Impulsivity/emotional dysregulation without full chronic multi-setting DMDD severity/duration | Treat ADHD first often |
| MDD (irritable mood allowed in youth) | 2-week episodic syndrome vs 12-month chronic pattern | Therapy and SSRI framing differs |
| ASD meltdowns | Sensory/rigidity triggers; developmental social-communication history | Adapt environment and communication |
| Trauma/PTSD | Hyperarousal, re-experiencing, avoidance chronology | Trauma-informed care |
| Medical/substance | New irritability with illness, steroids, stimulants misuse, sleep apnoea | Missed medical harm |
Always complete a bipolar screen before declaring "chronic irritability only," and complete a developmental/trauma screen before declaring "just bad behaviour."[15][16]
Assessment
Structure: multi-informant + multi-setting + onset before 10 + 12-month course + bipolar screen + comorbidity + risk + parenting ecology + school function.[4][13]
- Concrete outburst log: frequency, duration, intensity, triggers, recovery time, injury/property damage.
- Inter-outburst mood rating by parents and teachers separately.
- Developmental, ADHD, learning, ASD, anxiety, depression, substance, sleep histories.
- Family coercive cycles, parental mental health, domestic violence, maltreatment.
- Risk: aggression (who/what/weapons), self-harm, absconding, exploitation, school safety.
- Consent/competence and confidentiality limits — jurisdiction-specific statutes; state principles (least restrictive care, best interests, safeguarding duties), do not invent section numbers.[4][13][16]
Irritability scales (e.g. Affective Reactivity Index conceptual use; clinician-rated irritability measures in research) support measurement-based care; they do not diagnose DMDD alone.[13][14]
Investigations
There is no diagnostic blood test, EEG, or MRI for DMDD.[4][14]
Before selected pharmacotherapy: height/weight/BMI, BP, review of movement side-effects if antipsychotics considered, metabolic parameters as indicated, ECG when cardiac risk or other clinical indication, pregnancy test when relevant, UDS when substance use is plausible. Psychoeducational testing when learning disorder is likely. Imaging/EEG only for neurological red flags — not routine "mood work-up."[13][15]
Acute safety and safeguarding
School safety plans, supervised transitions, and carer crisis contacts are part of treatment, not optional extras.[11][13]
Definitive management
Psychosocial interventions (first-line)
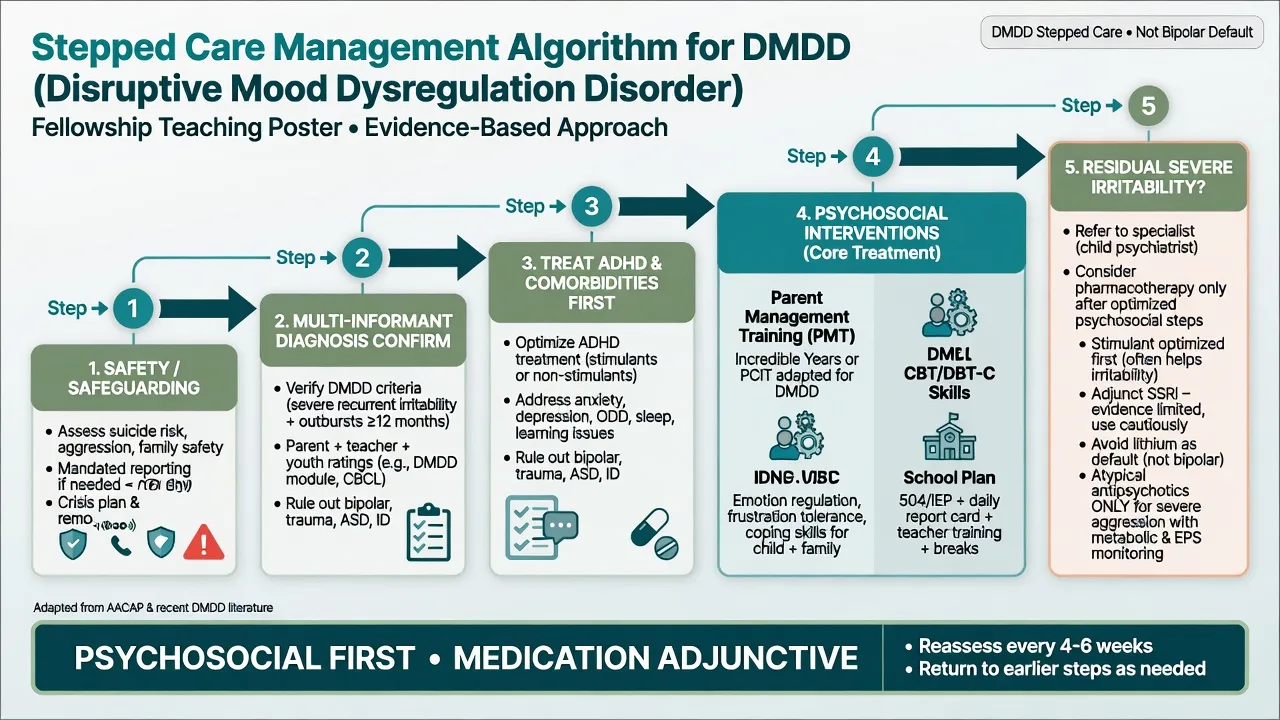
- Parent management training / behavioural parent training: consistent limits, labelled praise, planned ignoring of low-level defiance, calm consequence delivery, reduced coercive escalation. This is the backbone for outburst frequency reduction.[11][13]
- Child skills work: emotion recognition, frustration tolerance, problem-solving, and anger regulation (CBT-informed modules; school coaching).
- Integrative parent–child group therapy after stimulant stabilisation: Waxmonsky and colleagues randomised children with ADHD and SMD (after open stimulant optimisation) to an 11-week joint parent–child integrative group therapy versus community psychosocial care — a named psychosocial evidence anchor for severe nonepisodic irritability phenotypes.[11]
- DBT for preadolescent children (DBT-C): Perepletchikova et al. demonstrated feasibility and a positive response signal versus treatment-as-usual in 7–12-year-olds with DMDD — cite as promising specialised skills-based care, not universal first package everywhere.[12]
- School: behaviour support plans, predictable routines, reduced trigger load, exclusion-prevention, teacher–clinician liaison.[13][14]
Comorbidity treatment — especially ADHD
Optimise ADHD treatment when present. Stimulant medication often reduces secondary irritability driven by impulsive collisions with demands; many specialist protocols stabilise ADHD first before judging residual DMDD-level irritability (as in the Waxmonsky and Towbin trial pipelines).[10][11][13]
Pharmacotherapy — limited, specialist, adjunctive
There is no single licensed "DMDD drug" with the fluency of fluoxetine-for-youth-MDD. Fellowship answers emphasise evidence limits and reformulation.[13][14]
Lithium does not rescue SMD. Dickstein et al. conducted a randomised double-blind placebo-controlled trial of lithium in youths with SMD after placebo run-in; lithium did not demonstrate meaningful clinical superiority over placebo for this nonepisodic irritability phenotype — a classic trap against automatic "mood stabiliser = irritability treatment" thinking.[9]
Adjunctive citalopram + stimulant has RCT signal. Towbin et al. enrolled youth with chronic severe irritability (nearly all meeting DMDD criteria) after open methylphenidate lead-in, then randomised to citalopram versus placebo added to stimulant for 8 weeks; a significantly higher proportion of responders was seen with citalopram adjunct. Example viva framing (individualise; specialist CAMHS): after stimulant optimisation, consider citalopram at low starting doses (commonly 10 mg orally daily, titrating cautiously toward 20 mg daily as tolerated under specialist review) with early monitoring for activation, insomnia, agitation, and suicidality — the same black-box-aware youth SSRI safety culture used in depression care. Do not start SSRI without bipolar screen, safety plan, and carer involvement.[10][16]
Atypical antipsychotics. Sometimes used short-term for severe aggression when psychosocial measures and comorbidity treatment fail and risk is high — this is aggression management, not a DMDD-specific cure. If used (e.g. low-dose risperidone pathways familiar from disruptive behaviour/ASD irritability literature), document target behaviours, time-limited goals, and metabolic/EPS/prolactin monitoring. Avoid open-ended polypharmacy labelled "pediatric bipolar treatment" without manic episodes.[13][15]
Family psychoeducation
Explain in plain language: chronic severe irritability is real and impairing; it is usually not the same illness as classic bipolar disorder; adult risk leans anxiety and depression; skills and consistency change trajectories more than hunting for a single magic tablet. Offer hope without minimising harm.[3][4][6]
Landmark evidence (exam names)
| Anchor | Design takeaway | Clinical pearl |
|---|---|---|
| Leibenluft 2011 | SMD construct and bipolar boundaries | Chronic irritability ≠ mania by default |
| Copeland 2013 | Community prevalence of proposed DMDD | ~0.8–3.3% three-month; high comorbidity |
| Copeland 2014 | Adult outcomes of childhood DMDD | Anxiety/depression and functional impairment |
| Axelson LAMS 2012 | Proposed DMDD in manic-symptom enriched sample | Massive comorbidity; careful diagnosis |
| Stringaris 2009 / 2010 | Irritability adult outcomes; SMD vs BD manic risk | Internalising path; rare mania conversion |
| Stringaris & Goodman 2009 | Irritable/headstrong/hurtful dimensions | Irritable dimension → emotional outcomes |
| Dickstein lithium 2009 | Lithium vs placebo in SMD | Negative — do not assume bipolar meds work |
| Towbin citalopram 2020 | CTP + MPH vs PBO + MPH | Adjunctive SSRI response signal after stimulant |
| Waxmonsky group therapy | Integrative parent–child therapy post-stimulant | Named psychosocial RCT for SMD+ADHD |
| Perepletchikova DBT-C | DBT-C vs TAU in preadolescent DMDD | Feasibility + efficacy signal for skills therapy |
| AACAP bipolar parameter | Narrow bipolar assessment | Episodic criteria matter |
| RANZCP mood 2020 | Regional formulation-centred mood care | Youth-aware risk and formulation principles |
DMDD / SMD
- Chronic nonepisodic irritability
- Frequent outbursts + angry baseline
- Adult anxiety/depression path
- Psychosocial first
Pediatric bipolar
- Episodic manic/hypomanic periods
- Decreased need for sleep, grandiosity
- Higher mania recurrence risk
- Mood-stabiliser/antipsychotic logic differs
ODD
- Angry/argumentative/vindictive pattern
- Hierarchy: DMDD supersedes if full
- Parent training core shared
- May lack continuous severe mood
ADHD interface
- Often comorbid
- Stimulant optimisation first
- Secondary irritability common
- Does not exclude DMDD
Subtypes and scenarios
- ADHD + residual severe irritability after stimulant: add parent training intensity; consider specialist adjunct SSRI pathway only after behavioural optimisation.[10][11]
- "Bipolar child" on multiple agents without manic episodes: stop, reformulate, simplify, rebuild psychosocial plan.[1][9][15]
- Preschool severe tantrums: developmental temper is common; DSM age floor and specialist CAP assessment prevent overdiagnosis.[2][4]
- Adolescent residual irritability: watch anxiety/depression emergence; plan transition supports.[3][6]
- CD behaviours plus DMDD mood: multiagency intensity for rights-violating behaviours; mood label does not replace risk management.[5][13]
Complications and pitfalls
Other traps: dual-coding ODD+DMDD against hierarchy; missing trauma/ASD/learning; token two sessions of "parent advice" declared as failed psychosocial care; SSRI without monitoring; ignoring school exclusion as a maintaining factor.[4][12][13]
Prognosis and disposition
Many children improve with consistent behavioural systems and comorbidity care, but residual irritability and internalising risk warrant longitudinal follow-up. Disposition ladder: primary care/community CAMHS with school partnership → intensive community/day programmes for severe multi-domain impairment → inpatient only when risk exceeds community containment. Measure success by outburst frequency, school attendance, family conflict, and peer function, not checklist magic alone.[3][11][14]
Special populations
Preschoolers: highest apparent rates in community work — apply age rules and developmental caution.[2] Autistic youth: separate sensory meltdowns from DMDD criteria; adapt communication. Intellectual disability: collateral-heavy assessment. Youth in care and maltreated children: trauma-informed formulation is mandatory, not optional. Cultural safety (including Indigenous ANZ contexts) is a FRANZCP expectation — use interpreters, explore explanatory models, and avoid pathologising culturally normative discipline conflict without impairment analysis.[13][16]
Regional guideline deltas
ANZ (RANZCP): formulation-centred mood care and risk assessment principles from the 2020 mood disorder guidelines apply to youth irritability pathways; local Mental Health Act processes are state/territory specific — name principles, not invented sections.[16]
UK: CAMHS stepped care and NICE-style psychosocial emphasis for behavioural and emotional disorders in children; DMDD as DSM construct may be discussed alongside ICD framing in exams — state which system you use.[14]
US: AACAP bipolar practice parameter discipline (episodic criteria) remains examinable; DSM-5 DMDD is native language; stimulant-first then adjunct SSRI evidence (Towbin) is ABPN-friendly detail.[10][15]
Exam pearls
[4] [13] [4] [7] [3] [9] [10] [11] [12]Mnemonic for first-pass assessment: RAGE-MAP — Risk/safeguarding, Age rules and onset before 10, Grid multi-setting 12-month course, Episodes of mania screened out, Multi-informant mood/outburst log, ADHD and other comorbidity, Parent training and school plan first.[1][4][11]
Summary
Defend DMDD as chronic severe childhood irritability with frequent disproportionate outbursts, carved out to stop the wholesale conversion of explosive irritable children into "pediatric bipolar." Know Copeland prevalence and adult internalising outcomes, Leibenluft/Stringaris boundary science, ODD hierarchy, and a psychosocial-first algorithm with stimulant optimisation, named therapy trials (Waxmonsky, DBT-C), and cautious specialist pharmacology (Towbin citalopram adjunct; not lithium-as-default).[1][2][3][9][10][11][12]
References
- [1]Leibenluft E Severe mood dysregulation, irritability, and the diagnostic boundaries of bipolar disorder in youths Am J Psychiatry, 2011.PMID 21123313
- [2]Copeland WE, Angold A, Costello EJ, Egger H Prevalence, comorbidity, and correlates of DSM-5 proposed disruptive mood dysregulation disorder Am J Psychiatry, 2013.PMID 23377638
- [3]Copeland WE, Shanahan L, Egger H, Angold A, Costello EJ Adult diagnostic and functional outcomes of DSM-5 disruptive mood dysregulation disorder Am J Psychiatry, 2014.PMID 24781389
- [4]Roy AK, Lopes V, Klein RG Disruptive mood dysregulation disorder: a new diagnostic approach to chronic irritability in youth Am J Psychiatry, 2014.PMID 25178749
- [5]Axelson D, Findling RL, Fristad MA, et al. Examining the proposed disruptive mood dysregulation disorder diagnosis in children in the Longitudinal Assessment of Manic Symptoms study J Clin Psychiatry, 2012.PMID 23140653
- [6]Stringaris A, Cohen P, Pine DS, Leibenluft E Adult outcomes of youth irritability: a 20-year prospective community-based study Am J Psychiatry, 2009.PMID 19570932
- [7]Stringaris A, Baroni A, Haimm C, et al. Pediatric bipolar disorder versus severe mood dysregulation: risk for manic episodes on follow-up J Am Acad Child Adolesc Psychiatry, 2010.PMID 20410732
- [8]Stringaris A, Goodman R Three dimensions of oppositionality in youth J Child Psychol Psychiatry, 2009.PMID 19166573
- [9]Dickstein DP, Towbin KE, Van Der Veen JW, et al. Randomized double-blind placebo-controlled trial of lithium in youths with severe mood dysregulation J Child Adolesc Psychopharmacol, 2009.PMID 19232024
- [10]Towbin K, Vidal-Ribas P, Brotman MA, et al. A Double-Blind Randomized Placebo-Controlled Trial of Citalopram Adjunctive to Stimulant Medication in Youth With Chronic Severe Irritability J Am Acad Child Adolesc Psychiatry, 2020.PMID 31128268
- [11]Waxmonsky JG, Waschbusch DA, Belin P, et al. A Randomized Clinical Trial of an Integrative Group Therapy for Children With Severe Mood Dysregulation J Am Acad Child Adolesc Psychiatry, 2016.PMID 26903253
- [12]Perepletchikova F, Nathanson D, Axelrod SR, et al. Randomized Clinical Trial of Dialectical Behavior Therapy for Preadolescent Children With Disruptive Mood Dysregulation Disorder: Feasibility and Outcomes J Am Acad Child Adolesc Psychiatry, 2017.PMID 28942805
- [13]Baweja R, Mayes SD, Hameed U, Waxmonsky JG Disruptive mood dysregulation disorder: current insights Neuropsychiatr Dis Treat, 2016.PMID 27601906
- [14]Bruno A, Celebre L, Torre G, et al. Focus on Disruptive Mood Dysregulation Disorder: A review of the literature Psychiatry Res, 2019.PMID 31164249
- [15]McClellan J, Kowatch R, Findling RL, Work Group on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with bipolar disorder J Am Acad Child Adolesc Psychiatry, 2007.PMID 17195735
- [16]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391