Psych · Child and adolescent psychiatry — eating disorders
Eating disorders in adolescence
Also known as Adolescent anorexia nervosa · Adolescent bulimia nervosa · Binge-eating disorder adolescents · ARFID · Family-based treatment · FBT · Maudsley family therapy · Refeeding syndrome · Atypical anorexia nervosa
Exam-exhaustive fellowship reference on eating disorders in adolescence — DSM-5-TR/ICD-11 AN, BN, BED and ARFID; medical risk and admission thresholds; refeeding syndrome and higher-calorie refeeding evidence; family-based treatment; SSRIs in BN not AN; capacity and compulsory care principles. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Eating disorders in adolescence are high-yield FRANZCP CAP and general adult interface topics, MRCPsych CASCs, and ABPN items. Examiners test medical risk parameters, refeeding, FBT structure, pharmacotherapy boundaries, and capacity — not only diagnostic labels. A candidate who reads only this topic should defend diagnosis, differentials, admission thresholds, and stepped care at consultant depth.[2][3][5][22]
Overview and definition
Eating disorders are behavioural and cognitive syndromes centred on disordered eating and/or weight/shape control that cause medical and psychosocial harm. In adolescents the same core diagnoses apply as in adults, but growth trajectory, pubertal status, % median BMI, family systems, and developmental capacity reshape assessment and treatment intensity.[2][5][22]
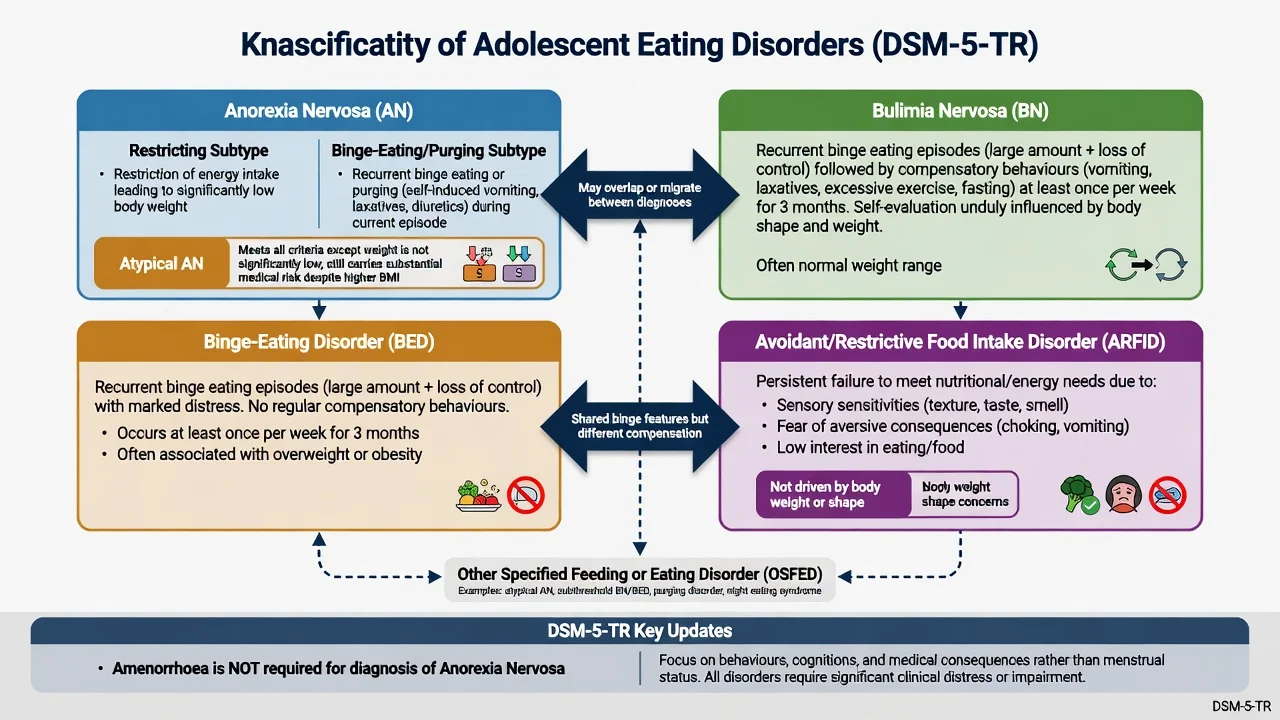
Anorexia nervosa (AN) involves restriction of energy intake relative to requirements leading to significantly low body weight (or failure to achieve expected growth), intense fear of weight gain or persistent behaviour that interferes with weight gain, and disturbance in body weight/shape experience or undue influence of weight/shape on self-evaluation (or persistent lack of recognition of seriousness of low weight). Amenorrhoea is not required for DSM-5/DSM-5-TR diagnosis — a classic exam trap from older criteria.[2][3][22]
Bulimia nervosa (BN) involves recurrent binge eating (unusually large amount in a discrete period with loss of control) plus recurrent inappropriate compensatory behaviours, at a frequency threshold commonly taught as at least once weekly for three months, with self-evaluation unduly influenced by body shape and weight; weight is often in the normal or high range.[2][3][24]
Binge-eating disorder (BED) involves recurrent binge eating with marked distress without regular compensatory behaviours that define BN.[3][19]
Avoidant/restrictive food intake disorder (ARFID) is persistent failure to meet nutritional/energy needs associated with significant weight loss or growth failure, nutritional deficiency, dependence on supplements/enteral feeding, or marked psychosocial impairment — not explained by body-image disturbance or available food scarcity. Presentations cluster around sensory sensitivity, fear of aversive consequences (choking/vomiting), or low interest in eating.[3][23]
Atypical AN (often coded under other specified feeding or eating disorder) meets AN psychological and behavioural criteria with recent significant weight loss, yet weight is not below conventional underweight cut-offs — medical risk can still be high.[3][5]
ICD-11 uses closely related feeding and eating disorder constructs; state which manual you are applying when examiners probe duration or amenorrhoea language.[2][3]
Classification
AN
- Restriction + fear of weight gain + body-image disturbance
- Restricting vs binge-eating/purging subtype
- Significantly low weight or growth failure
- High medical and suicide mortality risk
BN
- Binge + compensatory behaviours
- Often normal BMI — medical risk still real
- Self-evaluation shape/weight driven
- SSRI evidence (fluoxetine) stronger than in AN
BED
- Binge without regular compensation
- Distress and functional impairment
- CBT-oriented psychological care
- Adolescent RCT evidence emerging
ARFID
- Not body-image driven
- Sensory / fear / low-interest pathways
- Growth and nutrition risk
- Different therapy targets than AN
Epidemiology and risk factors
Epidemiology headlines (exam order of magnitude)
Community and clinical epidemiology show that eating disorders are uncommon relative to anxiety/depression but carry disproportionate morbidity and mortality. Incidence of AN peaks in adolescence; BN and BED also commonly emerge in youth. Service data show evolving incidence patterns over decades (for example shifts in BN presentation in some primary-care cohorts).[13]
Meta-analysis of mortality rates demonstrates elevated standardised mortality for AN and increased risk across eating disorders more broadly, with suicide an important contributor alongside medical complications — exam answers must not treat ED as purely “lifestyle” problems.[14]
Risk factors examiners expect: female sex (with male under-recognition), perfectionism and anxiety temperament, first-degree family history, genetic liability (GWAS implicating metabo-psychiatric biology in AN), thin-ideal sports/dance, bullying and trauma, and high body-image pressure environments including social media. Comorbid depression, OCD, anxiety disorders, autism spectrum traits, and deliberate self-harm are common and change risk and therapy design.[13][16][22]
ARFID is increasingly recognised in child and adolescent services, with age- and sex-pattern differences from classic AN and different clinical drivers.[23]
Pathophysiology
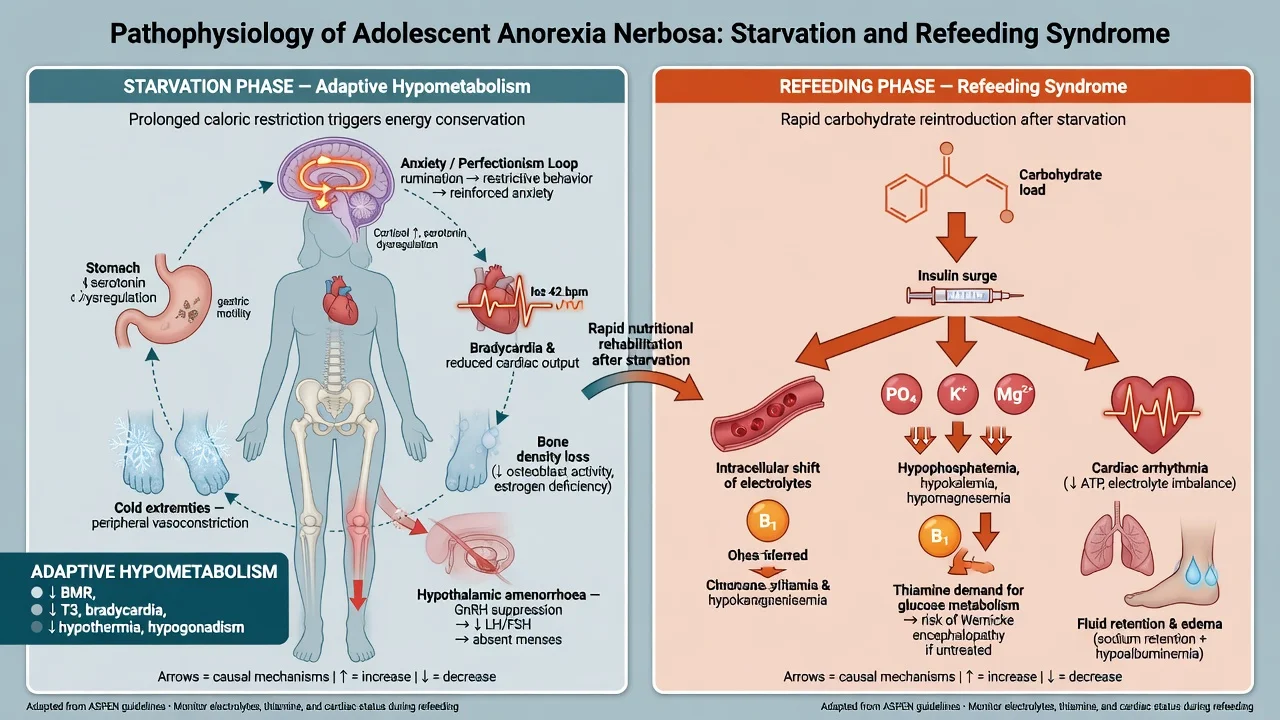
Starvation physiology. Energy deficit drives adaptive hypometabolism: bradycardia, orthostatic intolerance, hypothermia, reduced gut motility, bone mineral accrual failure, hypothalamic amenorrhoea or delayed puberty, cognitive narrowing, and heightened anxiety around food. These are medical consequences, not “commitment” to thinness.[5][20][22]
Psychological maintaining cycles. Overvaluation of weight and shape, dietary restraint, binge–purge cycles, compulsive exercise, and family mealtime conflict maintain illness. In ARFID the maintaining factors are sensory aversion, conditioned fear, or low appetite drive rather than weight phobia.[18][22][23]
Refeeding pathophysiology. Carbohydrate reintroduction stimulates insulin, driving intracellular shifts of phosphate, potassium and magnesium, increasing thiamine utilisation and risking oedema, cardiac arrhythmia and respiratory failure — the refeeding syndrome spectrum. Prevention is protocolised nutrition with thiamine and serial electrolytes, not improvisation.[8][21]
Genetics. Large-scale GWAS of AN identifies multiple risk loci and supports a metabo-psychiatric model rather than a purely sociocultural explanation — useful for family psychoeducation without genetic determinism.[16]
Clinical presentation
AN. Progressive restriction, rules about “safe” foods, fear of fatness or weight gain, body checking/avoidance, compulsive exercise, cold intolerance, lanugo, constipation, irritability, social withdrawal, and secondary amenorrhoea or delayed menarche. Insight ranges from good to poor; overvalued ideas can appear near-delusional without being primary psychosis.[20][22]
BN. Secret binge episodes, purging (vomiting, laxatives, diuretics), fasting or driven exercise, shame, and often normal weight. Medical clues: parotid hypertrophy, dental enamel erosion, Russell sign (knuckle calluses), reflux, irregular menses.[20][24]
BED. Recurrent binge eating with loss of control, eating alone due to embarrassment, marked distress; compensation is not regular. Weight may be elevated but is not diagnostic.[19]
ARFID. Longstanding selective eating, fear of choking after an incident, or apparent low drive to eat, with nutritional deficiency or growth faltering without weight/shape overvaluation.[23]
Atypical AN. Marked restriction and fear of weight gain after substantial loss from a higher starting weight — can present with identical medical instability to classic AN.[5]
Differential diagnosis
| Differential | Discriminators | Why it matters |
|---|---|---|
| Coeliac / IBD / hyperthyroidism / diabetes / malignancy | GI red flags, polyuria/polydipsia, night sweats, focal signs | Organic disease can kill if missed |
| Depression with appetite loss | Low mood primary; less weight phobia ritual | Treat mood but do not miss AN |
| OCD food contamination | Contamination logic vs shape overvaluation | ERP targets differ; can co-occur |
| Psychosis food delusion | Primary delusions/hallucinations | Antipsychotic pathway differs |
| ASD selective eating | Developmental history; sensory profile | Overlaps ARFID; adapt care |
| BDD | Appearance preoccupation not mainly weight | Different OCRD pathway |
| Substance / stimulant misuse | Appetite suppression, intoxication signs | Safety and toxicology |
Always exclude or co-manage organic causes when onset is atypical, weight loss is extreme without classic AN psychology, or systemic red flags exist.[2][20][22]
Clinical and bedside assessment
Structure the interview for the adolescent and carers: onset and rate of weight change; 24-hour intake; binge/purge methods and frequency; exercise; cold, fainting, chest pain, palpitations; menses; self-harm and suicide; substances; diabetes (insulin omission); family meals and accommodation; school attendance; prior treatment fidelity.[2][5]
Physical parameters that decide setting. Heart rate, blood pressure lying and standing, temperature, hydration, capillary glucose when indicated, ECG (bradycardia, QTc, arrhythmia), growth chart plotting and % median BMI for age/sex, and signs of purging complications.[5][20][25]
MSE. Body-image beliefs, fear of weight gain, insight, motivation stage, cognitive effects of starvation, and risk (suicide, medical non-adherence). Capacity is decision-specific — a young person may have capacity for some decisions and not for life-saving refeeding when illness distorts risk appraisal.[2][3]
Investigations and measurement
Baseline and monitoring set (typical adolescent restrictive ED work-up). Full blood count; urea and electrolytes including phosphate, magnesium and calcium; liver enzymes; glucose; thyroid function when indicated; coeliac serology when GI differential applies; pregnancy test when relevant; ECG. Consider bone densitometry after prolonged malnutrition or amenorrhoea per specialist paediatric guidance. Imaging or endoscopy only when organic differential is active — not as a routine “AN test.”[5][20]
Severity tracking uses weight trajectory / %mBMI, vital signs, electrolytes during refeeding, and structured symptom measures (for example EDE-Q concept in research/clinical practice) — never a single number alone.[2][5]
Management — medical resuscitation and admission thresholds
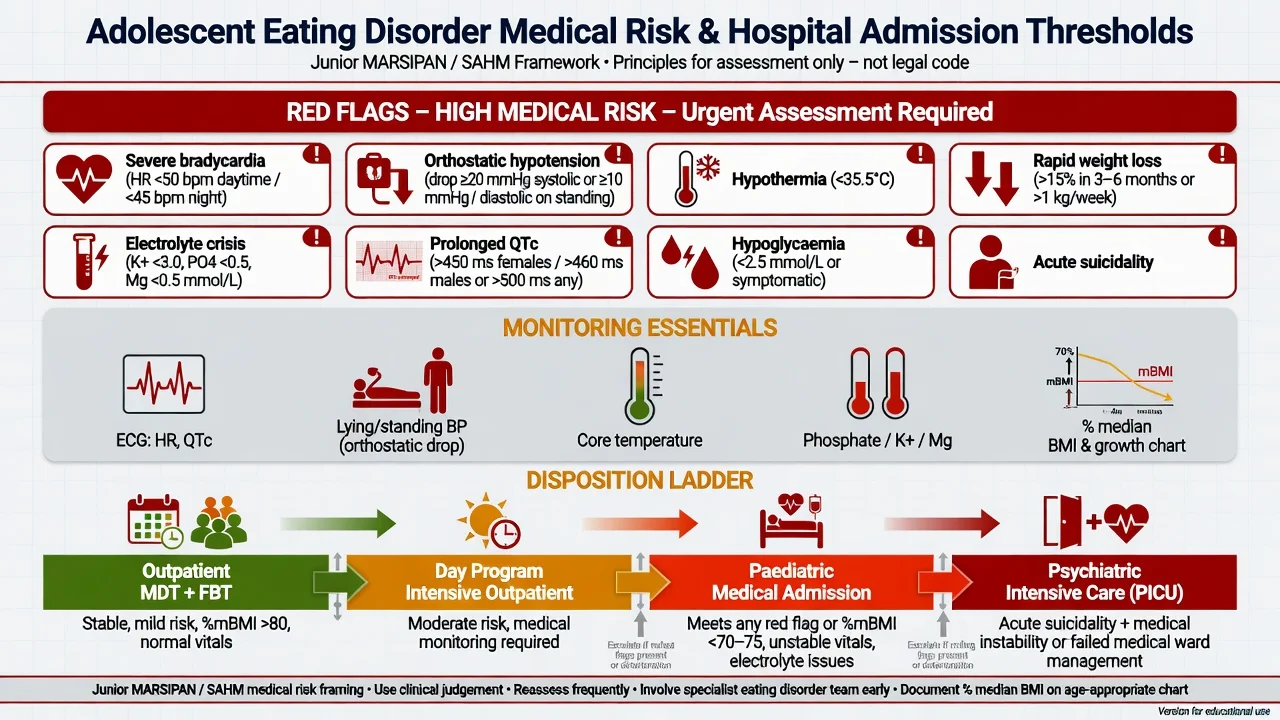
Admission decision framework (principles). Society for Adolescent Health and Medicine guidance and Junior MARSIPAN-style frameworks emphasise physiological risk, rate of weight loss, electrolytes/ECG, and ability to eat safely in the community, not weight cut-offs alone. Exact numerical cut-offs vary by local protocol — quote your hospital’s paediatric ED pathway and do not invent universal section numbers.[5][25]
On the medical ward: correct life threats first (ABC, glucose, electrolytes, arrhythmia), then commence protocolised refeeding with thiamine, frequent phosphate/K/Mg checks, vital signs, and ECG as indicated. Liaison psychiatry addresses distress, compulsive exercise, food refusal behaviours, self-harm, and family containment without undermining medical safety.[5][8][21]
Refeeding — modern evidence
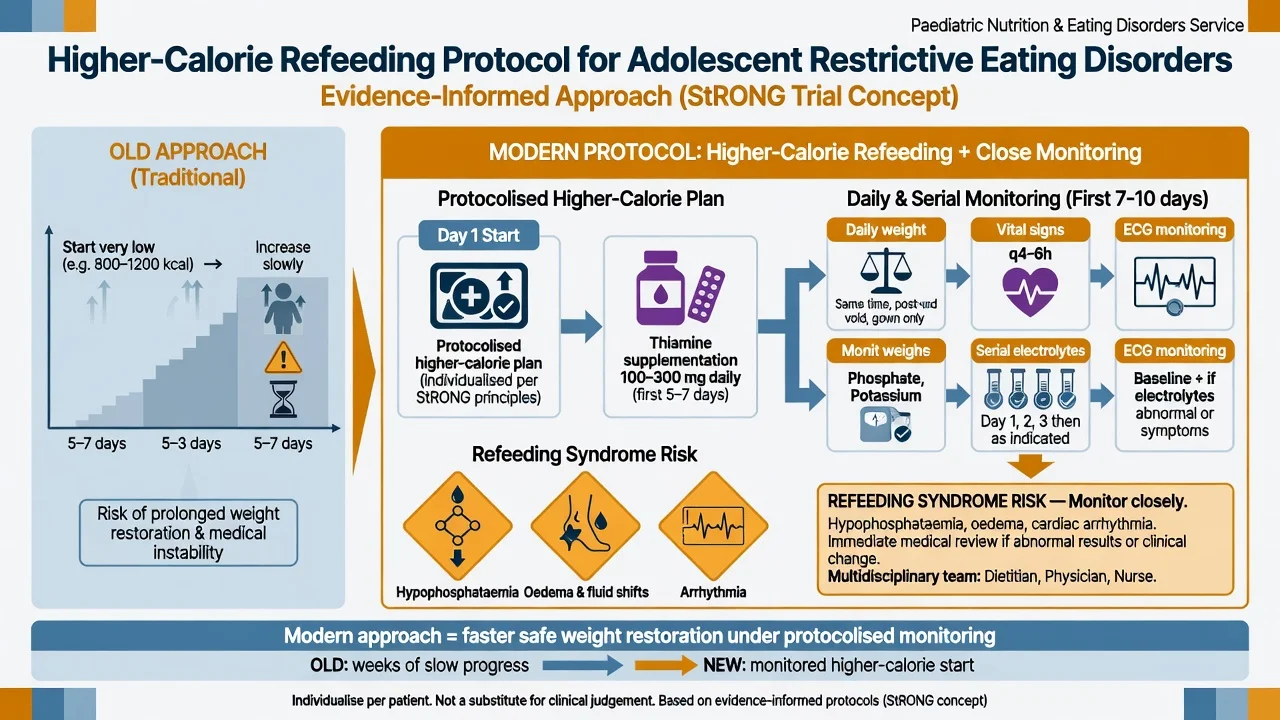
Historically, very low starting calories were used to avoid refeeding syndrome. Systematic review work highlighted heterogeneity of approaches and the need for better trials.[8] The multicentre Study of Refeeding to Optimize Inpatient Gains (StRONG) randomised adolescents and young adults with AN to higher-calorie versus lower-calorie refeeding and found faster weight restoration with higher-calorie refeeding without increased refeeding-related adverse events under structured monitoring in the short term.[6] One-year follow-up supported safety and outcome considerations of higher-calorie refeeding pathways.[7]
Exam stance: use a protocol (local paediatric ED / dietetic pathway), give thiamine, monitor phosphate, potassium, magnesium, and do not freestyle calories. Treat refeeding syndrome as a preventable medical emergency.[6][8][21]
Management — definitive psychological and pharmacological care
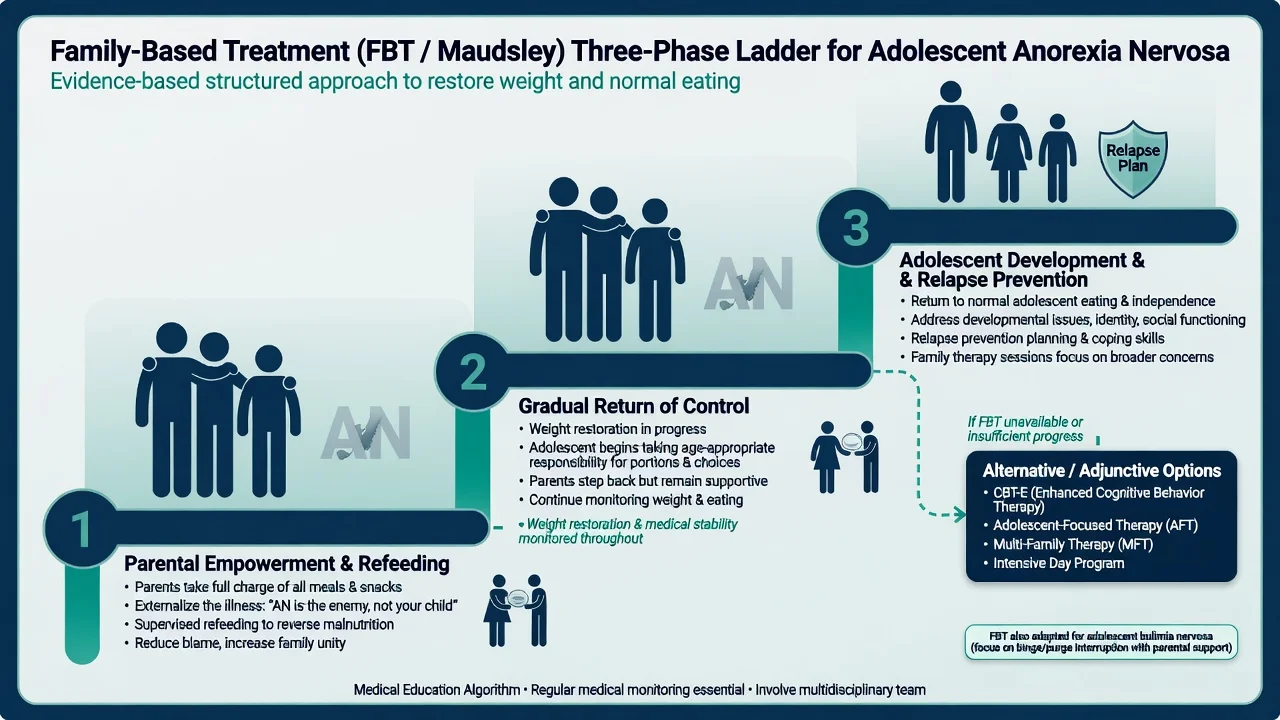
Family-based treatment (FBT / Maudsley)
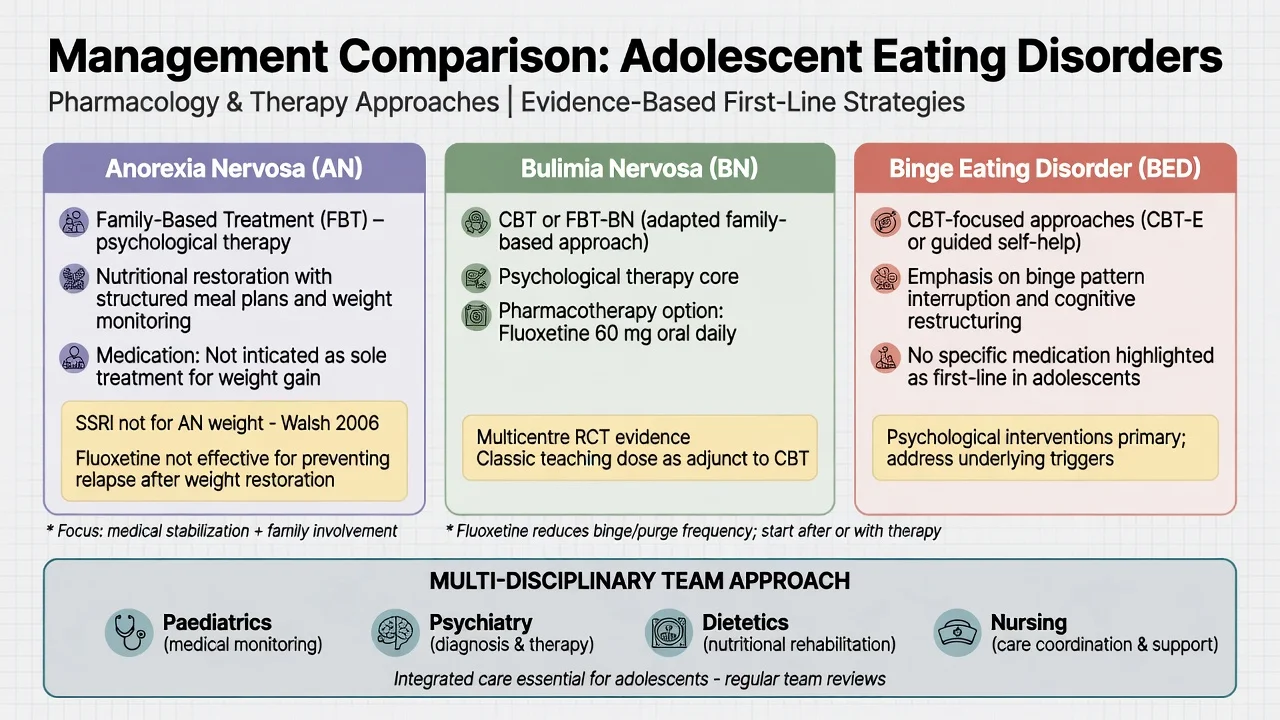
FBT is first-line psychological treatment for most medically stable adolescents with AN in RANZCP and major international guidelines. Core principles: agnostic aetiology (do not blame parents), externalise the illness, empower parents to take charge of refeeding in Phase 1, return control of eating to the adolescent in Phase 2 as weight restores, and address adolescent developmental issues and relapse prevention in Phase 3.[1][2][3][4]
Landmark RCT evidence: Lock and colleagues randomised adolescents with AN to FBT versus adolescent-focused individual therapy (AFT); FBT produced superior full remission rates at follow-up, establishing FBT as the evidence standard candidates must name.[1] Meta-analysis supports efficacy of FBT for adolescents with eating disorders.[4]
For adolescent BN, randomised comparison showed family-based treatment superior to supportive psychotherapy on binge–purge outcomes — examiners may ask FBT adaptations for BN (parental support for meal structure and reducing binge–purge opportunities while preserving developmentally appropriate autonomy where safe).[12]
Other psychological options
CBT-E (enhanced cognitive behaviour therapy) targets the transdiagnostic maintaining mechanisms of overvaluation of shape/weight, dietary restraint and mood intolerance; it is especially relevant for non-underweight presentations, BN, and older adolescents when FBT is unsuitable or declined, with randomised comparison against IPT in mixed eating-disorder samples supporting CBT-E effects.[18] Adolescent-focused therapy remains an alternative when FBT is not available or not appropriate. Day-patient models after short inpatient stabilisation can be non-inferior to prolonged inpatient care in selected adolescents (ANDI trial), supporting stepped intensity rather than automatic long admissions.[17]
For adolescent BED, age-adapted CBT has randomised clinical trial support for binge reduction.[19]
Pharmacotherapy — the exam traps
| Scenario | Exam answer | Evidence anchor |
|---|---|---|
| Adolescent BN + CBT/FBT | Consider fluoxetine; classic multicentre efficacy at 60 mg oral daily (titrate; monitor activation, suicidality, sexual/GI effects) | Fluoxetine BN Collaborative Study; long-term continuation data |
| Weight-restored AN relapse prevention | Do not rely on fluoxetine — RCT showed no benefit over placebo after weight restoration | Walsh et al. JAMA 2006 |
| AN weight gain as primary drug goal | Medication is not sole treatment; nutritional + psychological care first | RANZCP / APA guidelines |
| Severe AN with high anxiety (specialist) | Adjunctive olanzapine studied mainly in adult outpatients — modest BMI effect; metabolic monitoring; not a paediatric first-line default | Attia et al. 2019 |
Fluoxetine multicentre placebo-controlled data established efficacy in BN, with 60 mg daily the dose most clearly superior in classic teaching from the collaborative trial; longer-term fluoxetine treatment studies support maintenance benefit in BN responders.[10][11][24] Systematic review of BN RCTs supports CBT and antidepressant evidence more broadly.[24]
In AN after weight restoration, fluoxetine did not prevent relapse versus placebo in a rigorous RCT — a high-yield negative result.[9] Olanzapine versus placebo in adult outpatients with AN showed greater BMI increase with olanzapine but is not a substitute for refeeding and specialist psychological care; metabolic and QTc monitoring apply; paediatric use is specialist and off-guideline-as-first-line in many pathways.[15]
Never present an SSRI as the treatment that “makes them eat” in AN. Combine pharmacotherapy with psychological care and medical monitoring; assess suicidality when starting antidepressants in adolescents.[2][3][9]
Specific subtypes and scenarios
Restricting vs binge-purge AN. Purging adds electrolyte and arrhythmia risk even at low weight; monitor potassium aggressively.[20]
Male and gender-diverse youth. Under-diagnosed; muscularity-oriented body ideals and exercise compulsion may dominate; same medical risk rules apply.[13]
Athletes. Relative energy deficiency, performance culture, and delayed presentation; negotiate return-to-sport criteria with medical clearance.[5]
Diabetes. Intentional insulin omission for weight control is a medical emergency interface; joint diabetes–ED care.[2][20]
ASD comorbidity. Sensory ARFID-like features may coexist with AN; FBT/CBT need adaptations (visual structure, reduced abstract body-image language when unhelpful).[23]
Complications and pitfalls
Medical complications span cardiovascular (bradycardia, arrhythmia, refeeding oedema), electrolyte, gastrointestinal (superior mesenteric artery syndrome, gastroparesis), endocrine/bone, haematological, and dental domains in purging disorders.[20]
Classic pitfalls: discharging on BMI alone; missing atypical AN; starting refeeding without phosphate checks; blaming parents instead of empowering them in FBT; calling any family meeting “FBT”; using fluoxetine for AN weight restoration contrary to evidence; ignoring suicide risk; colluding with secrecy and under-weighing without a protocol.[2][5][9]
Prognosis and disposition
Earlier intervention and full weight restoration in adolescence improve outcomes relative to chronic adult courses, but relapse risk remains. Poor prognostic markers include longer duration untreated, lower nadir weight, purging, family conflict that blocks FBT, and multimorbidity.[13][14][22]
Stepped care. Outpatient FBT/MDT → intensive outpatient or day program → paediatric medical admission for instability → specialist psychiatric inpatient when behavioural intensity or risk exceeds medical-ward capacity. Plan transition to adult services before birthday cliffs.[2][3][17]
Special populations
Pre-pubertal and early-onset AN threaten linear growth and bone accrual — urgency of restoration is higher. Pregnancy is rare but high risk if it occurs. Cultural formulation matters in ANZ care, including Indigenous family structures and access barriers — avoid one-size communication scripts.[2][5]
Capacity, consent and legal principles
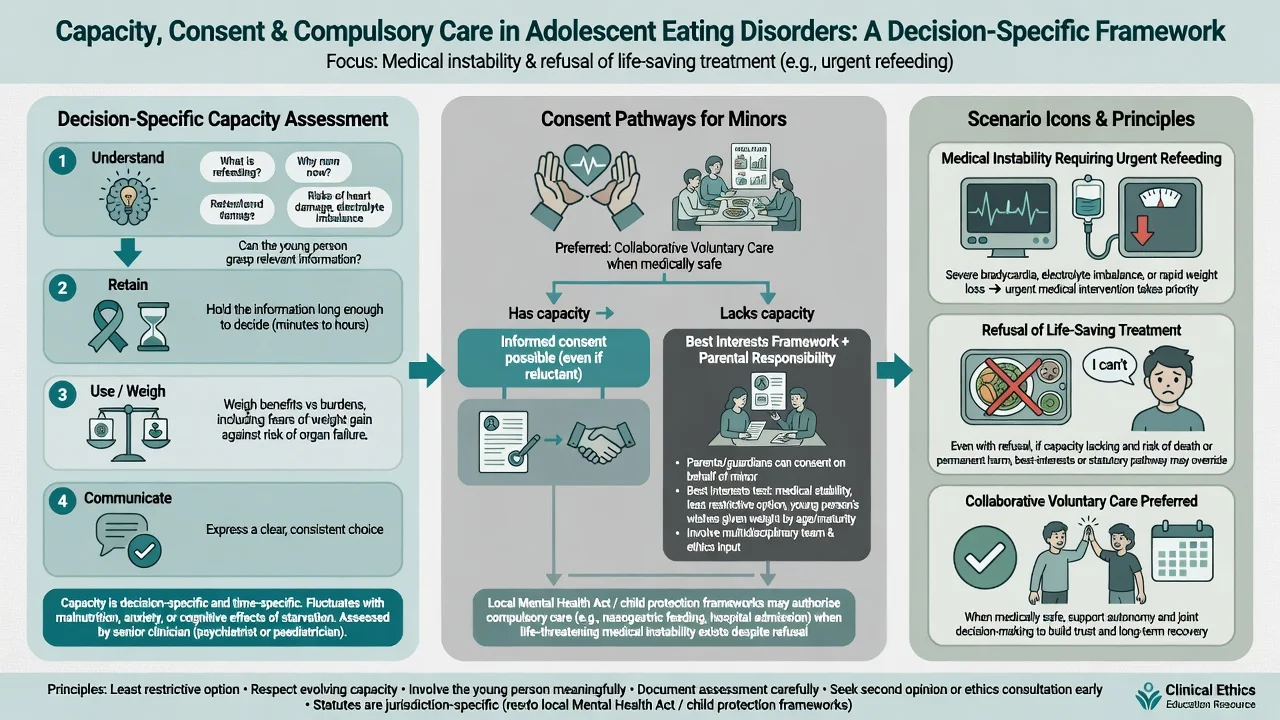
Assess capacity for the specific decision (for example agreeing to medical admission and refeeding): understand, retain, use/weigh, communicate. Starvation and overvalued ideas can impair weighing of medical risk. For minors, parental responsibility and best-interests frameworks usually govern; mature-minor/Gillick-type principles apply in some jurisdictions for some decisions. When life-saving treatment is refused and capacity is lacking, use local mental health, child protection, or inherent jurisdiction pathways — name the jurisdiction; do not invent section numbers for the wrong country.[2][3][25]
Evidence, guidelines and regional differences
ANZ (RANZCP 2014). Comprehensive ED guideline: multi-disciplinary care, FBT for adolescents with AN, medical risk management, cautious pharmacotherapy positioning.[2]
US (APA 2023). Updated practice guideline for eating disorders — assessment, levels of care, psychological treatments, and medication evidence summaries including BN pharmacotherapy and limited AN medication role.[3]
UK. NICE eating disorders guidance (NG69 principles): family therapy for children and young people with AN as first-line psychological treatment; do not offer medication as sole treatment for AN; medical risk monitoring. Junior MARSIPAN structures care of the really sick young person with AN.[25]
Medical risk. SAHM position paper and paediatric protocols guide physiological parameters and admission thinking globally.[5]
Landmark trials to name at viva: Lock 2010 FBT vs AFT; Couturier FBT meta-analysis; le Grange FBT for adolescent BN; StRONG higher-calorie refeeding; Walsh fluoxetine-negative after weight restoration in AN; Fluoxetine BN Collaborative Study; Attia olanzapine adult AN; ANDI day-patient non-inferiority; Hilbert CBT for adolescent BED.[1][4][6][9][10][12][15][17][19]
Exam pearls
FBT phases (exam string)
- Amenorrhoea is not required for DSM-5 AN.[3][22]
- Atypical AN can be as unstable as classic AN.[5]
- Fluoxetine 60 mg oral daily is the classic BN evidence dose; fluoxetine fails as AN relapse prevention after weight restoration.[9][10]
- Higher-calorie refeeding can be safe and faster with monitoring (StRONG) — not an excuse to skip phosphate checks.[6][7]
- Capacity is decision-specific; legal tools are jurisdiction-specific.[2][3]
References
- [1]Lock J, Le Grange D, Agras WS, Moye A, Bryson SW, Jo B. Randomized clinical trial comparing family-based treatment with adolescent-focused individual therapy for adolescents with anorexia nervosa Arch Gen Psychiatry, 2010.PMID 20921118
- [2]Hay P, Chinn D, Forbes D, Madden S, Newton R, Sugenor L, Touyz S, Ward W, Royal Australian and New Zealand College of Psychiatrists. Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for the treatment of eating disorders Aust N Z J Psychiatry, 2014.PMID 25351912
- [3]Crone C, Fochtmann LJ, Attia E, Boland R, Escobar J, Fornari V, Golden N, Guarda A, Jackson-Triche M, et al. The American Psychiatric Association Practice Guideline for the Treatment of Patients With Eating Disorders Am J Psychiatry, 2023.PMID 36722117
- [4]Couturier J, Kimber M, Szatmari P. Efficacy of family-based treatment for adolescents with eating disorders: a systematic review and meta-analysis Int J Eat Disord, 2013.PMID 22821753
- [5]Society for Adolescent Health and Medicine, Golden NH, Katzman DK, Sawyer SM, Ornstein RM, Rome ES, et al. Position Paper of the Society for Adolescent Health and Medicine: medical management of restrictive eating disorders in adolescents and young adults J Adolesc Health, 2015.PMID 25530605
- [6]Garber AK, Cheng J, Accurso EC, Adams SH, Buckelew SM, Kapphahn CJ, Kreiter A, Le Grange D, Machen VI, et al. Short-term Outcomes of the Study of Refeeding to Optimize Inpatient Gains for Patients With Anorexia Nervosa: A Multicenter Randomized Clinical Trial JAMA Pediatr, 2021.PMID 33074282
- [7]Golden NH, Cheng J, Kapphahn CJ, Buckelew SM, Machen VI, Kreiter A, Accurso EC, Adams SH, Le Grange D, et al. Higher-Calorie Refeeding in Anorexia Nervosa: 1-Year Outcomes From a Randomized Controlled Trial Pediatrics, 2021.PMID 33753542
- [8]Garber AK, Sawyer SM, Golden NH, Guarda AS, Katzman DK, Kohn MR, Le Grange D, Madden S, Whitelaw M, et al. A systematic review of approaches to refeeding in patients with anorexia nervosa Int J Eat Disord, 2016.PMID 26661289
- [9]Walsh BT, Kaplan AS, Attia E, Olmsted M, Parides M, Carter JC, Pike KM, Devlin MJ, Woodside B, et al. Fluoxetine after weight restoration in anorexia nervosa: a randomized controlled trial JAMA, 2006.PMID 16772623
- [10]Fluoxetine Bulimia Nervosa Collaborative Study Group. Fluoxetine in the treatment of bulimia nervosa. A multicenter, placebo-controlled, double-blind trial Arch Gen Psychiatry, 1992.PMID 1550466
- [11]Goldstein DJ, Wilson MG, Thompson VL, Potvin JH, Rampey AH Jr. Long-term fluoxetine treatment of bulimia nervosa. Fluoxetine Bulimia Nervosa Research Group Br J Psychiatry, 1995.PMID 7620754
- [12]le Grange D, Crosby RD, Rathouz PJ, Leventhal BL. A randomized controlled comparison of family-based treatment and supportive psychotherapy for adolescent bulimia nervosa Arch Gen Psychiatry, 2007.PMID 17768270
- [13]Smink FR, van Hoeken D, Hoek HW. Epidemiology of eating disorders: incidence, prevalence and mortality rates Curr Psychiatry Rep, 2012.PMID 22644309
- [14]Arcelus J, Mitchell AJ, Wales J, Nielsen S. Mortality rates in patients with anorexia nervosa and other eating disorders. A meta-analysis of 36 studies Arch Gen Psychiatry, 2011.PMID 21727255
- [15]Attia E, Steinglass JE, Walsh BT, Wang Y, Wu P, Schreyer C, Wildes J, Yilmaz Z, Guarda AS, et al. Olanzapine Versus Placebo in Adult Outpatients With Anorexia Nervosa: A Randomized Clinical Trial Am J Psychiatry, 2019.PMID 30654643
- [16]Watson HJ, Yilmaz Z, Thornton LM, Hübel C, Coleman JRI, Gaspar HA, Bryois J, Hinney A, Leppä VM, et al. Genome-wide association study identifies eight risk loci and implicates metabo-psychiatric origins for anorexia nervosa Nat Genet, 2019.PMID 31308545
- [17]Herpertz-Dahlmann B, Schwarte R, Krei M, Egberts K, Warnke A, Wewetzer C, Pfeiffer E, Fleischhaker C, et al. Day-patient treatment after short inpatient care versus continued inpatient treatment in adolescents with anorexia nervosa (ANDI): a multicentre, randomised, open-label, non-inferiority trial Lancet, 2014.PMID 24439238
- [18]Fairburn CG, Bailey-Straebler S, Basden S, Doll HA, Jones R, Murphy R, O'Connor ME, Cooper Z. A transdiagnostic comparison of enhanced cognitive behaviour therapy (CBT-E) and interpersonal psychotherapy in the treatment of eating disorders Behav Res Ther, 2015.PMID 26000757
- [19]Hilbert A, Petroff D, Neuhaus P, Schmidt R. Cognitive-Behavioral Therapy for Adolescents with an Age-Adapted Diagnosis of Binge-Eating Disorder: A Randomized Clinical Trial Psychother Psychosom, 2020.PMID 31533113
- [20]Westmoreland P, Krantz MJ, Mehler PS. Medical Complications of Anorexia Nervosa and Bulimia Am J Med, 2016.PMID 26169883
- [21]Mehanna HM, Moledina J, Travis J. Refeeding syndrome: what it is, and how to prevent and treat it BMJ, 2008.PMID 18583681
- [22]Zipfel S, Giel KE, Bulik CM, Hay P, Schmidt U. Anorexia nervosa: aetiology, assessment, and treatment Lancet Psychiatry, 2015.PMID 26514083
- [23]Katzman DK, Spettigue W, Agostino H, Couturier J, Dominic A, Findlay SM, Lam PY, Lane M, Maguire B, et al. Incidence and Age- and Sex-Specific Differences in the Clinical Presentation of Children and Adolescents With Avoidant Restrictive Food Intake Disorder JAMA Pediatr, 2021.PMID 34633419
- [24]Shapiro JR, Berkman ND, Brownley KA, Sedway JA, Lohr KN, Bulik CM. Bulimia nervosa treatment: a systematic review of randomized controlled trials Int J Eat Disord, 2007.PMID 17370288
- [25]Marikar D, Reynolds S, Moghraby OS. Junior MARSIPAN (Management of Really Sick Patients with Anorexia Nervosa) Arch Dis Child Educ Pract Ed, 2016.PMID 26407730