Psych · Child and adolescent psychiatry — elimination disorders
Elimination disorders: enuresis and encopresis
Also known as Nocturnal enuresis · Bedwetting · Diurnal enuresis · Encopresis · Faecal soiling · Fecal incontinence children · Monosymptomatic nocturnal enuresis · Functional constipation with overflow
Exam-exhaustive fellowship reference on childhood elimination disorders — DSM-5-TR and ICCS classification, enuresis pathophysiology triad, alarm versus desmopressin strategy, encopresis with constipation management (disimpaction and PEG), comorbidity and non-punitive care. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Elimination disorders are high-yield CAP stations across FRANZCP, MRCPsych, ABPN and MD/DNB. Examiners test age thresholds, primary versus secondary and ICCS mono- versus non-monosymptomatic language, the alarm-for-cure / desmopressin-for-dryness contrast, desmopressin hyponatraemia and imipramine toxicity traps, and the insight that most encopresis is overflow from constipation, not wilful soiling.[1][2][3][4][9]
Overview and definition
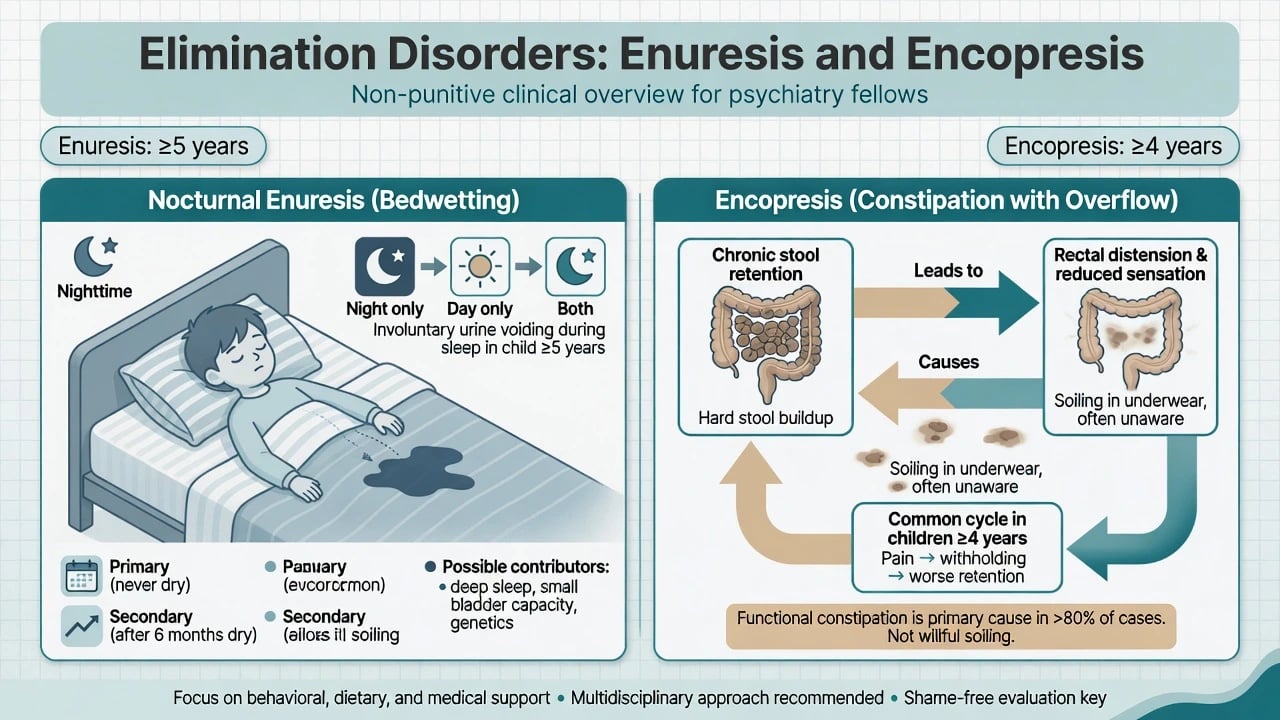
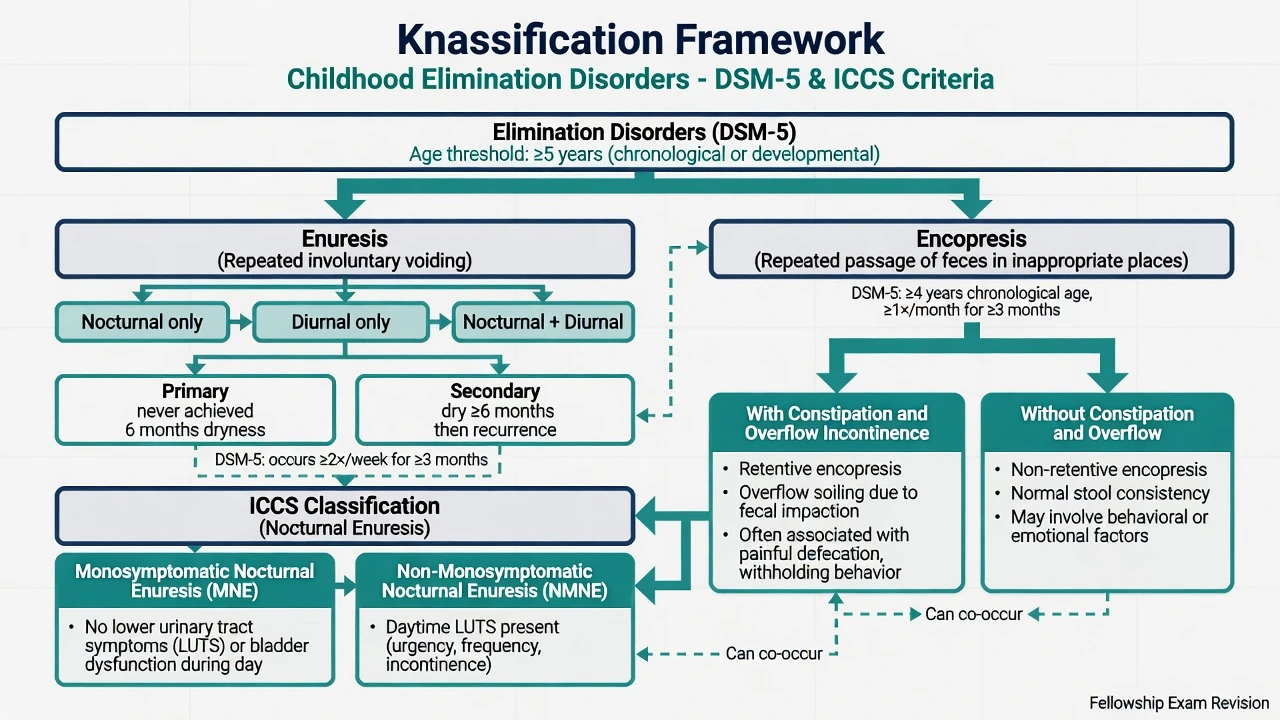
Enuresis is repeated voiding of urine into bed or clothes, whether involuntary or intentional, meeting frequency/duration or impairment criteria, after the child has reached a chronological age of at least 5 years (or equivalent developmental level), not solely explained by a substance or another medical condition.[1]
Encopresis is repeated passage of faeces into inappropriate places (for example clothing or floor), involuntary or intentional, at least once a month for at least 3 months, after chronological age at least 4 years (or equivalent developmental level), not exclusively due to a substance or medical condition except through the mechanism of constipation.[10][11]
Fellowship answers should hold both DSM-5-TR psychiatric nosology and ICCS continence language used by paediatrics and urology.[2][3]
Classification
Enuresis — skeleton candidates must own
| Axis | Distinctions |
|---|---|
| Timing (DSM) | Nocturnal only · Diurnal only · Nocturnal and diurnal |
| Course | Primary — never achieved sustained dryness · Secondary — relapse after a dry period (commonly taught as ≥6 months continence) |
| ICCS phenotype | MNE (monosymptomatic nocturnal enuresis) — night wetting without significant daytime LUTS · NMNE — night wetting plus daytime lower urinary tract symptoms |
| Frequency | DSM frequency threshold classically ≥2×/week for ≥3 months, or clinically significant distress/impairment |
ICCS terminology standardises lower urinary tract language in children and adolescents and underpins MNE versus NMNE teaching used in urology-aligned care pathways.[2][3] AACAP's practice parameter remains a core psychiatry-facing assessment and treatment skeleton for enuresis in exams.[1]
Encopresis — skeleton
| Specifier | Clinical meaning |
|---|---|
| With constipation and overflow incontinence | Retained stool, rectal loading, liquid/soft stool leaks around the mass; often misread as "diarrhoea" |
| Without constipation and overflow | Non-retentive soiling; higher behavioural/psychiatric interface; do not treat with endless laxatives if constipation is absent |
Functional faecal retention with encopresis is the dominant clinical pathway in paediatric series describing retentive soiling.[11]
MNE
- Night wetting only
- No major daytime LUTS
- Alarm or desmopressin pathway
- Usually clinical diagnosis
NMNE
- Daytime urgency/frequency/incontinence
- Often bowel-bladder dysfunction
- Treat daytime symptoms and constipation
- More specialist work-up
Retentive encopresis
- Constipation + overflow
- Withholding cycle
- Disimpact then maintain
- Most school-age soiling
Non-retentive
- No significant constipation
- Behavioural formulation
- Toileting programme
- Avoid useless chronic laxatives
Epidemiology and risk
Numbers candidates should own
Nocturnal enuresis is common in early school years and falls with age; residual adolescent and adult enuresis is less common but highly impairing for social development. Familial aggregation is well recognised for nocturnal enuresis phenotypes. Constipation, developmental delay, ADHD, ASD, sleep problems, psychosocial stress, and harsh toilet training environments cluster with both wetting and soiling presentations.[1][13]
Pathophysiology
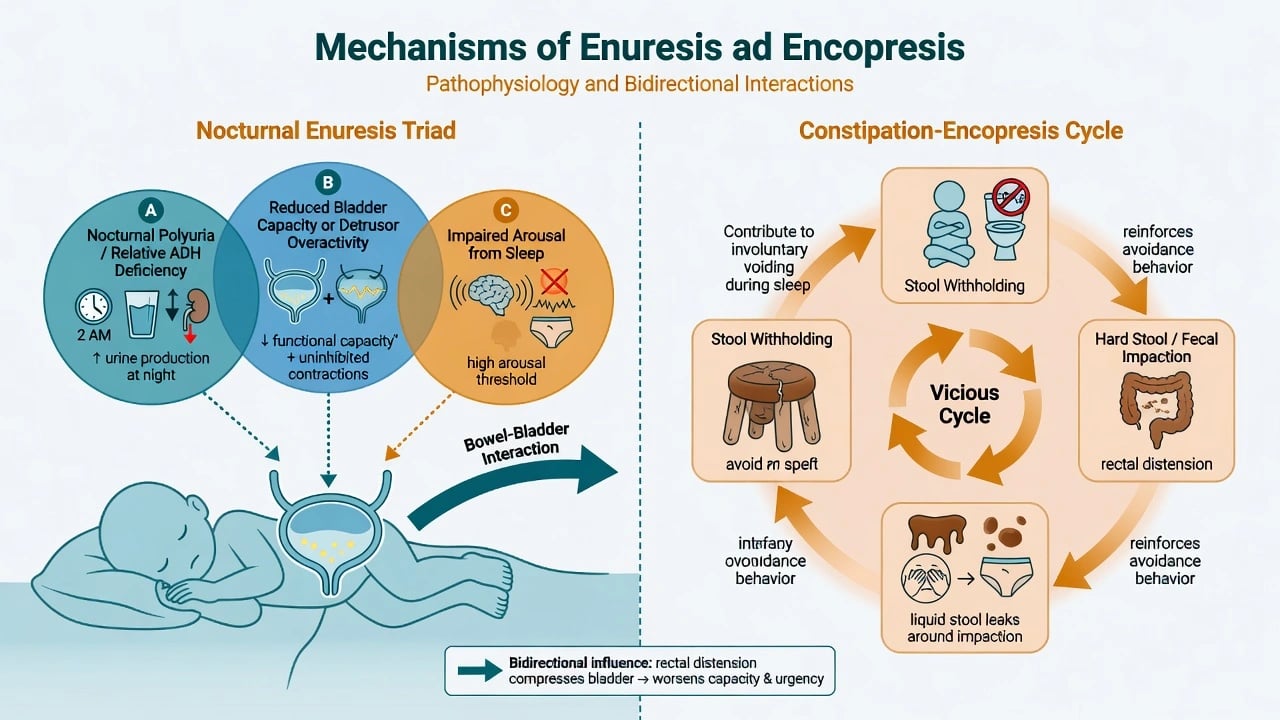
Nocturnal enuresis triad (Butler framework, ICCS-aligned teaching): (1) nocturnal polyuria — relative excess night urine production often linked to nocturnal vasopressin dynamics or evening fluid load; (2) reduced nocturnal bladder capacity or detrusor overactivity; (3) impaired arousal from sleep so the child does not wake to void. Individual children load differently on these factors; treatment matching (alarm conditioning versus antidiuretic strategy) follows the formulation.[2][13]
Constipation–encopresis cycle: pain or large stool → withholding → harder stool and rectal distension → reduced urge awareness → overflow soiling → shame and further avoidance of the toilet. Rectal loading also compresses the bladder and worsens urinary symptoms — the bowel–bladder axis examiners expect you to name.[9][11]
Clinical presentation
Enuresis history. Night only versus day; primary versus secondary; frequency and volume; dry spells; evening fluids; constipation markers; snoring/sleep-disordered breathing clues; family history; impact on sleepovers, camps, bullying, and parental intolerance.[1][4][13]
Encopresis history. Stained underwear, overflow liquid stool mistaken for diarrhoea, stool withholding postures, toilet refusal, large-calibre stools, abdominal pain, diet and toileting schedule, prior punitive responses.[9][11]
Impact language for MSE/formulation. Shame, secrecy, low mood, school avoidance, sibling conflict, carer burnout. Avoid moralistic wording ("lazy", "dirty", "attention-seeking") in notes and in front of the child.[1][10]
Differential diagnosis
Discriminators, not shopping lists:
- UTI / diabetes / CKD / structural uropathy — secondary onset, polyuria/polydipsia, dysuria, weight loss, continuous wetting (ectopic ureter in girls), abnormal growth or BP.[1][2]
- Neurogenic bladder/bowel — spinal stigmata, neurological signs, gait change, known neural tube defects.[2]
- Hirschsprung disease and other organic constipation — especially early severe constipation from infancy, failure to pass meconium history, red-flag GI features.[9]
- Medication effects — opioids, anticholinergics, some psychotropics altering bowel or bladder function.
- Maltreatment / trauma context — secondary incontinence can accompany adversity; soiling alone does not diagnose sexual abuse, but coercive toileting and other safeguarding indicators demand action.[1]
- Oppositional intentional soiling — possible after full medical exclusion and constipation treatment; still requires behavioural formulation, not punishment.
Assessment
Structure: phenotype + age threshold + primary/secondary + constipation + daytime LUTS + comorbidity + impact + parental response + red flags.[1][2][4]
- Confirm DSM age and frequency/impairment thresholds for enuresis or encopresis.
- Obtain a bladder and bowel diary (wet/dry nights, voids, stools, fluids) for 1–2 weeks when practical.[2][4]
- Screen constipation systematically even when the referral says "bedwetting only".[9][11]
- Classify MNE versus NMNE; map encopresis retentive versus non-retentive.[2][3]
- Screen ADHD, ASD, anxiety, learning, sleep, bullying, and family conflict.[1]
- Examine: growth, abdomen for faecal mass, spine, lower-limb neurology; genital examination only when indicated, with chaperone and sensitive consent.[1][2]
- Assess parental intolerance and any punitive practices — these predict engagement failure and psychological harm.[13]
Investigations
Most primary MNE is a clinical diagnosis. Investigate when secondary onset, daytime symptoms, polyuria/polydipsia, failure to respond, recurrent UTI, abnormal examination, or continuous wetting raise organic concern.[1][2]
- Urinalysis (± culture) when infection or secondary onset is possible.
- Glucose testing if polyuria, polydipsia, weight loss, or glycosuria risk.
- Renal/bladder ultrasound, uroflow, post-void residual, specialist urology for NMNE, continuous wetting, recurrent UTI, neurological signs, or treatment resistance.[2]
- Encopresis/constipation: clinical diagnosis preferred; avoid routine unnecessary radiation; specialist GI tests for red flags per paediatric guidance.[9]
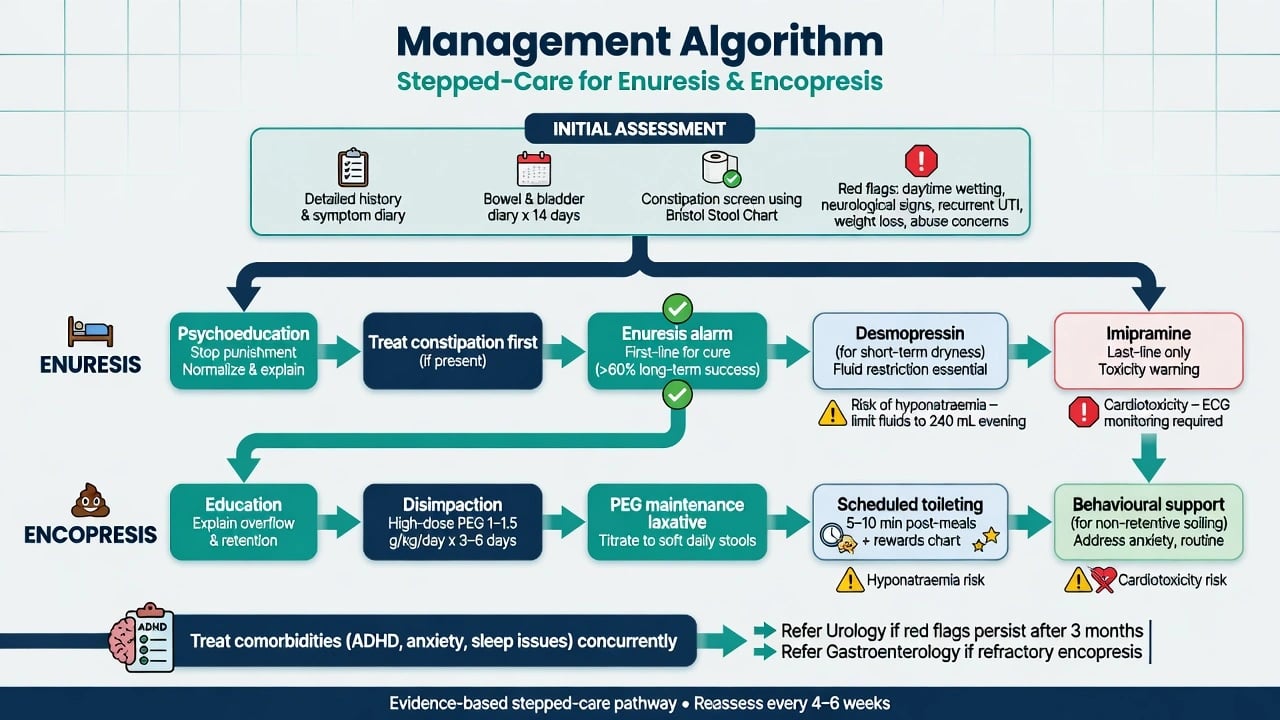
Before imipramine: cardiac history, consideration of ECG, and overdose-safety counselling. Before desmopressin: teach fluid restriction and hyponatraemia warning symptoms.[6][7][14]
Acute safety
Definitive management
Universal first steps (both disorders)
- Psychoeducation: common, usually involuntary, not laziness; stop punishment and shaming.[1][4]
- Treat constipation aggressively when present — wetting often improves when the bowel is cleared.[9][11]
- Optimise daytime voiding habits, fibre/fluid pattern appropriate to age, and toilet access at school.[1][2]
- Treat ADHD, anxiety, sleep problems and family conflict in parallel — they drive adherence failure.[1]
Enuresis — durable dryness versus short-term dryness
Enuresis alarm (first-line for cure). Conditioning treatment using a moisture sensor that wakes the child (and carers) at wetting. Cochrane synthesis supports alarm therapy as effective for achieving dryness; benefits are more likely to persist after treatment ends than with short-term drug-only approaches.[5] Meta-analytic comparison of alarm versus desmopressin for monosymptomatic enuresis supports superior sustained response with alarm strategies when the goal is durable cure.[8] NICE bedwetting guidance summarises alarm and desmopressin roles for UK-aligned exam answers.[4] AACAP similarly positions behavioural/alarm approaches centrally for many children seeking lasting dryness.[1]
Practical alarm pearls: family readiness, shared night-time plan, enough nights in a row, treat constipation first, and do not abandon after a few wet nights. Parental intolerance predicts drop-out.[5][13]
Desmopressin (short-term dryness). Synthetic antidiuretic analogue reducing nocturnal urine volume. Cochrane evidence supports efficacy for night dryness during treatment; relapse is common when stopped. Best uses: camps, sleepovers, or when alarm is impractical/failed/refused.[6] Prefer oral or oral-lyophilisate formulations where available; restrict evening free water; counsel headache, vomiting, hyponatraemia risk.[6][14]
Exam-level dosing framework (always individualise; check local product information and specialist advice):
| Agent | Typical paediatric framework | Monitoring / safety |
|---|---|---|
| Desmopressin oral / melt | Often start around 0.2 mg oral at bedtime (or age/weight-appropriate melt equivalent); some pathways titrate toward 0.4 mg if needed and tolerated — verify PI | Evening fluid restriction; stop if vomiting/diarrhoea; hyponatraemia symptoms; intermittent drug holidays as locally advised |
| Imipramine | Historical effective agent; third-line specialist only in modern pathways | Overdose lethality, arrhythmia risk, anticholinergic effects; safe storage; ECG considerations |
Imipramine and related tricyclics reduce wet nights versus placebo in Cochrane synthesis but carry a poorer safety profile than alarm or desmopressin for routine use — reserve for refractory specialist pathways.[7]
Anticholinergics (for example oxybutynin) may adjunct selected daytime overactive bladder / NMNE presentations under paediatric urology/continence guidance — not first-line monotherapy for pure MNE.[2]
Encopresis — treat the bowel first when retentive
ESPGHAN/NASPGHAN evidence-based recommendations for functional constipation structure the medical half of retentive encopresis care: education, disimpaction, then maintenance therapy to keep soft daily stools, plus toileting behaviour support.[9]
- Education — overflow is leakage around retained stool, not deliberate dirtiness.[9][11]
- Disimpaction — clear the loaded rectum/colon (oral high-dose osmotic regimens commonly preferred; enemas only with clear indication and non-punitive framing).[9]
- Maintenance — polyethylene glycol (PEG 3350) is a cornerstone osmotic option in children with chronic constipation with or without encopresis; titrate to soft daily stools for months, not days.[12] Exam framework often cites PEG 3350 oral titrated (commonly on the order of 0.5–1.5 g/kg/day in paediatric constipation pathways depending on phase and product — verify local PI and GI advice) with fluid intake and monitoring for diarrhoea/electrolyte issues in vulnerable children.[9][12]
- Toileting programme — sit 5–10 minutes after meals (gastrocolic reflex), foot support, reward charts for sitting and success, never punish accidents.[9][10]
- Behavioural/cognitive interventions add value especially for toileting refusal and non-retentive patterns; Cochrane supports behavioural approaches with or without other treatments for faecal incontinence in children.[10]
Non-retentive faecal incontinence: confirm absence of significant constipation; emphasise scheduled toileting, contingency management, school plan, and mental health intervention for anxiety/oppositional/trauma drivers rather than indefinite laxatives.[10][11]
Regional practice notes
ANZ practice typically routes uncomplicated MNE through primary care/paediatrics with continence services where available; CAMHS joins for comorbidity, trauma, severe family distress, or treatment refusal. Alarm first for durable dryness and desmopressin for situational dryness align with international evidence used in local teaching.[1][4][5]
Subtypes and scenarios
- Primary MNE, sleepover crisis: psychoeducation + desmopressin for the event + plan alarm for sustained cure.[4][6]
- Secondary enuresis: full organic and psychosocial review before assuming "stress only".[1]
- NMNE with constipation: clear bowel, daytime voiding schedule, then reassess night wetting.[2][9]
- Retentive encopresis mislabelled diarrhoea: stop antidiarrhoeals; disimpact and maintain.[9][11]
- ADHD + dual incontinence: treat ADHD and run structured toileting; do not wait for "perfect behaviour" before medical bowel care.[1]
- Adolescent residual enuresis: privacy-first care, peer stigma, shared decisions on alarm practicality versus medication windows.[4]
Complications and pitfalls
- Punishing wet or soiled nights.[1][13]
- Missing constipation while prescribing only enuresis drugs.[9][11]
- Desmopressin without fluid restriction → hyponatraemia.[6][14]
- Imipramine as first-line or accessible to younger siblings.[7]
- Labelling all soiling "behavioural" without disimpaction.[9][11]
- Alarm failure from inadequate instruction or family intolerance.[5][13]
- Ignoring school bullying and exclusion from camps.[1][4]
Prognosis and disposition
Spontaneous resolution of nocturnal enuresis is common across childhood, but waiting alone is not mandatory when impairment is high. Alarm therapy aims for sustained dryness; desmopressin usually works only while taken.[5][6][8] Retentive encopresis often needs months of maintenance laxatives; early cessation predicts relapse.[9][12]
Disposition. Uncomplicated MNE: primary care/paediatric continence pathway. Red flags or treatment resistance: paediatric urology. Refractory constipation/encopresis: paediatric gastroenterology. CAMHS: significant psychiatric comorbidity, trauma, severe parental–child conflict, or secondary psychological sequelae. Step intensity to impairment and risk, not to parental embarrassment alone.[1][2][4][9]
Special populations
Developmental delay / ID: use developmental-age thresholds; adapted toileting plans and longer timelines.[1] ASD: sensory toilet aversion, visual schedules, avoid forcing traumatic bathroom experiences.[10] ADHD: structured routines; medication optimisation can support adherence.[1] Out-of-home care: secondary incontinence common after placement stress; enforce non-punitive caregiving standards.[1] Cultural contexts: toilet-training norms vary; do not pathologise normative collective practices, but do not delay assessment after age thresholds when impairment exists.
Exam pearls
WET CLEAN plan
References
- [1]Fritz G, Rockney R, et al. Practice parameter for the assessment and treatment of children and adolescents with enuresis J Am Acad Child Adolesc Psychiatry, 2004.PMID 15564822
- [2]Neveus T, Eggert P, Evans J, et al. Evaluation of and treatment for monosymptomatic enuresis: a standardization document from the International Children's Continence Society J Urol, 2010.PMID 20006865
- [3]Neveus T, von Gontard A, Hoebeke P, et al. The standardization of terminology of lower urinary tract function in children and adolescents: report from the Standardisation Committee of the International Children's Continence Society J Urol, 2006.PMID 16753432
- [4]Nunes VD, O'Flynn N, Evans J, Sawyer L Management of bedwetting in children and young people: summary of NICE guidance BMJ, 2010.PMID 20980375
- [5]Caldwell PH, Codarini M, Stewart F, Hahn D, Sureshkumar P Alarm interventions for nocturnal enuresis in children Cochrane Database Syst Rev, 2020.PMID 32364251
- [6]Hahn D, et al. Desmopressin for nocturnal enuresis in children Cochrane Database Syst Rev, 2025.PMID 40728007
- [7]Caldwell PH, Sureshkumar P, Wong WC Tricyclic and related drugs for nocturnal enuresis in children Cochrane Database Syst Rev, 2016.PMID 26789925
- [8]Peng CC, Yang SS, Austin PF, Chang SJ Systematic Review and Meta-analysis of Alarm versus Desmopressin Therapy for Pediatric Monosymptomatic Enuresis Sci Rep, 2018.PMID 30425276
- [9]Tabbers MM, DiLorenzo C, Berger MY, et al. Evaluation and treatment of functional constipation in infants and children: evidence-based recommendations from ESPGHAN and NASPGHAN J Pediatr Gastroenterol Nutr, 2014.PMID 24345831
- [10]Brazzelli M, Griffiths PV, Cody JD, Tappin D Behavioural and cognitive interventions with or without other treatments for the management of faecal incontinence in children Cochrane Database Syst Rev, 2011.PMID 22161370
- [11]Loening-Baucke V Functional fecal retention with encopresis in childhood J Pediatr Gastroenterol Nutr, 2004.PMID 14676600
- [12]Pashankar DS, Bishop WP, Loening-Baucke V Long-term efficacy of polyethylene glycol 3350 for the treatment of chronic constipation in children with and without encopresis Clin Pediatr (Phila), 2003.PMID 14686553
- [13]Butler RJ Childhood nocturnal enuresis: developing a conceptual framework Clin Psychol Rev, 2004.PMID 15533278
- [14]Chin X, et al. Desmopressin therapy in children and adults: pharmacological considerations and clinical implications Eur J Clin Pharmacol, 2022.PMID 35199198