Psych · Child and adolescent psychiatry — neurodevelopmental
Language and communication disorders
Also known as Developmental language disorder · DLD · Specific language impairment · SLI · Speech sound disorder · Social pragmatic communication disorder · SPCD · Childhood-onset fluency disorder · Stuttering · Childhood apraxia of speech
Exam-exhaustive fellowship reference on language and communication disorders — DSM-5-TR/CATALISE classification, DLD vs SPCD vs ASD, epidemiology, SLT-first management including Lidcombe for stuttering, literacy and mental-health comorbidity. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Language and communication disorders are high-yield across FRANZCP CAP, MRCPsych, ABPN and MD/DNB because examiners test level-of-language mapping, the DLD vs SPCD vs ASD differential, population prevalence order-of-magnitude figures, and the trap of medicating “behaviour” without speech-language pathology (SLT). Psychiatrists coordinate formulation, comorbidity and risk; SLPs lead core intervention.[1][2][7][9]
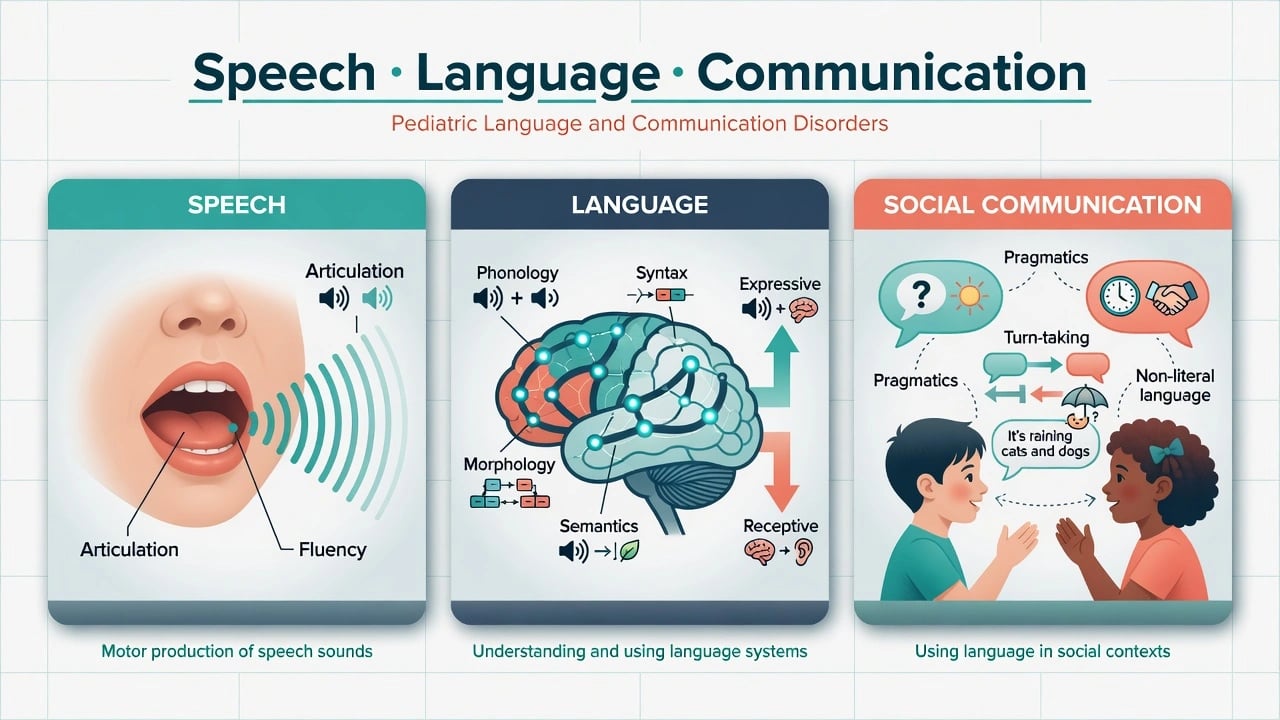
Overview and definition
Speech is the motor-acoustic production of sounds (articulation, phonology as surface errors, fluency, voice). Language is the symbolic system for understanding and producing meaning (receptive and expressive; domains: phonology, morphology, syntax, semantics). Communication includes verbal and non-verbal social use — pragmatics (turn-taking, topic maintenance, register, inference, non-literal language).[1][7]
A child may have fluent, well-articulated speech yet fail to understand classroom instructions (receptive language), or may have unintelligible speech with relatively better comprehension (speech sound disorder). Mixing these levels is an exam fail.[1][12]
Classification
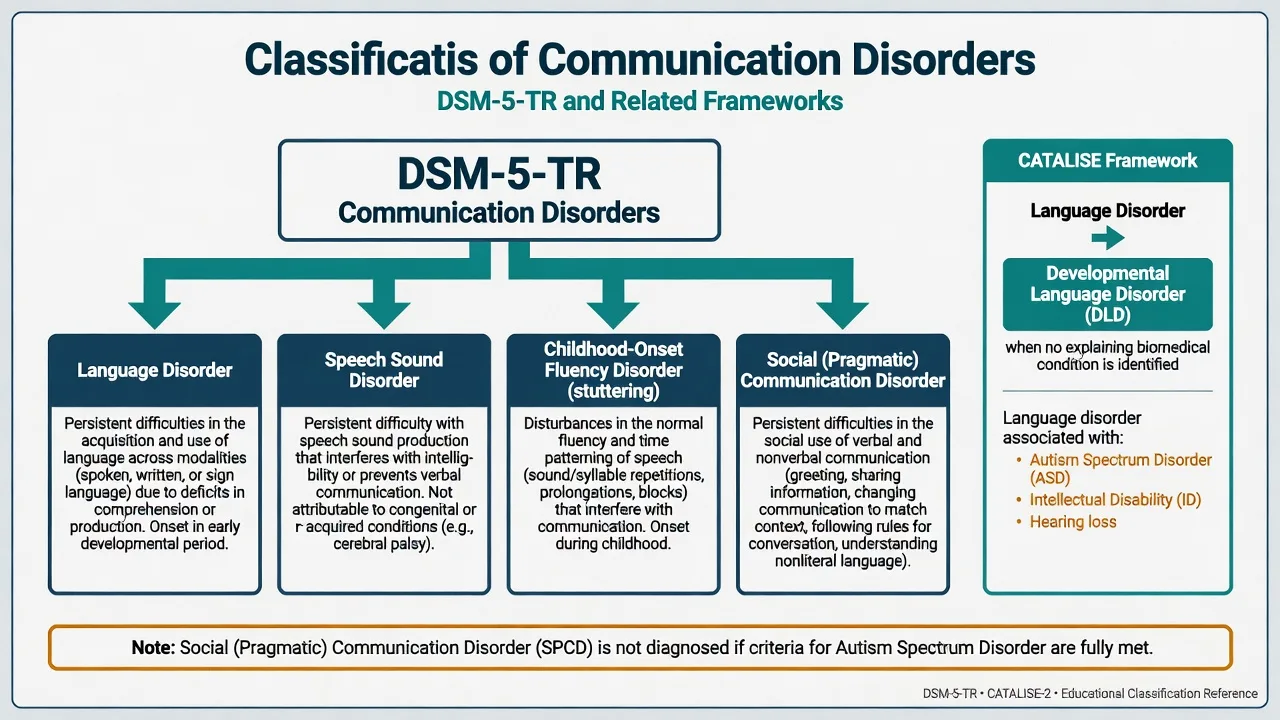
DSM-5-TR skeleton (must own)
| Diagnosis | Core rule of thumb |
|---|---|
| Language disorder | Persistent difficulties in acquisition and use of language across modalities (spoken, written, sign) due to deficits in comprehension or production; below age expectations; onset in early development; not better explained by hearing/sensory, motor, ID alone without disproportionate language profile as applied |
| Speech sound disorder | Persistent difficulty with speech sound production that interferes with intelligibility or communication; onset early; not attributable to congenital/acquired conditions alone without residual disorder concept |
| Childhood-onset fluency disorder (stuttering) | Disturbances in fluency and time patterning (repetitions, prolongations, blocks); anxiety about speaking may be present; onset in early developmental period |
| Social (pragmatic) communication disorder | Persistent deficits in social use of verbal and nonverbal communication; functional limits in communication/social participation/academics; not better explained by ASD, ID, or structural language disorder alone |
| Hierarchy note | If full ASD criteria are met, do not diagnose SPCD — ASD takes precedence for the social-communication domain |
| DSM-5-TR communication-disorder skeletons above are the examinable classification backbone used throughout this topic.[7][8] |
CATALISE: Language Disorder and DLD
The CATALISE Delphi consensus recommended clearer criteria for identifying language impairment and then standardised terminology.[1][2] Language Disorder refers to language difficulties that create obstacles to communication or learning in everyday life. Developmental language disorder (DLD) is used when the language disorder is not associated with a known differentiating biomedical condition (e.g. ASD, intellectual disability, genetic syndrome, sensorineural hearing loss, acquired brain injury). Historical specific language impairment (SLI) required relatively normal non-verbal IQ; CATALISE rejected rigid IQ-discrepancy gatekeeping as the sole entry criterion because pure “language-only” cases are uncommon and response to intervention is not cleanly stratified by NVIQ cut-offs.[1][2][3]
ICD-11 uses developmental language disorder and speech sound disorder concepts aligned with functional impairment — state which manual you are applying when thresholds are examined.[2]
Language disorder / DLD
- Form and content of language
- Receptive and/or expressive
- CATALISE DLD if no explaining biomedical condition
- SLT first-line
Speech sound disorder
- Articulation/phonology
- Intelligibility impact
- May co-occur with language delay
- Literacy risk
SPCD
- Pragmatics / social use
- Not full ASD (no RRB requirement met)
- Functional social-academic limits
- Careful ASD re-check
Stuttering
- Fluency and timing
- Preschool onset common
- Lidcombe evidence preschool
- Not 'just nerves'
Epidemiology and risk
Numbers candidates should own
Tomblin and colleagues’ kindergarten epidemiology remains the classic ~7% SLI prevalence estimate in monolingual English-speaking children using psychometrically defined criteria.[4] Norbury and colleagues’ SCALES population study found language disorder in about 7.6% of children at school entry when non-verbal ability was not used to exclude cases, underscoring that clinically important language disorder is common and not confined to children with average NVIQ.[3] Shriberg and colleagues estimated speech delay at about 3.8% in six-year-olds with comorbidity patterns relevant to literacy risk.[12] Zubrick and colleagues quantified late language emergence at 24 months and its predictors — LLE is common and many children catch up, but a clinically important subset persists.[10]
Risk context. Family history of speech, language or literacy difficulties, male sex, and socioeconomic disadvantage raise risk. Bilingual exposure does not cause DLD; disorder should be evident across languages when properly assessed.[1][10]
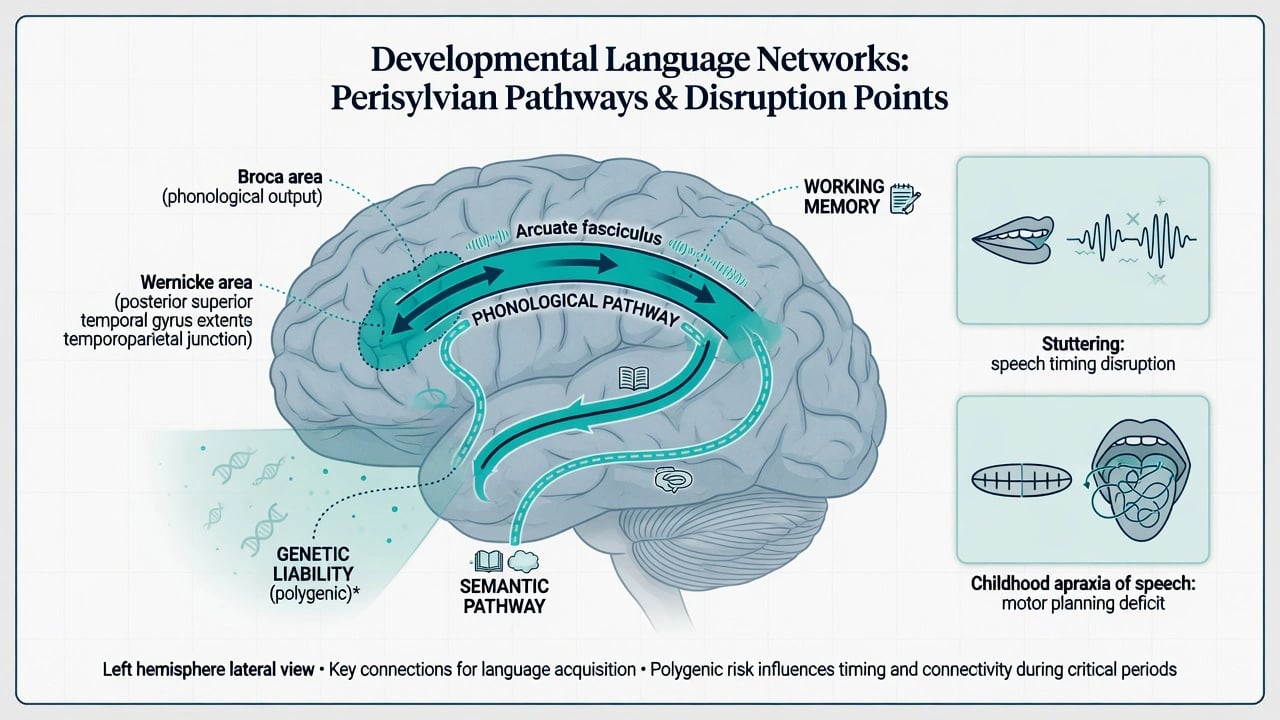
Pathophysiology
Teaching-level models emphasise disruption of distributed language networks (perisylvian cortex, dorsal phonological and ventral semantic pathways) and associated phonological working memory / procedural learning inefficiencies (classically illustrated by nonword-repetition deficits). Heritability is substantial and usually polygenic; rare variants (e.g. FOXP2-related speech-language disorder) illustrate severe genetic speech phenotypes but do not explain most DLD.[1][2] Stuttering involves multifactorial speech-motor timing and genetic liability — not pure psychogenesis. Childhood apraxia of speech reflects impaired planning and programming of speech movements and is an SLP diagnosis with intensive motor-learning-based therapy, not a psychiatric primary.[12] Imaging and genetics inform research and selected clinical pathways; they do not replace developmental history and standardised language assessment.[1]
Clinical presentation
Preschool. Delayed first words or word combinations, limited vocabulary, short utterances, poor response to name/instructions, unintelligible speech to unfamiliar listeners, frustration tantrums when not understood, reduced pretend play language.[1][10]
School age. Word-finding pauses, immature grammar, sparse narratives, failure on multi-step instructions, literacy failure, peer exclusion, “doesn’t listen” reports that may be receptive language rather than ADHD alone.[3][11]
SPCD. Difficulty using language for social purposes, matching communication to context, following conversation rules, understanding non-literal language and inference — with functional social and academic impact. Form of language may be relatively spared in pure pragmatic profiles, but mixed presentations are common.[7][8]
Stuttering. Sound/syllable repetitions, prolongations, blocks; secondary tension or avoidance; marked situational variability (often better reading alone than high-stakes speaking).[6]
MSE language. Sample spontaneous speech; check comprehension with multi-step commands; note repair strategies, gesture, frustration; screen mood, anxiety, ADHD features and autistic RRBs systematically.[7][9]
Differential diagnosis
Discriminators matter more than lists:
- Hearing impairment / OME — audiology is non-negotiable for persistent concerns.[1]
- Intellectual disability / GDD — language may be commensurate with overall development; still document profile and access needs.[1][2]
- ASD — presence of restricted/repetitive behaviours and broader social-reciprocity phenotype; SPCD is not coded when ASD criteria are met.[7][8]
- Selective mutism — anxiety-driven failure to speak in specific settings despite language competence elsewhere.
- ADHD — true comorbidity is common; also secondary inattention when instructions are not understood.[9]
- Acquired language loss / epileptic aphasia spectrum — regression and seizures are red flags, not DLD.[1]
- Bilingual difference — assess all languages with culturally appropriate tools and interpreters; disorder is not “English only” when the other language is solid.[1]
- Social deprivation — limited input can contribute to delay; do not dismiss persistent multi-domain impairment as “just environment.”
Assessment
Structure: level (speech/language/pragmatics) + onset + trajectory + hearing + home languages + family literacy + school function + comorbidity + risk.[1]
- Developmental language timeline (babble, first words, combinations, regression).
- Multi-informant history (parent, teacher) and work samples/video if needed.
- Direct language sample and comprehension checks in clinic.
- Refer to speech-language pathology for standardised assessment (conceptual tools: CELF, PLS, CCC-2 for pragmatic profile) — the psychiatrist owns indication and formulation, not tool administration.
- Systematic screen: ADHD, ASD, anxiety (including selective mutism), mood, ID, literacy, sleep, hearing.
- Safeguarding and bullying risk when communication failure drives isolation or aggression.
Investigations
Static developmental speech-language profiles do not need routine MRI or EEG. Obtain audiology for persistent concerns. Investigate when red flags appear: regression, seizures, progressive neurology, syndromic features warranting genetics, or acquired course.[1][2]
Acute safety
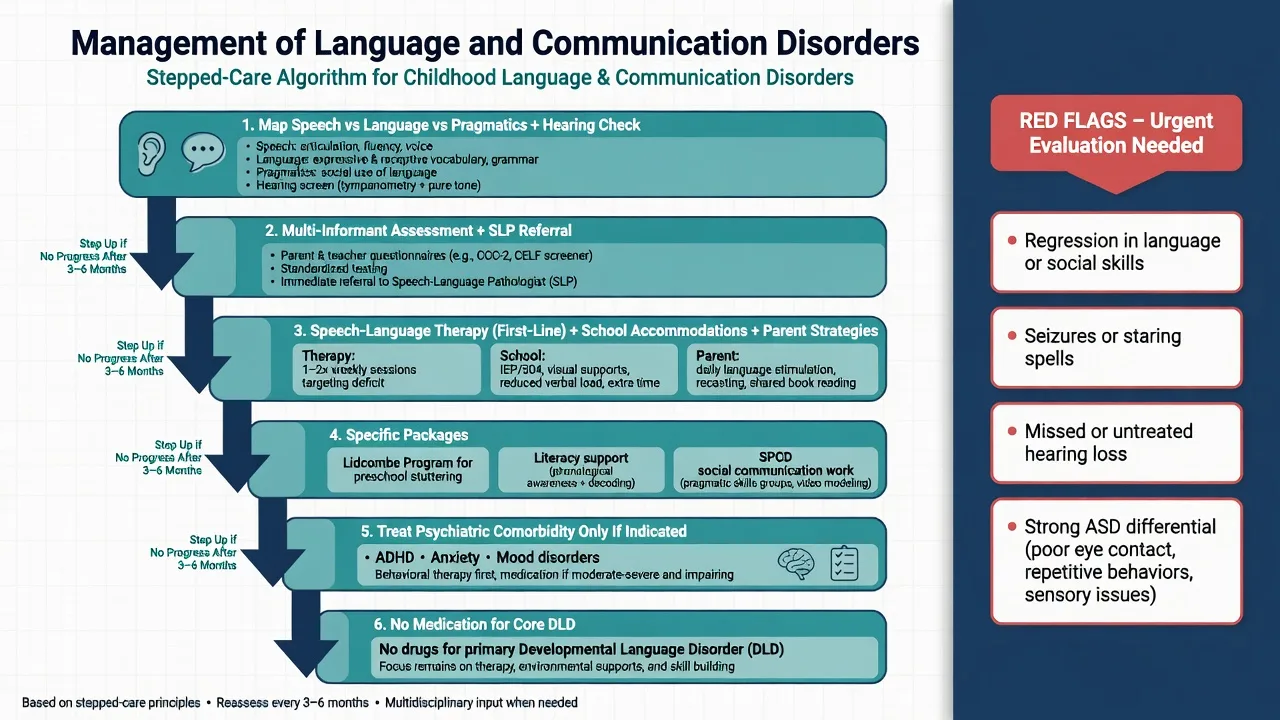
Definitive management
Speech-language therapy (first-line)
Evidence synthesised by Law and colleagues supports speech and language therapy for children with developmental speech and language delay/disorder, with clearer benefits for phonological and expressive vocabulary difficulties; receptive language outcomes are more mixed and may need longer, more intensive or context-embedded approaches.[5] Early identification and targeted SLT, parent-mediated language strategies, and classroom accommodations form the backbone of care. Psychiatry’s role is to secure referral, treat comorbidity that blocks therapy engagement, and advocate for educational supports.[1][5][11]
Late talkers
Many children with late language emergence catch up; monitor actively, enrich input, and escalate when delay is multi-domain, progressive relative to peers, or accompanied by comprehension deficits, family history of persistent DLD, or functional collapse.[10]
Stuttering — Lidcombe Programme
For preschool children who stutter, the Lidcombe Programme (parent-delivered contingencies under SLP supervision) demonstrated efficacy versus control in a randomised trial by Jones and colleagues — name this programme in exams.[6] School-age and adult stuttering care uses different packages (fluency shaping, stuttering modification, cognitive-behavioural components for social anxiety) delivered by SLP.
SPCD
Target social communication skills, pragmatic inference, and environmental scaffolding; involve school social skills programmes carefully (generalisation is hard). Revisit the ASD differential if RRBs emerge or history was incomplete. Do not promise “medication for SPCD.”[7][8]
Literacy cascade
Oral language underpins reading comprehension; children with DLD are at high risk of literacy failure and need integrated language–literacy intervention rather than phonics alone when oral language is weak.[11] Snowling and Hulme summarise intervention principles linking language and literacy pathways for exam-level teaching.[11]
Medication
No psychotropic medication treats core DLD, speech sound disorder, or SPCD. Use medicines only for comorbid ADHD, anxiety, depression or other indications, with the same monitoring standards as in those pathways, while ensuring language-accessible consent and psychoeducation.[5][9]
Regional practice notes
Australian and New Zealand CAP practice routes persistent speech-language concerns to paediatric speech pathology, audiology and school learning support, with psychiatry for comorbidity, risk and complex neurodevelopmental formulation. CATALISE DLD terminology is widely used in research and increasingly in clinical teaching alongside DSM-5-TR codes for documentation.[2][3]
Comorbidity focus: behaviour, ADHD and literacy
Meta-analyses by Yew and O’Kearney show that children with specific language impairments have elevated later internalising and externalising difficulties — examiners expect you to link communication failure to secondary behaviour and mental health risk, not only to “naughty” labelling.[9] ADHD and reading disorders commonly co-occur; treat each domain explicitly. Peer victimisation and reduced self-esteem are common and warrant school-based anti-bullying action.[9][11]
Prognosis and disposition
Many late talkers resolve; persistent DLD often continues to affect academic attainment, peer relations and later employment pathways. Early SLT, literacy support, treated comorbidity and family engagement improve functional outlook. Disposition: SLP care plan, school education adjustments (extra time, simplified instructions, visual supports), CAP follow-up for psychiatric comorbidity, and transition planning into adult services when residual impairment and mental health needs continue.[3][5][9][11]
Complications and pitfalls
- Calling the child oppositional when instructions are not understood.[9]
- Missing hearing loss.[1]
- Diagnosing SPCD without excluding ASD.[7][8]
- Blaming bilingualism.[1]
- Medicating core language disorder.[5]
- “Wait and see” forever for multi-domain persistent delay.[10]
- Ignoring literacy and mental-health cascade.[9][11]
Special populations
Bilingual/CALD. Assess all languages; use interpreters; avoid pathologising dialect. Indigenous families. Culturally safe assessment and school partnership. ASD/ID. Language disorder may be coded as associated with the biomedical/neurodevelopmental condition under CATALISE logic while still needing intensive communication support and AAC when indicated.[1][2] Deaf/hard of hearing. Prioritise language access (amplification, sign, bilingual approaches) — not a pure DLD pathway. Adolescents. Residual DLD presents as literacy failure, social isolation, anxiety, and sometimes justice-system vulnerability — reformulate “conduct” presentations with a language lens.[9]
Exam pearls
SPEAK CARE plan
References
- [1]Bishop DVM, Snowling MJ, Thompson PA, Greenhalgh T; CATALISE consortium CATALISE: A Multinational and Multidisciplinary Delphi Consensus Study. Identifying Language Impairments in Children PLoS One, 2016.PMID 27392128
- [2]Bishop DVM, Snowling MJ, Thompson PA, Greenhalgh T; CATALISE-2 consortium Phase 2 of CATALISE: a multinational and multidisciplinary Delphi consensus study of problems with language development: Terminology J Child Psychol Psychiatry, 2017.PMID 28369935
- [3]Norbury CF, Gooch D, Wray C, et al. The impact of nonverbal ability on prevalence and clinical presentation of language disorder: evidence from a population study J Child Psychol Psychiatry, 2016.PMID 27184709
- [4]Tomblin JB, Records NL, Buckwalter P, et al. Prevalence of specific language impairment in kindergarten children J Speech Lang Hear Res, 1997.PMID 9430746
- [5]Law J, Garrett Z, Nye C The efficacy of treatment for children with developmental speech and language delay/disorder: a meta-analysis J Speech Lang Hear Res, 2004.PMID 15324296
- [6]Jones M, Onslow M, Packman A, et al. Randomised controlled trial of the Lidcombe programme of early stuttering intervention BMJ, 2005.PMID 16096286
- [7]Norbury CF Practitioner review: Social (pragmatic) communication disorder conceptualization, evidence and clinical implications J Child Psychol Psychiatry, 2014.PMID 24117874
- [8]Swineford LB, Thurm A, Baird G, Wetherby AM, Swedo S Social (pragmatic) communication disorder: a research review of this new DSM-5 diagnostic category J Neurodev Disord, 2014.PMID 25484991
- [9]Yew SG, O'Kearney R Emotional and behavioural outcomes later in childhood and adolescence for children with specific language impairments: meta-analyses of controlled prospective studies J Child Psychol Psychiatry, 2013.PMID 23082773
- [10]Zubrick SR, Taylor CL, Rice ML, Slegers DW Late language emergence at 24 months: an epidemiological study of prevalence, predictors, and covariates J Speech Lang Hear Res, 2007.PMID 18055773
- [11]Snowling MJ, Hulme C Interventions for children's language and literacy difficulties Int J Lang Commun Disord, 2012.PMID 22268899
- [12]Shriberg LD, Tomblin JB, McSweeny JL Prevalence of speech delay in 6-year-old children and comorbidity with language impairment J Speech Lang Hear Res, 1999.PMID 10599627