Psych · Child and adolescent psychiatry — psychopharmacology
Paediatric psychopharmacology
Also known as Pediatric psychopharmacology · Child and adolescent psychotropic medication · Youth psychopharmacology · CAP prescribing · SSRI black-box children · ADHD medication children · Antipsychotic metabolic monitoring youth · Gillick competence medication
Exam-exhaustive fellowship reference on paediatric psychopharmacology — developmental PK/PD, when to medicate, SSRI black-box communication and youth dosing, ADHD stimulants and non-stimulants with growth/CV monitoring, antipsychotic metabolic risk (Correll, TEOSS), ASD irritability (RUPP), consent/capacity with parents (Gillick), emergency adverse effects, and landmark CAP trials (TADS, CAMS, MTA, Cipriani, Cortese). Distinct from adult drug monographs and single-disorder hubs. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Psychotropic prescribing in under-18s is a high-yield cross-class viva for FRANZCP CAP and generalist interfaces, MRCPsych CASC, ABPN, and MD/DNB. Examiners test developmental PK/PD, black-box communication, agent-level doses, metabolic and growth monitoring, Gillick/parental consent, and landmark trial names — not adult-only algorithms pasted onto children.[14][15][20]
This topic is the CAP prescribing spine. Single-disorder hubs (youth depression, ADHD across the lifespan, early-onset psychosis, ASD) supply syndrome depth; adult monographs supply receptor tables. Here the centre of gravity is how to prescribe safely across classes in youth.[9][12][20]
Definition and classification
Paediatric psychopharmacology is the evidence-based use of medicines for mental disorders in children and adolescents, integrating developmental pharmacokinetics and pharmacodynamics, multi-informant outcome measurement, family systems, school function, and consent law. Medication is a tool within a formulation, not a substitute for diagnosis, psychological care, or environmental change.[14][15][20]
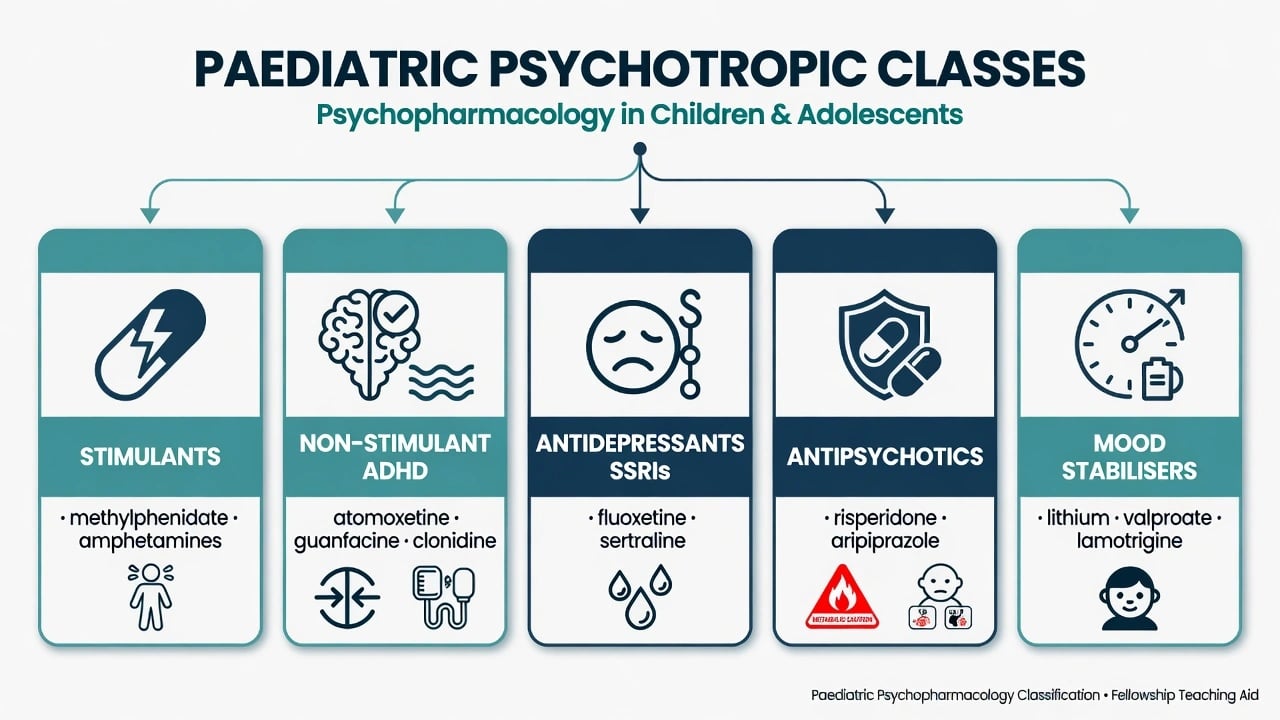
| Class | Core CAP uses | Exam frame |
|---|---|---|
| Stimulants (methylphenidate, amphetamines, lisdexamfetamine) | Impairing ADHD | First-line after multi-setting diagnosis; growth, BP/HR, diversion |
| Non-stimulant ADHD (atomoxetine, guanfacine XR, clonidine XR) | ADHD when stimulants fail/not tolerated/high diversion risk; sometimes tics/comorbidity | Slower onset; alpha-2 taper rules |
| SSRIs (fluoxetine, sertraline, others) | Depression, anxiety, OCD pathways | Black-box monitoring; fluoxetine best-evidenced in youth MDD |
| Antipsychotics (risperidone, aripiprazole, others) | Early psychosis, mania, severe irritability/aggression (selected) | Metabolic risk high in SGA-naive youth |
| Mood stabilisers | Adolescent bipolar and related | Specialist monitoring; pointer to dedicated topics |
| Short-term benzodiazepines / hypnotics | Acute anxiety/agitation adjuncts | Avoid long-term anxiolytic culture in CAP |
On-label vs off-label. Many youth prescriptions are off-label by age or indication depending on jurisdiction. Examiners expect documented indication, alternatives considered, consent discussion, and monitoring — not a claim that off-label equals forbidden or that on-label equals risk-free.[14][15]
Epidemiology and risk context
Psychotropic use in youth has increased in many health systems, producing dual exam traps: undertreatment of moderate–severe illness (especially depression with black-box fear) and overtreatment (especially antipsychotics for behavioural dysregulation without behavioural formulation).[1][12][21]
Risk headlines examiners expect
Pathophysiology and developmental pharmacology
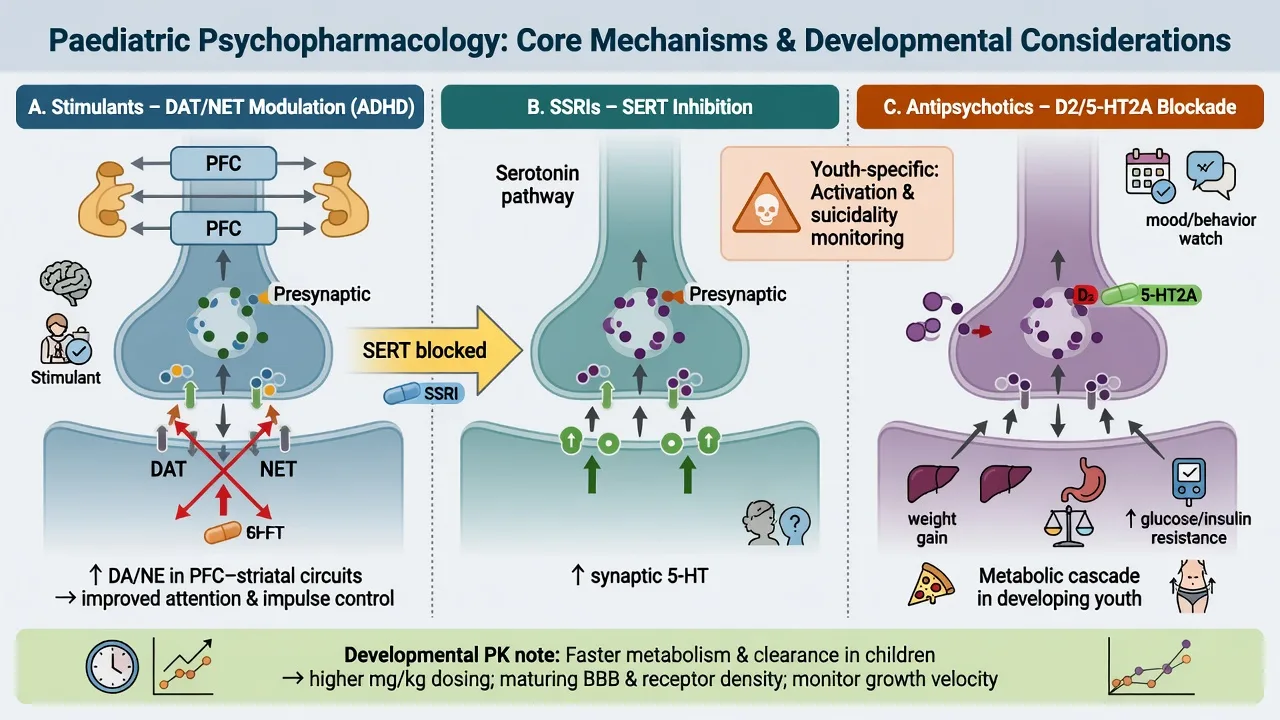
- Stimulants increase extracellular dopamine and noradrenaline via DAT/NET effects; therapeutic oral ADHD doses differ from recreational kinetics — still counsel misuse risk in adolescents.[9][15]
- Atomoxetine is a selective NET inhibitor with slower clinical onset than stimulants; useful when diversion risk is high or stimulants poorly tolerated.[16][23]
- SSRIs inhibit SERT; youth trials show high placebo response and a small suicidality signal requiring early monitoring rather than nihilism.[1][4]
- Antipsychotics act primarily via D2 (± 5-HT2A) antagonism; histaminergic and other receptor profiles drive sedation and metabolic risk — first exposure in youth can produce substantial weight gain within weeks.[11][12]
- Developmental PK: children may clear some agents faster; start low, titrate to effect, avoid adult loading habits. Puberty, body composition, and adherence culture change exposure over time.[14][15]
Clinical presentation targets and adverse phenotypes
Prescribe to named target symptoms and functional goals (school attendance, aggression frequency, CGI, ADHD rating scales, PHQ-A), not vague "settling". Carers and teachers often detect school-day coverage gaps or evening rebound; the young person may prioritise side-effects (appetite, sexual function, dulling, weight).[15][18][21]
Adverse phenotypes to name in viva: SSRI activation/akathisia/insomnia; stimulant anorexia, insomnia, tics fluctuation, mood lability; alpha-2 sedation and hypotension; SGA weight gain, dyslipidaemia, glucose dysregulation, prolactin effects (especially risperidone); EPS/dystonia; rare NMS or serotonin toxicity with polypharmacy.[1][12][18][19]
Differential when medication "fails"
| Apparent non-response | Discriminators | Next step logic |
|---|---|---|
| Wrong diagnosis | Bipolar spectrum, trauma, ASD, substance, organic | Reformulate before stacking drugs |
| Inadequate trial | Subtherapeutic dose, less than 4–6 weeks at target, non-adherence | Optimise single agent |
| Diversion / partial dosing | Missing pills, weekend-only use, peer supply | Supervised long-acting; non-stimulant |
| Activation vs bipolar switch | Elevated mood, decreased sleep need, grandiosity | Stop/hold antidepressant path; specialist mood review |
| Stimulant psychosis/mood | Timeline with dose escalations | Stop stimulant; medicalise; reassess |
| Environmental maintainers | Family conflict, bullying, sleep debt | Psychosocial intensity, not only polypharmacy |
Assessment before the first dose
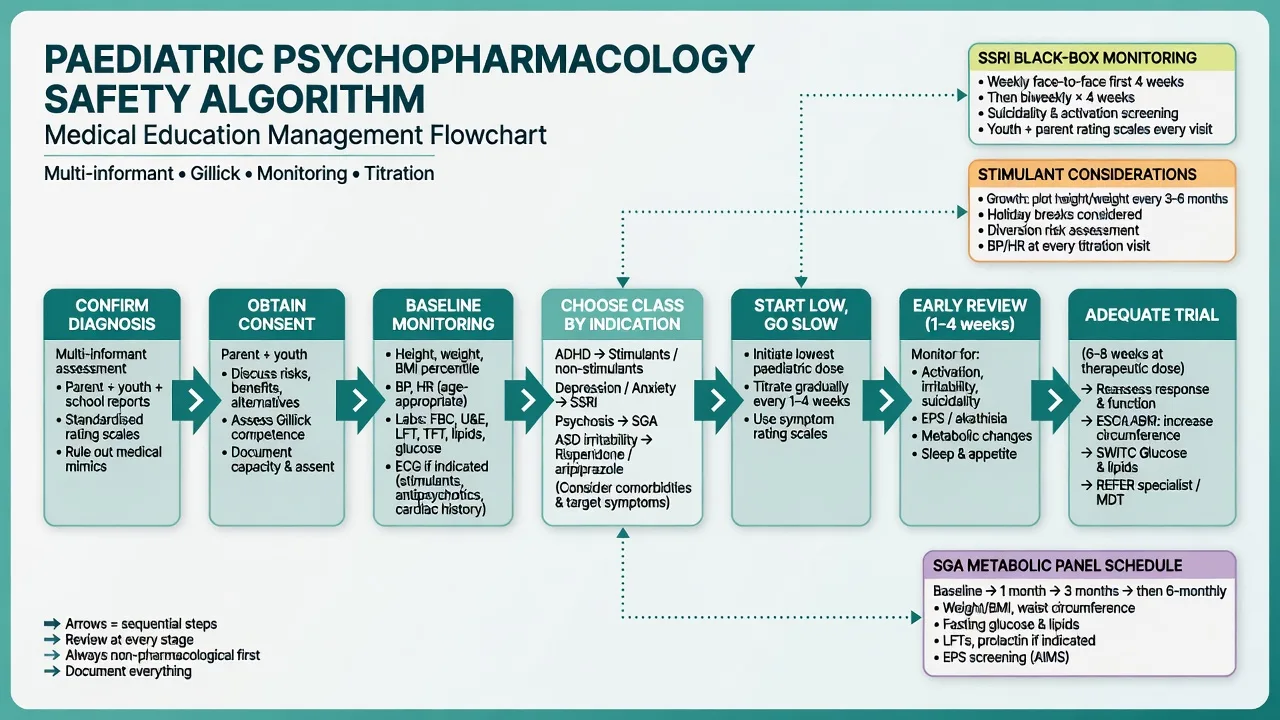
Checklist. Diagnostic confidence with multi-informant data; impairment severity; prior/concurrent psychological care; suicide/self-harm and violence risk; bipolar screen before antidepressants; substance use; cardiac and seizure history; family mental illness and medication attitudes; pregnancy risk in adolescents; safeguarding context.[14][15][21]
Consent and capacity (parents and youth). Assess Gillick/developmental competence: understanding of condition, proposed medicine, benefits, harms, alternatives, and ability to weigh and communicate a choice voluntarily. Involve parents/carers as default in CAP; mature minors may consent in some jurisdictions, but safety and family engagement still shape practice. Explain confidentiality limits before private youth interviews. When carers disagree or a young person refuses, use least-restrictive pathways and jurisdiction-specific mental health law principles — do not invent statute section numbers in exams.[14][20][21]
Document before prescribing: target symptoms, agent/dose/route, early review plan, emergency contacts, means restriction if overdose risk, and what would count as failure or harm.[14][15][21]
Investigations and baseline monitoring
No lab diagnoses ADHD or depression. Pre-treatment minimums follow practice-parameter style safety baselines rather than diagnostic testing.[14][15]
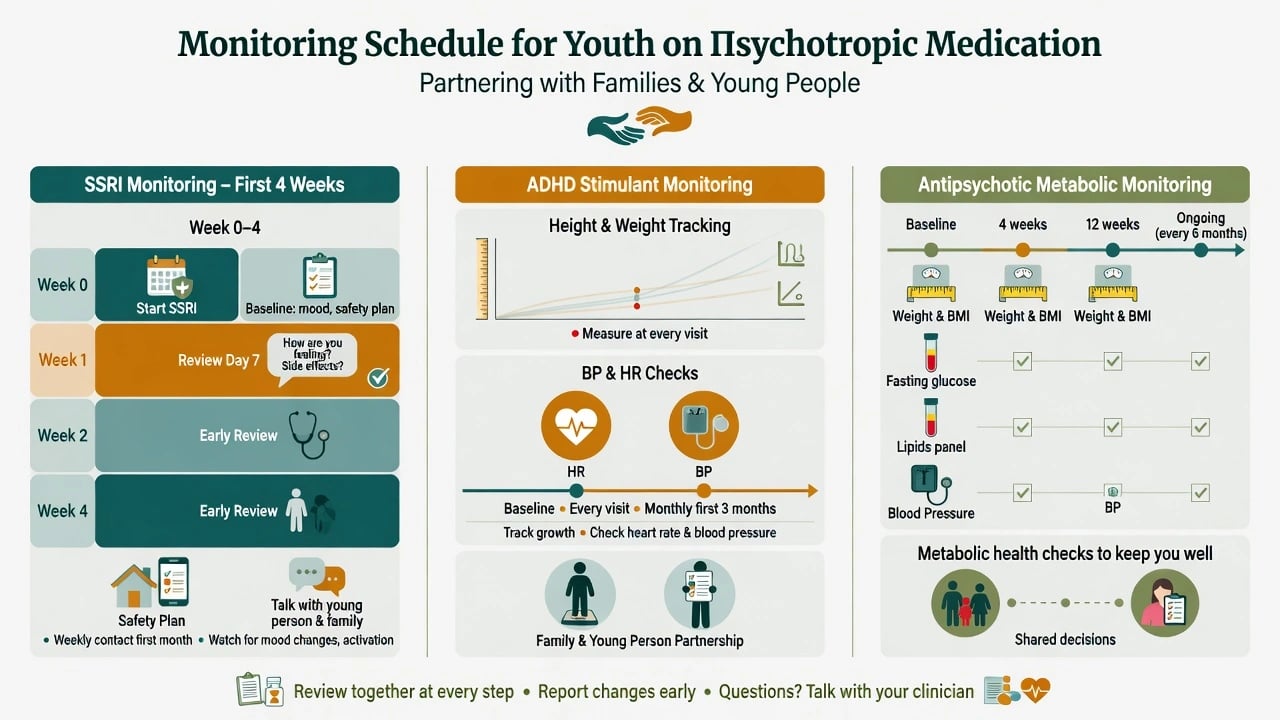
- All classes: height, weight, BMI centile trajectory, BP, HR; pregnancy test when relevant; targeted history.[15][18]
- Stimulants/atomoxetine: cardiac history (syncope, family sudden death, structural heart disease). ECG when history/symptoms warrant — not every guideline mandates universal ECG for every healthy child, but know when to obtain.[10][15][22]
- Antipsychotics: fasting glucose or HbA1c, lipids, BP, weight; prolactin if symptoms; ECG if QTc risk factors or polypharmacy.[12]
- Mood stabilisers: agent-specific panels (e.g. lithium U&E/thyroid; valproate LFTs/FBC and teratogenicity counselling) — specialist detail in dedicated topics.[20]
Acute and emergency management
- Acute dystonia: anticholinergic treatment pathway and dose review.[18]
- NMS: stop antipsychotic, emergency medical care, supportive treatment.[11][18]
- Serotonin toxicity: stop serotonergic agents, emergency care.[1][14]
- Stimulant cardiac symptoms: hold agent, medical review.[10][18]
- Suspected SGA-related hyperglycaemic crisis: emergency medical pathway.[12]
Definitive management — class-by-class
General rules
- Prefer psychosocial interventions first or in parallel according to severity and guideline pathways.[14][15][21]
- One medication change at a time when possible.[14][15]
- Adequate dose and duration before declaring failure.[2][15]
- Measurement-based care (scales + school/family function).[14][21]
- Plan duration and exit strategy at initiation.[14][15]
SSRIs and the black-box
FDA paediatric meta-analysis (Hammad et al.) found a small absolute increase in suicidal ideation/behaviour signals with antidepressants versus placebo in short trials, without establishing a large completed-suicide signal in those datasets. Communicate absolute and relative risk honestly; the clinical implication is closer early monitoring and safety planning, not reflexive refusal to treat moderate–severe depression.[1][14][21]
Youth depression — first-line pharmacotherapy. When medication is indicated, fluoxetine is the best-evidenced SSRI. Example initiating regimen (individualise): fluoxetine 10 mg orally once daily for several days to about 1 week if smaller, younger, or activation-prone, then 20 mg orally daily; selected adolescents may titrate toward 40 mg daily under specialist review if partial response and good tolerability. Review early (often within the first week in higher-risk youth, then frequently through month one) for activation, insomnia, agitation, akathisia, and suicidal thinking. Plan an adequate trial (commonly 4–6 weeks at a therapeutic dose with adherence) before switching.[2][5][4][21]
Landmark sequencing. TADS supports fluoxetine and combination treatment acutely for adolescent depression; ADAPT cautions that adding a CBT package to SSRI plus high-quality specialist care is not always superior at primary endpoint; TORDIA supports switch antidepressant + CBT after SSRI resistance rather than endless same-drug inertia; Cipriani network meta-analysis favours fluoxetine among many agents for youth MDD efficacy/tolerability balance.[2][3][4][6]
Anxiety. CAMS showed combination CBT + sertraline superior acute response rates to either monotherapy, with both active arms beating placebo — use for moderate–severe childhood anxiety when medication is considered, not as a replacement for therapy access when therapy alone is appropriate.[7]
Example anxiety start (individualise, specialist context): sertraline often initiated around 25 mg orally daily then titrated (common paediatric trial ranges extend toward 50–200 mg daily depending on age/response/tolerability) with the same early activation/suicidality monitoring as other SSRIs.[7][1]
ADHD medications
After multi-setting ADHD diagnosis and psychoeducation, stimulants are first-line for impairing symptoms in most guidelines and network evidence; MTA established intensive medication management superiority for core ADHD symptoms versus community care at 14 months, with later follow-up nuance about long-term advantages.[8][9][15]
Example stimulant starts (individualise; use local formulary formulations) follow AACAP/European adverse-effect guidance culture: start low, titrate to function, prefer long-acting coverage when diversion or school-day adherence is a concern.[15][18][9]
- Methylphenidate immediate-release often starts around 5 mg orally two or three times daily with titration by effect and side-effects; long-acting formulations preferred for school coverage and diversion reduction once dose established — total daily doses commonly titrated in the 0.3–1.0 mg/kg/day teaching range depending on product and response, staying within product maxima.[15][18]
- Lisdexamfetamine example paediatric starts often 20–30 mg orally once daily in the morning, titrated weekly by response/tolerability within licensed maxima for age/product.[24][9]
Monitoring: height/weight trajectory, appetite, sleep, BP/HR, mood, tics, misuse/diversion. Serious cardiovascular events are uncommon in large cohorts, but history screening and symptom vigilance remain mandatory.[10][18][19][22]
Non-stimulants. Atomoxetine example: approximately 0.5 mg/kg/day orally for at least 3 days then target around 1.2 mg/kg/day (typical max teaching near 1.4 mg/kg/day or product cap), once daily or split; slower onset (weeks); counsel hepatic and suicidality warnings per local labelling; useful when diversion risk high or stimulants fail/not tolerated.[16][23][18]
Guanfacine XR and clonidine XR: alpha-2 agonists for ADHD (± combination contexts); start low (product-specific paediatric schedules, e.g. guanfacine XR often 1 mg orally daily titrated weekly) with BP/HR monitoring; taper to stop — do not abrupt-cease after prolonged use (rebound hypertension risk).[17][25][18]
Antipsychotics and metabolic risk
First-time SGA use in children and adolescents is associated with clinically important weight gain and metabolic change within weeks (Correll et al.) — baseline and longitudinal weight, BMI, glucose, and lipids are not optional paperwork.[12]
TEOSS compared molindone, olanzapine, and risperidone in early-onset schizophrenia spectrum disorders: comparable efficacy framing with olanzapine showing greater weight gain — examiners expect you not to pick olanzapine as casual first-line in youth solely for convenience.[11]
ASD irritability. RUPP (McCracken et al.) showed risperidone reduced severe tantrums, aggression, and self-injury versus placebo in autistic children — this treats target irritability/aggression, not core social-communication deficits. Behavioural interventions remain foundational; use lowest effective dose and metabolic monitoring.[13]
Example youth antipsychotic starts (individualise, specialist): risperidone often 0.25–0.5 mg orally daily initially in smaller children, titrated cautiously (many ASD/aggression protocols cluster toward low total daily doses with functional targets); aripiprazole often starts 2 mg orally daily with slow titration. Prefer monotherapy; reassess need frequently; avoid "forever PRN stacking".[11][12][13]
Mood stabilisers (pointer)
Adolescent bipolar pharmacotherapy (lithium, valproate with teratogenicity counselling, selected antipsychotics) requires specialist protocols, serum levels where relevant, and contraception counselling — use dedicated bipolar/mood-stabiliser topics for full dose tables; here the exam pearl is do not treat bipolar depression as uncomplicated unipolar SSRI monotherapy.[20]
Landmark evidence table
| Landmark | Takeaway for CAP prescribing |
|---|---|
| Hammad 2006 | Small absolute suicidality signal on paediatric antidepressants — monitor early |
| TADS 2004 | Fluoxetine and combination therapy strong acute signals in adolescent MDD |
| ADAPT 2007 | CBT add-on not always superior to SSRI + specialist care at primary endpoint |
| TORDIA 2008 | After SSRI failure: switch + CBT beats switch alone |
| Cipriani 2016 NMA | Fluoxetine most consistent among youth antidepressants studied |
| CAMS 2008 | CBT + sertraline best acute childhood anxiety response rates |
| MTA 1999 | Carefully managed medication powerful for core ADHD symptoms |
| Cortese 2018 NMA | Stimulants highly efficacious; tolerability trade-offs by age group |
| Cooper 2011 | Serious CV events uncommon; still screen and monitor |
| TEOSS 2008 | Youth antipsychotic comparative efficacy; olanzapine weight liability |
| Correll 2009 | Rapid cardiometabolic risk with first SGA exposure in youth |
| RUPP 2002 | Risperidone for severe ASD irritability/aggression targets |
SSRI youth
- Fluoxetine first in MDD
- Black-box = early review
- TADS/TORDIA literacy
- Combine with therapy when feasible
ADHD meds
- Stimulant-first impairing ADHD
- Plot growth + BP/HR
- Atomoxetine if diversion risk
- Alpha-2 taper rules
SGA youth
- Metabolic from day one
- Lowest effective dose
- TEOSS weight lesson
- RUPP target irritability not autism core
Consent CAP
- Gillick assessment
- Parents usually essential
- Safety limits confidentiality
- No invented statute numbers
Subtypes and scenarios
- First SSRI in adolescent MDD with parental black-box fear: absolute-risk language, monitoring calendar, means restriction, therapy plan.[1][2][21]
- School-age ADHD start: multi-setting confirmation, long-acting preference, school liaison, growth plot.[8][15]
- Adolescent first SGA for psychosis: metabolic contract, family education, early weight action plan.[11][12]
- ASD severe irritability: behavioural first-line emphasis; risperidone/aripiprazole only for severe target behaviours with monitoring.[13]
- Complex polypharmacy review: strip to formulation; one change at a time; check interactions and QTc when combining.[14][20]
- Transition-age youth: adherence, diversion, handover to adult services with clear regimen summary.[15]
Complications and pitfalls
Other traps: antipsychotics for generic "behaviour" without formulation; missing metabolic labs; declaring stimulant failure without school data or adequate dose; promising absolute confidentiality; abrupt alpha-2 cessation; polypharmacy before reformulation.[12][15][18]
Prognosis and disposition
Success is functional recovery (school, family, peer, sleep) plus symptom change. Share care with GP/paediatrics for growth and metabolic follow-up. Step up to specialist CAMHS/inpatient when risk, non-response, or adverse effects exceed community containment. Plan medication holidays or deprescribing trials only when stable and supervised.[14][15][21]
Special populations
Pre-pubertal children: thinner evidence for many agents — specialist oversight and psychosocial intensity first. Intellectual disability/ASD: high polypharmacy risk; behavioural formulation first for many targets. Substance-using adolescents: diversion-aware stimulant choices. Looked-after children: clarify consent authorities. Indigenous and culturally diverse families: cultural safety in explanatory models and decision styles (FRANZCP expectation). Pregnant adolescents: dual risk–benefit under perinatal frameworks.[13][14][20]
Regional guideline deltas
ANZ (RANZCP): formulation-centred mood and youth care principles within mood disorder guidance; local prescribing formularies and Mental Health Act processes are state/territory specific — name principles, not invented sections.[20]
UK: NICE-style stepped care for depression/ADHD/psychosis in young people; ADAPT familiarity; CAMHS service design varies by era.[6]
US: AACAP practice parameters, FDA black-box labelling for antidepressants, GLAD-PC primary-care pathways for adolescent depression.[14][15][21]
Exam pearls
[1] [2] [4] [5] [12] [14] [20]Mnemonic for first prescription skeleton: START-SAFE — Syndrome confirmed multi-informant, Targets written, Adverse-effect plan, Risk/suicide screen, Titrate one drug, Schedule early review, Access means restriction, Family consent/Gillick, Exit/duration plan.[1][14][15]
Summary
Defend paediatric psychopharmacology as developmental, multi-system prescribing: solid diagnosis, parent-and-youth consent, class-specific evidence (TADS/CAMS/MTA/TEOSS/RUPP/Correll/Cipriani/Cortese), black-box-aware SSRI starts, stimulant-first ADHD with growth vigilance, and metabolic-first antipsychotic culture — always one thoughtful change at a time, measured against school and family function rather than pill counts alone.[1][2][7][8][9][11][12][13]
References
- [1]Hammad TA, Laughren T, Racoosin J Suicidality in pediatric patients treated with antidepressant drugs Arch Gen Psychiatry, 2006.PMID 16520440
- [2]March J, Silva S, Petrycki S, et al. Fluoxetine, cognitive-behavioral therapy, and their combination for adolescents with depression: Treatment for Adolescents With Depression Study (TADS) randomized controlled trial JAMA, 2004.PMID 15315995
- [3]Brent D, Emslie G, Clarke G, et al. Switching to another SSRI or to venlafaxine with or without cognitive behavioral therapy for adolescents with SSRI-resistant depression: the TORDIA randomized controlled trial JAMA, 2008.PMID 18314433
- [4]Cipriani A, Zhou X, Del Giovane C, et al. Comparative efficacy and tolerability of antidepressants for major depressive disorder in children and adolescents: a network meta-analysis Lancet, 2016.PMID 27289172
- [5]Emslie GJ, Heiligenstein JH, Wagner KD, et al. Fluoxetine for acute treatment of depression in children and adolescents: a placebo-controlled, randomized clinical trial J Am Acad Child Adolesc Psychiatry, 2002.PMID 12364842
- [6]Goodyer I, Dubicka B, Wilkinson P, et al. Selective serotonin reuptake inhibitors (SSRIs) and routine specialist care with and without cognitive behaviour therapy in adolescents with major depression: randomised controlled trial BMJ, 2007.PMID 17556431
- [7]Walkup JT, Albano AM, Piacentini J, et al. Cognitive behavioral therapy, sertraline, or a combination in childhood anxiety N Engl J Med, 2008.PMID 18974308
- [8]The MTA Cooperative Group A 14-month randomized clinical trial of treatment strategies for attention-deficit/hyperactivity disorder. The MTA Cooperative Group. Multimodal Treatment Study of Children with ADHD Arch Gen Psychiatry, 1999.PMID 10591283
- [9]Cortese S, Adamo N, Del Giovane C, et al. Comparative efficacy and tolerability of medications for attention-deficit hyperactivity disorder in children, adolescents, and adults: a systematic review and network meta-analysis Lancet Psychiatry, 2018.PMID 30097390
- [10]Cooper WO, Habel LA, Sox CM, et al. ADHD drugs and serious cardiovascular events in children and young adults N Engl J Med, 2011.PMID 22043968
- [11]Sikich L, Frazier JA, McClellan J, et al. Double-blind comparison of first- and second-generation antipsychotics in early-onset schizophrenia and schizo-affective disorder: findings from the treatment of early-onset schizophrenia spectrum disorders (TEOSS) study Am J Psychiatry, 2008.PMID 18794207
- [12]Correll CU, Manu P, Olshanskiy V, et al. Cardiometabolic risk of second-generation antipsychotic medications during first-time use in children and adolescents JAMA, 2009.PMID 19861668
- [13]McCracken JT, McGough J, Shah B, et al. Risperidone in children with autism and serious behavioral problems N Engl J Med, 2002.PMID 12151468
- [14]Birmaher B, Brent D, AACAP Work Group on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with depressive disorders J Am Acad Child Adolesc Psychiatry, 2007.PMID 18049300
- [15]Pliszka S; AACAP Work Group on Quality Issues Practice parameter for the assessment and treatment of children and adolescents with attention-deficit/hyperactivity disorder J Am Acad Child Adolesc Psychiatry, 2007.PMID 17581453
- [16]Michelson D, Allen AJ, Busner J, et al. Once-daily atomoxetine treatment for children and adolescents with attention deficit hyperactivity disorder: a randomized, placebo-controlled study Am J Psychiatry, 2002.PMID 12411225
- [17]Sallee FR, McGough J, Wigal T, et al. Guanfacine extended release in children and adolescents with attention-deficit/hyperactivity disorder: a placebo-controlled trial J Am Acad Child Adolesc Psychiatry, 2009.PMID 19106767
- [18]Graham J, Banaschewski T, Buitelaar J, et al. European guidelines on managing adverse effects of medication for ADHD Eur Child Adolesc Psychiatry, 2011.PMID 21042924
- [19]Cortese S, Holtmann M, Banaschewski T, et al. Practitioner review: current best practice in the management of adverse events during treatment with ADHD medications in children and adolescents J Child Psychol Psychiatry, 2013.PMID 23294014
- [20]Malhi GS, Bell E, Bassett D, et al. The 2020 Royal Australian and New Zealand College of Psychiatrists clinical practice guidelines for mood disorders Aust N Z J Psychiatry, 2021.PMID 33353391
- [21]Cheung AH, Zuckerbrot RA, Jensen PS, et al. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): Part II. Treatment and Ongoing Management Pediatrics, 2018.PMID 29483201
- [22]Hennissen L, Bakker MJ, Banaschewski T, et al. Cardiovascular Effects of Stimulant and Non-Stimulant Medication for Children and Adolescents with ADHD: A Systematic Review and Meta-Analysis of Trials of Methylphenidate, Amphetamines and Atomoxetine CNS Drugs, 2017.PMID 28236285
- [23]Newcorn JH, Kratochvil CJ, Allen AJ, et al. Atomoxetine and osmotically released methylphenidate for the treatment of attention deficit hyperactivity disorder: acute comparison and differential response Am J Psychiatry, 2008.PMID 18281409
- [24]Biederman J, Boellner SW, Childress A, et al. Lisdexamfetamine dimesylate and mixed amphetamine salts extended-release in children with ADHD: a double-blind, placebo-controlled study Biol Psychiatry, 2007.PMID 17631866
- [25]Jain R, Segal S, Kollins SH, et al. Clonidine extended-release tablets for pediatric patients with attention-deficit/hyperactivity disorder J Am Acad Child Adolesc Psychiatry, 2011.PMID 21241954