Psych · Child and adolescent psychiatry — specific learning disorder
Specific learning disorder
Also known as Specific learning disorder · Specific learning disability · Dyslexia · Dyscalculia · Dysgraphia · Reading disability · Disorder of written expression · Mathematics learning disability · Developmental learning disorder
Exam-exhaustive fellowship reference on specific learning disorder — DSM-5-TR domains (reading, written expression, mathematics), dyslexia science, instructional-response identification, comorbidity with ADHD, and multiagency educational management. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Specific learning disorder is high-yield across FRANZCP CAP, MRCPsych, ABPN and MD/DNB because examiners test whether you can name domains and severity, separate SLD from ID/ADHD/language disorder/poor teaching, use instructional-response thinking, and build a plan centred on evidence-based academic intervention plus accommodations and comorbidity care. This topic is written so a candidate who has read nothing else can defend those points at consultant depth.[1][6][7]
Overview and definition
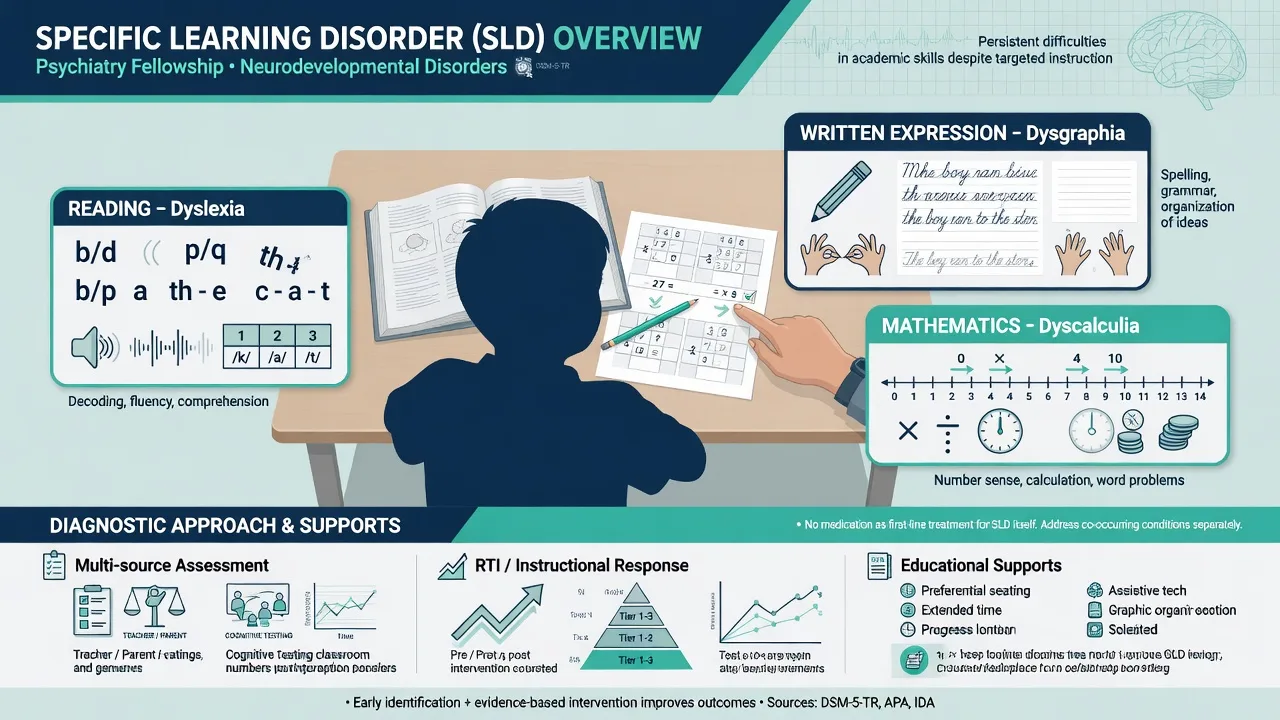
Specific learning disorder describes persistent difficulties learning and using academic skills. Skills must be substantially and quantifiably below those expected for chronological age, cause functional interference (school, work, daily activities), begin during school-age years (though full recognition may be delayed until demands exceed compensation), and persist despite targeted intervention. Exclusion gates matter: not better accounted for by intellectual disability, uncorrected visual or auditory acuity problems, other mental or neurological disorders, psychosocial adversity, lack of proficiency in the language of academic instruction, or inadequate educational instruction.[1][6][15]
Formulation first. Test scores open and close diagnostic gates; formulation explains developmental language history, instructional opportunity, family academic history, attention/executive function, mood/anxiety secondary effects, cultural-linguistic context, and what to do next. CAP language and learning parameters emphasise multi-source developmental and educational assessment rather than a single clinic snapshot.[1]
Classification framework
Three academic domains (exam skeleton)
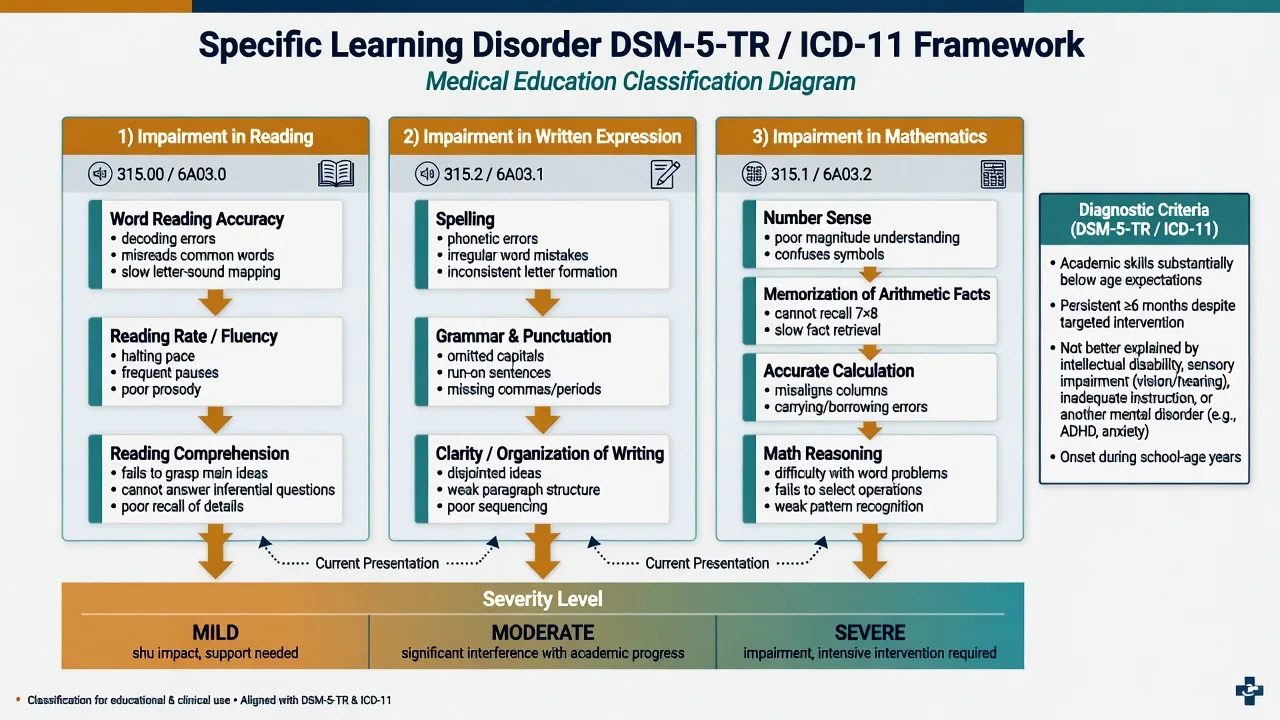
| Domain (DSM-5-TR style) | Core skill probes | Common labels |
|---|---|---|
| Reading | Word reading accuracy; reading rate/fluency; reading comprehension | Dyslexia (often word-level decoding/fluency) |
| Written expression | Spelling accuracy; grammar and punctuation; clarity/organisation of written expression | Dysgraphia (terminology varies; graphomotor vs linguistic) |
| Mathematics | Number sense; memorisation of arithmetic facts; accurate/fluent calculation; mathematical reasoning | Dyscalculia |
| Domain map for exams; a child may meet criteria in one or more domains.[6][13][15] |
Severity (mild / moderate / severe) reflects the degree of academic and adaptive impact and the intensity of supports required, not a single cut-score fetish.[6]
Historical discrepancy versus instructional response
Older IQ–achievement discrepancy models (achievement far below IQ) under-served many struggling readers and over-emphasised a single test day. Contemporary science privileges inadequate response to effective, well-implemented instruction plus documented skill deficits — response-to-intervention (RTI) / multi-tiered systems of support thinking integrated with comprehensive evaluation.[6][7]
Snowling and Hulme's classification commentary for DSM-era reform stresses that reading disorders are heterogeneous (word-level vs language-based comprehension failure) and that oral language is not an optional footnote.[14][15]
Reading SLD
- Decoding / fluency core
- Phonological vulnerability
- Structured literacy Rx
- Dyslexia shorthand
Writing SLD
- Spelling + organisation
- Graphomotor may contribute
- Assistive tech useful
- Oral > written ideas
Math SLD
- Number sense gaps
- Fact retrieval weak
- Word-problem load
- Dyscalculia science
Not SLD alone
- Global ID lag
- No opportunity to learn
- Uncorrected sensory loss
- Primary language disorder only
Epidemiology and risk
Patterns candidates should own
Community studies show meaningful prevalence of domain-specific learning disorders with gender differences that vary by domain — reading difficulties are often identified more frequently in boys in school-referred samples, while patterns for mathematics differ; always interpret ascertainment bias.[8]
Familial aggregation for reading disability is robust; twin and molecular work support substantial heritability with a polygenic architecture (dozens of genome-wide significant loci in large dyslexia GWAS), not a single dyslexia gene test for clinics.[3][16]
Risk concentrates with family history of learning problems, early language delay, weak phonological awareness, ADHD traits, and limited access to high-quality early literacy instruction. Poverty and disrupted schooling raise under-identification and under-intervention risk without making SLD a pure social label.[4][6]
Comorbidity among reading, writing and math disabilities is common, as is ADHD–reading disability dual presentation with additive functional burden.[10][11]
Pathophysiology and mechanisms
Reading disability / dyslexia
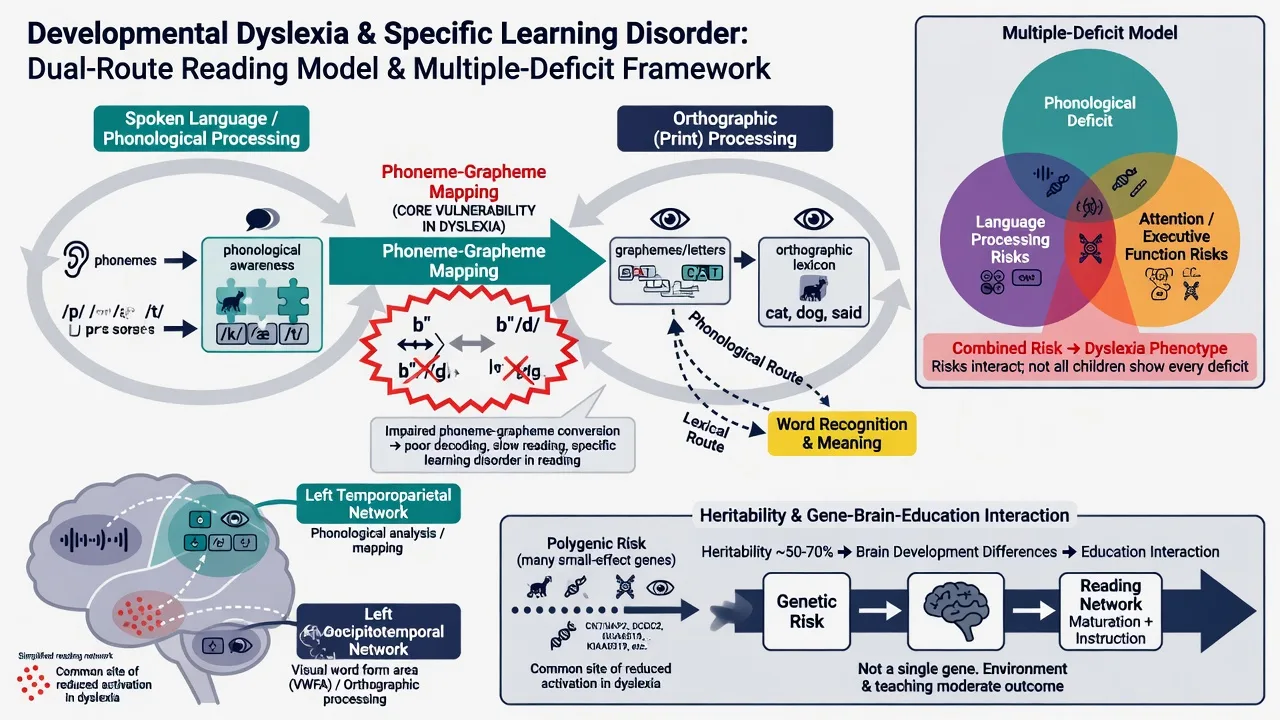
Four decades of research converge on phonological processing weaknesses and inefficient phoneme–grapheme mapping as core to many cases of word-level reading disability, within a distributed left-hemisphere reading network — not a primary vision problem as the main causal story for typical developmental dyslexia.[2][3][4]
Oral language skills (vocabulary, grammar, listening comprehension) strongly shape reading comprehension outcomes even when decoding is remediated — Snowling and Hulme re-centre language in the reading disorders research agenda.[14]
Multiple-deficit model
Pennington's multiple-deficit model argues single cognitive deficits are often insufficient; combinations of phonological, language, and attention/executive risks raise probability of clinically impairing learning disorders and help explain comorbidity patterns.[9][10]
Mathematics and written expression
Dyscalculia frameworks highlight foundational numerical capacity / number sense difficulties with educationally actionable implications rather than pure motivational failure.[12]
Disorder of written expression / dysgraphia involves overlapping orthographic, linguistic, graphomotor and executive-organisation components; assessment separates handwriting mechanics from spelling and composition quality.[13]
Clinical presentation
What teachers and parents report
- Avoidance of reading aloud; slow effortful decoding; wild guesses from pictures/context
- Spelling that mirrors phonological errors; sparse written work despite rich oral ideas
- Incomplete maths homework; reliance on fingers; collapse on word problems
- Homework battles, "lazy" attributions, demoralisation, irritability when academic demand rises
- Secondary anxiety, school refusal, or disruptive behaviour as performance pressure mounts These multi-domain school presentations are classic referral triggers for SLD assessment and formulation.[1][2][6]
Adolescent and adult presentations include slow reading under time pressure, exam underperformance despite knowledge, and occupational literacy/numeracy barriers despite compensatory intelligence.[1][2][6]
Age banding
Early primary: decoding and spelling struggle despite exposure. Middle childhood: fluency and written output gaps widen; comorbidity attention/anxiety more visible. Secondary: curriculum volume and exam speed unmask compensated readers; identity and self-esteem stakes rise. Adult: tertiary/vocational discovery when supports fall away.[1][6]
Differential diagnosis
- Intellectual disability — broad cognitive and adaptive deficits; academic lag roughly proportional; still describe relative academic strengths/weaknesses carefully.[1][6]
- Language disorder — oral language impairment drives literacy failure; SLD reading comprehension subtype may be language-based (Snowling/Hulme framing).[14][15]
- ADHD — incomplete work and careless errors without true skill deficit vs true dual diagnosis (common).[11]
- Sensory impairment — uncorrected hearing/vision mimicking academic failure.[1]
- Inadequate instruction / interrupted schooling / second-language acquisition — opportunity and language-of-instruction gates before SLD label.[6][7]
- Anxiety, depression, trauma — performance drop without primary skill disorder (or secondary to SLD).[1]
- ASD — uneven academic profile with social-communication phenotype.[1]
Bedside assessment
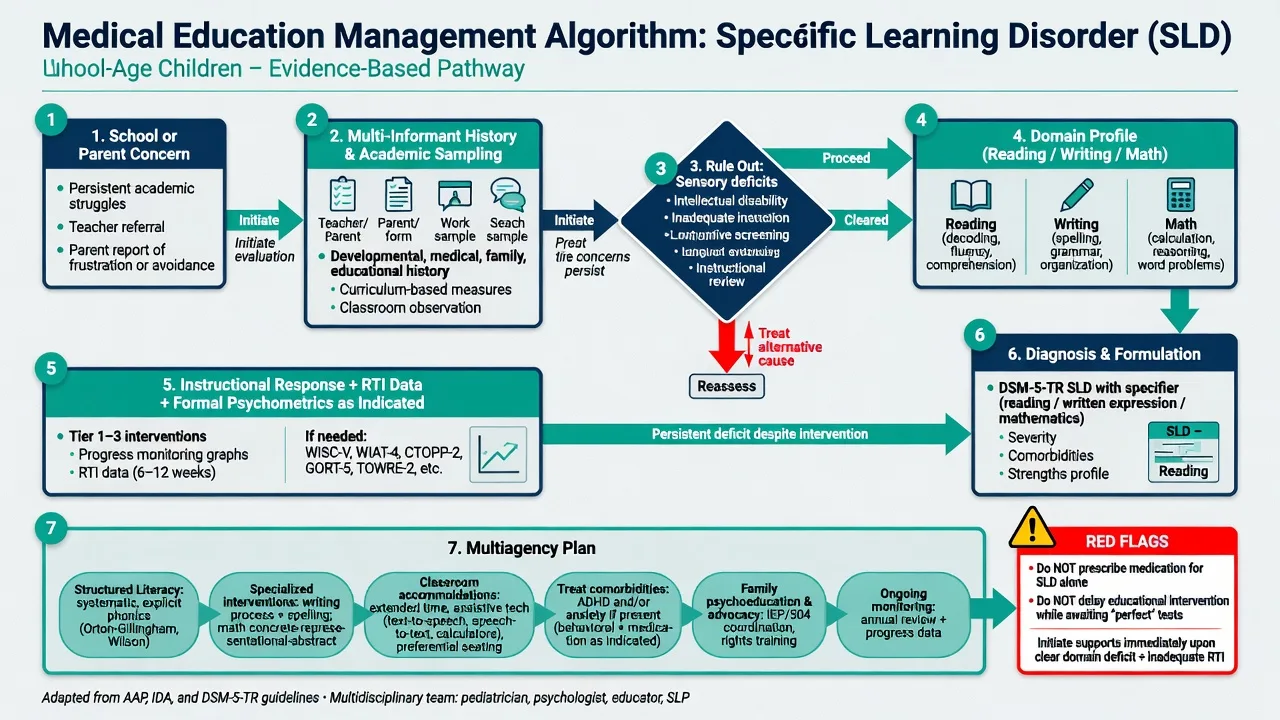
- Multi-informant history: pregnancy/neonatal, milestones (especially language), early literacy exposure, school trajectory year-by-year, interventions tried and response, family academic history, medical/sensory status, bullying, mood.
- Work samples and curriculum-based measures; teacher report of instructional intensity.
- Mental state: self-concept as learner, anxiety about school, attention, hopelessness, self-harm if demoralisation severe.
- Screen ADHD, anxiety, depression; adaptive function if ID in differential.
- Document hearing and vision.
- Consent/assent; interpreters for CALD families — bilingualism is not pathology.[1][6][7]
Investigations and psychometrics
There is no laboratory test for SLD. Investigation is exclusionary and formulation-supporting.[1]
- Confirm hearing and vision; medical/neurological review if regression or focal signs.
- Educational psychology / neuropsychology: standardised achievement (decoding, fluency, comprehension; spelling/writing; mathematics) ± cognitive profile.
- Instructional response data are identification-critical — a single low score without intervention history is incomplete science.[6][7]
- Speech-language assessment when oral language contribution is suspected; occupational therapy when graphomotor dysgraphia is prominent.[13][14]
Do not require a rigid historical IQ–discrepancy cut alone to unlock supports when skill deficits and poor instructional response are clear.[6][7]
Acute safety
Definitive management
Educational intervention (core treatment)
For word-level reading disabilities, meta-analysis of randomised trials supports phonics-based treatment approaches as the intervention class with the clearest efficacy signal among tested modalities.[5]
Fellowship language: intensive, systematic, explicit instruction (often described as structured literacy frameworks in educational practice) targeting phonological awareness, phoneme–grapheme mapping, decoding, fluency and then comprehension — matched to assessed profile and oral language needs.[4][5][14]
Mathematics and writing interventions should be similarly explicit, cumulative and practice-rich, addressing number sense/fact retrieval or spelling–composition–handwriting components as indicated.[12][13]
Do not wait for a perfect complete battery if functional need for intensive support is already clear — parallel assessment and intervention.[6][7]
Accommodations and systems
Classroom and exam accommodations (extra time, reduced copying, text-to-speech, speech-to-text, note-taking supports, alternative demonstration of knowledge) reduce unnecessary disability from time/format barriers while skill intervention proceeds. Exact schemes are jurisdiction-specific (NCCD/IEP/EHCP-type pathways) — state principles, not invented section numbers.[1][6]
Psychiatric comorbidity
Treat ADHD, anxiety and depression on disorder-specific evidence. Medication does not remediate dyslexia, but treating ADHD can improve availability for learning; treating anxiety can reduce avoidance. Avoid polypharmacy aimed at "making them try harder."[1][11]
Family psychoeducation
SLD is neurodevelopmental and heritable in many pedigrees; it is not laziness. Strengths-based advocacy, realistic timelines, and alliance with school learning-support teams are therapeutic acts.[2][3][16]
Australian and New Zealand practice pairs school learning support and educational psychology pathways with CAMHS input when comorbidity, risk or diagnostic complexity is high. Use local NCCD/education adjustment processes; cultural safety for Aboriginal and Torres Strait Islander and Māori learners is mandatory — do not pathologise bilingual development or collective caregiving.[1][6]
| Target | Prefer | Avoid |
|---|---|---|
| Identification | Skill deficit + instructional response + multi-source history | IQ-discrepancy only; single test day |
| Reading Rx | Systematic phonics / structured literacy intensity | Vision training as primary dyslexia cure |
| Writing/math | Explicit domain-matched instruction + OT/SALT as needed | "Try harder" without skill teaching |
| Classroom | Accommodations + intervention | Accommodations alone forever |
| Medication | Treat ADHD/mood/anxiety if criteria met | Stimulants for pure SLD |
| Framing | Neurodevelopmental skill disorder | Laziness / bad parenting |
| Framework for exams; individualise and follow local education governance.[5][6][7][11] |
Formulation (exam product)
A complete SLD formulation includes: academic trajectory and domains affected; biological factors (family history, polygenic risk narrative, language/phonological vulnerabilities, ADHD traits, sensory status); psychological factors (self-concept, anxiety, avoidance, attention); social/systemic factors (instructional quality/intensity, school fit, peers/bullying, culture/language, resources); 4Ps; risk; working diagnoses (SLD with domain/severity specifiers ± comorbidity); and a plan mapped to factors (intervention intensity, accommodations, comorbidity care, review metrics).[1][6][9]
Prognosis and disposition
SLD is typically persistent. Skills often improve substantially with early intensive evidence-based intervention, yet reading/writing/math may remain effortful relative to peers. Untreated or unsupported SLD elevates risk of school disengagement, low self-esteem and secondary mental health problems. Disposition matches intensity of educational need and psychiatric risk; plan transition supports for secondary, tertiary and workplace accommodations.[2][3][6]
Special populations
Twice-exceptional (gifted + SLD) students may compensate until curriculum acceleration exposes specific skill gaps — do not dismiss parent/teacher concern because conversation sounds bright. CALD and bilingual learners need language-of-instruction care. Looked-after children may have both true SLD and opportunity gaps. In ID or ASD, specify relative academic profiles rather than assuming global explanation for every skill gap.[1][6][14]
Evidence and guidelines (exam anchors)
- AACAP practice parameters for language and learning disorders (assessment/treatment principles).[1]
- Peterson & Pennington dyslexia reviews; Vellutino four-decade synthesis.[2][3][4]
- Galuschka phonics meta-analysis; Grigorenko/Fletcher SLD science and instructional-response identification.[5][6][7]
- Moll prevalence; Willcutt comorbidity; Pennington multiple-deficit model.[8][9][10][11]
- Butterworth dyscalculia; Chung written expression; Snowling/Hulme language–reading reviews; Doust polygenic dyslexia loci.[12][13][14][15][16]
Exam pearls
SLD exam anchors
High-yield one-liners: SLD is not low IQ. Dyslexia is not cured by glasses training as primary care. ADHD comorbidity is common — assess both. Never call it laziness. Parallel intervention while you finish testing. Hearing and vision before complex labelling.[1][4][11]
References
- [1]American Academy of Child and Adolescent Psychiatry Practice parameters for the assessment and treatment of children and adolescents with language and learning disorders. AACAP J Am Acad Child Adolesc Psychiatry, 1998.PMID 9785728
- [2]Peterson RL, Pennington BF Developmental dyslexia Lancet, 2012.PMID 22513218
- [3]Peterson RL, Pennington BF Developmental dyslexia Annu Rev Clin Psychol, 2015.PMID 25594880
- [4]Vellutino FR, Fletcher JM, Snowling MJ, Scanlon DM Specific reading disability (dyslexia): what have we learned in the past four decades? J Child Psychol Psychiatry, 2004.PMID 14959801
- [5]Galuschka K, Ise E, Krick K, Schulte-Körne G Effectiveness of treatment approaches for children and adolescents with reading disabilities: a meta-analysis of randomized controlled trials PLoS One, 2014.PMID 24587110
- [6]Grigorenko EL, Compton DL, Fuchs LS, Wagner RK, Willcutt EG, Fletcher JM Understanding, educating, and supporting children with specific learning disabilities: 50 years of science and practice Am Psychol, 2020.PMID 31081650
- [7]Miciak J, Fletcher JM The Critical Role of Instructional Response for Identifying Dyslexia and Other Learning Disabilities J Learn Disabil, 2020.PMID 32075514
- [8]Moll K, Kunze S, Neuhoff N, Bruder J, Schulte-Körne G Specific learning disorder: prevalence and gender differences PLoS One, 2014.PMID 25072465
- [9]Pennington BF From single to multiple deficit models of developmental disorders Cognition, 2006.PMID 16844106
- [10]Willcutt EG, McGrath LM, Pennington BF, Keenan JM, DeFries JC, Olson RK, Wadsworth SJ Understanding Comorbidity Between Specific Learning Disabilities New Dir Child Adolesc Dev, 2019.PMID 31070302
- [11]Willcutt EG, Petrill SA Comorbidity between reading disability and ADHD in a community sample: Implications for academic, social, and neuropsychological functioning Mind Brain Educ, 2023.PMID 38898939
- [12]Butterworth B, Varma S, Laurillard D Dyscalculia: from brain to education Science, 2011.PMID 21617068
- [13]Chung PJ, Patel DR, Nizami I Disorder of written expression and dysgraphia: definition, diagnosis, and management Transl Pediatr, 2020.PMID 32206583
- [14]Snowling MJ, Hulme C Annual Research Review: Reading disorders revisited - the critical importance of oral language J Child Psychol Psychiatry, 2021.PMID 32956509
- [15]Snowling MJ, Hulme C Annual research review: the nature and classification of reading disorders--a commentary on proposals for DSM-5 J Child Psychol Psychiatry, 2012.PMID 22141434
- [16]Doust C, Fontanillas P, Eising E, Gordon SD, et al. Discovery of 42 genome-wide significant loci associated with dyslexia Nat Genet, 2022.PMID 36266505