Psych · Child and adolescent psychiatry — neurodevelopmental
Tic disorders and Tourette syndrome
Also known as Tourette syndrome · Tourette's disorder · Gilles de la Tourette syndrome · Chronic tic disorder · Persistent motor tic disorder · Provisional tic disorder · CBIT · Habit reversal training
Exam-exhaustive fellowship reference on tic disorders and Tourette syndrome — DSM-5-TR classification, CSTC pathophysiology, CBIT evidence, alpha-2 agonists and antipsychotics with dosing and monitoring, and ADHD/OCD comorbidity management. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
Target exams
Red flags
Tic disorders and Tourette syndrome are high-yield across FRANZCP CAP, MRCPsych, ABPN and MD/DNB. Examiners test classification without coprolalia myths, the natural history of peak-and-improve course, CBIT by name, disciplined pharmacology (alpha-2 agonists before or instead of heavy antipsychotics when appropriate), and the management of ADHD and OCD comorbidity — including the trap that stimulants are absolutely contraindicated.[3][5][9][15]
Overview and definition
A tic is a sudden, rapid, recurrent, non-rhythmic motor movement or vocalisation. Tics are typically suggestible, briefly suppressible, and associated with a rising premonitory urge that is relieved by performance of the tic — a negative-reinforcement loop that behaviour therapy targets.[5][19]
Simple motor tics include eye blinking, facial grimacing, head jerking and shoulder shrugging. Simple phonic (vocal) tics include sniffing, throat clearing, grunting and squeaking. Complex forms include coordinated sequences, echopraxia, copropraxia, words or phrases, echolalia, palilalia and — in a minority — coprolalia. Coprolalia is neither required nor typical for a Tourette diagnosis — a classic exam myth.[5][8]

Classification
DSM-5-TR skeleton (must own)
| Diagnosis | Core rule of thumb |
|---|---|
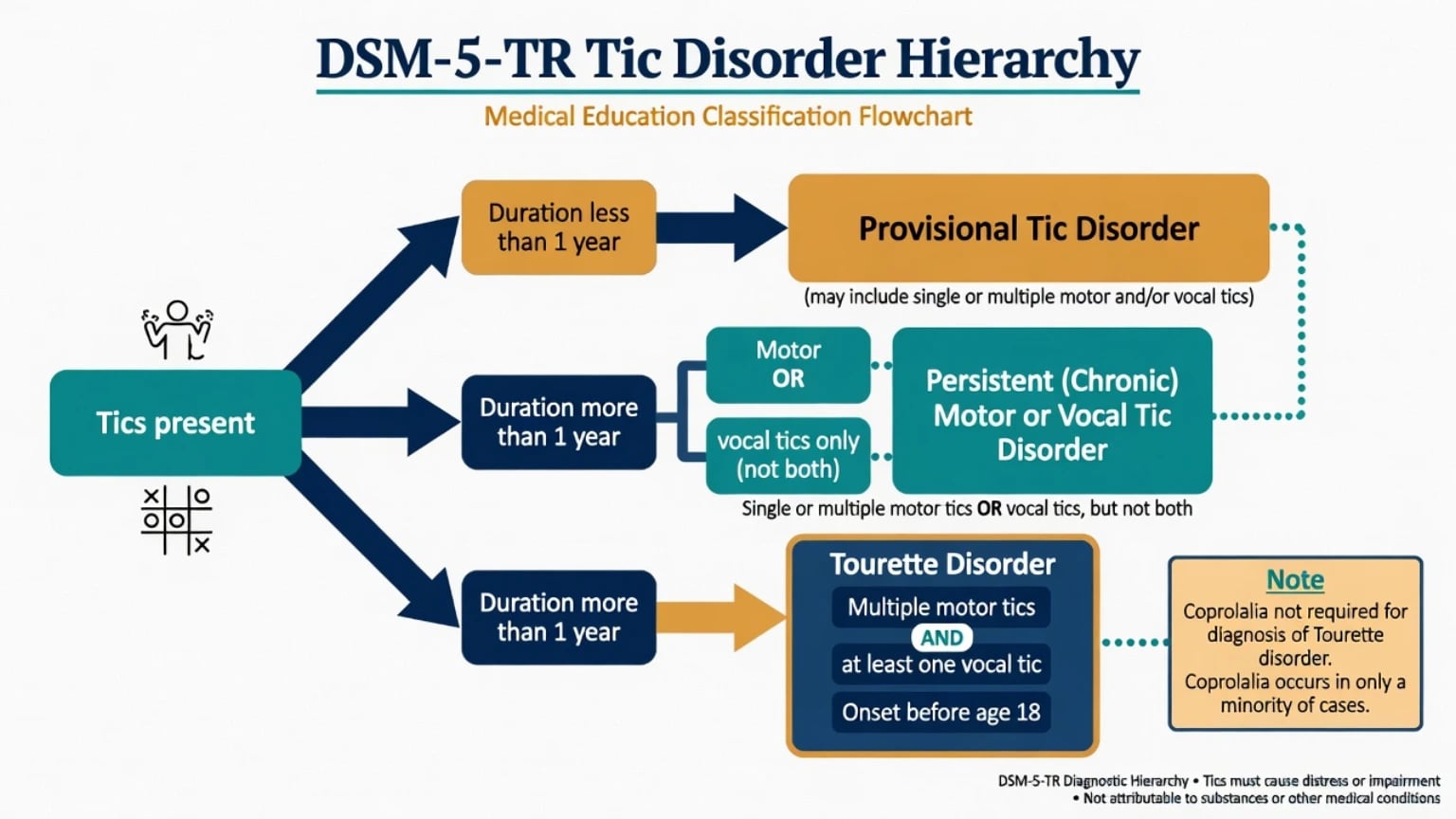
| Provisional tic disorder | Single or multiple motor and/or vocal tics; less than 1 year since first tic; onset before 18; not substance/medical |
| Persistent (chronic) motor or vocal tic disorder | Motor or vocal tics (not both) present at some time; more than 1 year since first tic; onset before 18 |
| Tourette's disorder | Multiple motor and at least one vocal tic at some time (not necessarily concurrent); more than 1 year since first tic; onset before age 18; not attributable to substance or another medical condition |
| Other specified / unspecified | Clinically significant tics not meeting full criteria |
| Hierarchy note | If Tourette criteria are met, do not also diagnose provisional or persistent motor/vocal tic disorder for the same presentation |
| DSM-5-TR duration, onset-before-18, and motor-plus-vocal rules above are the examinable classification skeleton used throughout this topic.[5] |
ICD-11 retains Tourette syndrome and chronic motor or vocal tic disorder concepts. State which manual you are applying when thresholds are examined. Functional neurological tic-like behaviours may enter the differential in abrupt late-onset presentations and should not be forced into lifelong primary tic nosology without formulation.[16]
Provisional
- Duration under 1 year
- Often mild/transient
- Psychoeducation first
- Many remit
Persistent motor/vocal
- Over 1 year
- Motor OR vocal only
- May still be mild
- Same stepped care logic
Tourette
- Multiple motor + at least one vocal
- Not necessarily concurrent
- Onset before 18; course over 1 year
- High comorbidity rates
Not required
- Coprolalia
- Daily continuous tics
- Abnormal MRI
- Childhood IQ test
Epidemiology and risk
Numbers candidates should own
Knight and colleagues' systematic review and meta-analysis quantified population prevalence estimates for tic disorders and demonstrated how case definition and sampling drive rates — exam answers should use order-of-magnitude figures, not false clinic precision.[18] International clinical databases show very high rates of ADHD, OCD and other neuropsychiatric comorbidity in people meeting Tourette criteria.[8] Hirschtritt and colleagues quantified lifetime psychiatric comorbidity and familial relationships in Tourette syndrome, reinforcing shared liability with OCD and ADHD rather than a pure "motor only" disease model.[6]
Course. Tic severity often peaks in late childhood or early adolescence, with many individuals improving substantially into adulthood; residual mild tics are common. Prognosis for function is frequently determined more by comorbidity and social environment than by peak YGTSS alone.[7][19]
Pathophysiology
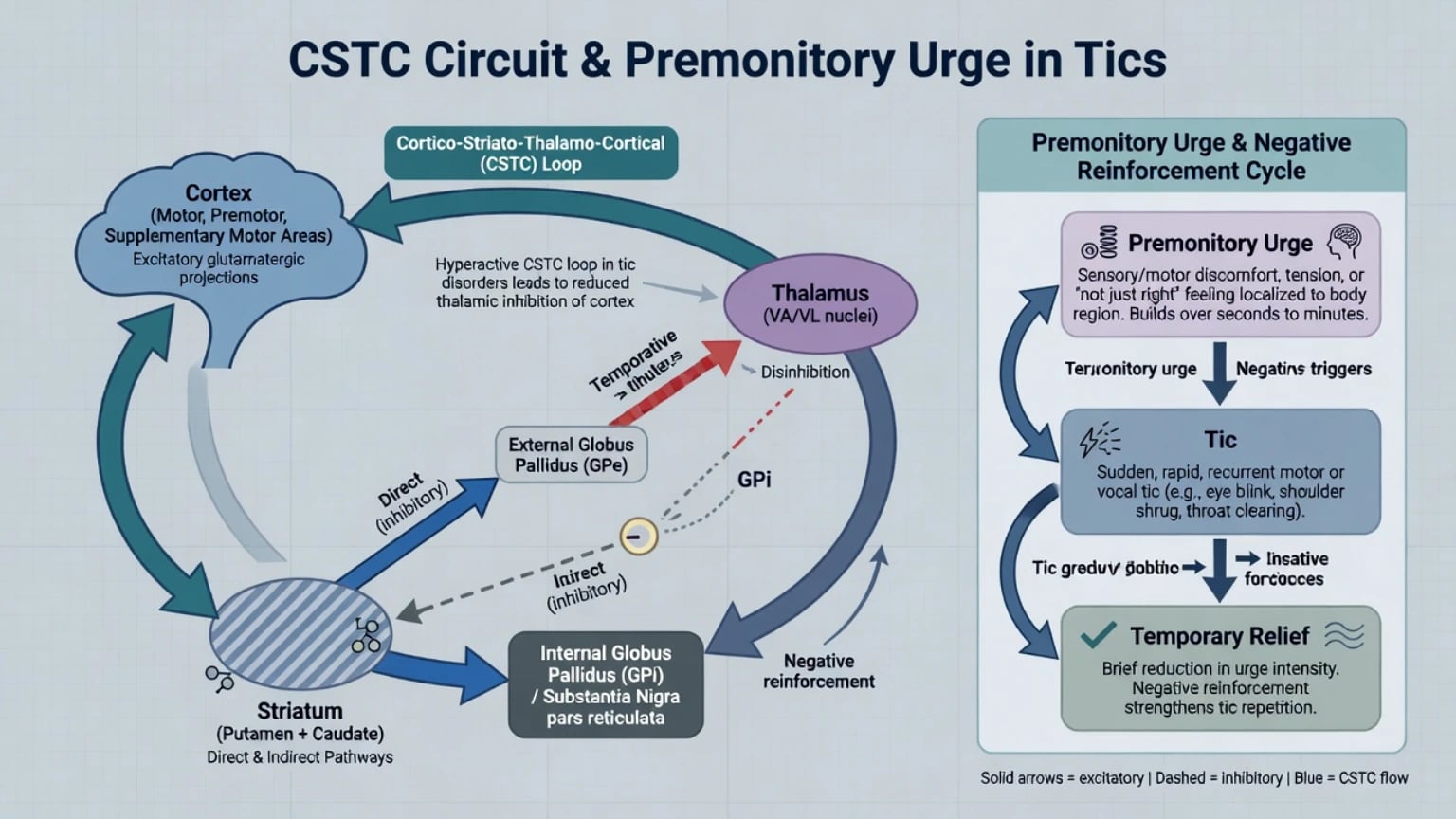
Teaching-level pathophysiology emphasises cortico-striato-thalamo-cortical (CSTC) circuit dysregulation with impaired inhibition of motor programmes. Dopaminergic modulation of striatal pathways is clinically relevant because D2-antagonist antipsychotics reduce tics — mechanism is not full explanation. Premonitory sensory phenomena and urge-driven performance with temporary relief explain why habit reversal (competing response) and related CBIT components work.[5][15] Genetic contribution is substantial and polygenic at population level; first-degree family history of tics, OCD or ADHD is clinically useful risk context, not a diagnostic test.[6]
Clinical presentation
History. Age and type of first tic; subsequent repertoire; waxing and waning; suppressibility and cost; premonitory urges; triggers (stress, excitement, fatigue, screen transitions); school, peer and family impact; self-injurious tics; sleep; bullying and shame.[5][19]
Observation. Many children suppress in clinic; accept parent video and school reports. Describe topography without moral language. Complex phonic tics can be mistaken for oppositional behaviour or respiratory disease (chronic "sniff/cough" work-ups).[5]
MSE. Note observed tics, urge language, insight, mood, anxiety, ADHD features, and OCD phenomena. Assess suicide risk when bullying, depression or severe shame are present.[6]
Differential diagnosis
Discriminators matter more than lists:
- Stereotypies — more rhythmic/patterned, often earlier onset, associated with ASD/ID, less urge-driven suppressibility pattern.
- Compulsions — goal-directed, rule-bound, anxiety-reducing; complex tics are urge-driven and less "purposeful," though mixed phenomenology is common in TS+OCD.
- Myoclonus, dystonia, chorea, seizures — neurological red flags, especially if progressive or without suppressibility/urge features.
- Drug-induced movements — stimulant unmasking/worsening of tics possible but not universal; antipsychotics risk tardive syndromes; document temporal course.
- Functional tic-like behaviours — often abrupt, elaborate, socially mediated onset in adolescence/adulthood without classic childhood TS course; formulate carefully and avoid punitive framing.
- PANDAS/PANS — historically controversial constructs; do not over-attribute ordinary developmental tics to streptococcal infection without specialist criteria and work-up logic.
Assessment
Structure: phenotype + duration + onset age + impairment + comorbidity + risk + family beliefs + school ecology.[5]
- Map motor and phonic tics with timeline (first tic → 12-month rule).
- Multi-informant history and, if needed, video.
- Screen systematically for ADHD, OCD/related, anxiety, mood, ASD, learning, sleep and substances — comorbidity is the rule, not the exception.[6][8]
- Functional impact: classroom, handwriting, speaking in class, sport, friendships, family conflict.
- Risk: self-injurious tics, bullying, school refusal, self-harm.
- Shared decision-making with young person and caregivers; correct punishment myths.
YGTSS (Yale Global Tic Severity Scale) is the clinician gold standard for severity (number, frequency, intensity, complexity, interference for motor and phonic domains, plus impairment). Use for measurement-based care; it does not replace clinical diagnosis.[19]
Investigations
Classic developmental tics are a clinical diagnosis. Routine MRI, EEG or extensive blood panels are not indicated without red flags (late abrupt progressive course, focal neurology, encephalopathy, seizures, regression).[5]
Before alpha-2 agonists or antipsychotics: height/weight/BMI, BP, HR, cardiac history, baseline movement examination; metabolic labs as indicated for antipsychotics; ECG when cardiac risk factors or interacting drugs warrant. Serial vitals on clonidine/guanfacine; metabolic/EPS/prolactin vigilance on risperidone and related agents.[11][12][14][17]
Acute safety
Definitive management
Psychoeducation and watchful care
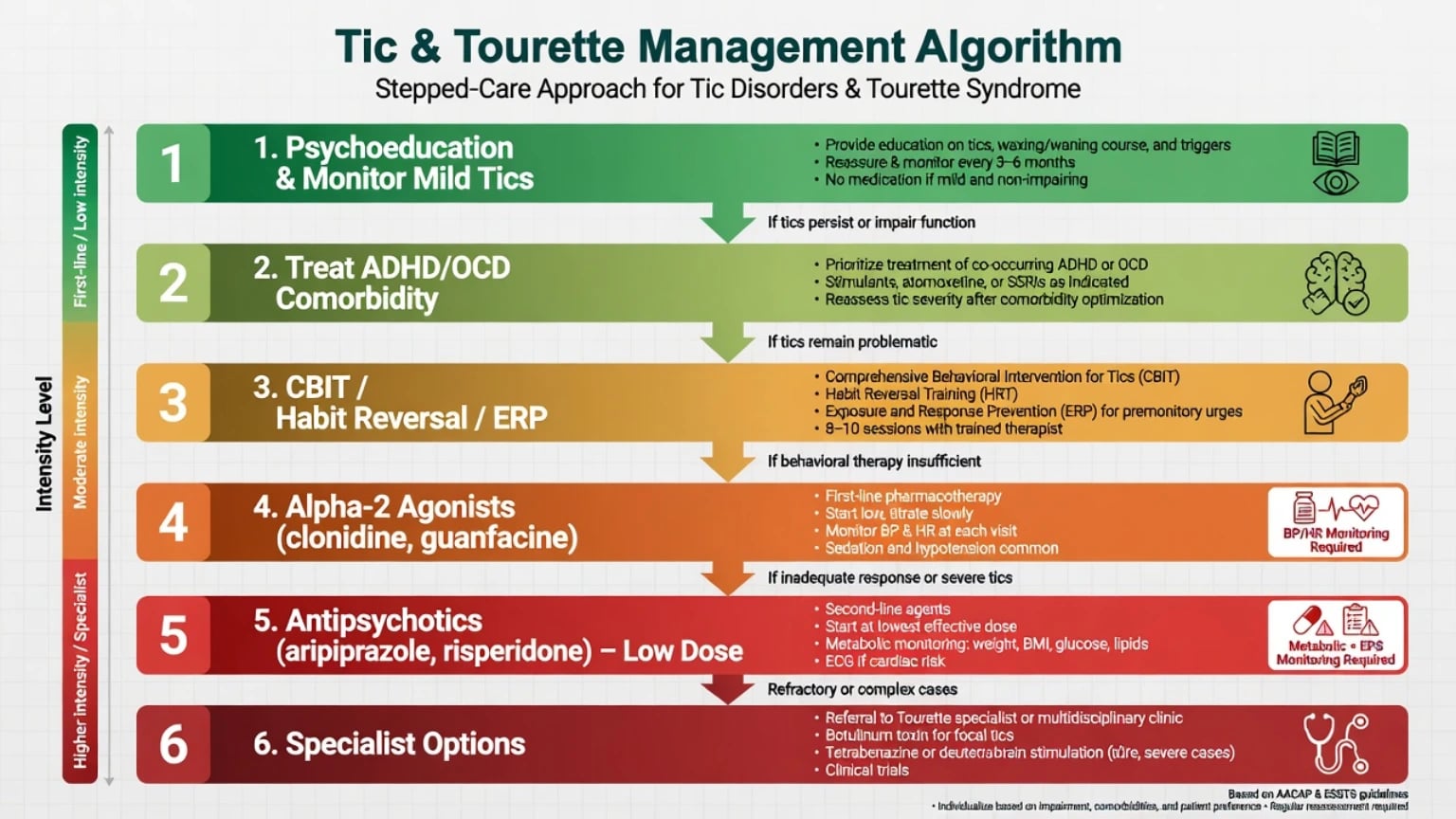
For mild, non-impairing tics: explain natural history (peak then often improve), suppressibility myths, and the harm of punishment. School advice: ignore tics when safe, allow brief breaks, no public shaming, exam accommodations if needed. Treat sleep, anxiety and ADHD drivers that amplify tic expression.[5][7][16]
Comprehensive Behavioral Intervention for Tics (CBIT)
CBIT combines habit reversal training (awareness training, competing response practice), function-based interventions (identify antecedents/consequences that worsen tics), and relaxation components. In children and adolescents, the multicentre RCT by Piacentini and colleagues showed CBIT superior to supportive control for tic severity — foundational exam evidence.[1] In adults, Wilhelm and colleagues demonstrated benefit of behaviour therapy versus supportive control.[2] European ESSTS guidance positions evidence-based psychological interventions (CBIT/HRT and related packages including exposure and response prevention for tics) as core treatments.[15][16]
AAN 2019 practice guideline recommendations support clinician counselling about CBIT and shared decisions on when to use behavioural versus pharmacological strategies.[3][4]
Pharmacotherapy — when and how
Medication is for impairing tics after informed discussion, often alongside or after behavioural options, or when CBIT is inaccessible/ineffective/not preferred. Treat comorbidity in parallel.[3][14][17]
Alpha-2 adrenergic agonists (often first pharmacological class in youth)
Clonidine and guanfacine reduce tics in many patients and help ADHD-related hyperactivity/impulsivity. Scahill and colleagues showed guanfacine superior to placebo for children with tic disorders and ADHD on ADHD outcomes with tic-relevant benefit context — foundational alpha-2 evidence in this dual population.[10] Canadian pharmacotherapy guidance and later AAN/ESSTS syntheses support alpha-2 agonists as relatively well-tolerated first medication options for many youth.[3][14][17]
Exam-level dosing frameworks (always individualise; check local product information and specialist advice):
| Agent | Typical paediatric framework | Monitoring |
|---|---|---|
| Clonidine (oral) | Low start (often on the order of 0.05 mg at night or divided; titrate slowly toward roughly 0.1–0.3 mg/day in divided doses in many protocols — product- and weight-dependent) | BP, HR, sedation, dry mouth; taper on cessation |
| Guanfacine (IR/XR where available) | IR often started around 0.5–1 mg daily with slow titration (trial literature commonly used total daily doses in the 1–4 mg range depending on age/weight/response); XR products are formulation-specific | BP, HR, sedation, constipation; taper when stopping |
| Abrupt cessation of long-term alpha-2 agonists risks rebound hypertension and autonomic symptoms — teach tapering.[10][14][17] |
Antipsychotics (more severe impairing tics)
Dopamine D2-blocking agents have the strongest traditional anti-tic efficacy but higher adverse-effect burden. Modern practice prefers aripiprazole and risperidone over first-generation agents for many patients.[3][14][17]
Aripiprazole. Multicentre paediatric RCTs (including Yoo et al. and Sallee et al.) support efficacy versus placebo for Tourette's disorder. Typical exam framework: start low (commonly 2 mg oral daily in children/adolescents, titrate slowly; many responders in the approximate 2–10 mg/day range depending on age/weight/response — verify PI). Monitor weight, metabolic parameters, akathisia, sedation, and rare impulse-control issues.[12][13]
Risperidone. Placebo-controlled trial data support tic reduction. Exam framework: start very low (e.g. 0.25–0.5 mg oral daily, titrate slowly; effective totals often in the approximate 0.5–2 mg/day paediatric range in tic trials — individualise). Monitor weight, BMI, glucose/lipids, EPS, sedation and prolactin-related effects (galactorrhoea, menstrual change, sexual side-effects).[11][14][17]
Older agents (haloperidol, pimozide) are historically effective but carry higher EPS, prolactin and (for pimozide) QTc concerns — reserve for specialist refractory pathways.[14][17]
| Scenario | Prefer | Caution |
|---|---|---|
| Mild non-impairing tics | Psychoeducation | Unnecessary medication |
| Impairing tics, BT available | CBIT ± meds | Waiting forever if severe self-injury |
| Youth needing meds, ADHD features | Alpha-2 agonist trial | Sedation; taper rules |
| Severe impairing tics | Aripiprazole or risperidone low-dose | Metabolic/EPS/prolactin |
| TS + ADHD core symptoms | Treat ADHD (see below) | Automatic stimulant ban myth |
| TS + OCD | CBT/ERP ± SSRI for OCD | Mistaking compulsions for tics only |
| Framework for exams; verify local product information and governance.[1][3][9][14][17] |
Regional practice notes
Australian and New Zealand practice aligns with stepped psychoeducation, access to behavioural interventions where available, alpha-2 agonists for many youth needing medication, and cautious antipsychotic use with metabolic monitoring. Commissioning of formal CBIT varies by service; name the components (HRT + function-based strategies) even when a branded CBIT programme is unavailable.[5][16]
Comorbidity focus: ADHD and OCD
ADHD
ADHD is among the most common comorbidities and often drives academic failure, injury risk and family conflict more than tics alone.[6][8]
Exam trap: "Stimulants are contraindicated in Tourette." The Tourette's Syndrome Study Group RCT in children with ADHD and tics found that methylphenidate and clonidine (alone and combined, depending on outcomes) can be used with benefit for ADHD; tics were not systematically worsened as a class effect in the manner folklore suggests.[9] Bloch and colleagues' meta-analysis of ADHD treatments in youth with comorbid tics similarly supports that stimulants can be effective for ADHD without a consistent large tic-worsening signal across studies — still monitor tics individually.[20] Alpha-2 agonists remain attractive when both ADHD and tics are targets or when stimulant risk/preference warrants alternatives.[10][14]
OCD and related phenomena
OCD and tic-related obsessive-compulsive symptoms are common; lifetime comorbidity is high in clinical and family studies.[6] Discriminate urge-driven complex tics from anxiety-reducing compulsions, then treat OCD with exposure and response prevention and, when indicated, SSRI pathways per OCD standards — while not abandoning tic-specific CBIT if tics remain impairing. "Just right" phenomena and symmetry concerns sit at the TS–OCD interface and should be formulated, not forced into one box.[5][6][15]
Prognosis and disposition
Many children improve after the early-adolescent peak; residual tics may persist without major impairment. Higher childhood severity, complex tics, and untreated ADHD/OCD predict more difficulty. Adult residual TS can still impair work, relationships and mood — adult behaviour therapy evidence exists.[2][7] Disposition: step intensity to impairment; maintain school liaison; plan transition to adult services when needed; review long-term antipsychotics for ongoing indication and metabolic burden.[3][14]
Complications and pitfalls
- Punishing or publicly shaming tics.[5]
- Missing ADHD/OCD while chasing every visible tic with antipsychotics.[6]
- Absolute stimulant ban in TS+ADHD without individualised trial/monitoring logic.[9][20]
- Starting high-dose antipsychotic without CBIT discussion or alpha-2 consideration when appropriate.[3][17]
- Omitting metabolic and movement monitoring on risperidone/aripiprazole.[11][12]
- Abrupt alpha-2 cessation.[14]
- Overcalling PANDAS or functional vs primary tic without careful formulation.[5][16]
Special populations
Preschool: mostly provisional tics; caregiver guidance; medication rare. Adolescents: peak severity, bullying, exam stress. Adults: residual tics, workplace stigma, adult CBIT evidence. ASD/ID: stereotypy differential; adapted behavioural strategies. Pregnancy: specialist shared decision if ongoing alpha-2 or antipsychotic treatment. Cultural safety: reduce stigma; partner with schools and families without pathologising difference.[2][5][7]
Exam pearls
TIC CARE plan
References
- [1]Piacentini J, Woods DW, Scahill L, et al. Behavior therapy for children with Tourette disorder: a randomized controlled trial JAMA, 2010.PMID 20483969
- [2]Wilhelm S, Peterson AL, Piacentini J, et al. Randomized trial of behavior therapy for adults with Tourette syndrome Arch Gen Psychiatry, 2012.PMID 22868933
- [3]Pringsheim T, Okun MS, Müller-Vahl K, et al. Practice guideline recommendations summary: Treatment of tics in people with Tourette syndrome and chronic tic disorders Neurology, 2019.PMID 31061208
- [4]Pringsheim T, Holler-Managan Y, Okun MS, et al. Comprehensive systematic review summary: Treatment of tics in people with Tourette syndrome and chronic tic disorders Neurology, 2019.PMID 31061209
- [5]Murphy TK, Lewin AB, Storch EA, Stock S Practice parameter for the assessment and treatment of children and adolescents with tic disorders J Am Acad Child Adolesc Psychiatry, 2013.PMID 24290467
- [6]Hirschtritt ME, Lee PC, Pauls DL, et al. Lifetime prevalence, age of risk, and genetic relationships of comorbid psychiatric disorders in Tourette syndrome JAMA Psychiatry, 2015.PMID 25671412
- [7]Bloch MH, Leckman JF Clinical course of Tourette syndrome J Psychosom Res, 2009.PMID 19913654
- [8]Freeman RD, Fast DK, Burd L, et al. An international perspective on Tourette syndrome: selected findings from 3,500 individuals in 22 countries Dev Med Child Neurol, 2000.PMID 10972415
- [9]Tourette's Syndrome Study Group Treatment of ADHD in children with tics: a randomized controlled trial Neurology, 2002.PMID 11865128
- [10]Scahill L, Chappell PB, Kim YS, et al. A placebo-controlled study of guanfacine in the treatment of children with tic disorders and attention deficit hyperactivity disorder Am J Psychiatry, 2001.PMID 11431228
- [11]Scahill L, Leckman JF, Schultz RT, et al. A placebo-controlled trial of risperidone in Tourette syndrome Neurology, 2003.PMID 12682319
- [12]Sallee F, Kohegyi E, Zhao J, et al. Randomized, Double-Blind, Placebo-Controlled Trial Demonstrates the Efficacy and Safety of Oral Aripiprazole for the Treatment of Tourette's Disorder in Children and Adolescents J Child Adolesc Psychopharmacol, 2017.PMID 28686474
- [13]Yoo HK, Joung YS, Lee JS, et al. A multicenter, randomized, double-blind, placebo-controlled study of aripiprazole in children and adolescents with Tourette's disorder J Clin Psychiatry, 2013.PMID 24021518
- [14]Roessner V, Eichele H, Stern JS, et al. European clinical guidelines for Tourette syndrome and other tic disorders-version 2.0. Part III: pharmacological treatment Eur Child Adolesc Psychiatry, 2022.PMID 34757514
- [15]Andrén P, Jakubovski E, Murphy TL, et al. European clinical guidelines for Tourette syndrome and other tic disorders-version 2.0. Part II: psychological interventions Eur Child Adolesc Psychiatry, 2022.PMID 34313861
- [16]Müller-Vahl KR, Szejko N, Verdellen C, et al. European clinical guidelines for Tourette syndrome and other tic disorders: summary statement Eur Child Adolesc Psychiatry, 2022.PMID 34244849
- [17]Pringsheim T, Doja A, Gorman D, et al. Canadian guidelines for the evidence-based treatment of tic disorders: pharmacotherapy Can J Psychiatry, 2012.PMID 22397999
- [18]Knight T, Steeves T, Day L, et al. Prevalence of tic disorders: a systematic review and meta-analysis Pediatr Neurol, 2012.PMID 22759682
- [19]Leckman JF, Riddle MA, Hardin MT, et al. The Yale Global Tic Severity Scale: initial testing of a clinician-rated scale of tic severity J Am Acad Child Adolesc Psychiatry, 1989.PMID 2768151
- [20]Bloch MH, Panza KE, Landeros-Weisenberger A, Leckman JF Meta-analysis: treatment of attention-deficit/hyperactivity disorder in children with comorbid tic disorders J Am Acad Child Adolesc Psychiatry, 2009.PMID 19625978