Psych · Child and adolescent psychiatry — service interface
Transition from CAMHS to adult services
Also known as CAMHS to AMHS transition · Child to adult mental health transition · Transitional age youth mental health · Youth mental health service boundary · Managed transition psychiatry · Care discontinuity at age 18
Exam-exhaustive fellowship reference on transition from CAMHS/CAP to adult mental health services — transfer versus transition, TRACK and MILESTONE evidence, age-boundary epidemiology, dual-threshold care gaps, managed transition components, youth 12–25 models, capacity and family involvement, and disposition pathways. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
The CAMHS–adult boundary is a high-yield service-interface topic for FRANZCP CAP and generalist viva, MRCPsych CASC, and essay work on systems of care. Examiners test whether you can separate transfer from transition, quote TRACK/MILESTONE logic, risk-stratify who needs specialist adult pathways, and write a disposition that does not abandon high-need youth at 18.[2][4][13]
Overview and definition
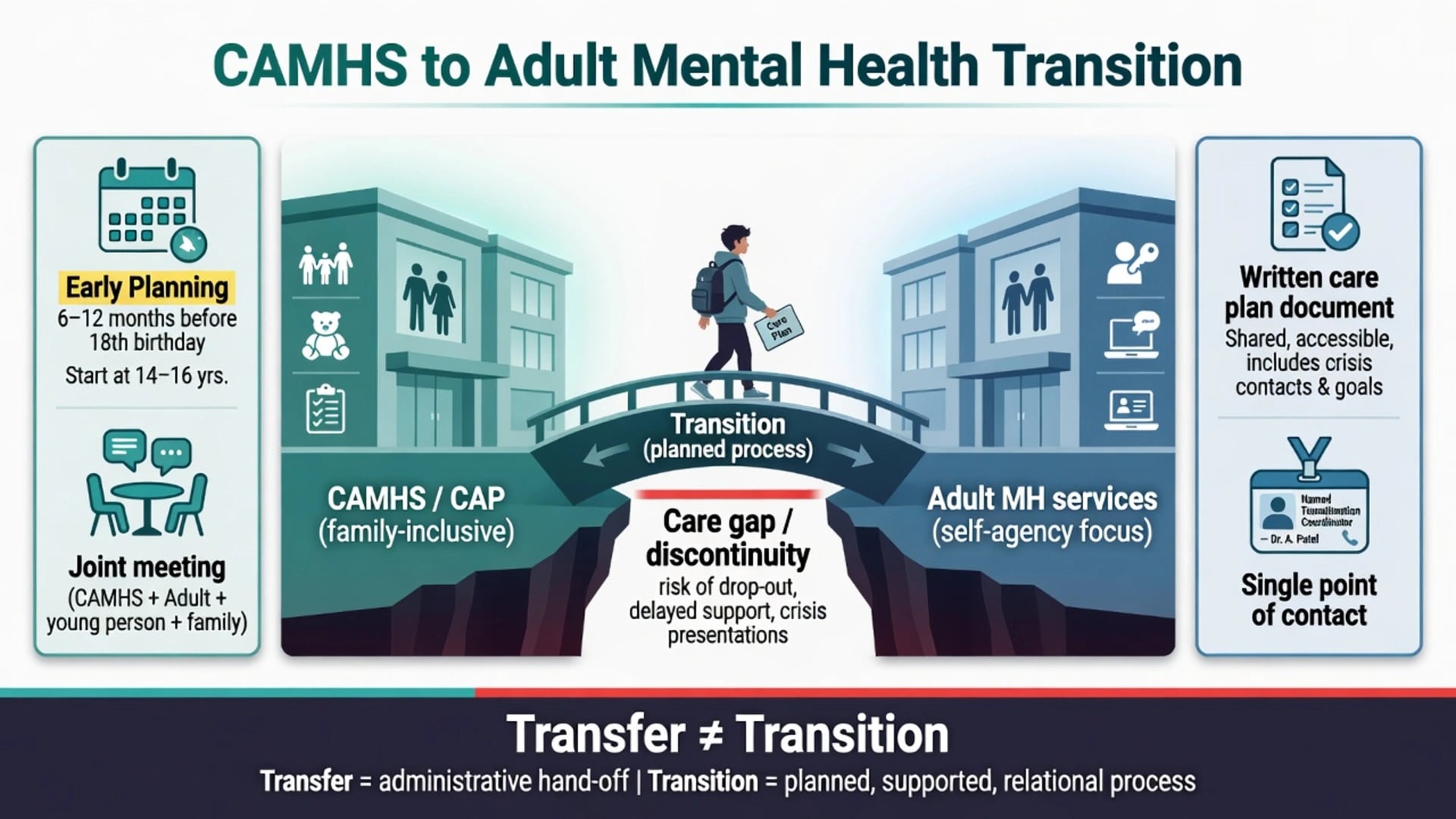
Blum and colleagues defined healthcare transition as the purposeful, planned movement of adolescents and young adults with chronic conditions from child-centred to adult-oriented health-care systems. The goal is uninterrupted, developmentally appropriate care — not a single hand-off letter on the eighteenth birthday.[1]
In mental health, transfer is the administrative move of an open case (or a referral). Transition spans preparation, information continuity, joint working, transfer, and successful engagement in the receiving service. Paul and colleagues synthesised TRACK findings around this distinction and the policy implications of age-based service architecture.[4][2]
DSM-5-TR and ICD-11 classify disorders, not transition quality. The exam task is clinical need, risk, capacity, pathway matching, and service design literacy.[9][10]
Classification of pathways
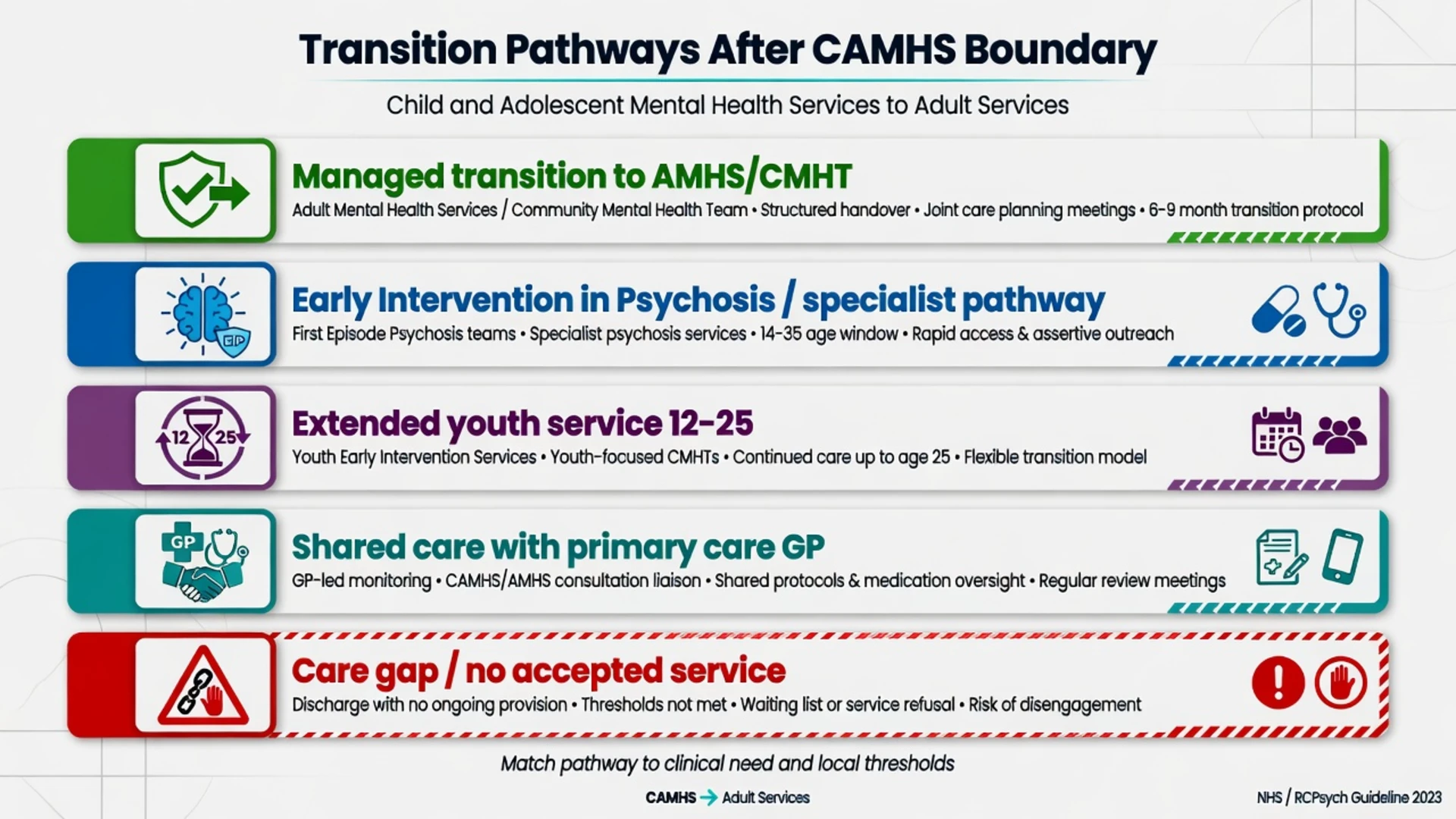
Managed AMHS
- Severe/enduring illness
- Joint meetings + parallel care
- Named adult clinician
Specialist stream
- EIP, ED, adult ADHD/ASD
- Often better continuity if accessed
- Thresholds still apply
Youth 12–25
- McGorry-style redesign
- Removes harmful 18 cut-off
- Availability varies by region
Shared care / GP
- Stable lower-intensity need
- Clear re-referral triggers
- Medication monitoring plan
Care gap
- No accepting service
- Risk of crisis re-entry
- Requires interim cover
TRACK protocol work in Greater London documented variable local protocols and limited standardisation of transition processes even within one metropolitan system — examiners use this to reject assumptions that "policy means practice".[3]
Epidemiology and the size of the gap
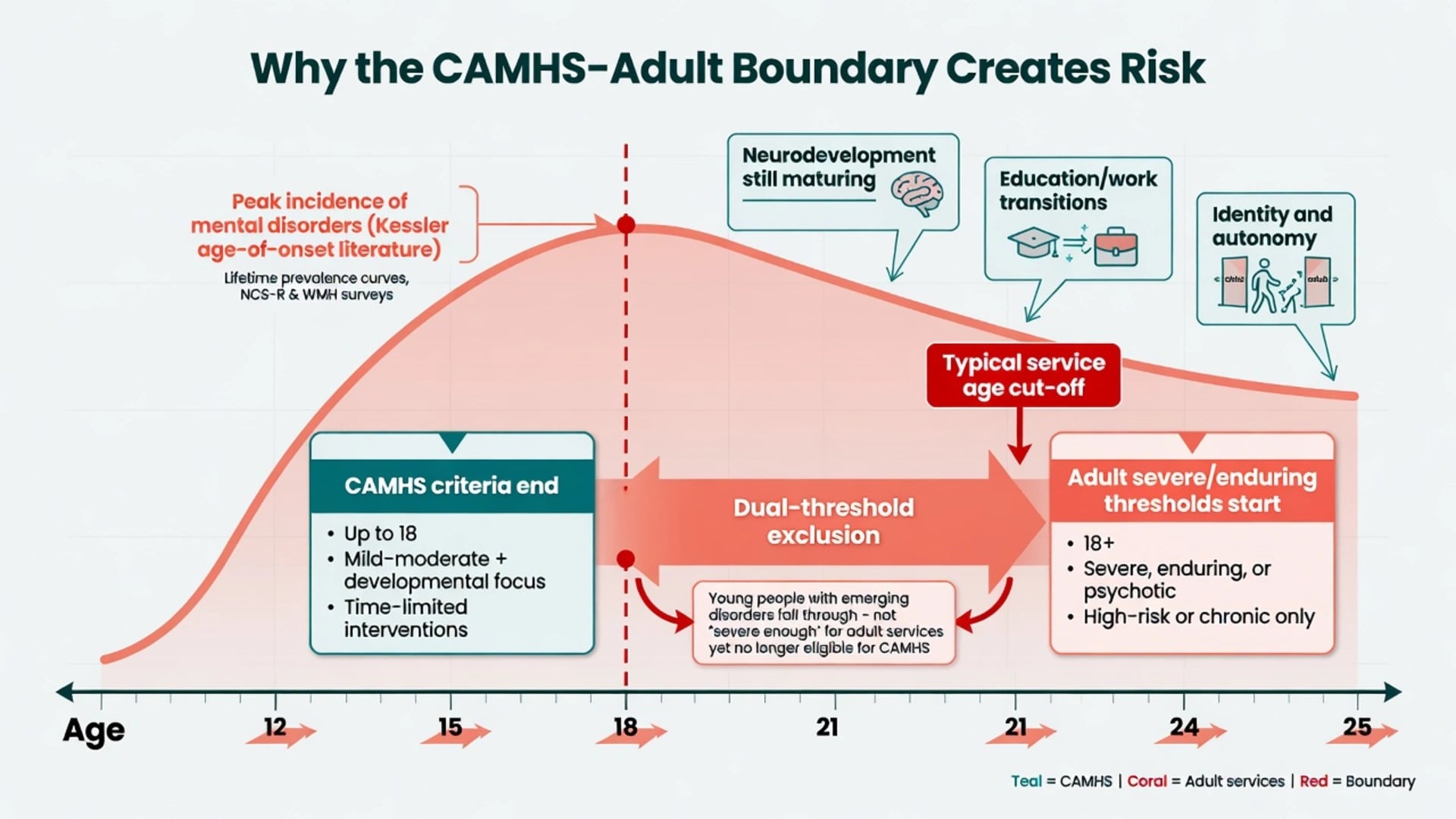
Most lifetime mental disorders have onset in childhood, adolescence, or early adulthood. Kessler and colleagues mapped age-of-onset distributions in the National Comorbidity Survey Replication and subsequent reviews: the peak incidence years straddle typical CAMHS upper age limits.[10][9]
In the TRACK multiperspective study, transition for the vast majority of service users was poorly planned, poorly executed, and poorly experienced.[2] Appleton and colleagues' systematic review of outcomes at the CAMHS boundary found that roughly a quarter of young people transitioned to AMHS, another quarter remained in CAMHS after crossing the boundary age, and outcomes for the remainder were often unknown or discontinuous — the operational definition of falling through the gap for a large group.[7]
TRACK analyses linked AMHS referral likelihood to severe and enduring illness, being on medication, prior Mental Health Act admission, and comorbidity; presentations such as emerging personality disorder and some neurodevelopmental profiles were frequently left without a clean specialist landing zone.[2][4] Islam and colleagues followed young people who failed to make the transition and highlighted adverse service and clinical trajectories after the gap.[6]
Mechanisms — developmental–service mismatch
There is no single neurotransmitter explanation. The mechanism is developmental–service mismatch: peak incidence of serious mental illness collides with an administrative age cut-off, adult entry thresholds that exclude many impairing but non-"severe enduring" presentations, loss of family-inclusive practice, and rupture of therapeutic relationships.[9][2][11]
McGorry and colleagues argue that integrated youth mental health models for approximately ages 12–25 redesign care around developmental epidemiology rather than paediatric versus adult institutional history, reducing the harmful hard stop at 18 for many early intervention populations.[11][12]
Childhood service contact does not automatically inoculate against adult disorder; Copeland and colleagues' analyses of real-world childhood mental health services and later adult psychiatric risk caution against assuming that prior CAMHS involvement equals completed treatment or low future need.[15]
Clinical presentations at the boundary
Expect planned transition clinics and crisis-at-boundary presentations that mirror TRACK multiperspective and outcome literature.[2][6]
Planned: stable ADHD on stimulant with residual organisational impairment; ASD with anxiety needing adult neurodevelopmental mapping; OCD or depression with ongoing therapy needs; bipolar or psychosis in remission still on mood stabiliser/antipsychotic.[2][4]
Crisis-at-boundary: self-harm escalation near 17–18; first-episode psychosis; medical risk in eating disorder; care-leaving youth with placement change and mental health exit on the same calendar; DNAs misfiled as "closed well".[6][7]
Family dynamics: parents describe abrupt "expulsion" from CAMHS; adult services default to young-adult confidentiality; Hovish qualitative work documents multi-perspective distress when process quality is poor.[5]
Differential — need, threshold, and appropriateness
Appropriate step-down
- Sustained recovery
- Primary-care capable
- Clear re-entry triggers
Specialist still needed
- Active risk or complex meds
- Severe enduring illness
- Specialist psychotherapy need
Threshold rejection
- AMHS declines 'not severe'
- No alternative mapped
- Gap by design
False closure
- DNAs = assumed well
- No risk review
- Crisis later in ED
Discriminators: current risk formulation, functional impairment, medication complexity, therapy intensity, housing/care status, and whether an adult pathway actually accepts the presentation — not chronological age alone.[2][7]
Assessment and transition readiness
Start planning early — commonly from mid-teens or at least 6–12 months before the local upper age limit, not at the final session.[1][8][3]
Need and risk map: diagnosis stability; suicide/self-harm/violence risk; substance use; education/work; housing and care status; legal status history; open child-protection issues; carer burden.[2][6]
Transition readiness: illness and medication knowledge; ability to book and attend appointments; crisis plan literacy; digital access; preference for parental involvement.[8][5]
Capacity and consent. Use functional capacity assessment (understand, appreciate, reason/weigh, communicate a choice) for treatment decisions and for information-sharing with parents — Appelbaum framework. Document preferences; apply safeguarding overrides when serious harm risk requires sharing regardless of preference under local law (principle-level; no invented sections).[14]
Written package for the receiving service: formulation, risks, what worked/failed, current meds with doses and monitoring, allergies, rating scales, crisis plan, and named receiving clinician or team with next appointment date.[2][8]
"Investigations" — information and medical baselines
This is not a panel-of-bloods topic. The quality of the information transfer package is the investigation equivalent. Reconfirm diagnoses that may be outdated (especially ADHD, bipolar versus trauma/personality formulations). If psychotropics will continue or restart after a gap, re-establish baseline BP, HR, weight, and ECG when indicated by agent and history; consider pregnancy status and substance use as clinically indicated before re-prescribing stimulants or antipsychotics.[8][2]
Acute management at the boundary
Do not discharge high-risk youth solely because they have reached the CAMHS upper age if adult triage is weeks away and no interim owner exists. ED re-presentation of recent CAMHS leavers should trigger urgent retrieval of prior notes and risk formulation rather than a blank-slate assessment.[6][7]
Definitive management — managed transition
Crowley's systematic review of transitional care programmes across chronic conditions (including mental health populations in the broader literature) supports structured programmes over ad hoc transfer, while noting limited high-quality trial evidence historically.[8] TRACK multiperspective and qualitative work define the lived components of good process: planning, joint working, information continuity, and young-person involvement.[2][5]
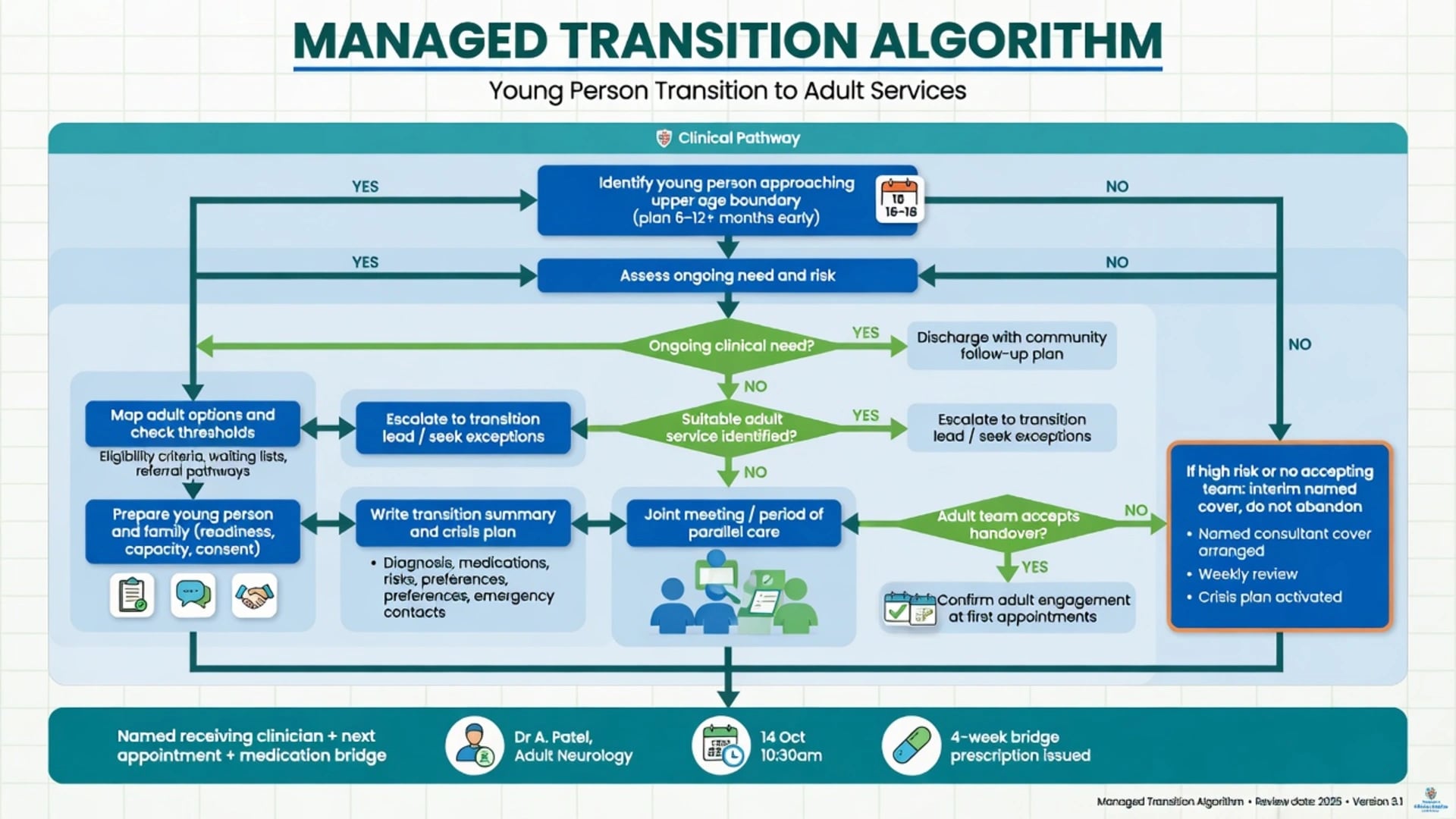
Core managed-transition bundle (exam checklist) drawn from TRACK process findings and transitional care reviews:[2][8]
- Early identification of boundary-approaching open cases.[3][8]
- Need-based pathway mapping (AMHS CMHT, EIP, eating disorders, adult ADHD/neurodevelopmental, personality-disorder psychological pathway, primary care shared care, NGO/youth service).[4][11]
- Young-person-led preparation with negotiated family role.[5][14]
- Written transition plan and clinical summary.[2][8]
- Joint meeting and period of parallel care where possible.[2][4]
- Named transition coordinator / receiving clinician and booked first adult appointment.[2][8]
- Medication bridge — never end effective treatment solely for administrative age reasons without adult prescribing cover.[2][6]
- Follow-through audit of engagement at first adult contacts.[7][13]
The MILESTONE randomised clinical trial evaluated managed transition at the child–adult mental health boundary (including structured transition readiness tools and processes) for mental health outcomes — cite it as the major modern experimental attempt to improve boundary care beyond observational TRACK work.[13]
Medication continuity examples (agent-level principles, not universal recipes): if a young person remains on long-acting methylphenidate or atomoxetine for ADHD, or on an SSRI such as fluoxetine or sertraline for ongoing major depression/anxiety with residual symptoms, arrange the adult or shared-care prescriber before the final CAMHS supply runs out; document dose, formulation, monitoring (BP/HR/growth history for stimulants; review mood, suicidality, sexual side-effects, and adherence for SSRIs), and next review date. Cite nearby clinical process evidence rather than inventing mandatory national dose schedules.[2][8]
Subtypes and high-yield scenarios
ADHD and neurodevelopmental conditions. Adult ADHD and ASD pathways are uneven; many youth lose stimulant treatment and occupational supports. Map shared care early.[7][11]
Early psychosis. EIP models often intentionally span youth and early adulthood — use them when criteria are met to avoid the general CMHT threshold trap.[11][12]
Eating disorders. Medical risk can rise if specialist input stops at a weight-restored but still psychologically fragile phase coinciding with age cut-off.[7]
Emerging personality disorder and complex trauma. TRACK highlighted this group as vulnerable to falling between services; map evidence-informed psychological pathways rather than pure rejection letters.[2][4]
Looked-after and care-leaving youth. Dual exits (care system and mental health) multiply discontinuity; joint multi-agency planning is mandatory in principle.[6][5]
Intellectual disability / autism with dual diagnosis. Adult ID or neurodevelopmental teams may use different thresholds and communication styles; prepare accommodations in the written plan.[11]
Complications and pitfalls
- Planning only at the last appointment.[2]
- Assuming adult acceptance without checking thresholds.[3][7]
- Stopping medication at discharge without adult cover.[6]
- Equating DNA with recovery.[6][7]
- Inventing NICE NG43 clause numbers or local policy sections under exam pressure — state process principles (early planning, named coordinator, information continuity, young-person involvement) instead.[8][1]
- Ignoring capacity and information-sharing preferences.[14]
- Culturally unsafe adult placements for Indigenous and CALD youth driving disengagement.[11][12]
Prognosis and disposition
Poorly managed transition associates with disengagement and crisis re-entry; structured managed processes aim to improve continuity and experience, with MILESTONE adding randomised evaluation of managed transition packages.[2][6][13] Disposition must name the receiving owner, next appointment, medication bridge, crisis contacts, and who will notice non-engagement. Audit markers used in literature and service improvement include proportion referred, accepted, and still engaged at follow-up windows.[7][13]
Special populations and regional models
Youth mental health redesign (including headspace-style enhanced primary care for adolescents and young adults) and state/territory CAMHS age policies are examinable at principle level. Use McGorry service design arguments for 12–25 models alongside local public AMHS thresholds. Do not invent state protocol numbers; describe early planning, shared care with GPs, and specialist streams (EIP, eating disorders).[11][12]
Evidence and guidelines (exam anchors)
| Anchor | Why examiners care |
|---|---|
| Blum 1993 | Canonical definition of transition as planned process |
| TRACK 2008–2016 programme | Protocols, multiperspective outcomes, qualitative experience, failed-transition follow-up |
| Appleton 2019 SR | ~1/4 to AMHS synthesis |
| Crowley 2011 SR | Broader transitional care programme evidence |
| Kessler age-of-onset | Why the boundary is epidemiologically absurd |
| McGorry 2013/2022 | Youth service redesign alternative |
| MILESTONE RCT 2023 | Managed transition experimental evaluation |
| Appelbaum 2007 | Capacity at the adult-style consent interface |
Exam pearls
BRIDGE (managed transition)
Fellowship answers name the local pathway in principles, protect high-risk youth with interim cover, involve the young person as decision-maker under capacity law, and treat transition as a clinical intervention rather than clerical discharge.[1][2][13][14]
References
- [1]Blum RW, Garell D, Hodgman CH, et al. Transition from child-centered to adult health-care systems for adolescents with chronic conditions. A position paper of the Society for Adolescent Medicine J Adolesc Health, 1993.PMID 8312295
- [2]Singh SP, Paul M, Ford T, et al. Process, outcome and experience of transition from child to adult mental healthcare: multiperspective study Br J Psychiatry, 2010.PMID 20884954
- [3]Singh SP, Paul M, Ford T, Kramer T, Weaver T Transitions of care from Child and Adolescent Mental Health Services to Adult Mental Health Services (TRACK Study): a study of protocols in Greater London BMC Health Serv Res, 2008.PMID 18573214
- [4]Paul M, Ford T, Kramer T, Islam Z, Harley K, Singh SP Transfers and transitions between child and adult mental health services Br J Psychiatry Suppl, 2013.PMID 23288500
- [5]Hovish K, Weaver T, Islam Z, Paul M, Singh SP Transition experiences of mental health service users, parents, and professionals in the United Kingdom: a qualitative study Psychiatr Rehabil J, 2012.PMID 22246124
- [6]Islam Z, Ford T, Kramer T, et al. Mind how you cross the gap! Outcomes for young people who failed to make the transition from child to adult services: the TRACK study BJPsych Bull, 2016.PMID 27280035
- [7]Appleton R, Connell C, Fairclough E, Tuomainen H, Singh SP Outcomes of young people who reach the transition boundary of child and adolescent mental health services: a systematic review Eur Child Adolesc Psychiatry, 2019.PMID 30850925
- [8]Crowley R, Wolfe I, Lock K, McKee M Improving the transition between paediatric and adult healthcare: a systematic review Arch Dis Child, 2011.PMID 21388969
- [9]Kessler RC, Amminger GP, Aguilar-Gaxiola S, Alonso J, Lee S, Ustün TB Age of onset of mental disorders: a review of recent literature Curr Opin Psychiatry, 2007.PMID 17551351
- [10]Kessler RC, Berglund P, Demler O, Jin R, Merikangas KR, Walters EE Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication Arch Gen Psychiatry, 2005.PMID 15939837
- [11]McGorry P, Bates T, Birchwood M Designing youth mental health services for the 21st century: examples from Australia, Ireland and the UK Br J Psychiatry Suppl, 2013.PMID 23288499
- [12]McGorry PD, Mei C, Chanen A, Hodges C, Alvarez-Jimenez M, Killackey E Designing and scaling up integrated youth mental health care World Psychiatry, 2022.PMID 35015367
- [13]Singh SP, Tuomainen H, Bouliotis G, et al. Effect of managed transition on mental health outcomes for young people at the child-adult mental health service boundary: a randomised clinical trial Psychol Med, 2023.PMID 37310306
- [14]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [15]Copeland WE, Tong G, Shanahan L Do "Real World" Childhood Mental Health Services Reduce Risk for Adult Psychiatric Disorders? J Am Acad Child Adolesc Psychiatry, 2022.PMID 35063586