Psych · Child and adolescent psychiatry — youth self-harm and suicide
Youth self-harm and suicide
Also known as Adolescent self-harm · Adolescent suicide · Youth NSSI · CAMHS self-harm · Paediatric suicide risk · Child adolescent deliberate self-harm · Teen suicide attempt · Youth safety planning
Exam-exhaustive fellowship reference on youth (child and adolescent) self-harm and suicide — epidemiology, developmental risk and protective factors, NSSI vs suicide attempt on the intent continuum, psychosocial assessment with private youth interview plus family and school interfaces, Gillick/developmental competence and confidentiality limits, safety planning and means restriction without graphic methods, CAMHS disposition pathways, DBT-A and family intervention evidence, antidepressant monitoring context, and non-stigmatising language. Distinct from adult suicide-risk-assessment and adult self-harm-and-crisis-intervention topics. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
12 MCQs with explanations
Target exams
Red flags
Overview and definition
Youth self-harm and suicide is a core child and adolescent psychiatry and emergency/CAMHS skillset: clarifying intent, understanding developmental context, treating medical need first, completing structured psychosocial assessment with young person and carers, and implementing safety planning, family work, school interface, and stepped aftercare.[1][2][3]
This topic is related to but distinct from adult suicide-risk-assessment (ideation-to-action models, lithium/clozapine anti-suicide pharmacology) and adult self-harm-and-crisis-intervention (general hospital self-harm pathway). Here the centre of gravity is developmental, family, school, Gillick/developmental competence, safeguarding, and CAMHS disposition.[1][8]
Language is clinical and ethical. Prefer self-harm, suicide attempt, NSSI, and died by suicide. Avoid pejorative labels (attention-seeking, manipulative, committed suicide). Asking about suicide does not create risk in screened youth populations; silence and stigma impair engagement.[25][3]
| Term | Working meaning in youth services |
|---|---|
| Self-harm (service/research sense) | Intentional self-poisoning or self-injury irrespective of suicidal intent |
| NSSI | Self-injury without intent to die; often affect regulation in adolescents |
| Suicide attempt | Self-injurious behaviour with at least some intent to die |
| Mixed / unclear intent | Ambivalence common in youth — document both poles |
| Youth / child-adolescent | Service-defined; many hospital cohorts use under-18; developmental stage matters more than a single age cut-off |
Classification — intent continuum
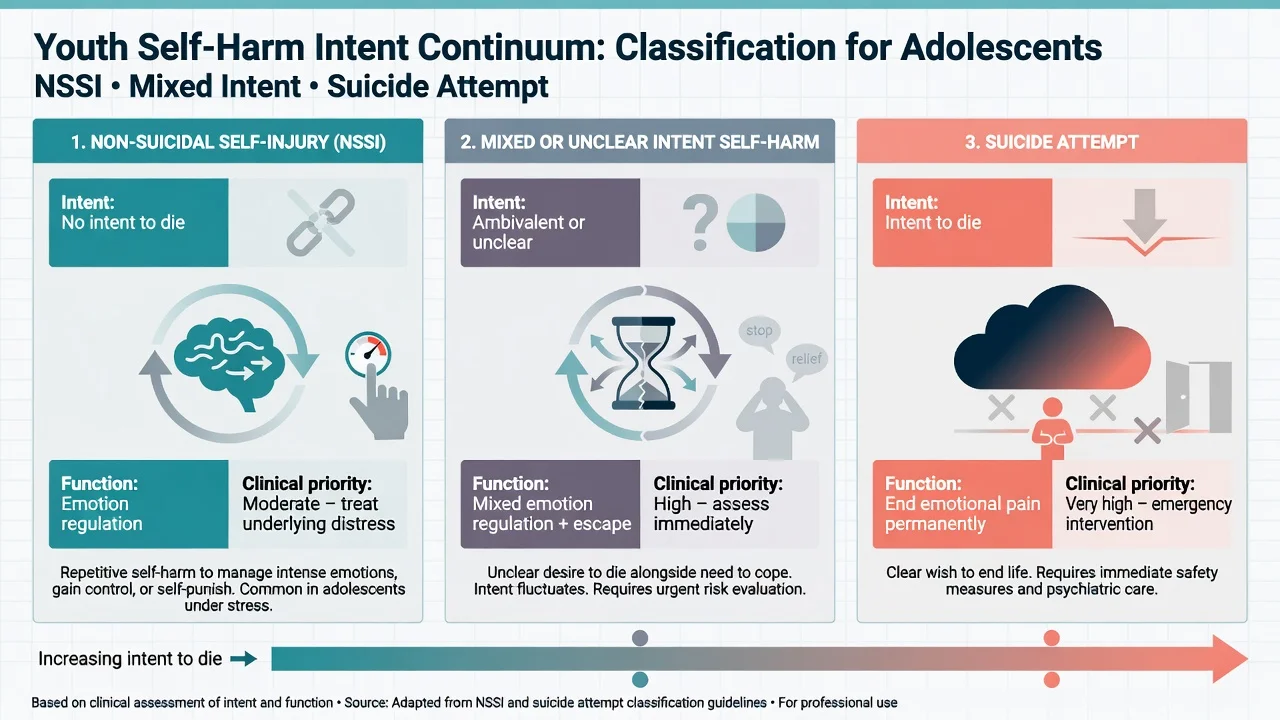
NSSI is typically used to reduce aversive affect, generate feeling when numb, self-punish, or influence a relational context — not to die. Suicide attempts include at least partial intent to die. Young people commonly move between categories over months; chronic NSSI elevates lifetime suicide attempt risk and must not be dismissed as trivial.[6][7]
DSM-5-TR places NSSI as a condition for further study. ICD-11 and service datasets often code intentional self-harm behaviourally. Fellowship answers state the divergence rather than forcing one taxonomy onto every presentation.[1][4]
- No intent to die
- Affect regulation common
- Often repeated pattern
- Still full assessment
- May coexist with SI
- Ambivalence about dying
- Partial suicidal thoughts
- Common after interpersonal crisis
- Document both poles
- Treat highest credible risk
- Some intent to die
- Impulsive or planned
- Expectation of death matters
- Peak near-term risk window
- Safety plan + disposition
Epidemiology and risk factors
Community NSSI is common in adolescents and young adults; population surveys show substantial non-suicidal self-harm with incomplete service contact.[4][5] Non-fatal self-harm presentations are often over-represented among adolescent females in hospital datasets, whereas suicide deaths show different sex patterns that rise through mid-to-late adolescence — examiners test both facts without collapsing them.[1][2]
After hospital-treated self-harm, repetition is common and suicide and premature mortality risk remain elevated. Multicentre English data on children and adolescents show important later mortality after non-fatal self-harm — youth self-harm is a serious risk marker, not a benign rite of passage.[8][10][11]
Risk factors cluster as prior self-harm/NSSI, depression and anxiety, hopelessness, trauma and adverse childhood experiences, bullying (including online), LGBTQ+ minority stress, substance use, family conflict and parental mental illness, sleep disruption, impulsivity/ADHD traits, social isolation, and life problems across home, school, and peers.[6][9][16] Protective factors include connectedness (family, school, peers), help-seeking skills, reasons for living, cultural belonging, and access to responsive care.[1][2]
Fifty years of risk-factor research shows modest predictive power for individual suicidal outcomes; crude high/low stratification is not a crystal ball. Formulation of dynamic risk, needs, and safety resources drives disposition.[15][16]
Pathophysiology and developmental mechanisms
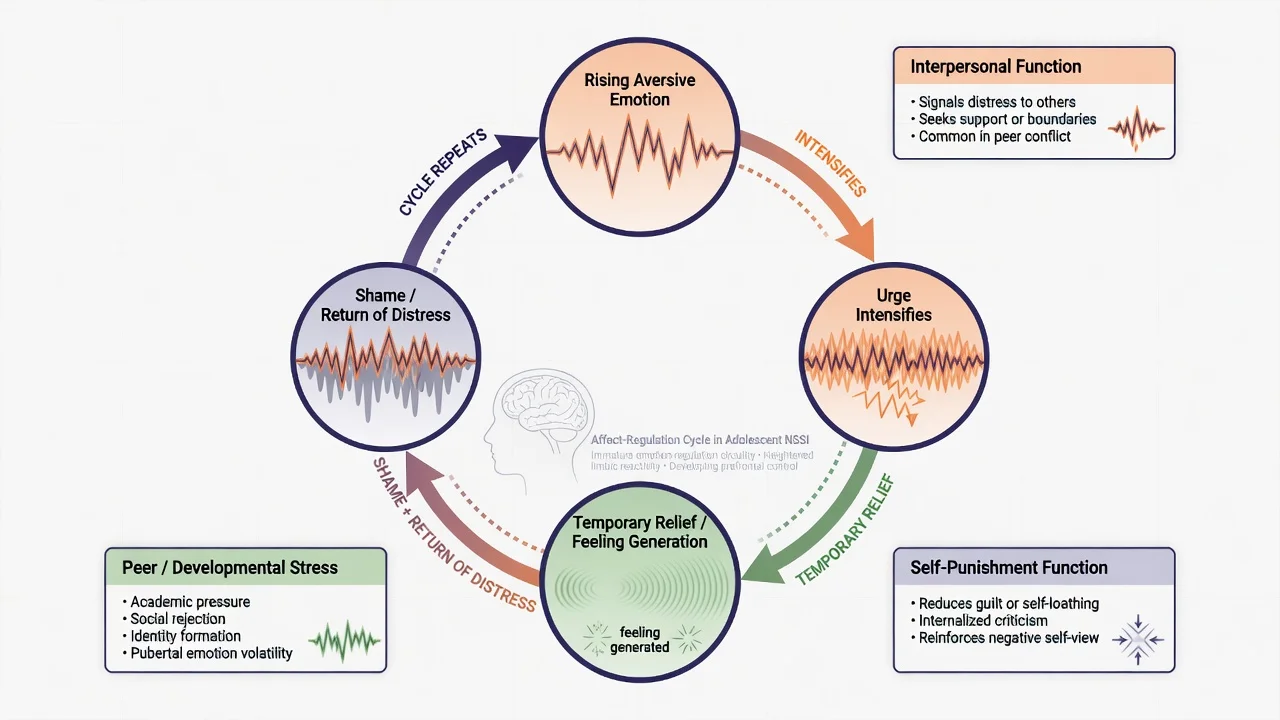
The dominant psychological model for NSSI is affect regulation: aversive emotion rises, urge intensifies, the act produces temporary relief or feeling generation, then shame and return of distress sustain the cycle.[7] Developmental context matters — adolescent reward/peer sensitivity, incomplete emotion-regulation skills, sleep disruption, and high interpersonal stakes amplify crisis intensity.[1][2]
Where suicidal intent is present, stress-diathesis and ideation-to-action ideas apply with youth-specific amplifiers: impulsivity, acute interpersonal loss or humiliation, intoxication, and limited future orientation in the moment.[3][16] Substance use increases transition risk from ideation or chronic NSSI to more dangerous acts in a single night.[1][3]
Clinical presentation
Presentations include ED after self-poisoning or self-injury, medical ward liaison, CAMHS crisis, GP or school counsellor disclosure, parent discovery of injuries or messages, and youth justice/out-of-home-care settings.[2][9]
MSE themes: shame, minimisation after survival, relief versus disappointment, intoxication, dissociation after NSSI, hopelessness, fluctuating intent within one interview, and fear of parental reaction. Atypical patterns examiners probe: pre-adolescent self-harm; autistic youth with sensory/communication overlays; cultural idioms of distress; high-lethality intent minimised as "accident"; LGBTQ+ youth with minority stress and family rejection.[1][2]
Differential diagnosis
Discriminators matter more than lists. NSSI vs suicide attempt vs mixed intent — ask expected outcome and wish to die; do not infer intent from method alone.[7][14] Body-focused repetitive behaviours and self-injury in intellectual disability or autism need functional analysis (sensory, communication, environment) distinct from affect-regulation NSSI.[1] Organic drivers: intoxication/withdrawal, medical toxicity, delirium, severe pain, akathisia from medication.[3] Primary mood, psychosis, PTSD, eating disorder, emerging personality pathology as treatable drivers — not excuses to skip risk work.[2][6] Avoid pejorative "attention-seeking" as a default formulation — it fails CASC standards and blocks alliance.[1]
Clinical and bedside assessment
Process principles (exam gold)
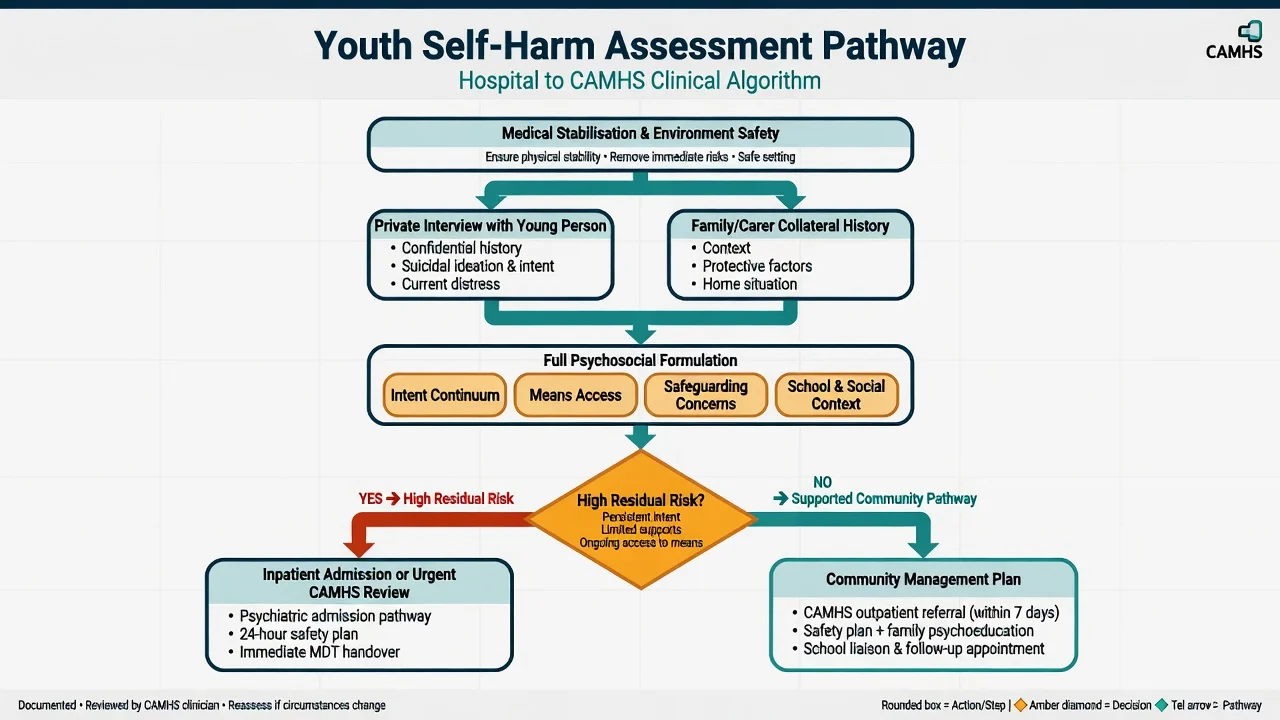
NICE-style process standards that transfer to ANZ CAMHS practice culture include: compassion and non-stigmatising care from first contact; medical assessment and treatment first when needed; offer psychosocial assessment to everyone presenting with self-harm; assess needs, risks, and social context; involve family/carers when safe; provide information, safety planning, and booked aftercare. Psychosocial assessment is an intervention, not optional paperwork — associated with better process outcomes in hospital self-harm cohorts.[12][13]
Private interview, family, and confidentiality
Always attempt a private interview with the young person (without parents in the room for part of the assessment), then a family session. Explain confidentiality limits up front: information is private unless safety, safeguarding, or legal duties require sharing. Developmental competence / Gillick-type concepts (jurisdiction-specific) inform consent and information-sharing — do not invent statute numbers across countries; state the principle and apply local law.[1][2]
Structured episode history
Cover precipitants (interpersonal conflict, bullying/online harms, exams, trauma reminders, substances, identity-related stress); intent continuum at the time and now; planning versus impulsivity; alcohol and other substances; past self-harm chronology and functions of NSSI; means access at home (medications and other hazards — clinically necessary detail only, no graphic method coaching); protective factors and reasons for living; full MSE with quoted content; safeguarding screen; school engagement; and collateral from carers, school (with consent/safety framing), GP, and prior CAMHS notes.[7][9][14]
C-SSRS concepts can structure ideation severity and behaviour enquiry in adolescents and adults; they do not replace formulation or guarantee prediction.[14][15]
Investigations
Investigations follow the medical presentation: observations, ECG when cardiotoxic overdose is possible, paracetamol and other levels as indicated by local toxicology protocols, metabolic bloods, pregnancy test when relevant. Toxicology screens have false negatives and do not replace history.[3] Organic red flags (fever, fluctuating consciousness, focal neurology) trigger broader medical work-up. Depression/anxiety scales and functional NSSI checklists are adjuncts — not discharge tickets.[15]
Management — immediate (crisis)
Immediate priorities: ABC and medical care; environment safety and proportionate observation; treat pain, withdrawal, and severe agitation; engage with calm, validating, non-stigmatising language; do not use no-suicide contracts; begin collaborative means restriction with carers; if risk is high and the young person lacks capacity for necessary care, use least restrictive legal pathways under jurisdiction-specific child/adolescent mental health law.[3][17]
Management — definitive and stepwise
Safety planning (youth-adapted Stanley-Brown)
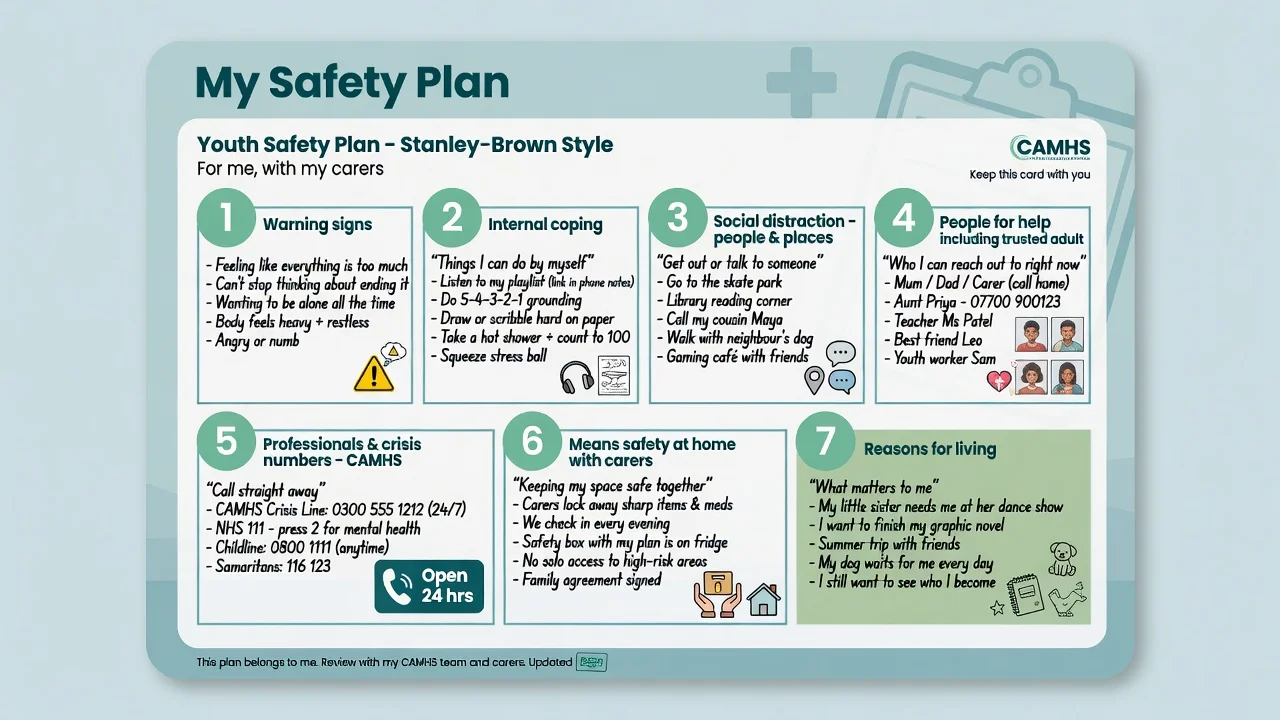
The Safety Planning Intervention with structured follow-up reduced suicidal behaviour versus usual ED care in a large RCT of suicidal ED patients — adapt for youth by naming trusted adults, school-day coping, CAMHS crisis numbers, and carer roles in means safety. The young person keeps a written copy.[17] For NSSI-dominant presentations, add urge management and function-matched skills while still screening suicidal intent each contact.[7][20]
Means restriction
Collaborative, respectful restriction of accessible means at home (excess medication storage/disposal with carers; other environmental hazards relevant to the case) is core crisis work. Avoid graphic method coaching; document only what is clinically necessary.[3][17]
Structured psychological therapies (youth evidence)
- DBT for adolescents (DBT-A): Mehlum et al. showed reduced self-harm versus enhanced usual care in a randomised trial of adolescents with repeated suicidal and self-harming behaviour, with sustained signals at longer follow-up analyses.[18][19] Meta-analytic synthesis supports DBT-A effects on adolescent self-harm and suicidal ideation with heterogeneity across studies.[20]
- Therapeutic interventions overall: Ougrin meta-analysis found therapeutic interventions superior to control conditions on average for adolescent self-harm/suicide attempts; engagement and treatment components matter.[21]
- Cochrane (Witt) children/adolescents: structured psychosocial interventions have the best evidence base among psychological options, with moderate and heterogeneous effects — not a single universal protocol.[22]
- Systemic family therapy (SHIFT): pragmatic multicentre RCT versus treatment as usual after self-harm — primary outcome mixed/null at main endpoint; still examinable as a major family-therapy trial with implementation lessons (family engagement, not "family therapy for all").[23]
- SAFETY program: cognitive-behavioural family treatment-development trial for adolescent suicide attempters — model for integrated youth-family CBT safety work.[24]
- Common elements across effective youth treatments include emotion regulation, problem-solving, family communication, safety planning, and treatment engagement (Ougrin practitioner review).[28]
Pharmacotherapy context in youth
Treat underlying disorders (depression, anxiety, ADHD, psychosis) when indicated. There is no single "anti-NSSI tablet". Network meta-analysis of new-generation antidepressants in children and adolescents informs efficacy/tolerability discussions; monitor mood, agitation, and emergence of suicidal ideation after starting or changing antidepressants, especially early in treatment — do not withhold indicated treatment from fear alone, and do not use medication as a substitute for psychosocial safety planning.[27][1]
Brief contact and aftercare culture
Planned non-demanding contact and rapid booked follow-up sit within a broader aftercare culture (adult postcard/BIC literature informs principle even when youth-specific trials differ). Never discharge to an empty plan.[12][17]
School interface and family work
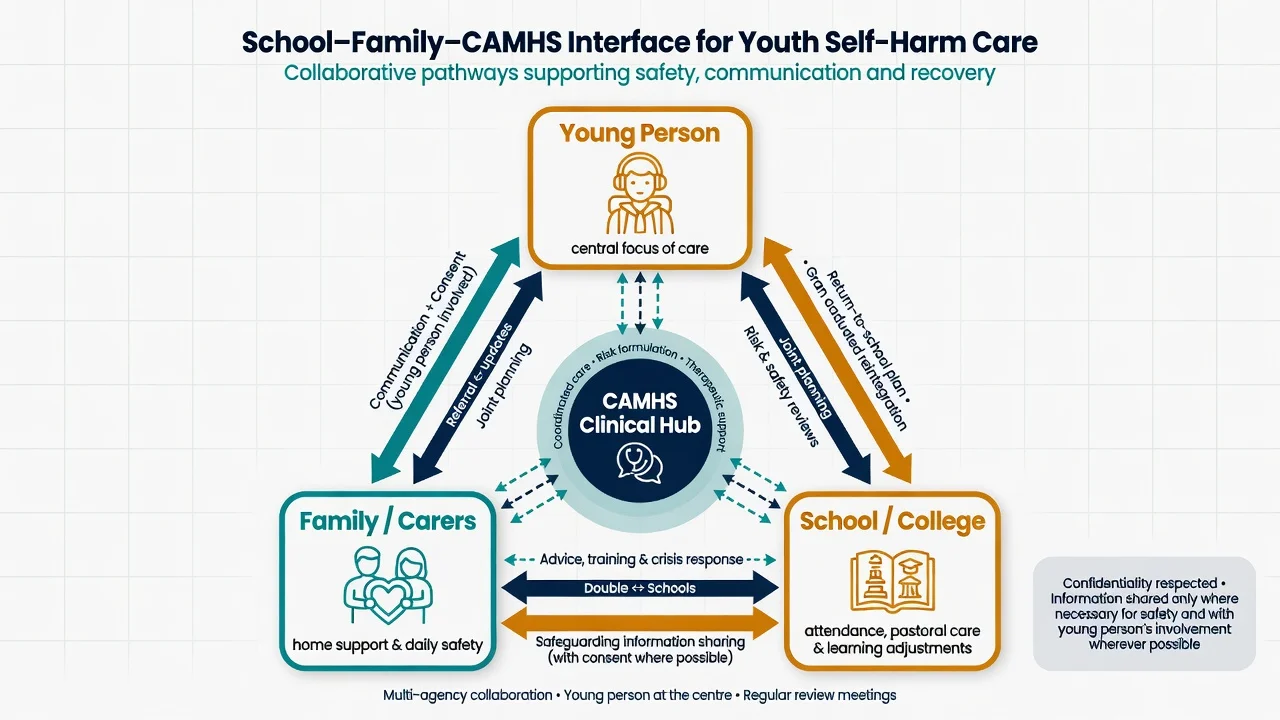
School is both a risk context (bullying, exam stress, peer contagion concerns) and a protective setting (connectedness, monitoring, return-to-school plans). Negotiate information-sharing carefully: partial disclosure may be required for safety; absolute secrecy is not promised when risk is high.[1][9][26]
School-based prevention evidence includes the SEYLE cluster RCT of school suicide-prevention programmes in Europe — examiners may ask about universal mental-health awareness approaches versus screening; Gould showed that asking about suicide in school screening did not increase distress or suicidal ideation versus control.[25][26]
Family work addresses conflict, expressed emotion, supervision of means, and alliance against pejorative labels. Validate parental fear without endorsing "attention-seeking" framing in front of the young person.[23][24]
Specific subtypes and scenarios
| Scenario | Emphasis |
|---|---|
| First hospital presentation, mixed intent | Medical care; full psychosocial assessment; safety plan; urgent CAMHS |
| Chronic NSSI, no current SI | Function analysis; skills pathway (often DBT-A); still screen SI |
| Escalating NSSI with emerging SI | Reformulate; increase intensity; means restriction with carers |
| Clear suicide attempt | Peak near-term risk; observation; low threshold for intensive care |
| School disclosure / bullying | School safety plan; anti-bullying pathways; partial info-sharing |
| LGBTQ+ minority stress | Affirming stance; family rejection assessment; community supports |
| Autistic / neurodivergent youth | Communication adaptations; sensory/functional analysis; carer coaching |
| Looked-after / out-of-home care | Multi-agency; placement stability; safeguarding |
| Frequent ED attendance | Shared formulation; crisis plan with ED; structured therapy pathway |
| Cultural minority / Indigenous youth | Cultural safety, community supports, interpreter, trauma-informed care |
Complications and pitfalls
- Dismissing youth self-harm as "attention-seeking" or "just drama"
- Interviewing only parents; skipping private youth interview
- Promising absolute confidentiality when safety requires disclosure
- No-suicide contracts; empty discharge; no means work with carers
- Graphic method discussion that teaches technique
- Missing safeguarding (abuse, exploitation, domestic violence)
- Scale-only decisions without developmental formulation
- Ignoring school, online harms, or peer context
- Withholding indicated antidepressants purely from black-box anxiety without monitoring plan
Prognosis and disposition
Hospital-treated self-harm in children and adolescents associates with elevated later mortality risk — disposition must respect that seriousness even when the current act looks "superficial".[8][11]
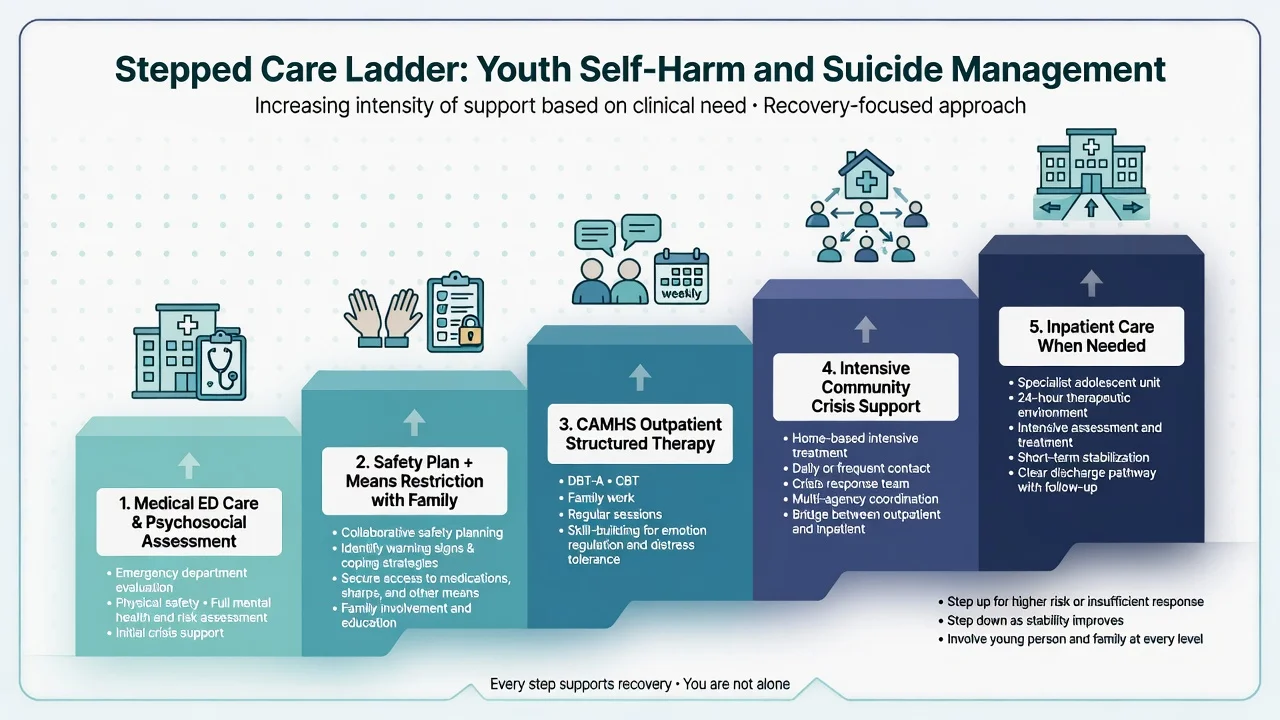
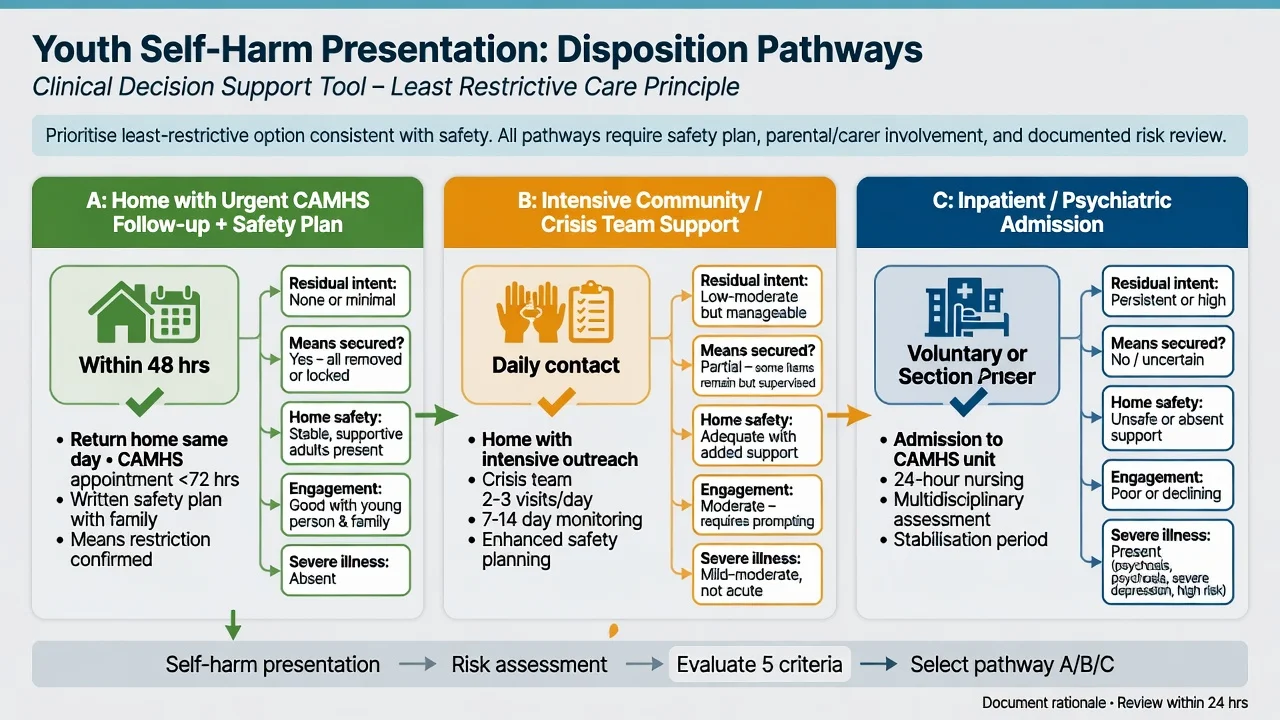
Disposition ladder (least restrictive safe option): match intensity to residual dynamic risk after hospital-treated self-harm.[8][12][17]
- Home with urgent CAMHS follow-up — engageable young person, carers able to supervise means and safety plan, residual risk manageable, booked rapid review (hours to a few days, not weeks-only).[8][17]
- Intensive community / crisis team — higher dynamic risk, need for frequent contact, partial home safety, or complex family work.[12][17]
- Inpatient — residual high intent, unsecured means, unsafe or rejecting home, inability to engage, severe psychiatric illness, or safeguarding that precludes safe community care.[8][12]
Legal status follows jurisdiction-specific child/adolescent mental health law — name the principle of least restriction and local application; do not invent section numbers for all countries.[1][12]
Special populations
Pre-adolescent children need developmentally adapted interviews, strong safeguarding focus, and careful interpretation of intent language.[2] LGBTQ+ youth face elevated suicide-related outcomes in many datasets — assess minority stress, family acceptance, and bullying without pathologising identity.[1] Neurodevelopmental disorders require communication adaptations and functional analysis of self-injury.[1] Indigenous and culturally diverse youth need culturally safe engagement and community supports.[1] Youth in care / justice need multi-agency plans and placement stability work.[9] Co-occurring substance use is both a risk amplifier and a treatment target.[3]
Evidence, guidelines, and regional differences
Landmark named evidence for viva: Hawton 2020 youth mortality after self-harm;[8] Mehlum DBT-A RCT and follow-up;[18][19] Ougrin adolescent therapy meta-analysis;[21] Witt Cochrane children/adolescents;[22] SHIFT family therapy pragmatic RCT;[23] SAFETY family CBT development trial;[24] Stanley SPI RCT;[17] Gould screening safety RCT;[25] SEYLE school prevention cluster RCT;[26] Franklin risk-factor meta-analysis;[16] Large critique of crude risk stratification.[15]
RANZCP and local CAMHS operational policies emphasise least-restrictive care, family-inclusive practice, cultural safety (including Aboriginal and Torres Strait Islander and Māori frameworks as applicable), and clear crisis pathways. Exact admission criteria and legal instruments are state/territory or national — quote local policy in clinical work; in exams state principles and flag jurisdiction. Core process evidence still includes psychosocial assessment and structured aftercare after self-harm.[12][13][17]
Exam pearls
YOUTHSAFE
Self-test: what makes youth different from adult self-harm viva?
Answer anchors: developmental competence and confidentiality limits; mandatory private interview plus family; school interface; safeguarding thresholds; CAMHS disposition ladder; DBT-A/SHIFT/SAFETY evidence names; non-stigmatising language with angry parents; Hawton 2020 mortality data for children/adolescents; no graphic methods.[8][18][23][25]
References
- [1]Cha CB, Franz PJ, M Guzmán E, et al. Annual Research Review: Suicide among youth - epidemiology, (potential) etiology, and treatment J Child Psychol Psychiatry, 2018.PMID 29090457
- [2]Bridge JA, Goldstein TR, Brent DA Adolescent suicide and suicidal behavior J Child Psychol Psychiatry, 2006.PMID 16492264
- [3]Turecki G, Brent DA Suicide and suicidal behaviour Lancet, 2016.PMID 26385066
- [4]Swannell SV, Martin GE, Page A, et al. Prevalence of nonsuicidal self-injury in nonclinical samples: systematic review, meta-analysis and meta-regression Suicide Life Threat Behav, 2014.PMID 24422986
- [5]McManus S, Gunnell D, Cooper C, et al. Prevalence of non-suicidal self-harm and service contact in England, 2000-14: repeated cross-sectional surveys of the general population Lancet Psychiatry, 2019.PMID 31175059
- [6]Fox KR, Franklin JC, Ribeiro JD, et al. Meta-analysis of risk factors for nonsuicidal self-injury Clin Psychol Rev, 2015.PMID 26416295
- [7]Klonsky ED The functions of deliberate self-injury: a review of the evidence Clin Psychol Rev, 2007.PMID 17014942
- [8]Hawton K, Bale L, Brand F, et al. Mortality in children and adolescents following presentation to hospital after non-fatal self-harm in the Multicentre Study of Self-harm: a prospective observational cohort study Lancet Child Adolesc Health, 2020.PMID 31926769
- [9]Townsend E, Ness J, Waters K, et al. Life problems in children and adolescents who self-harm: findings from the multicentre study of self-harm in England Child Adolesc Ment Health, 2022.PMID 35042280
- [10]Owens D, Horrocks J, House A Fatal and non-fatal repetition of self-harm. Systematic review Br J Psychiatry, 2002.PMID 12204922
- [11]Geulayov G, Casey D, Bale L, et al. Suicide following presentation to hospital for non-fatal self-harm in the Multicentre Study of Self-harm: a long-term follow-up study Lancet Psychiatry, 2019.PMID 31706930
- [12]Kapur N, Steeg S, Turnbull P, et al. Hospital management of suicidal behaviour and subsequent mortality: a prospective cohort study Lancet Psychiatry, 2015.PMID 26254717
- [13]Kapur N, Murphy E, Cooper J, et al. Psychosocial assessment following self-harm: results from the multi-centre monitoring of self-harm project J Affect Disord, 2008.PMID 17761308
- [14]Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults Am J Psychiatry, 2011.PMID 22193671
- [15]Large MM, Ryan CJ, Carter G, et al. Can we usefully stratify patients according to suicide risk? BMJ, 2017.PMID 29042363
- [16]Franklin JC, Ribeiro JD, Fox KR, et al. Risk factors for suicidal thoughts and behaviors: A meta-analysis of 50 years of research Psychol Bull, 2017.PMID 27841450
- [17]Stanley B, Brown GK, Brenner LA, et al. Comparison of the Safety Planning Intervention With Follow-up vs Usual Care of Suicidal Patients Treated in the Emergency Department JAMA Psychiatry, 2018.PMID 29998307
- [18]Mehlum L, Tørmoen AJ, Ramberg M, et al. Dialectical behavior therapy for adolescents with repeated suicidal and self-harming behavior: a randomized trial J Am Acad Child Adolesc Psychiatry, 2014.PMID 25245352
- [19]Mehlum L, Ramberg M, Tørmoen AJ, et al. Dialectical Behavior Therapy Compared With Enhanced Usual Care for Adolescents With Repeated Suicidal and Self-Harming Behavior: Outcomes Over a One-Year Follow-Up J Am Acad Child Adolesc Psychiatry, 2016.PMID 27015720
- [20]Kothgassner OD, Goreis A, Robinson K, et al. Efficacy of dialectical behavior therapy for adolescent self-harm and suicidal ideation: a systematic review and meta-analysis Eur Child Adolesc Psychiatry, 2021.PMID 33875025
- [21]Ougrin D, Tranah T, Stahl D, et al. Therapeutic interventions for suicide attempts and self-harm in adolescents: systematic review and meta-analysis J Am Acad Child Adolesc Psychiatry, 2015.PMID 25617250
- [22]Witt KG, Hetrick SE, Rajaram G, et al. Interventions for self-harm in children and adolescents Cochrane Database Syst Rev, 2021.PMID 33677832
- [23]Cottrell DJ, Wright-Hughes A, Collinson M, et al. Effectiveness of systemic family therapy versus treatment as usual for young people after self-harm: a pragmatic, phase 3, multicentre, randomised controlled trial Lancet Psychiatry, 2018.PMID 29449180
- [24]Asarnow JR, Berk M, Hughes JL, et al. The SAFETY Program: a treatment-development trial of a cognitive-behavioral family treatment for adolescent suicide attempters J Clin Child Adolesc Psychol, 2015.PMID 25255931
- [25]Gould MS, Marrocco FA, Kleinman M, et al. Evaluating iatrogenic risk of youth suicide screening programs: a randomized controlled trial JAMA, 2005.PMID 15811983
- [26]Wasserman D, Hoven CW, Wasserman C, et al. School-based suicide prevention programmes: the SEYLE cluster-randomised, controlled trial Lancet, 2015.PMID 25579833
- [27]Hetrick SE, McKenzie JE, Bailey AP, et al. New generation antidepressants for depression in children and adolescents: a network meta-analysis Cochrane Database Syst Rev, 2021.PMID 34029378
- [28]Meza JI, Zullo L, Vargas SM, Ougrin D, et al. Practitioner Review: Common elements in treatments for youth suicide attempts and self-harm - a practitioner review based on review of treatment elements associated with better outcomes J Child Psychol Psychiatry, 2023.PMID 36878853