Psych · Consultation-liaison psychiatry
Autoimmune encephalitis and organic psychosis
Also known as Anti-NMDA receptor encephalitis · NMDAR encephalitis · Autoimmune psychosis · Antibody-mediated encephalitis · Organic psychosis · Secondary psychosis · Paraneoplastic encephalitis · Limbic encephalitis
Exam-exhaustive fellowship topic on autoimmune encephalitis presenting as organic psychosis — red flags, Graus AE and Pollak autoimmune-psychosis criteria, anti-NMDAR staged course, MRI/EEG/CSF/autoantibody work-up, immunotherapy principles, paraneoplastic search, FEP interface, and cautious symptomatic psychotropics. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Psychiatrists fail this topic when they treat every new psychosis as primary FEP, or when they chase isolated serum antibodies without a clinical syndrome. Examiners reward red-flag recognition, correct work-up hierarchy, honest limits of antibody testing, and early multidisciplinary immunotherapy — not a full neuroimmunology textbook recitation.[6][5][17]
Overview and definition
Organic (secondary) psychosis is psychosis caused by a medical, neurologic, toxic, or metabolic process rather than a primary psychotic disorder. Autoimmune encephalitis (AE) is a group of inflammatory brain diseases driven by immune responses against neuronal antigens; many present with prominent psychiatric features before hard neurology appears.[4][5]
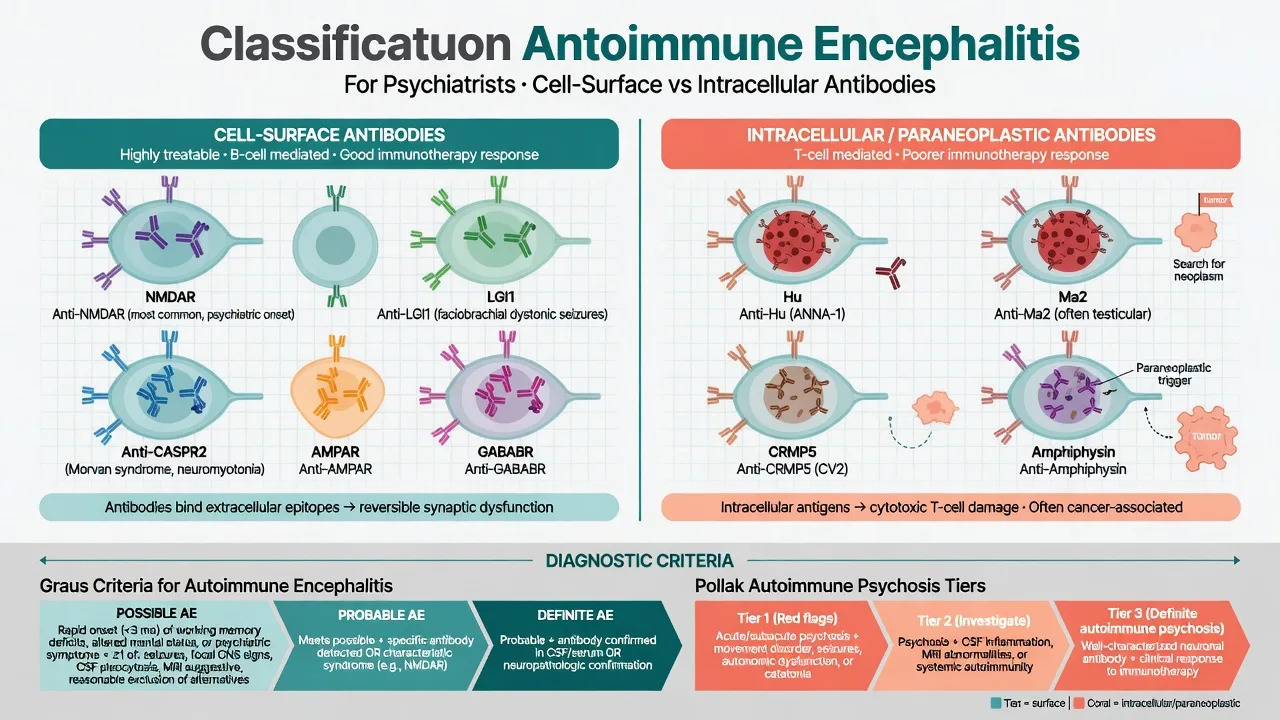
Antibody-mediated encephalitis (cell-surface or synaptic antibodies such as NMDAR, LGI1, CASPR2) is the psychiatry-relevant core: antibodies are often directly pathogenic, immunotherapy response is often good, and tumours (especially ovarian teratoma in anti-NMDAR disease) are disease-modifying targets.[1][4] Classic intracellular paraneoplastic antibodies (Hu, Ma2, CV2/CRMP5, amphiphysin) more often mark T-cell–mediated injury with poorer immunotherapy response and stronger cancer linkage — still organic psychosis differentials, different prognosis conversation.[4][3]
DSM-5-TR / ICD-11 frame secondary psychotic syndromes by medical cause; AE is not a freestanding DSM code you invent — you diagnose the encephalitis syndrome and treat the cause.[5]
Classification frameworks examiners expect
Graus 2016 — autoimmune encephalitis
Graus and colleagues provide a practical clinical approach to possible, probable, and definite AE using syndrome, MRI/EEG/CSF support, and antibody confirmation, designed so treatment is not indefinitely delayed by serology turnaround.[3] Key operational message for psychiatry: probable AE can be treated while awaiting definitive antibody results when the clinical–paraclinical package fits.[3][12]
Pollak 2020 — autoimmune psychosis consensus
An international consensus (Pollak et al., Lancet Psychiatry) proposes structured criteria for possible, probable, and definite autoimmune psychosis, translating AE logic into psychosis-first presentations and guiding when to escalate investigations and immunotherapy discussions.[5] Use it as a psychiatry-facing scaffold that still depends on neurologic partnership and rigorous antibody methodology — not as a licence to immunosuppress every atypical FEP.[5][17]
Antibody map (high-yield)
| Antibody | Typical phenotype | Psychiatry relevance | Tumour notes |
|---|---|---|---|
| NMDAR | Multistage encephalitis; psychosis, catatonia, dyskinesias, autonomic, hypoventilation | Prototype organic psychosis AE | Ovarian teratoma especially young women |
| LGI1 | Limbic encephalitis; FBDS; memory loss; hyponatraemia | Older adults mislabelled late-onset psychosis | Lower tumour rate than classic paraneoplastic |
| CASPR2 | Morvan/neuromyotonia spectrum; insomnia; autonomic | Severe insomnia, confusion | Thymoma associations in spectrum |
| AMPAR / GABABR | Limbic encephalitis ± seizures | Cognitive–psychiatric front | Higher paraneoplastic rates (e.g. SCLC for some) |
| Intracellular (Hu, Ma2, etc.) | Often multifocal, progressive | Organic psychosis possible | Strong cancer link; limited Ab-driven recovery |
Epidemiology and risk
Dubey and colleagues showed AE is not vanishingly rare relative to infectious encephalitis in modern diagnostics — the psychiatric trap is rarity framing that delays work-up.[10] Titulaer's large anti-NMDAR cohort established treatment-response and prognostic benchmarks still used in viva answers.[2]
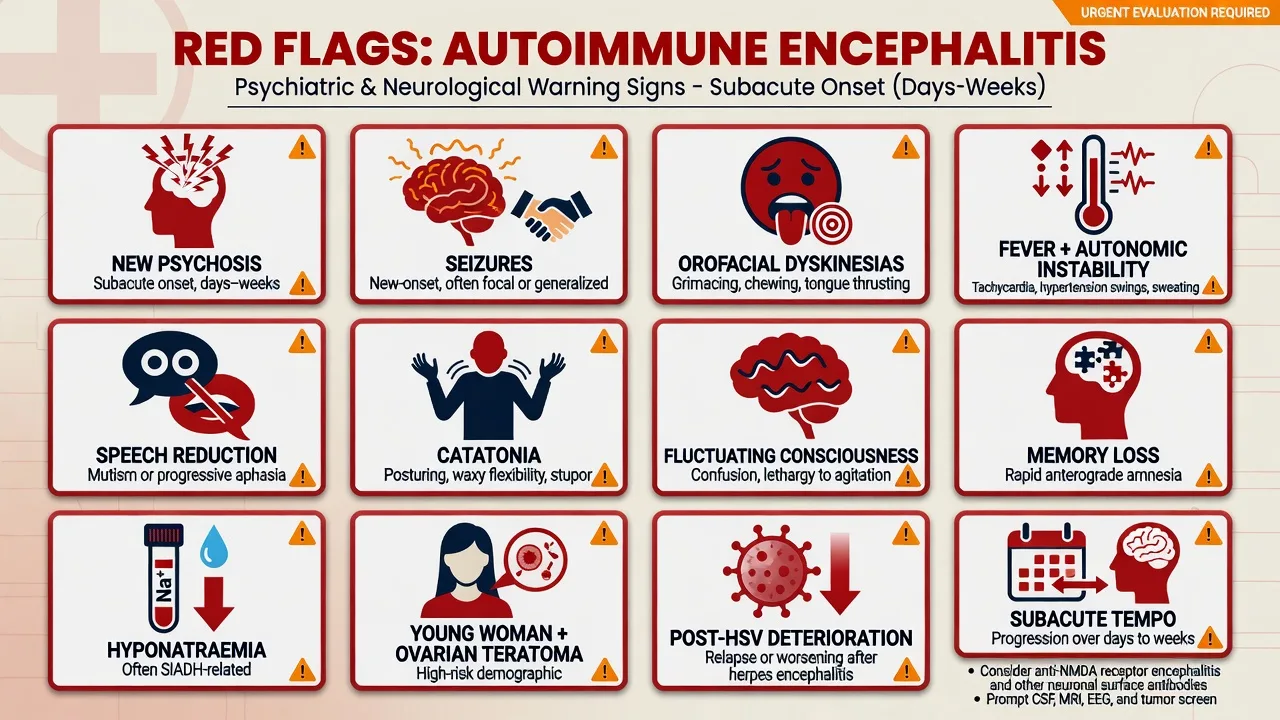
Risk clues: female sex and reproductive age (teratoma), recent HSV encephalitis, subacute tempo, seizures, movement disorders, hyponatraemia (think LGI1), and first presentation outside the usual FEP demography without substance explanation.[2][8][11]
Pathophysiology (psychiatry depth, not fluff)
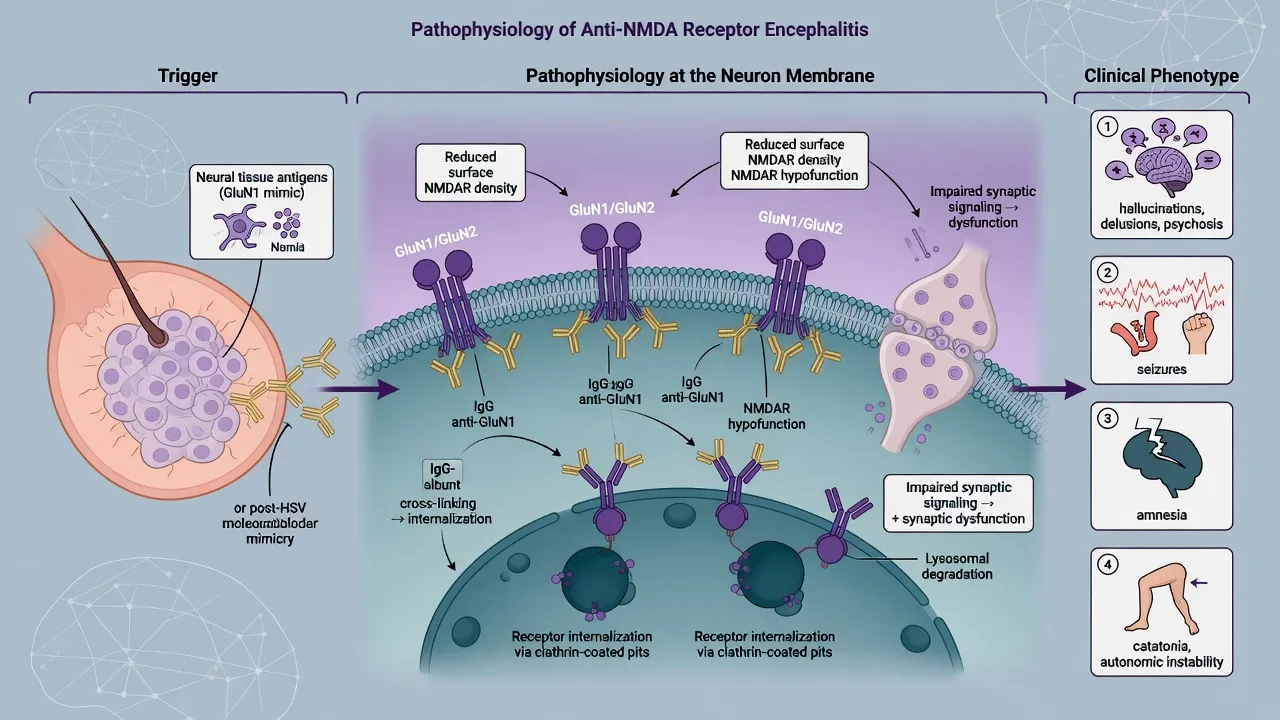
In anti-NMDAR encephalitis, IgG antibodies target the GluN1 (NR1) subunit of the NMDA receptor, causing receptor cross-linking and internalisation with reversible reduction of surface NMDAR — experimental and clinical observations that explain both psychiatric phenotype and treatment responsiveness when injury is not yet fixed.[1][4] Triggers include ovarian teratoma (neural tissue expressing NMDAR) and herpes simplex encephalitis as a post-infectious autoimmune sequel; many cases remain idiopathic.[1][11][4]
Cell-surface diseases differ mechanistically from many intracellular-antibody paraneoplastic syndromes, where cytotoxic T-cell injury dominates and antibody titres are biomarkers more than primary effectors — prognosis and immunotherapy expectations diverge accordingly.[4]
Clinical presentation
Anti-NMDAR staged course
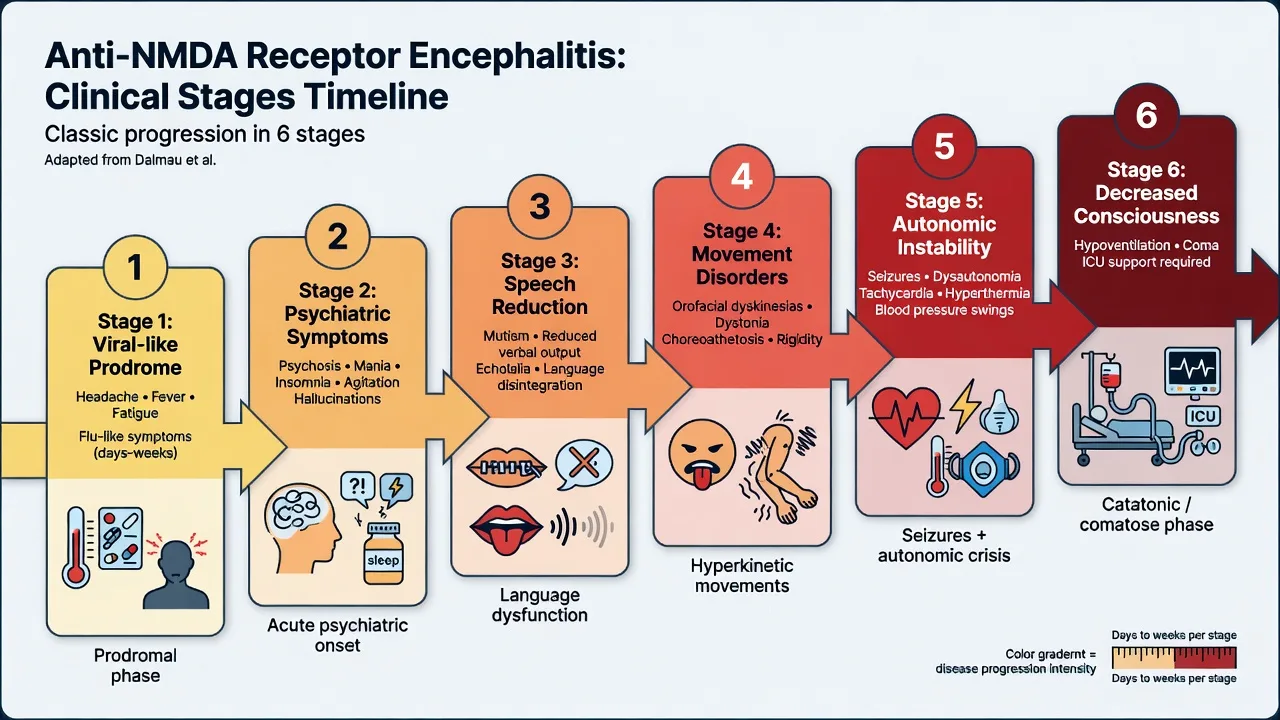
Fellowship stems often walk through: viral-like prodrome → psychiatric psychosis, mania, anxiety, insomnia, aggression → speech reduction or mutism → orofacial and limb dyskinesias, dystonia, catatonia → seizures and autonomic instability → central hypoventilation requiring ICU.[1][2][4] Not every patient is textbook sequential; pure or prolonged psychiatric phases occur and are exactly why psychiatry must own recognition.[7][6]
Psychopathology synthesis (Al-Diwani)
Individual-patient-data synthesis of adult NMDAR-antibody encephalitis shows a mixed mood–psychosis–catatonia–behavioural phenotype rather than a single first-rank schizophrenia clone. Expect mood lability, delusions, hallucinations, aggression, insomnia, and catatonic signs — often with rapid evolution that outpaces ordinary FEP tempo.[7]
LGI1 and CASPR2 (do not forget older adults)
Faciobrachial dystonic seizures (FBDS) — brief ipsilateral face and arm jerks — are a highly specific clinical clue to LGI1 antibody disease and often precede frank limbic encephalitis; hyponatraemia is common.[8][9] CASPR2 spectrum includes neuromyotonia, Morvan syndrome features, severe insomnia, and autonomic disturbance.[9] Mislabeling these as late-onset primary psychosis loses the immunotherapy window.
Red flags and differential
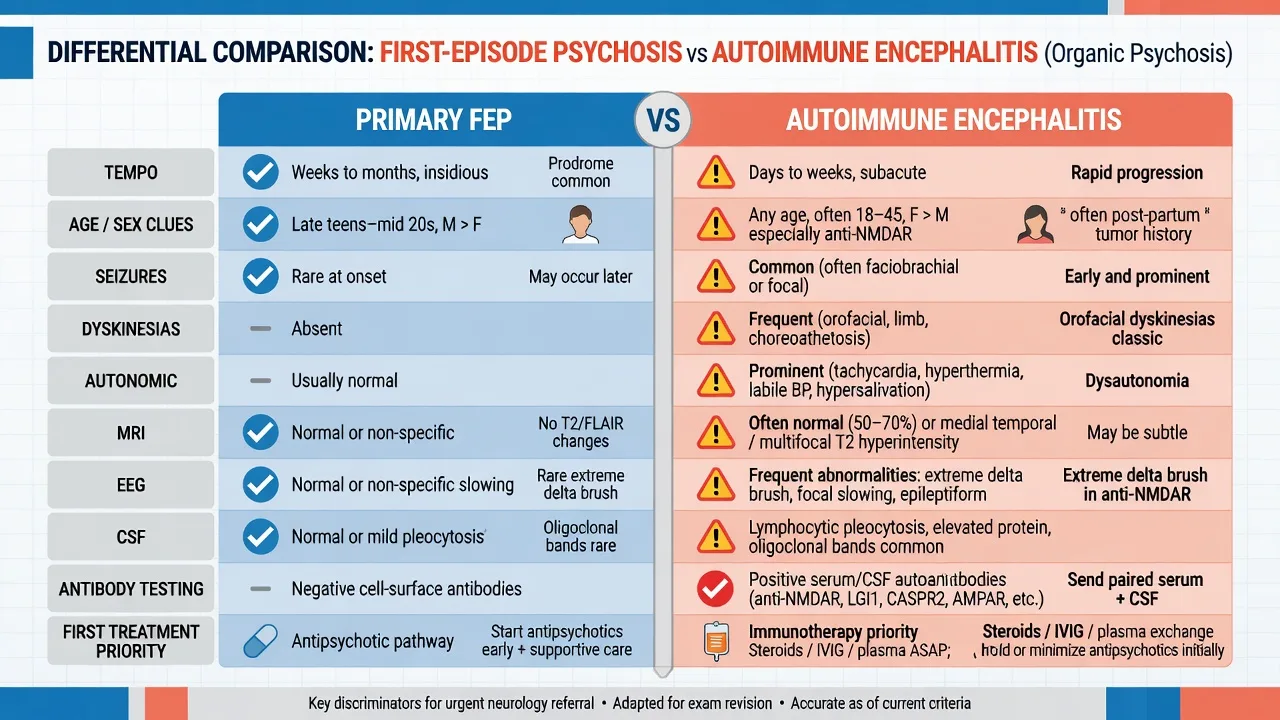
- Weeks–months prodrome more common
- Fewer hard neurologic signs early
- Baseline labs/metabolic focus
- Antipsychotic + EIS model first-line
- Selective AE testing if red flags emerge
- Days–weeks explosive tempo
- Seizures, dyskinesias, autonomic, speech change
- EEG/CSF often abnormal; MRI may be normal
- Immunotherapy + tumour search first-line when probable
- Psychotropics supportive only
- HSV encephalitis — antiviral urgency
- Delirium/metabolic/toxic
- NMS / serotonin toxicity / malignant catatonia
- CNS lupus, steroid psychosis, seizure-related
- Mass lesion / autoimmune limbic differentials
Discriminators, not laundry lists: clonus/hyperreflexia with serotonergics → serotonin toxicity pathway; lead-pipe rigidity after dopamine antagonists → NMS; pure environmental heat → heat stroke; CSF lymphocytic pleocytosis + subacute encephalitis → infectious and autoimmune tracks in parallel until HSV PCR and AE work-up clarify.[12][3]
Assessment at the bedside
- Tempo chart — hour/day evolution from premorbid baseline; viral prodrome; sleep collapse.
- Collateral — speech change, facial movements, nocturnal seizures, personality rupture.
- MSE with examples — fluctuating alertness; catatonic excitement or stupor; poorly systematised psychosis evolving over days.
- Neurologic screen — FBDS, orofacial dyskinesia, myoclonus, tone, pupils, autonomic vitals.
- Risk — suicide, violence, vulnerability, absconding; capacity for LP/MRI/immunotherapy; local Mental Health Act principles (jurisdiction-specific statutes — do not invent foreign section numbers).
- Apply structured red-flag and Pollak-style thresholds to decide investigation intensity.[6][5][7]
Investigations
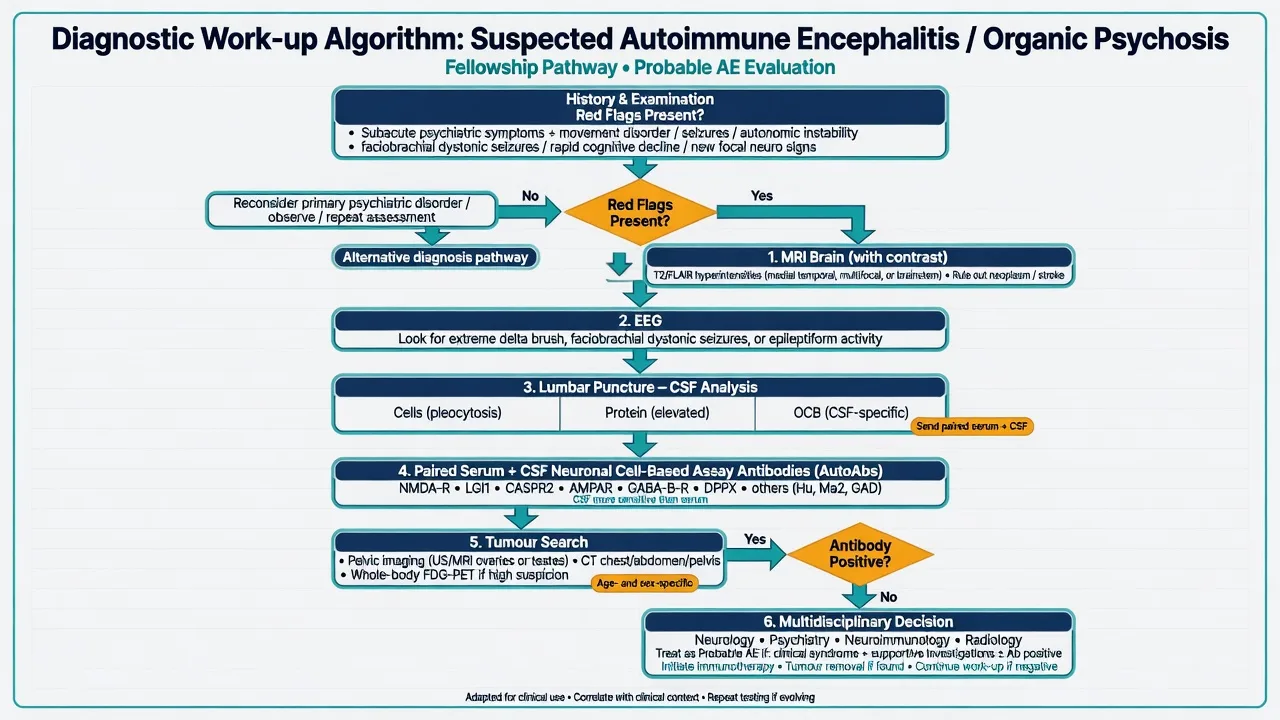
| Domain | What to do | Why it matters |
|---|---|---|
| Baseline | FBC, U&E (Na+), LFTs, glucose, CRP, B12, thyroid, infection screen, urine drug screen, pregnancy test | Exclude common organic causes; hyponatraemia flags LGI1 spectrum |
| MRI brain | Urgent when red flags; often normal or subtle in NMDAR; medial temporal T2/FLAIR in limbic AE | Normal MRI does not exclude anti-NMDAR disease |
| EEG | Almost always useful; slowing common; extreme delta brush associated with NMDAR (supportive, not required) | Captures encephalopathy and non-convulsive seizures |
| CSF | Cells, protein, glucose, OCB, HSV PCR as indicated; paired serum + CSF neuronal Abs on cell-based assays | Gold-standard context for NMDAR disease; pleocytosis supports AE |
| Tumour search | Pelvic US/MRI for teratoma in relevant patients; broader CT/PET strategy by Ab and age/sex | Tumour removal is disease-modifying |
| Testing strategy | Targeted testing driven by red flags preferred over unthinking universal FEP panels | Avoid false positives and missed high-risk cases |
Antibody testing pitfalls: commercial serum-only tests can miss or overcall; CSF increases diagnostic confidence in anti-NMDAR disease; isolated low-level serum positivity without syndrome is not automatic "autoimmune psychosis."[4][17][13] Lennox found serum neuronal cell-surface antibodies enriched in FEP versus controls, but clinical relevance requires full phenotype and methodologic care — Guasp and Dalmau caution against over-searching unselected psychiatric populations.[15][17] Australian early-psychosis testing guidance (Scott) and later FEP service analyses (Cohn) support thoughtful targeted testing, not dogma that every mild FEP needs a full AE panel.[13][14]
Acute management
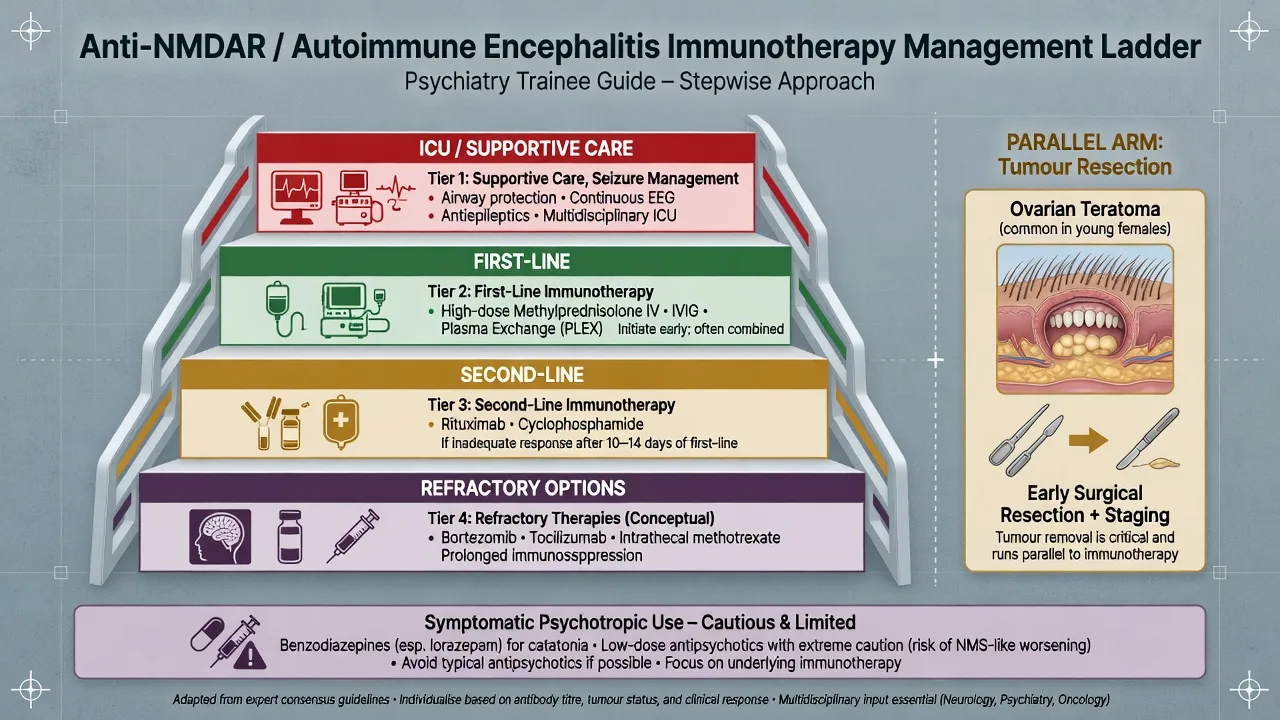
Medical priorities first: airway and ventilation risk (especially anti-NMDAR hypoventilation), seizure control, autonomic instability, DVT prophylaxis, aspiration precautions, and ICU liaison.[2][12]
Symptomatic psychotropics: use the lowest effective doses for dangerous agitation or psychosis as a bridge. Prefer cautious titration; benzodiazepines are first-line for catatonia and often for agitation. Avoid reflexive high-potency parenteral antipsychotic stacking that risks obscuring NMS/catatonia differentials. Antipsychotics do not replace immunotherapy.[5][12][7]
Definitive management — immunotherapy principles
First-line immunotherapy
Observational cohorts (Titulaer) and best-practice recommendations (Abboud) support early first-line immunotherapy once infectious mimics needing antivirals are addressed in parallel as clinically indicated: high-dose corticosteroids (commonly IV methylprednisolone about 1 g daily for 3–5 days in adult protocols — confirm local neurology protocol and product information), IV immunoglobulin (IVIG) (commonly total 2 g/kg divided over 2–5 days), and/or therapeutic plasma exchange (often about 5 exchanges on alternate days in many centres).[2][12][18] Exact combinations are specialist-led; psychiatry's job is to not block timely treatment while capacity and legal pathways are secured.[12][5]
Second-line and refractory
If response is inadequate, rituximab and/or cyclophosphamide are standard second-line escalations in anti-NMDAR and related AE pathways (dosing is neurology/oncology protocol–specific; example rituximab schedules include 375 mg/m² weekly × 4 or 1 g fortnightly × 2 — always under specialist governance).[2][12][18] Refractory disease may involve additional agents such as tocilizumab in selected cohort experience — know it exists; do not claim large RCT proof.[16]
Tumour treatment
In anti-NMDAR encephalitis with ovarian teratoma, prompt tumour resection plus immunotherapy associates with better outcomes — delaying imaging in young women with probable disease is an exam-fail.[1][2]
Do not wait forever for the lab
When probable AE criteria are met, start immunotherapy while antibody results pend, after appropriate infectious evaluation — delayed treatment predicts worse outcomes in large cohorts.[2][3][12]
Subtypes and scenarios
| Scenario | Fellowship pearl |
|---|---|
| Classic young woman + psychosis + dyskinesias | Anti-NMDAR until proven otherwise; pelvic imaging + CSF Abs + early immunotherapy |
| Older man + hyponatraemia + FBDS | LGI1 spectrum; do not call primary late-onset schizophrenia |
| Behavioural relapse after HSV encephalitis | Post-infectious AE (Armangue ~27%); reassess Abs and immunotherapy need |
| Antibody-negative probable AE | Treat on Graus/clinical package; serial review; avoid nihilism and overtreatment extremes |
| Isolated serum Ab, classic FEP otherwise | Do not immunosuppress on the lab alone (Guasp/Dalmau caution) |
| Intracellular paraneoplastic Abs | Aggressive cancer search; tempered immunotherapy expectations |
Complications and pitfalls
- Escalating antipsychotics only while encephalitis progresses.
- Reassured by normal MRI.
- Serum-only testing.
- Overcalling disease from incidental antibodies.
- Missing teratoma.
- Missing post-HSV AE.
- ICU complications: status epilepticus, dysautonomia, hypoventilation, VTE, infection on immunotherapy.
- Premature diagnostic fatalism ("schizophrenia forever") within weeks of onset.[6][2][17][11]
Prognosis and disposition
In Titulaer's multi-institutional anti-NMDAR cohort, most patients improved with immunotherapy and tumour treatment when needed, but recovery often unfolded over months, with substantial early ICU utilisation and residual cognitive/psychiatric morbidity in a minority — early treatment and tumour removal are key modifiable factors.[2] Disposition needs joint neuroimmunology + psychiatry follow-up, relapse education, rehabilitation, and careful psychotropic de-prescription as the encephalitis remits.[12][5]
Special populations
- Children/adolescents: movement disorders and speech regression may dominate over adult-like delusions; paediatric consensus (Nosadini) prioritises corticosteroids plus IVIG/PLEX pathways.[18]
- Older adults: weight LGI1/CASPR2 and limbic phenotypes heavily.[8][9]
- Pregnancy: multidisciplinary fetal–maternal–neurology planning; still pursue diagnosis and indicated immunotherapy.
- Intellectual disability/autism: new regression or catatonia deserves organic work-up, not diagnostic overshadowing.
- Cultural formulation: content of psychosis may be culturally shaped; red flags and tempo still drive investigation.[5][6]
Evidence, guidelines, and regional practice
FRANZCP candidates should cite targeted AE investigation in early psychosis guided by red flags (Scott ANZJP; service-level testing audits such as Cohn), escalate CL psychiatry–neurology pathways early, and avoid both under-investigation of explosive atypical psychosis and uncritical universal antibody screening of all mild FEP.[13][14][5]
Named landmarks to drop in viva: Dalmau 2008 series; Titulaer 2013 outcomes; Graus 2016 criteria; Dalmau/Graus NEJM 2018; Pollak 2020 consensus; Herken/Prüss red flags; Al-Diwani psychopathology; Irani FBDS; Armangue post-HSV; Dubey epidemiology; Abboud 2021 recommendations.[1][2][3][4][5][6][7][8][11][10][12]
Exam pearls
AE-PSYCH
- Normal MRI ≠ not NMDAR.[4][2]
- Extreme delta brush supports but does not prove anti-NMDAR encephalitis.[4]
- Post-HSV behavioural relapse ≈ think AE, not only viral reactivation.[11]
- FBDS ≈ LGI1 until proven otherwise.[8]
- First-line: steroids ± IVIG ± PLEX; second-line: rituximab/cyclophosphamide; parallel: tumour resection.[2][12]
- Do not immunosuppress the lab result without the syndrome.[17]
- Legal pathway: least restrictive care enabling life-saving investigation/treatment under local law — never invent interstate section numbers.[5]
Self-test: 30-second stem
A 23-year-old woman develops persecutory delusions and insomnia over 10 days after a viral-like prodrome. On day 12 she is mute with orofacial dyskinesias; temperature is normal; MRI is reported normal. Staff request IM antipsychotics only. What is your plan? Model: This is a classic anti-NMDAR red-flag package despite normal MRI. Escalate medical work-up: EEG, LP with CSF (including HSV PCR as indicated) and paired serum–CSF NMDAR cell-based assay, pelvic imaging for teratoma, neurology/ICU as needed. Start first-line immunotherapy when probable AE criteria are met; use benzodiazepines/cautious psychotropics for safety only — not as definitive care.[1][2][6][12]
References
- [1]Dalmau J, Gleichman AJ, Hughes EG, et al. Anti-NMDA-receptor encephalitis: case series and analysis of the effects of antibodies Lancet Neurol, 2008.PMID 18851928
- [2]Titulaer MJ, McCracken L, Gabilondo I, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study Lancet Neurol, 2013.PMID 23290630
- [3]Graus F, Titulaer MJ, Balu R, et al. A clinical approach to diagnosis of autoimmune encephalitis Lancet Neurol, 2016.PMID 26906964
- [4]Dalmau J, Graus F Antibody-Mediated Encephalitis N Engl J Med, 2018.PMID 29490181
- [5]Pollak TA, Lennox BR, Müller S, et al. Autoimmune psychosis: an international consensus on an approach to the diagnosis and management of psychosis of suspected autoimmune origin Lancet Psychiatry, 2020.PMID 31669058
- [6]Herken J, Prüss H Red Flags: Clinical Signs for Identifying Autoimmune Encephalitis in Psychiatric Patients Front Psychiatry, 2017.PMID 28261116
- [7]Al-Diwani A, Handel A, Townsend L, et al. The psychopathology of NMDAR-antibody encephalitis in adults: a systematic review and phenotypic analysis of individual patient data Lancet Psychiatry, 2019.PMID 30765329
- [8]Irani SR, Michell AW, Lang B, et al. Faciobrachial dystonic seizures precede Lgi1 antibody limbic encephalitis Ann Neurol, 2011.PMID 21416487
- [9]van Sonderen A, Petit-Pedrol M, Dalmau J, et al. The value of LGI1, Caspr2 and voltage-gated potassium channel antibodies in encephalitis Nat Rev Neurol, 2017.PMID 28418022
- [10]Dubey D, Pittock SJ, Kelly CR, et al. Autoimmune encephalitis epidemiology and a comparison to infectious encephalitis Ann Neurol, 2018.PMID 29293273
- [11]Armangue T, Spatola M, Vlagea A, et al. Frequency, symptoms, risk factors, and outcomes of autoimmune encephalitis after herpes simplex encephalitis: a prospective observational study and retrospective analysis Lancet Neurol, 2018.PMID 30049614
- [12]Abboud H, Probasco JC, Irani S, et al. Autoimmune encephalitis: proposed best practice recommendations for diagnosis and acute management J Neurol Neurosurg Psychiatry, 2021.PMID 33649022
- [13]Scott JG, Gillis D, Swayne A, et al. Testing for antibodies to N-methyl-d-aspartate receptor and other neuronal cell surface antigens in patients with early psychosis Aust N Z J Psychiatry, 2018.PMID 29923413
- [14]Cohn SL, Mohan A, Lappin JM, et al. Anti-N-Methyl-d-Aspartate Receptor Antibody Testing in First-Episode Psychosis: Universal or Targeted Testing J Neuropsychiatry Clin Neurosci, 2023.PMID 36128677
- [15]Lennox BR, Palmer-Cooper EC, Pollak T, et al. Prevalence and clinical characteristics of serum neuronal cell surface antibodies in first-episode psychosis: a case-control study Lancet Psychiatry, 2017.PMID 27965002
- [16]Lee WJ, Lee ST, Moon J, et al. Tocilizumab in Autoimmune Encephalitis Refractory to Rituximab: An Institutional Cohort Study Neurotherapeutics, 2016.PMID 27215218
- [17]Guasp M, Dalmau J Searching for Neuronal Antibodies in Psychiatric Diseases: Uncertain Findings and Implications Neurology, 2023.PMID 37353340
- [18]Nosadini M, Thomas T, Eyre M, et al. International Consensus Recommendations for the Treatment of Pediatric NMDAR Antibody Encephalitis Neurol Neuroimmunol Neuroinflamm, 2021.PMID 34301820