Psych · Consultation-liaison — burns and critical illness psychiatry
Burns and critical illness psychiatry
Also known as Burns psychiatry · Burn unit psychiatry · Self-inflicted burns · Post-burn PTSD · Burn scar body image · Critical illness psychiatry · PICS after burns · Carbon monoxide delayed neuropsychiatric sequelae
Exam-exhaustive fellowship reference on consultation-liaison psychiatry after burn injury and critical illness: ASD/PTSD and depression trajectories, body-image distress, self-inflicted burns and suicide risk, burn-unit delirium, smoke/CO neuropsychiatric sequelae, capacity, pain–trauma coupling, and PICS/PICS-F. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
9 MCQs with explanations
Target exams
Red flags
Fellowship examiners treat this as a dual C-L domain: (1) acute trauma plus lifelong disfigurement psychology after burns, and (2) critical-illness brain failure and survivorship when burn injury drives ICU care. The candidate who only says "refer psychology" or "give haloperidol for dressing agitation" fails.[1][3][10][12]
Definition and scope
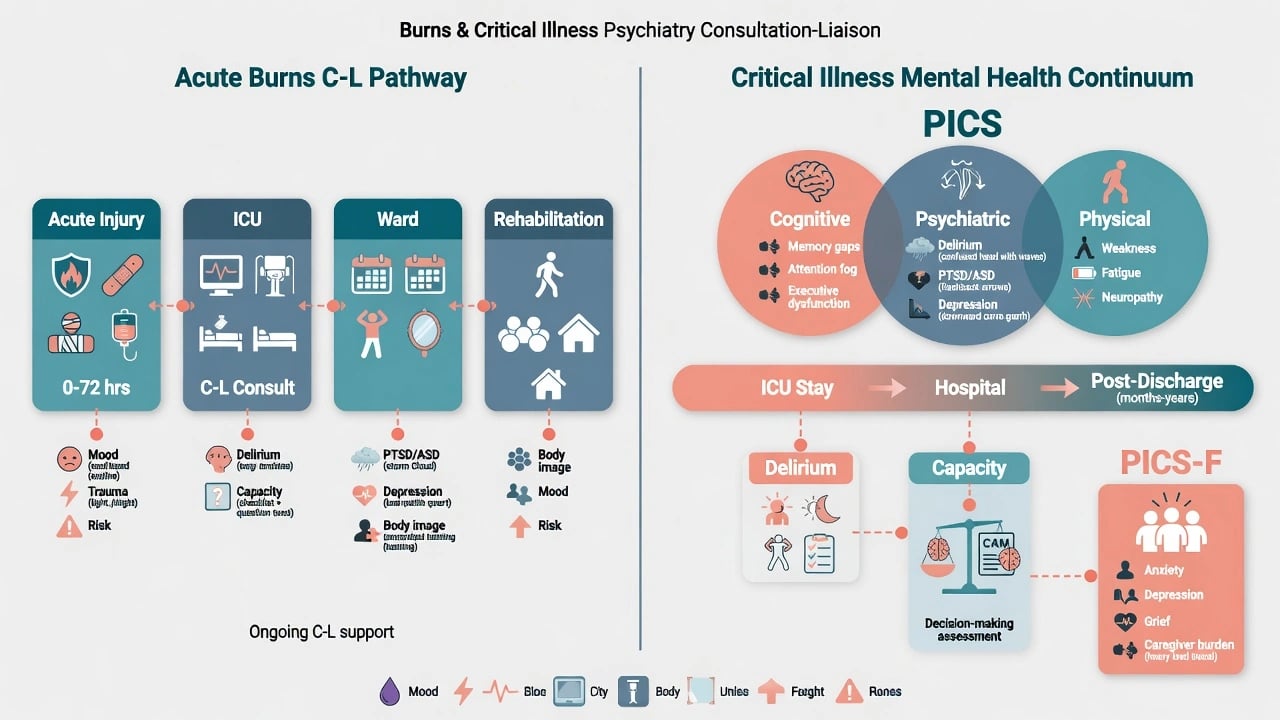
Burns psychiatry is the psychiatric and psychosocial assessment and care of people with thermal, chemical, electrical, and related injuries across acute resuscitation, burn ICU, surgical ward, and rehabilitation/community phases. Core tasks: trauma and mood surveillance, intentional-injury risk, pain–behaviour interface, body-image and social reintegration, substance issues, capacity for repeated procedures, and family work.[1][3][5]
Critical-illness psychiatry in this topic is the interface role when burns drive ICU admission: delirium recognition and behavioural safety, capacity for ICU decisions, family distress, and post-ICU psychiatric sequelae — complementary to dedicated delirium and transplant/ICU topics.[10][11][12][14]
Post-intensive care syndrome (PICS) denotes new or worsening cognitive, psychiatric, and/or physical impairment after critical illness. PICS-Family (PICS-F) captures analogous morbidity in relatives.[13][14]
Classification of presentations
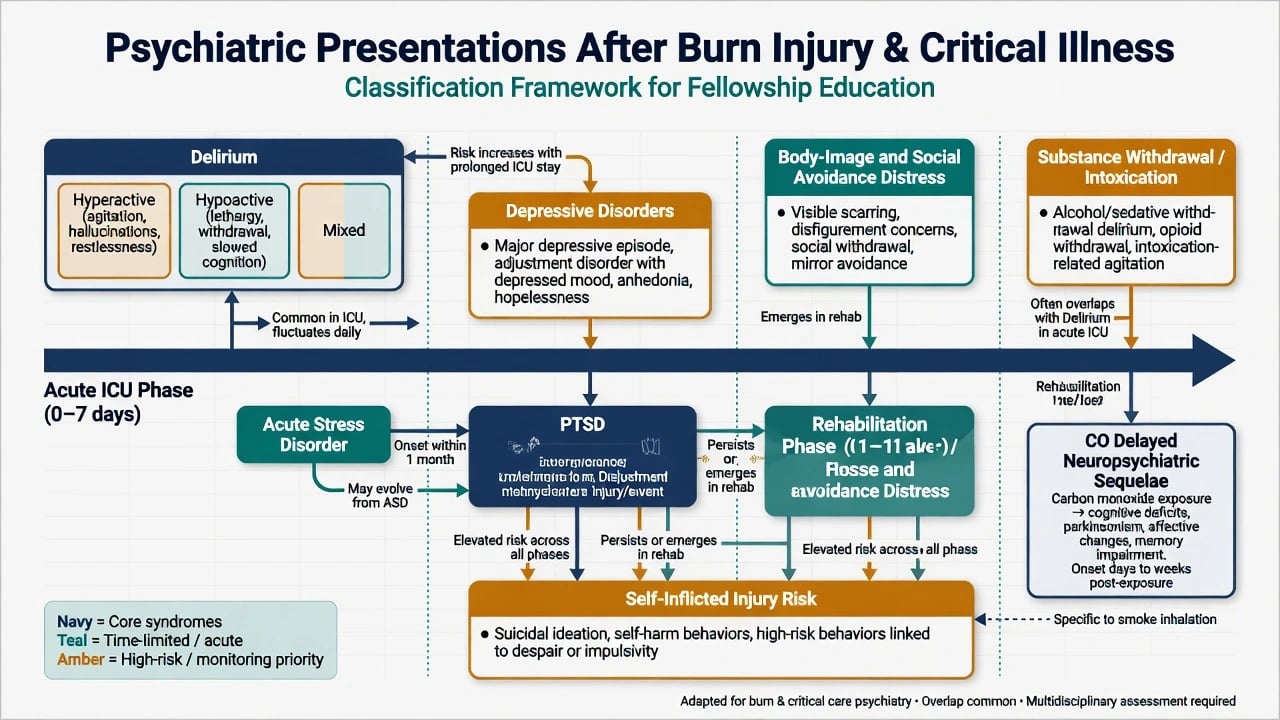
There is no burn-specific DSM code. Examinable clusters map to standard nosology timed against the injury course.[1][4][10][15]
| Cluster | When it peaks | Discriminators |
|---|---|---|
| Delirium (hyperactive / hypoactive / mixed) | ICU and early ward; fluctuates | Inattention + acute change; motor subtype |
| ASD → PTSD | Days–weeks → beyond 1 month | Intrusions of fire/ICU, avoidance, hyperarousal |
| Depressive disorders | Hospital and post-discharge | Anhedonia, guilt, SI — not only "understandable sadness" |
| Body-image / social avoidance distress | Scar maturation and re-entry | Mirror avoidance, intimacy/work withdrawal |
| Substance withdrawal / intoxication | Early admission | Timeline of last use; may co-drive delirium |
| Self-inflicted injury frame | Presentation | Intent, planning, psychosis, substance, prior attempts |
| CO delayed neuropsychiatric sequelae | Days–weeks after lucid interval | Cognitive, affective, motor change after smoke/CO |
Epidemiology and risk
Syntheses of burn-scar psychopathology emphasise high burdens of PTSD, depression, and body-image problems that justify routine psychological pathways rather than ad hoc referral.[1] Thombs and colleagues' systematic review found major depression on structured interview in roughly 4–10% of adult burn patients in hospital and the year after discharge, while depressive symptom rates on scales are substantially higher — examiners expect both figures and the method distinction.[2] Longitudinal work shows substantial rates of moderate-to-severe depressive symptoms early after injury with meaningful persistence in a large fraction at longer follow-up.[5]
Prospective major-burn cohorts document ASD and PTSD prevalence, course, and predictors (including pain and early distress), making trauma screening examinable at multiple time points.[3][4] PTSD and pain jointly associate with functional disability after major burns — pain is not "only surgical."[6]
Self-inflicted burns are a minority of admissions but are enriched for major psychiatric illness; within major psychiatric illness cohorts the incidence of self-inflicted burn is clinically meaningful, and intentional injuries often carry larger TBSA and longer stays.[8][9] Suicide by burning remains a high-lethality method with heavy psychiatric comorbidity in case series.[9]
After critical illness generally, PTSD symptoms are common enough among ICU survivors to mandate follow-up thinking; PICS is the named survivorship frame from multi-stakeholder consensus work.[13][14]
Mechanisms
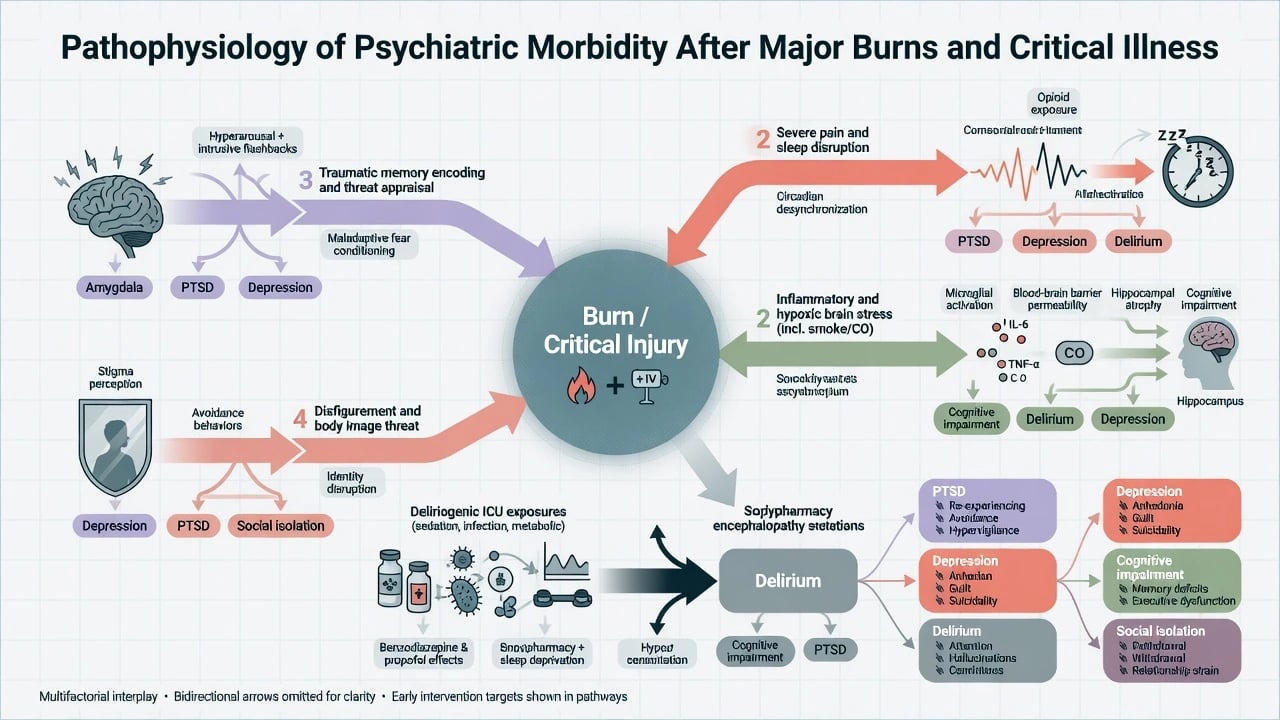
Multi-domain drivers of post-burn psychiatric morbidity include traumatic memory encoding of the fire and hospital course, severe pain and sleep fragmentation, systemic inflammation and hypoxic stress (including smoke/CO), threat to body integrity and social identity, and deliriogenic ICU exposures (infection, metabolic derangement, opioids, benzodiazepines, sedation depth).[1][6][10][12]
Carbon monoxide poisoning can produce delayed neuropsychiatric sequelae after a lucid interval — cognitive change, affective disturbance, and sometimes motor features — which is why fire/smoke stems require a toxicology timeline as well as a trauma timeline.[15] Hyperbaric oxygen for acute CO poisoning has randomised evidence for reducing cognitive sequelae in a landmark trial; local availability and indication thresholds vary by service.[15]
Clinical presentation
Acute ICU/ward. Flashbacks of flames, panic at the smell of dressings or smoke, hypervigilance at night, pulling lines during dressing changes, or the opposite: quiet inattention and fragmented speech (hypoactive delirium). Passive death wishes after first mirror exposure of facial or hand scars are high-yield stems.[1][4][10]
Intentional injury. Accelerant self-immolation with major depression or psychosis; impulsive self-harm with limited intent; substance-facilitated injury. Always assess current intent, residual means access, command hallucinations, and protective factors — not mechanism alone.[8][9]
Rehabilitation. Social withdrawal, sexual/relationship avoidance, vocational disability, body-checking, anger at appearance outcomes, and delayed PTSD as physical pain eases.[1][6]
Post-ICU. Delusional memories of staff "trying to hurt me," hospital avoidance delaying grafting or clinic, caregiver insomnia and hyperarousal (PICS-F).[13][14]
Differential discriminators
| Presentation | Prefer | Against |
|---|---|---|
| Agitation at dressing change | Pain + delirium + trauma cue | Primary mania without attention testing |
| Quiet compliance | Hypoactive delirium | "Good patient" / pure depression |
| Flashbacks after ICU | PTSD / ASD; residual delusional memory | Ongoing delirium if still fluctuating inattention |
| Refuses further grafting | Capable values-based refusal after teach-back | Incapacity from delirium/depression without support |
| Cognitive change weeks after house fire | CO delayed sequelae + depression/PTSD | Pure functional cognitive disorder without work-up |
| Self-inflicted burn | Full risk formulation | Automatic detention without assessment |
Assessment
Structure the burns C-L interview: mechanism and intent; substance timeline; psychiatric history and prior self-harm; pain scores and sleep; trauma symptoms; mood and suicide risk; body-image concerns; social support and housing after discharge; capacity for the specific procedure today.[1][8][16]
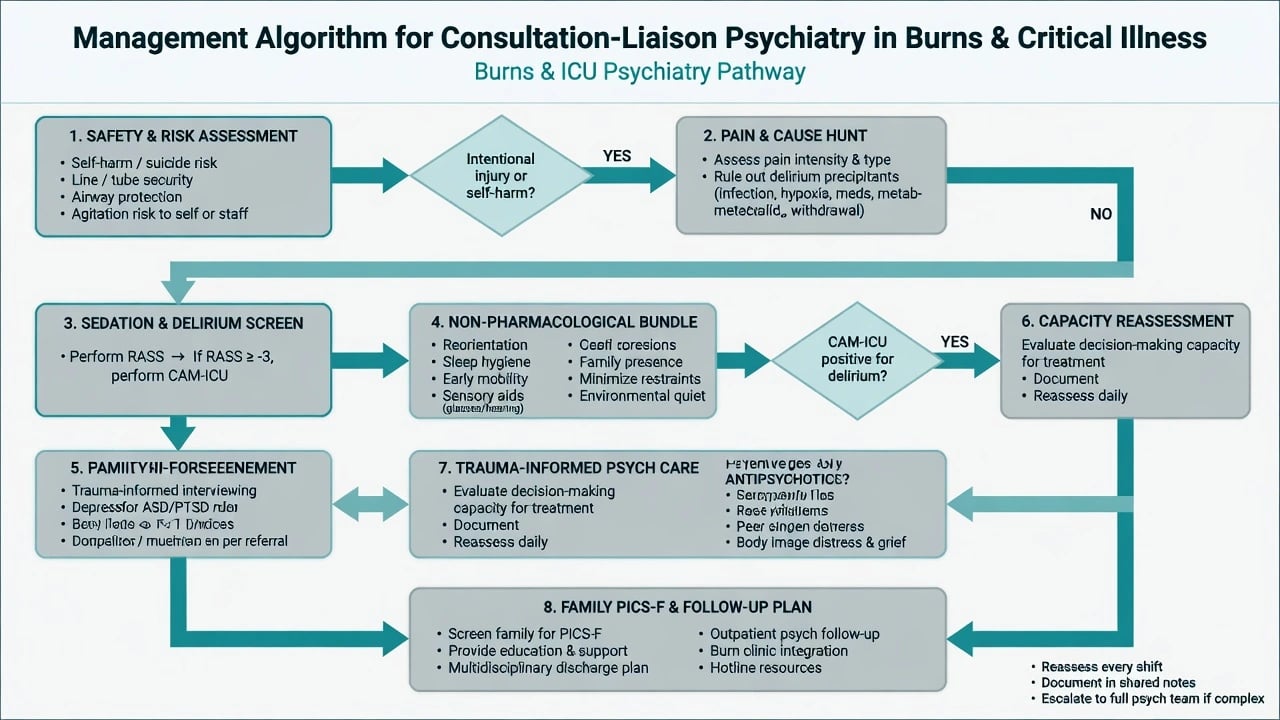
ICU interface sequence: RASS for arousal, then CAM-ICU when sufficiently arousable; document motor subtype; treat pain as first-line behavioural medicine.[11][12] Delirium is common enough in hospitalised adults with acute burns that systematic screening is justified; drivers overlap general ICU risk plus burn-specific pain and infection burden.[10]
Capacity is decision-specific and time-specific. The four functional abilities remain: understand relevant information; appreciate the situation and consequences; reason (use or weigh) options; communicate a choice — after material disclosure.[16] Grafting, debridement, intubation, and discharge against advice are separate decisions. Supported decision-making first: quieter environment, simpler language, timing off sedation peaks, interpreter, family as support not automatic substitute. Emergency necessity for life-saving care when incapacity and serious harm applies under local law — do not invent statute numbers.[16]
Investigations (psychiatry role)
- Delirium cause panel owned by burn/ICU teams; psychiatry audits deliriogenic medications and withdrawal risk.[10][12]
- Toxicology as clinically indicated; carboxyhaemoglobin and CO exposure history in smoke inhalation.[15]
- Cognitive screen when delayed CO sequelae or prolonged ICU cognitive change is suspected.[14][15]
- Baseline metabolic panel and ECG awareness before antipsychotics/antidepressants in critical illness (QTc, renal/hepatic failure, interactions with antiemetics and methadone where used).[12]
Acute and emergency management
- Safety — protect airway devices and grafts; 1:1 observation when suicide/self-harm risk is high after intentional injury; secure means.[8][9]
- Pain and cause hunt — hypoxia, hypoglycaemia, infection, constipation, urinary retention, withdrawal, under-analgesia.[10][12]
- Non-pharmacological bundle — reorientation, sleep hygiene, early mobility as burns allow, family presence, sensory aids, minimise restraints, environmental quiet — aligned with PADIS-informed ICU practice.[12]
- Limited short-term antipsychotics only for severe distress or dangerous agitation after medical causes and non-drug measures, with daily review — not as disease-modifying therapy for the delirium syndrome.[12] Agent choice must respect QTc, Parkinsonism risk, seizure threshold, and organ failure (local protocol).
- Capacity emergencies — treat under necessity principles when incapacity and life-threatening burn pathology; reassess when lucid.[16]
Definitive management
Trauma and mood
- Trauma-informed ward culture: predict painful procedures, offer control, avoid surprise exposure of scars without preparation.[1][3]
- Structured psychological approaches for acute post-trauma distress have proof-of-concept randomised support in burned patients (CBT-based protocols targeting ASD/PTSD/MDD risk pathways).[7] When PTSD criteria are met and medical stability allows, offer guideline-concordant trauma-focused psychological therapy (service-dependent modality).
- Treat depression as outcomes-relevant morbidity; symptom burden is high early and can persist — do not dismiss as inevitable reaction to scarring.[2][5]
- Coordinate antidepressants with burn physiology (nutrition, absorption after GI compromise, seizure threshold with some agents, QTc with others); start low and monitor closely in critical illness — agent selection is individualised with the medical team.
Pain–PTSD coupling
PTSD and pain amplify disability together; joint management (adequate analgesia, adjuvants, psychological pain coping, sleep) is examinable as psychiatric care.[6]
Body image and social reintegration
Target shame, mirror exposure hierarchies, graded social exposure, peer support, vocational rehab, and sexual/relationship counselling when relevant — core burn-scar psychology, not vanity work.[1]
Self-inflicted burns pathway
Full risk assessment; treat underlying mood/psychosis/substance use; involve mental health legislation only when statutory criteria are met for psychiatric treatment — it does not automatically authorise all surgical procedures.[8][9][16] Ongoing C-L engagement during grafting and rehab is the standard, not a single "cleared" note.
Critical-illness survivorship
Name PICS domains; screen PTSD/depression after ICU; consider ICU diaries where services use them (evidence for reduced new-onset PTSD after critical illness in a randomised trial — transferable principle to burn ICU programmes); screen families for PICS-F.[13][14]
Special populations
- Children/adolescents: developmental body image, school re-entry, caregiver guilt and PTSD.
- Older adults: scald mechanisms, high delirium risk, frailty, capacity complexity.
- Intellectual disability: supported decision-making for repeated procedures — not automatic exclusion from complex care.
- Cultural and Indigenous contexts: formulation of disfigurement meaning, family authority, fire-related collective trauma.
- Pregnancy after critical burn illness: joint obstetric–burn–psychiatry planning for psychotropics and pain.
Evidence and guidelines (named anchors)
| Anchor | Exam use |
|---|---|
| Van Loey and Van Son (2003) | Burn-scar psychopathology epidemiology and management frame |
| Thombs depression systematic review (2006) | MDD vs symptom-scale rates after burns |
| Wiechman depression trajectory (2001) | Early high symptom burden and persistence |
| Fauerbach distress cohort (2007); McKibben ASD/PTSD (2008) | Prospective trauma course after major burns |
| Corry PTSD and pain (2010) | Functional disability coupling |
| Fauerbach CBT acute posttrauma distress (2020) | Early psychological intervention signal |
| Atwell (2019); Smith (2023) | Self-inflicted burns and suicide by burning |
| Stanley delirium burns systematic review (2022) | Delirium burden in acute burns |
| CAM-ICU (Ely); PADIS 2018 (Devlin) | ICU screening and bundle philosophy |
| Needham PICS conference (2012); Parker PTSD meta-analysis (2015) | Critical-illness survivorship |
| Weaver HBO CO trial (2002) | Named CO cognitive sequelae trial |
| Appelbaum capacity (2007) | Four abilities; decision-specific capacity |
Region notes
ANZ (FRANZCP primary). C-L psychiatrists embed in major burn centres; mental health acts and guardianship/capacity statutes differ by state/territory — principles only in exam answers. ICU practice aligns with PADIS-informed bundles adapted locally.[12][16]
UK (MRCPsych). Capacity language often maps to MCA-style understand/retain/use-or-weigh/communicate; major burn centres use integrated psychology pathways.[16]
US (ABPN). Burn Model System-style longitudinal psychology is a frequent reference culture; capacity is clinical with state law overlay.[3][16]
India (MD/DNB, NEET-SS). Resource and caregiver structure heavily influence rehab and intentional-injury aftercare; still apply functional capacity and trauma/depression screening logic.[1][16]
Exam pearls
Bottom line for viva
Be the psychiatrist who can run a structured burns C-L assessment, separate trauma, depression, delirium, and body-image tracks, manage intentional injury without legal fiction, speak RASS/CAM-ICU/PADIS fluently without over-owning intensive care medicine, assess capacity without outcome bias, and follow survivors and families into PICS and PTSD care.[1][4][10][12][14][16]
References
- [1]Van Loey NE, Van Son MJ Psychopathology and psychological problems in patients with burn scars: epidemiology and management Am J Clin Dermatol, 2003.PMID 12680803
- [2]Thombs BD, Bresnick MG, Magyar-Russell G Depression in survivors of burn injury: a systematic review Gen Hosp Psychiatry, 2006.PMID 17088165
- [3]Fauerbach JA, McKibben J, Bienvenu OJ, et al. Psychological distress after major burn injury Psychosom Med, 2007.PMID 17585064
- [4]McKibben JB, Bresnick MG, Wiechman Askay SA, Fauerbach JA Acute stress disorder and posttraumatic stress disorder: a prospective study of prevalence, course, and predictors in a sample with major burn injuries J Burn Care Res, 2008.PMID 18182894
- [5]Wiechman SA, Ptacek JT, Patterson DR, et al. Rates, trends, and severity of depression after burn injuries J Burn Care Rehabil, 2001.PMID 11761394
- [6]Corry NH, Klick B, Fauerbach JA Posttraumatic stress disorder and pain impact functioning and disability after major burn injury J Burn Care Res, 2010.PMID 20061832
- [7]Fauerbach JA, Gehrke AK, Mason ST, et al. Cognitive Behavioral Treatment for Acute Posttrauma Distress: A Randomized, Controlled Proof-of-Concept Study in Burned Patients Arch Phys Med Rehabil, 2020.PMID 30776324
- [8]Atwell K, Bartley C, Cairns B, Charles A Incidence of self-inflicted burn injury in patients with Major Psychiatric Illness Burns, 2019.PMID 30429073
- [9]Smith JM, Fine JR, Romanowski KS, et al. Suicide by self-inflicted burns - A persistent psychiatric problem Burns, 2023.PMID 35810037
- [10]Stanley GHM, Barber ARJ, O'Brien AM, et al. Delirium in hospitalised adults with acute burns - A systematic review Burns, 2022.PMID 35701326
- [11]Ely EW, Inouye SK, Bernard GR, et al. Delirium in mechanically ventilated patients: validity and reliability of the confusion assessment method for the intensive care unit (CAM-ICU) JAMA, 2001.PMID 11730446
- [12]Devlin JW, Skrobik Y, Gélinas C, et al. Clinical Practice Guidelines for the Prevention and Management of Pain, Agitation/Sedation, Delirium, Immobility, and Sleep Disruption in Adult Patients in the ICU Crit Care Med, 2018.PMID 30113379
- [13]Parker AM, Sricharoenchai T, Raparla S, et al. Posttraumatic stress disorder in critical illness survivors: a metaanalysis Crit Care Med, 2015.PMID 25654178
- [14]Needham DM, Davidson J, Cohen H, et al. Improving long-term outcomes after discharge from intensive care unit: report from a stakeholders' conference Crit Care Med, 2012.PMID 21946660
- [15]Weaver LK, Hopkins RO, Chan KJ, et al. Hyperbaric oxygen for acute carbon monoxide poisoning N Engl J Med, 2002.PMID 12362006
- [16]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292