Psych · Consultation-liaison — capacity and consent
Capacity and informed consent
Also known as Decision-making capacity · Informed consent · Competence to consent · MacCAT-T · Best interests · Substituted decision-making · Treatment refusal · Mental capacity assessment
Exam-exhaustive fellowship reference on decision-specific capacity and informed consent — four functional abilities (understand/appreciate/reason/communicate and MCA-style understand/retain/use-weigh/communicate), assessment method and teach-back, fluctuating capacity, valid consent elements, best interests and substitute decision principles, mental health law vs capacity law interface, CASC skills. Statutes are jurisdiction-specific; no invented section numbers. FRANZCP-primary, globally tagged.
On this page & tools
Your progress
Saved locally on this device.
10 MCQs with explanations
Target exams
Red flags
Overview and definition
Decision-making capacity is a clinical judgment about whether a person can make a specific decision at a specific time. Legal competence (terminology varies) often refers to a formal status determination by a court or tribunal. Clinicians assess capacity continuously at the bedside; courts resolve contested competence. Keep the terms clear in exams and notes.[1][11]
Informed consent (and informed refusal) requires three pillars: the person has capacity for that decision; they receive adequate material information (risks, benefits, alternatives, including doing nothing); and the choice is voluntary (free from coercion and undue influence).[2][11]
Core legal-ethical maxims examiners expect (presumption of capacity; decision- and time-specificity; unwise decisions may still be capable decisions; supports before substitution):[2][11]
| Principle | Clinical meaning |
|---|---|
| Presumption of capacity | Adults are assumed capable until evidence shows otherwise |
| Decision-specific | Capacity for antibiotics is not capacity for complex chemotherapy or financial instruments |
| Time-specific | Capacity can fluctuate (delirium, intoxication, settling psychosis) |
| Unwise ≠ incapable | A capable person may refuse recommended care |
| Supports first | Maximise decision-making ability before substituting |
These maxims organise bedside assessment and documentation across jurisdictions even when statutes differ.[2][11]

The four abilities (and jurisdiction language)
The modern functional model derives from Appelbaum and Grisso: capacity rests on four abilities rather than a psychiatric diagnosis.[1][2]
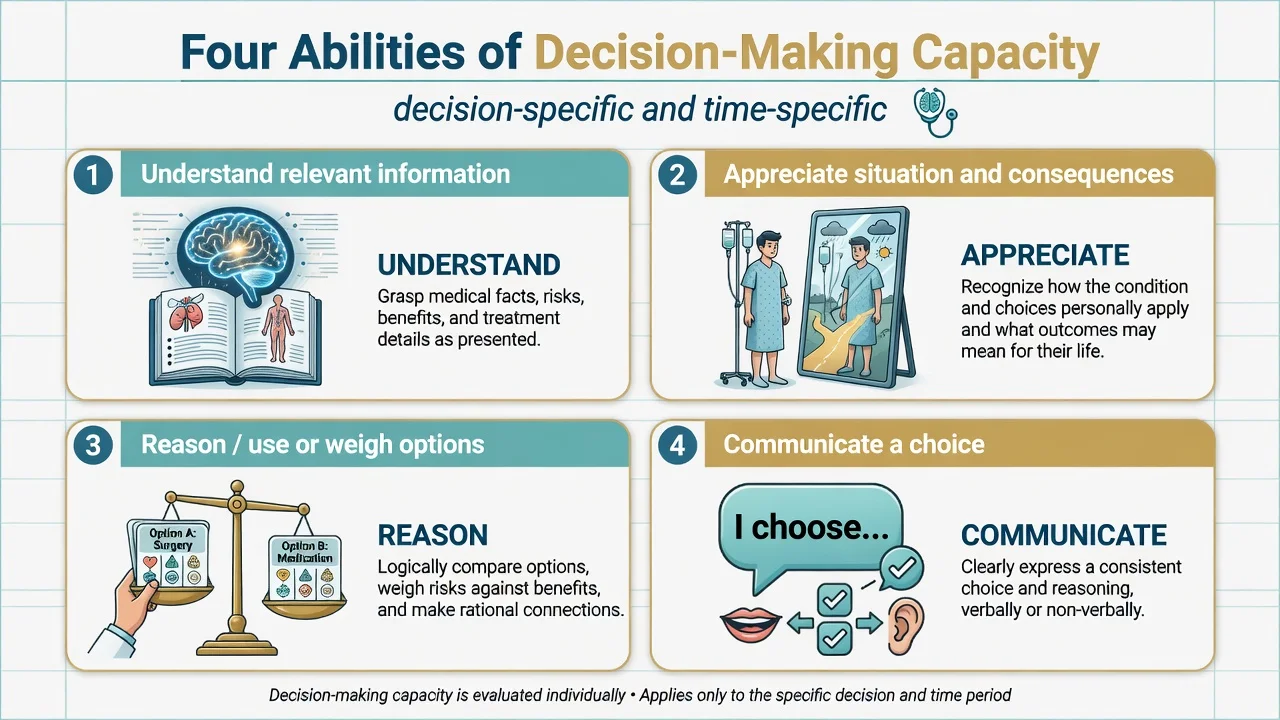
| Ability (Appelbaum/Grisso) | Common statute-style wording | Bedside probe |
|---|---|---|
| Understand relevant information | Understand / retain | Teach-back of condition, proposed treatment, main risks and alternatives |
| Appreciate situation and consequences | Use information as applied to self | Does the person accept that the information applies to them (not only abstractly)? |
| Reason about options | Use or weigh | Can they compare options and give a consistent rationale? |
| Express a choice | Communicate | Clear, stable choice by speech, writing, or other reliable means |
Appreciate is the ability most often failed when insight is poor (e.g. delusional denial of illness) even if factual understanding looks intact. Reason/weigh is vulnerable in severe executive dysfunction, mania, or profound depression that collapses future-oriented evaluation.[8][9][16]
Do not invent local section numbers. In FRANZCP/MRCPsych settings, candidates often reference UK Mental Capacity Act principles as a teaching scaffold, but Australian/NZ consent and guardianship schemes, US state laws, and other jurisdictions differ. State principles; name your jurisdiction when known.[2][11]
Informed consent elements
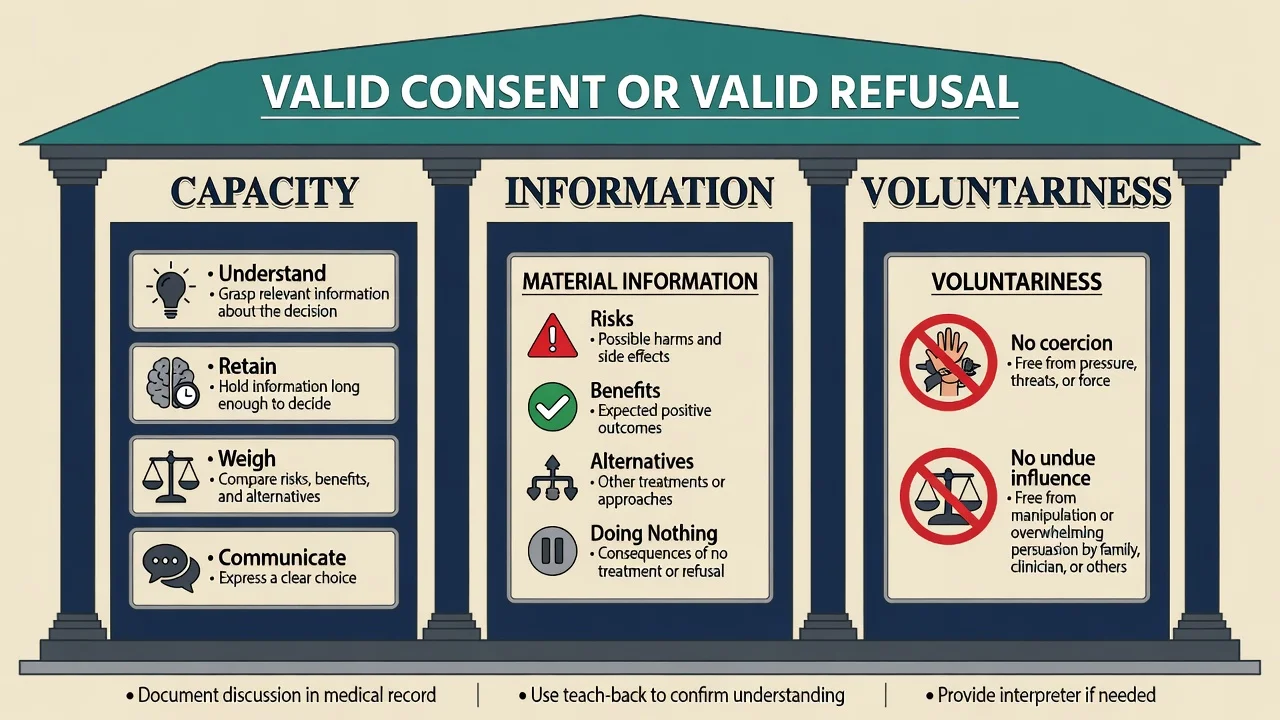
Information must be material to a reasonable person in the patient's position (and, in many systems, to what this patient would want to know): nature of condition, proposed intervention, expected benefits, material risks, alternatives including no treatment, and uncertainties. Voluntariness fails under coercion, threats, or undue influence even if cognitive abilities are intact. Quiet assent without understanding is not valid consent.[2][11]
Epidemiology and clinical burden
Mental incapacity is common in hospital medicine. In a landmark medical-inpatient study, a substantial minority lacked capacity for treatment decisions, with cognitive impairment a major associated factor — quiet incapacity is easy to miss if teams only seek signatures.[4]
Among psychiatric inpatients, systematic reviews and cross-sectional work show incapacity is frequent, varies by diagnosis, and associates with poor insight; reliability of structured assessment can be good when methods are standardised.[5][6][7][8] A 2024 systematic review and meta-analysis updates treatment decision-making capacity estimates in psychiatric inpatients and reinforces diagnosis-linked heterogeneity.[13]
Depression does not automatically remove capacity; many depressed patients retain it, but severe illness can impair appreciation and weighing — assess, do not assume.[9]
Mechanisms — why capacity fails
Attention, working memory, language, and executive function support understanding, retention, and reasoning. Psychotic delusions and anosognosia selectively damage appreciation. Mania may preserve fluent speech while destroying consistent weighing. Delirium produces fluctuating attentional failure. Intoxication creates reversible windows of incapacity. Cognitive impairment in schizophrenia maps onto specific capacity components rather than a uniform deficit.[12][16][8]
Clinical presentation (C-L stems)
Typical consultation-liaison referrals: refuses surgery or antibiotics; wants to leave against medical advice; consent for ECT or clozapine monitoring procedures; research consent; residential placement in dementia; oncology goals of care; transfusion refusal; dialysis withdrawal. Presentations include loud capable refusal, loud incapable refusal driven by delusion, and quiet assent without understanding.[2][10]
Differential and discriminators
- Understands and appreciates
- Weighs and chooses consistently
- May be unwise
- Respect and document
- Fails one or more abilities
- After adequate disclosure
- Supports tried
- Emergency / delay / substitute
- Language barrier (use interpreter)
- Coercion/undue influence
- Diagnosis alone
- Disagreement with doctor
Capacity for treatment is not the same as forensic fitness to plead or competence to stand trial. Do not import the wrong legal test.[11]
Bedside assessment method
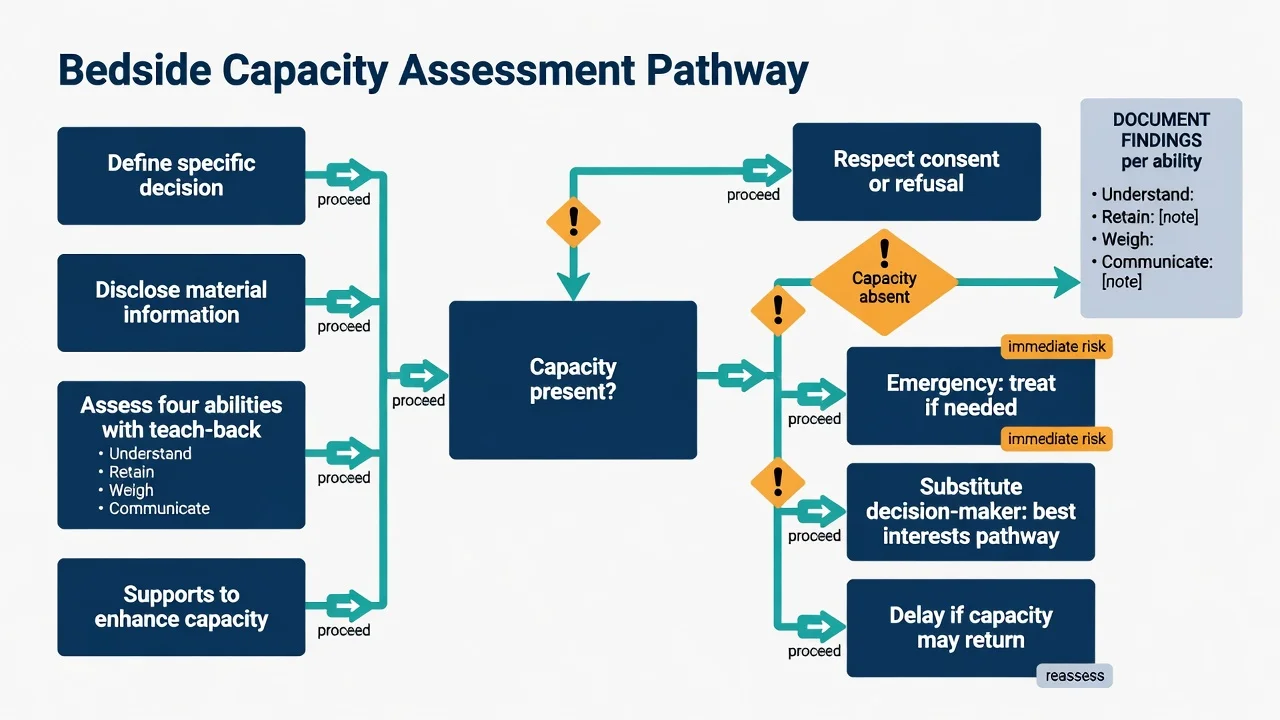
Practical sequence
- Name the decision precisely (e.g. "consent for laparoscopic cholecystectomy this admission", not "medical decisions").
- Optimise the setting — quiet room, glasses/hearing aids, interpreter, written aids, timing when least delirious or least sedated.
- Disclose material information in plain language; check understanding before judging incapacity.
- Probe each ability with open questions and teach-back; avoid yes/no suggestibility.
- Offer supports to enhance capacity; reassess.
- Conclude for this decision at this time; plan review if fluctuation expected.
- Document information given, findings per ability, conclusion, who was consulted, and next review.[2][10][12]
Structured tools
The MacCAT-T operationalises understanding, appreciation, reasoning, and expressing a choice for treatment decisions and improves standardisation; it supports, but does not replace, clinical and legal judgment.[3] Brief instruments used more in research consent contexts still require clinical integration. Cognitive screens (MoCA/MMSE) correlate imperfectly with capacity — useful adjuncts, never sole criteria.[10][12]
The JAMA Rational Clinical Examination review summarises that clinicians should use a systematic approach; no single screening question replaces a full functional assessment when stakes are high.[10]
CAPACITE
Decision-specificity and sliding scale
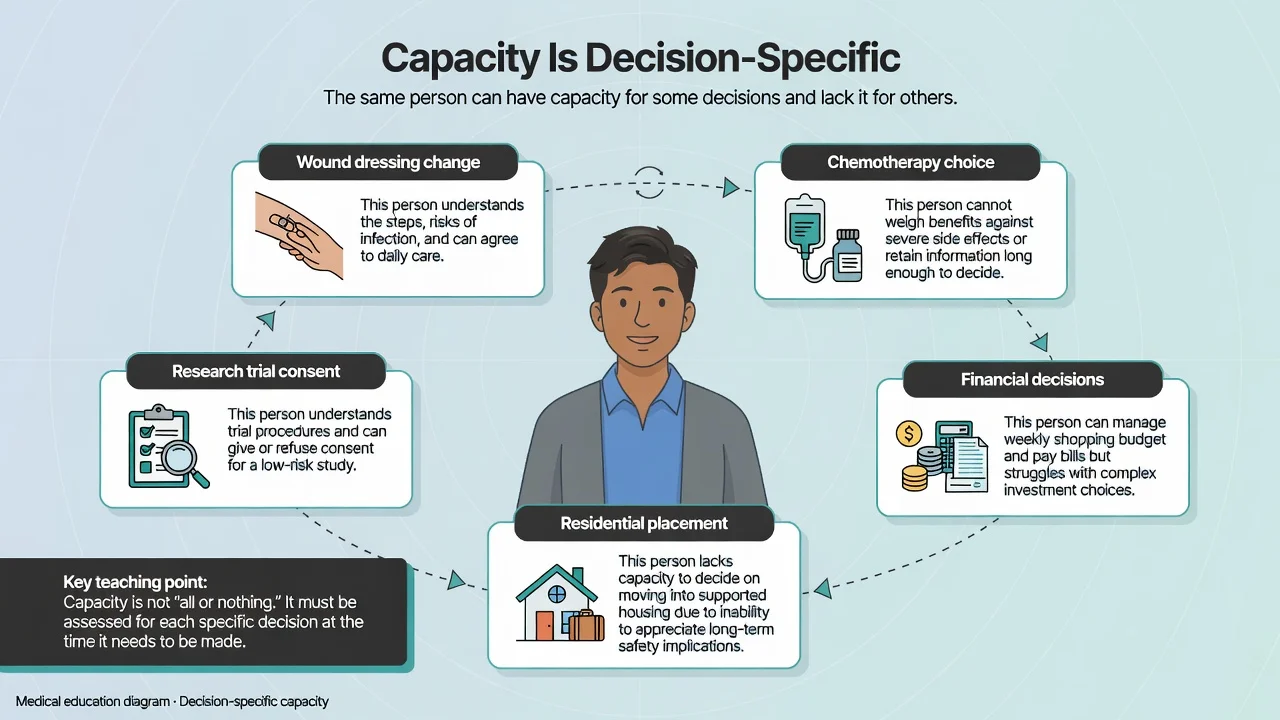
Riskier or more complex decisions demand more robust demonstration of abilities (clinical sliding-scale idea), while low-risk decisions may be within residual capacity even in significant cognitive impairment. Older adults with dementia often retain capacity for some choices and not others — do not globalise from a MoCA score.[14][15][2]
Fluctuating capacity
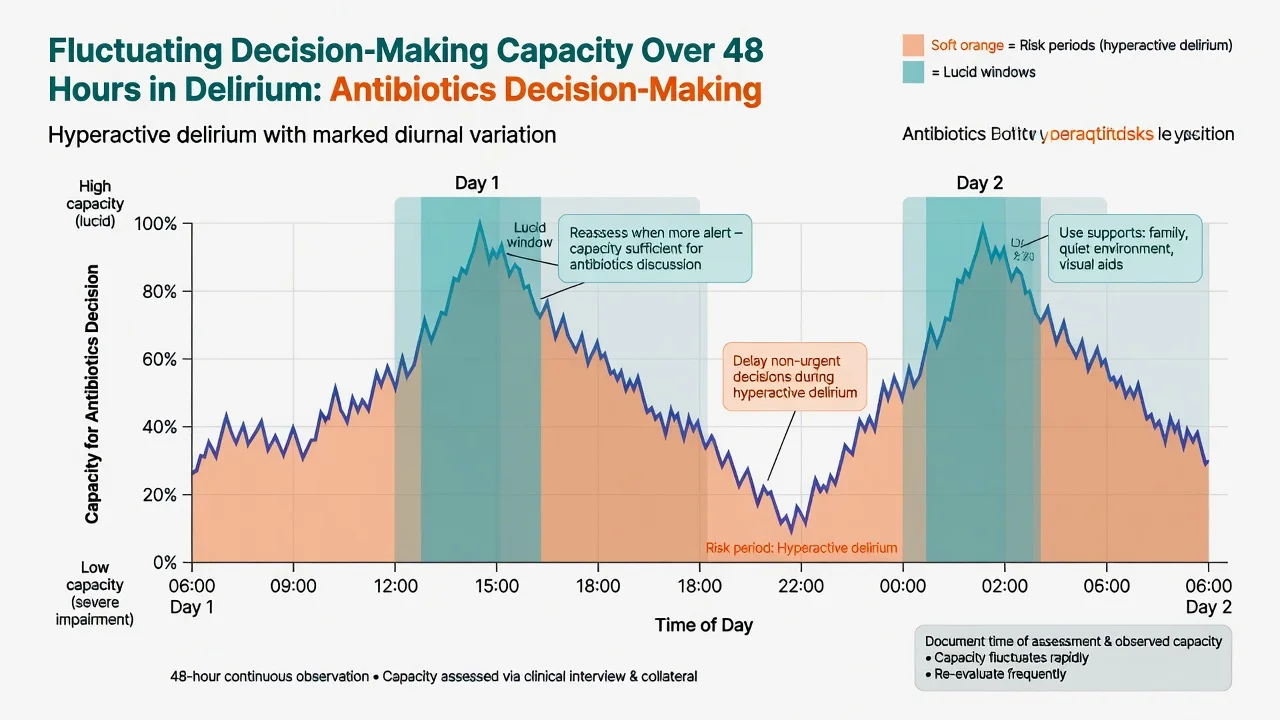
Delirium, post-ictal states, intoxication/withdrawal, and settling mania or psychosis produce fluctuation. If delay is safe, wait and reassess. If treatment cannot wait and capacity is absent, use emergency principles under local law and document necessity, attempts to enhance capacity, and the plan to re-consent when capacity returns.[2][4][10]
When capacity is absent
Branching options
| Path | When | Principles |
|---|---|---|
| Emergency treatment | Immediate serious harm risk; cannot wait | Necessity / statutory emergency powers; document; least that is needed |
| Delay and enhance | Decision can wait; reversible cause | Treat delirium/psychosis; supports; reassess |
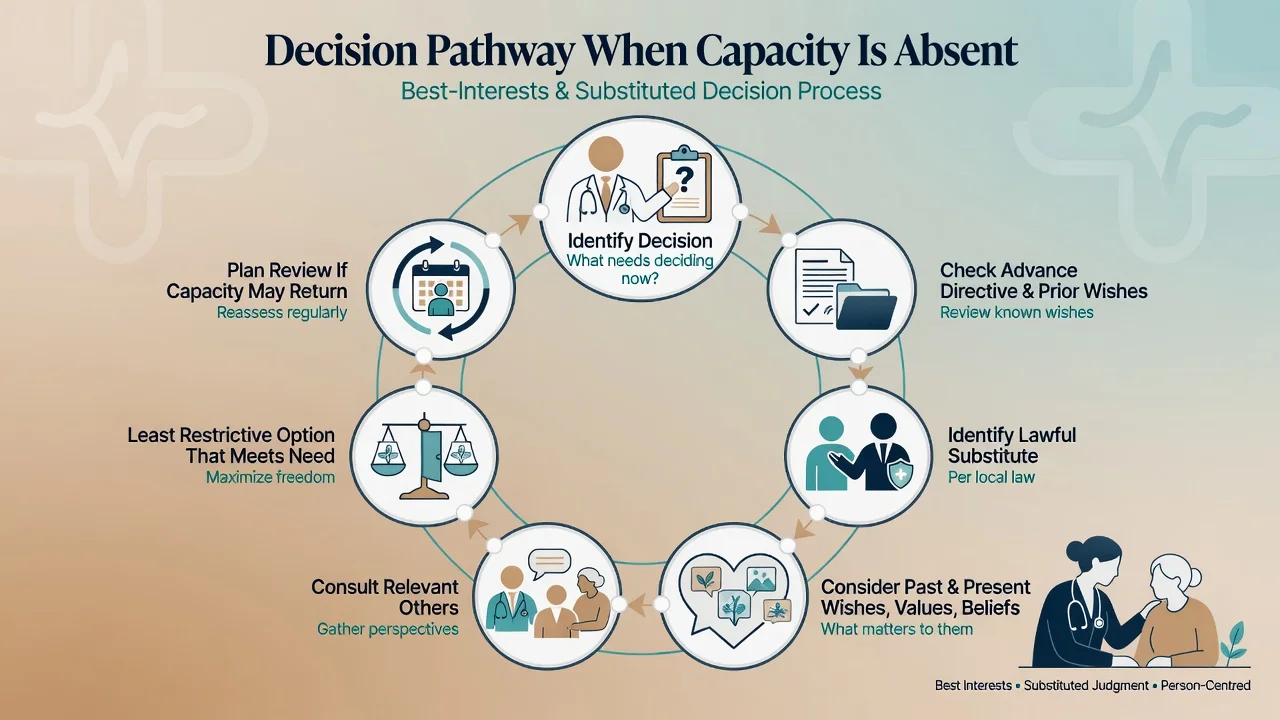
| Substitute / best interests | Capacity absent; decision needed | Lawful proxy/guardian or best-interests process under local law |
| Mental health pathway | Criteria met for compulsory psychiatric care | Separate statute; does not auto-authorise all medical procedures |
Best interests / substituted judgment (labels vary by jurisdiction) generally require attention to past and present wishes, values, beliefs, the least restrictive option that meets the need, and consultation with those close to the person — not clinician preference alone. Advance directives, if valid and applicable, often take priority; check local validity rules.[2][11]
Supported decision-making (maximising the person's own decision with help) is ethically preferred and aligns with contemporary disability-rights directions; substitute decision-making is a last resort after supports fail, not the first move.[11][12]
Mental health law vs capacity / consent law
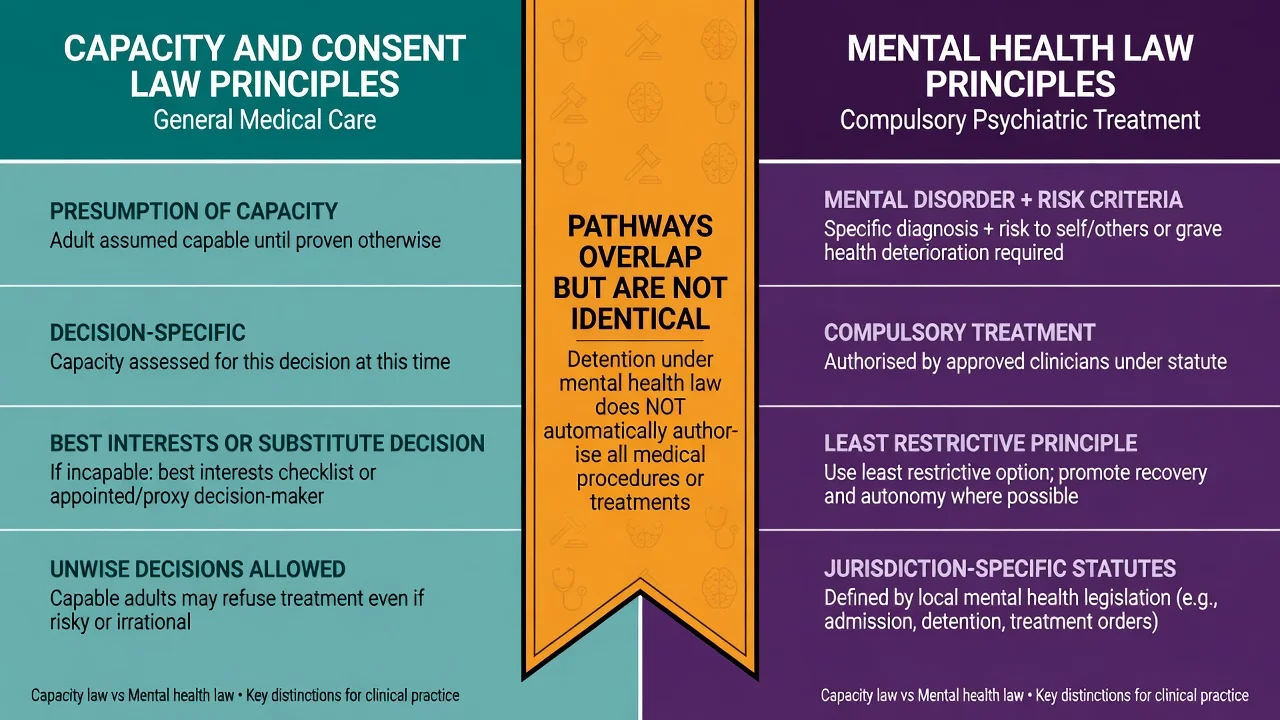
Exam gold: compulsory psychiatric treatment under mental health legislation typically turns on mental disorder plus risk (or equivalent statutory criteria) and least-restrictive principles. General medical consent for surgery, antibiotics, or oncology usually follows capacity/guardianship/consent frameworks. A person detained for psychiatric care may still have capacity for a medical procedure — or may lack it and need a separate substitute pathway. Never invent section numbers; say "under local mental health / guardianship legislation".[2][11]
Special populations
Older adults / dementia. Residual capacity is common for simple decisions; complex treatment and placement need careful assessment. Family report of "he always wanted X" informs best interests but does not replace assessment of current capacity.[14][15]
Intellectual disability. Assume capacity until assessed; invest heavily in supported decision-making and accessible information before any substitute pathway.[2][12]
Youth. Age thresholds and mature-minor doctrines are jurisdiction-specific; assess evolving capacity rather than age alone when local law allows.[2][11]
Perinatal. Pregnancy does not remove autonomy. Assess capacity as usual; severe perinatal psychosis may impair appreciation or weighing of obstetric decisions.[2][9]
Cultural and language factors. Interpreter first. Do not pathologise culturally framed illness explanations as automatic incapacity — test whether the person can still understand, appreciate, weigh, and choose.[2][10]
Research consent. Standards are typically stricter; use validated research-capacity approaches and legal representatives per ethics frameworks when capacity is impaired.[12]
Documentation standard (exam-ready)
Write: decision defined; information disclosed (key points); findings for each ability with quotes or paraphrases; supports offered; conclusion (capacity present/absent for this decision at this time); pathway chosen; review plan; people consulted. Avoid "lacks capacity" as a free-floating label.[2][10]
Pitfalls
- Outcome bias (refusal = incapacity)
- Diagnosis bias (psychosis = incapacity)
- Skipping disclosure
- Ignoring coercion
- Freezing fluctuating assessments
- Using family as unlawful substitute
- Conflating MHA powers with general medical consent
- Inventing statute sections in answers
- Quiet assent without teach-back
Prognosis and disposition
Many incapacity states are temporary. Plan for recovery of capacity and re-consent. Disposition is a formulation: treat under emergency powers, wait, substitute, or use mental health pathways for psychiatric treatment when criteria are met — state which path and why.[2][5][13]
CASC and communication skills
CASC stations reward clear disclosure, teach-back, non-coercive exploration of refusal, and accurate pathway language without invented statute numbers.[1][2]
- Explain risks/benefits/alternatives simply; check understanding without humiliation.
- Explore reasons for refusal with curiosity, not argument.
- Separate alliance-building from coercion.
- When discussing substitute decision-makers, be transparent and empathic with family while protecting the person's legal rights.
- If delaying surgery for delirium clearance, explain the safety rationale to the surgical team in plain capacity language.
These communication moves implement the same functional assessment standards used in written exams.[2][10]
Exam pearls
Landmark anchors to cite by name: Appelbaum and Grisso abilities framework and 2007 NEJM review; MacCAT-T; Raymont medical inpatients; Cairns psychiatric prevalence/reliability; Okai review; Owen diagnosis/insight; Hindmarch depression; Sessums JAMA RCE; Palmer capacity assessment reviews; Kim/Karlawish dementia competence literature; Marcó-García 2024 meta-analysis.[1][2][3][4][5][7][13]
References
- [1]Appelbaum PS, Grisso T Assessing patients' capacities to consent to treatment N Engl J Med, 1988.PMID 3200278
- [2]Appelbaum PS Clinical practice. Assessment of patients' competence to consent to treatment N Engl J Med, 2007.PMID 17978292
- [3]Grisso T, Appelbaum PS, Hill-Fotouhi C The MacCAT-T: a clinical tool to assess patients' capacities to make treatment decisions Psychiatr Serv, 1997.PMID 9355168
- [4]Raymont V, Bingley W, Buchanan A, et al. Prevalence of mental incapacity in medical inpatients and associated risk factors: cross-sectional study Lancet, 2004.PMID 15488217
- [5]Cairns R, Maddock C, Buchanan A, et al. Prevalence and predictors of mental incapacity in psychiatric in-patients Br J Psychiatry, 2005.PMID 16199799
- [6]Cairns R, Maddock C, Buchanan A, et al. Reliability of mental capacity assessments in psychiatric in-patients Br J Psychiatry, 2005.PMID 16199798
- [7]Okai D, Owen G, McGuire H, et al. Mental capacity in psychiatric patients: Systematic review Br J Psychiatry, 2007.PMID 17906238
- [8]Owen GS, David AS, Richardson G, et al. Mental capacity, diagnosis and insight in psychiatric in-patients: a cross-sectional study Psychol Med, 2009.PMID 18940026
- [9]Hindmarch T, Hotopf M, Owen GS Depression and decision-making capacity for treatment or research: a systematic review BMC Med Ethics, 2013.PMID 24330745
- [10]Sessums LL, Zembrzuska H, Jackson JL Does this patient have medical decision-making capacity? JAMA, 2011.PMID 21791691
- [11]Buchanan A Mental capacity, legal competence and consent to treatment J R Soc Med, 2004.PMID 15340019
- [12]Palmer BW, Harmell AL Assessment of Healthcare Decision-making Capacity Arch Clin Neuropsychol, 2016.PMID 27551024
- [13]Marcó-García S, Ariyo K, Owen GS, et al. Decision making capacity for treatment in psychiatric inpatients: a systematic review and meta-analysis Psychol Med, 2024.PMID 38433596
- [14]Kim SY, Karlawish JH, Caine ED Current state of research on decision-making competence of cognitively impaired elderly persons Am J Geriatr Psychiatry, 2002.PMID 11925276
- [15]Karlawish JH, Casarett DJ, James BD, et al. The ability of persons with Alzheimer disease (AD) to make a decision about taking an AD treatment Neurology, 2005.PMID 15883310
- [16]Palmer BW, Jeste DV Relationship of individual cognitive abilities to specific components of decisional capacity among middle-aged and older patients with schizophrenia Schizophr Bull, 2006.PMID 16192412